

Incidence, Predictive Factors and Long-Term Clinical Impact of Left Ventricular Remodeling According to the Completeness of Revascularization in Patients with ST-Elevation Myocardial Infarction and Multivessel Disease
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
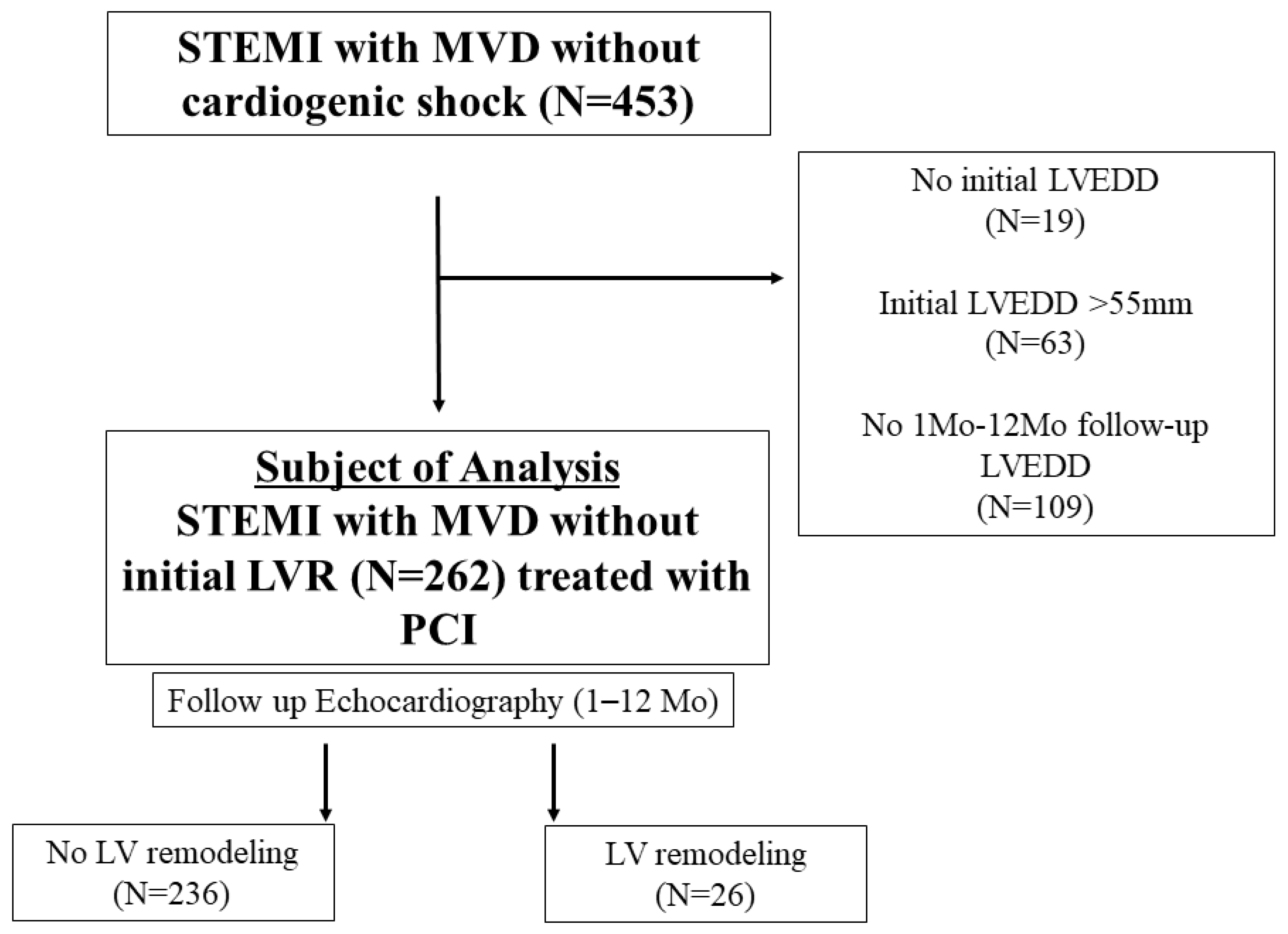
2.1. Study Population
2.2. Treatment and Data Collection
2.3. Study Definitions and Outcomes
2.4. Statistical Analysis
3. Results
3.1. Baseline, Therapeutic, and Angiographic Characteristics
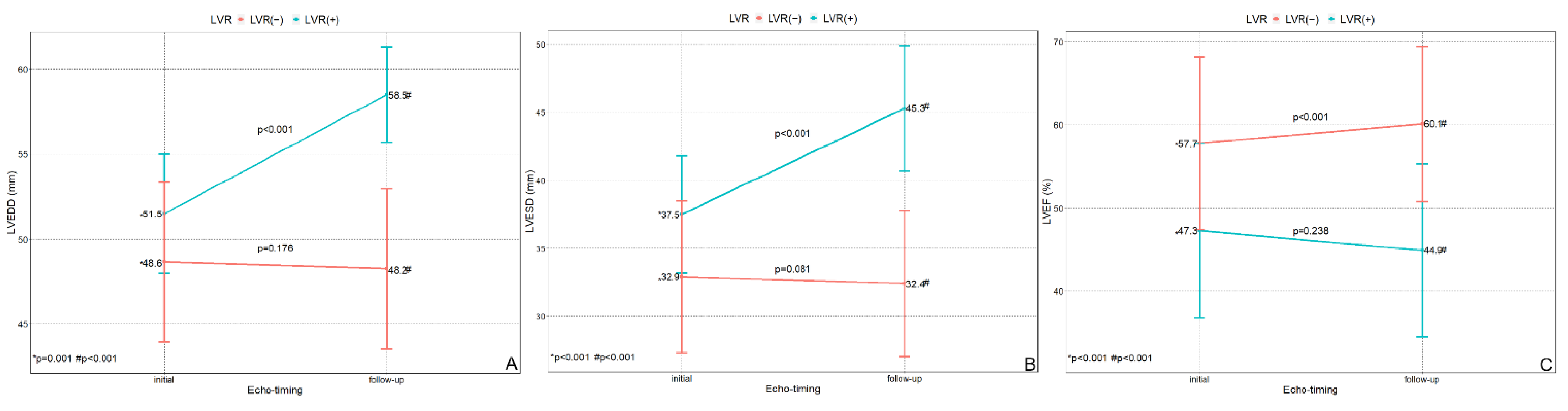
3.2. Echocardiographic Data
3.3. Factors Related to LVR
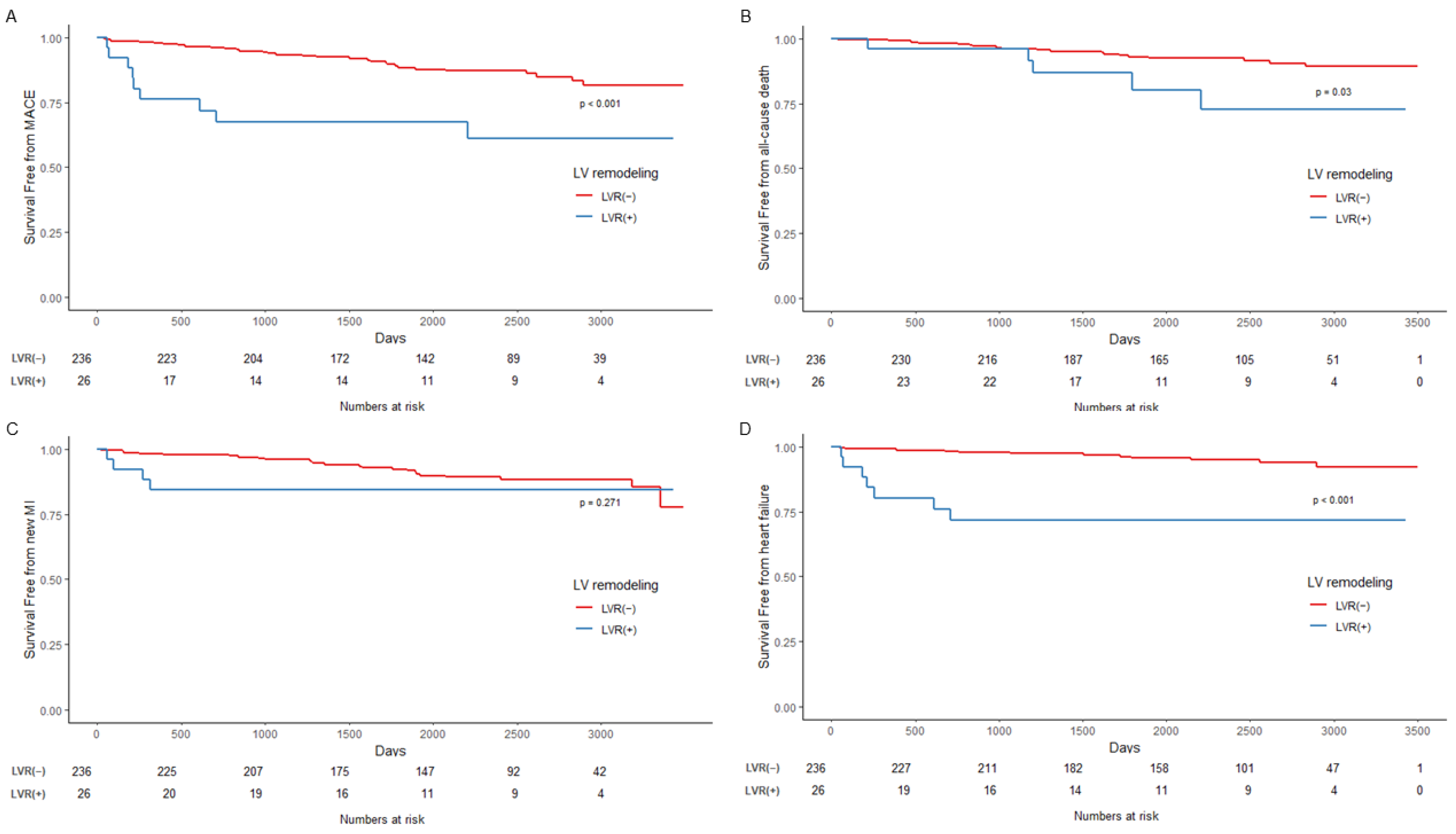
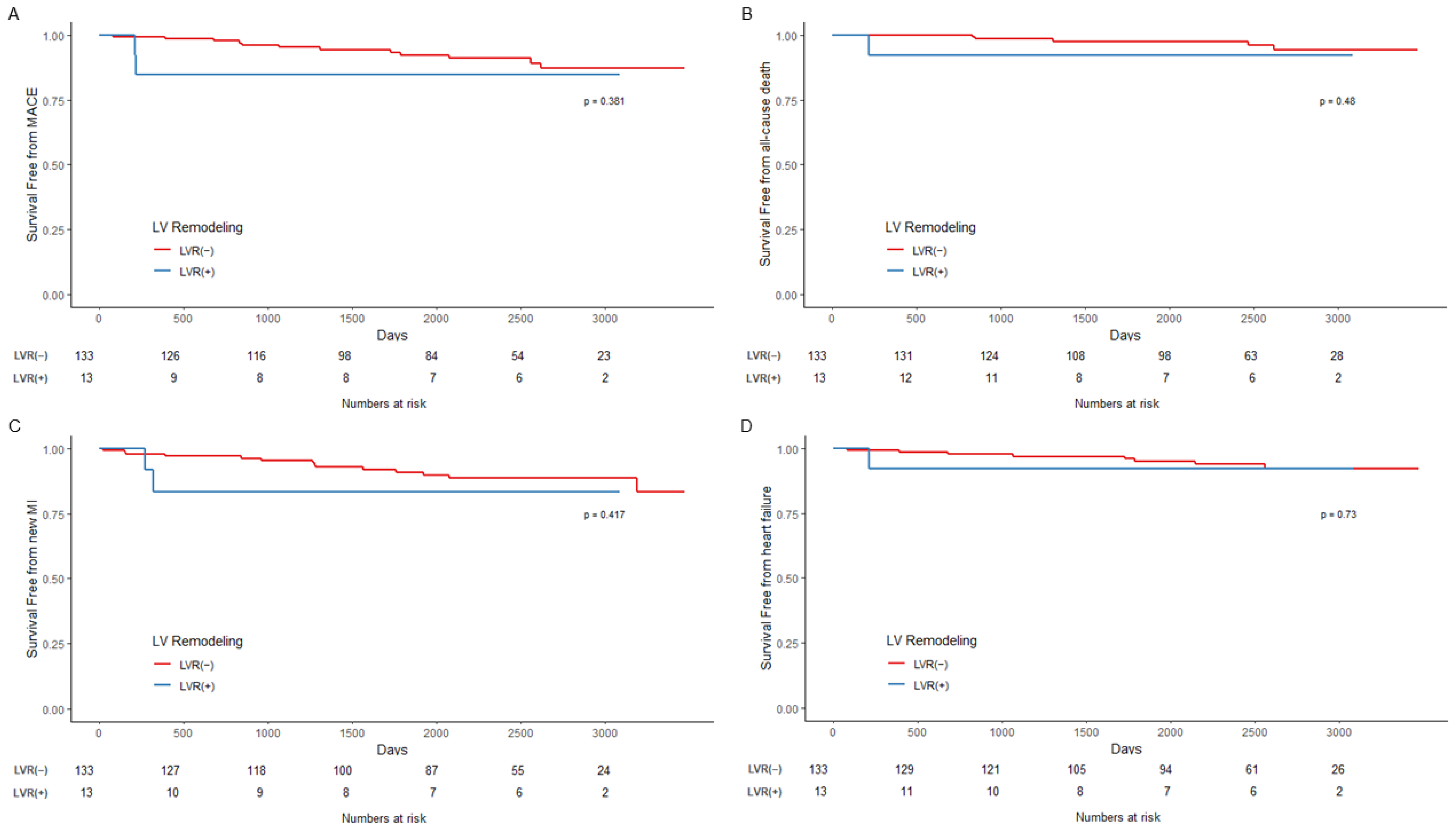
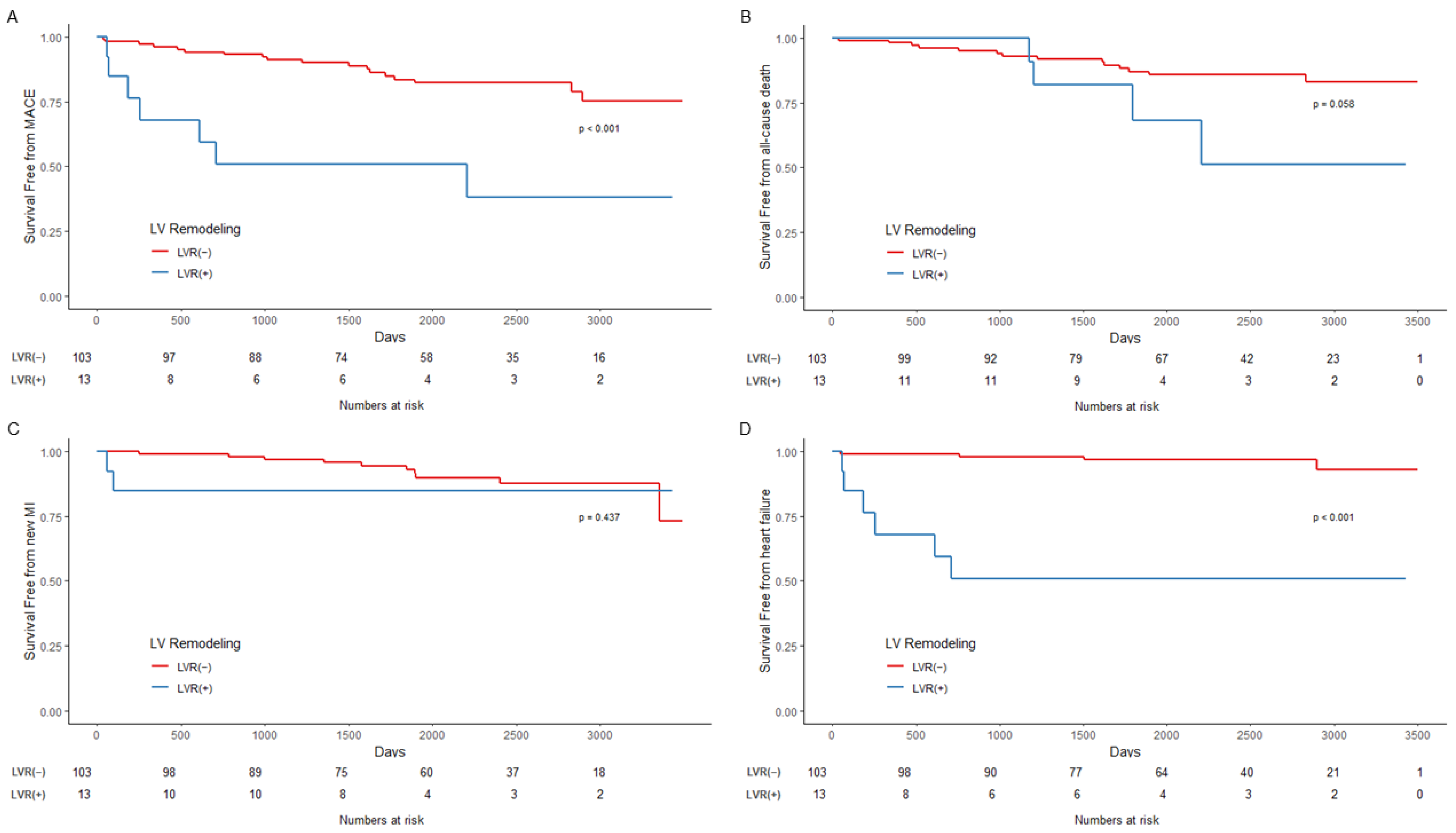
3.4. Outcomes According to LVR and PCI Strategy and Survival Analysis
4. Discussion
4.1. Definition and Incidence of LVR
4.2. Risk Factors for LVR Development
4.3. LVR and the Completeness of Revascularization: Impact on Long-Term Clinical Outcomes in STEMI with MVD
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Frantz, S.; Hundertmark, M.J.; Schulz-Menger, J.; Bengel, F.M.; Bauersachs, J. Left ventricular remodelling post-myocardial infarction: Pathophysiology, imaging, and novel therapies. Eur. Heart J. 2022, 43, ehac223. [Google Scholar] [CrossRef] [PubMed]
- Bolognese, L.; Neskovic, A.N.; Parodi, G.; Cerisano, G.; Buonamici, P.; Santoro, G.M.; Antoniucci, D. Left ventricular remodeling after primary coronary angioplasty: Patterns of left ventricular dilation and long-term prognostic implications. Circulation 2002, 106, 2351–2357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Bijl, P.; Abou, R.; Goedemans, L.; Gersh, B.J.; Holmes, D.R., Jr.; Ajmone Marsan, N.; Delgado, V.; Bax, J.J. Left Ventricular Post-Infarct Remodeling: Implications for Systolic Function Improvement and Outcomes in the Modern Era. JACC Heart Fail. 2020, 8, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Park, D.W.; Clare, R.M.; Schulte, P.J.; Pieper, K.S.; Shaw, L.K.; Califf, R.M.; Ohman, E.M.; Van de Werf, F.; Hirji, S.; Harrington, R.A.; et al. Extent, location, and clinical significance of non-infarct-related coronary artery disease among patients with ST-elevation myocardial infarction. JAMA 2014, 312, 2019–2027. [Google Scholar] [CrossRef]
- Tarantini, G.; Napodano, M.; Gasparetto, N.; Favaretto, E.; Marra, M.P.; Cacciavillani, L.; Bilato, C.; Osto, E.; Cademartiri, F.; Musumeci, G.; et al. Impact of multivessel coronary artery disease on early ischemic injury, late clinical outcome, and remodeling in patients with acute myocardial infarction treated by primary coronary angioplasty. Coron. Artery Dis. 2010, 21, 78–86. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; White, H.D.; Joint ESC/ACCF/AHA/WHF Task Force for the Redefinition of Myocardial Infarction. Universal definition of myocardial infarction. Eur. Heart J. 2007, 28, 2525–2538. [Google Scholar]
- Choi, J.O.; Shin, M.S.; Kim, M.J.; Jung, H.O.; Park, J.R.; Sohn, I.S.; Kim, H.; Park, S.M.; Yoo, N.J.; Choi, J.H.; et al. Normal Echocardiographic Measurements in a Korean Population Study: Part I. Cardiac Chamber and Great Artery Evaluation. J. Cardiovasc. Ultrasound 2015, 23, 158–172. [Google Scholar] [CrossRef] [Green Version]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–270. [Google Scholar] [CrossRef]
- van der Bijl, P.; Abou, R.; Goedemans, L.; Gersh, B.J.; Holmes, D.R., Jr.; Ajmone Marsan, N.; Delgado, V.; Bax, J.J. Left ventricular remodelling after ST-segment elevation myocardial infarction: Sex differences and prognosis. ESC Heart Fail. 2020, 7, 474–481. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Palomares, J.F.; Gavara, J.; Ferreira-Gonzalez, I.; Valente, F.; Rios, C.; Rodriguez-Garcia, J.; Bonanad, C.; Garcia Del Blanco, B.; Minana, G.; Mutuberria, M.; et al. Prognostic Value of Initial Left Ventricular Remodeling in Patients With Reperfused STEMI. JACC Cardiovasc. Imaging 2019, 12, 2445–2456. [Google Scholar] [CrossRef]
- Reindl, M.; Reinstadler, S.J.; Tiller, C.; Feistritzer, H.J.; Kofler, M.; Brix, A.; Mayr, A.; Klug, G.; Metzler, B. Prognosis-based definition of left ventricular remodeling after ST-elevation myocardial infarction. Eur. Radiol. 2019, 29, 2330–2339. [Google Scholar] [CrossRef] [PubMed]
- Bulluck, H.; Go, Y.Y.; Crimi, G.; Ludman, A.J.; Rosmini, S.; Abdel-Gadir, A.; Bhuva, A.N.; Treibel, T.A.; Fontana, M.; Pica, S.; et al. Defining left ventricular remodeling following acute ST-segment elevation myocardial infarction using cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2017, 19, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dujardin, K.S.; Enriquez-Sarano, M.; Rossi, A.; Bailey, K.R.; Seward, J.B. Echocardiographic assessment of left ventricular remodeling: Are left ventricular diameters suitable tools? J. Am. Coll. Cardiol. 1997, 30, 1534–1541. [Google Scholar] [CrossRef] [Green Version]
- Lombardo, A.; Niccoli, G.; Natale, L.; Bernardini, A.; Cosentino, N.; Bonomo, L.; Crea, F. Impact of microvascular obstruction and infarct size on left ventricular remodeling in reperfused myocardial infarction: A contrast-enhanced cardiac magnetic resonance imaging study. Int. J. Cardiovasc. Imaging 2012, 28, 835–842. [Google Scholar] [CrossRef] [PubMed]
- Masci, P.G.; Ganame, J.; Francone, M.; Desmet, W.; Lorenzoni, V.; Iacucci, I.; Barison, A.; Carbone, I.; Lombardi, M.; Agati, L.; et al. Relationship between location and size of myocardial infarction and their reciprocal influences on post-infarction left ventricular remodelling. Eur. Heart J. 2011, 32, 1640–1648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palazzuoli, A.; Beltrami, M.; Gennari, L.; Dastidar, A.G.; Nuti, R.; McAlindon, E.; Angelini, G.D.; Bucciarelli-Ducci, C. The impact of infarct size on regional and global left ventricular systolic function: A cardiac magnetic resonance imaging study. Int. J. Cardiovasc. Imaging 2015, 31, 1037–1044. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chia, S.; Senatore, F.; Raffel, O.C.; Lee, H.; Wackers, F.J.; Jang, I.K. Utility of cardiac biomarkers in predicting infarct size, left ventricular function, and clinical outcome after primary percutaneous coronary intervention for ST-segment elevation myocardial infarction. JACC Cardiovasc. Interv. 2008, 1, 415–423. [Google Scholar] [CrossRef] [Green Version]
- Hallen, J. Troponin for the estimation of infarct size: What have we learned? Cardiology 2012, 121, 204–212. [Google Scholar] [CrossRef]
- DeGeare, V.S.; Boura, J.A.; Grines, L.L.; O’Neill, W.W.; Grines, C.L. Predictive value of the Killip classification in patients undergoing primary percutaneous coronary intervention for acute myocardial infarction. Am. J. Cardiol. 2001, 87, 1035–1038. [Google Scholar] [CrossRef]
- Khot, U.N.; Jia, G.; Moliterno, D.J.; Lincoff, A.M.; Khot, M.B.; Harrington, R.A.; Topol, E.J. Prognostic importance of physical examination for heart failure in non-ST-elevation acute coronary syndromes: The enduring value of Killip classification. JAMA 2003, 290, 2174–2181. [Google Scholar] [CrossRef] [Green Version]
- Oh, P.C.; Choi, I.S.; Ahn, T.; Moon, J.; Park, Y.; Seo, J.G.; Suh, S.Y.; Ahn, Y.; Jeong, M.H. Predictors of recovery of left ventricular systolic dysfunction after acute myocardial infarction: From the korean acute myocardial infarction registry and korean myocardial infarction registry. Korean Circ. J. 2013, 43, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Agra Bermejo, R.; Cordero, A.; Garcia-Acuna, J.M.; Gomez Otero, I.; Varela Roman, A.; Martinez, A.; Alvarez Rodriguez, L.; Abou-Jokh, C.; Rodriguez-Manero, M.; Cid Alvarez, B.; et al. Determinants and Prognostic Impact of Heart Failure and Left Ventricular Ejection Fraction in Acute Coronary Syndrome Settings. Rev. Esp. Cardiol. (Engl. Ed.) 2018, 71, 820–828. [Google Scholar] [CrossRef] [PubMed]
- Vicent, L.; Velasquez-Rodriguez, J.; Valero-Masa, M.J.; Diez-Delhoyo, F.; Gonzalez-Saldivar, H.; Bruna, V.; Devesa, C.; Juarez, M.; Sousa-Casasnovas, I.; Fernandez-Aviles, F.; et al. Predictors of high Killip class after ST segment elevation myocardial infarction in the era of primary reperfusion. Int. J. Cardiol. 2017, 248, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthelemy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef] [PubMed]
- Lawton, J.S.; Tamis-Holland, J.E.; Bangalore, S.; Bates, E.R.; Beckie, T.M.; Bischoff, J.M.; Bittl, J.A.; Cohen, M.G.; DiMaio, J.M.; Don, C.W.; et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e18–e114. [Google Scholar] [CrossRef]
- Smits, P.C.; Boxma-de Klerk, B.M. Fractional Flow Reserve-Guided Multivessel Angioplasty in Myocardial Infarction. N. Engl. J. Med. 2017, 377, 397–398. [Google Scholar] [CrossRef]
- Wald, D.S.; Morris, J.K.; Wald, N.J.; Chase, A.J.; Edwards, R.J.; Hughes, L.O.; Berry, C.; Oldroyd, K.G.; Investigators, P. Randomized trial of preventive angioplasty in myocardial infarction. N. Engl. J. Med. 2013, 369, 1115–1123. [Google Scholar] [CrossRef] [Green Version]
- Bainey, K.R.; Engstrom, T.; Smits, P.C.; Gershlick, A.H.; James, S.K.; Storey, R.F.; Wood, D.A.; Mehran, R.; Cairns, J.A.; Mehta, S.R. Complete vs Culprit-Lesion-Only Revascularization for ST-Segment Elevation Myocardial Infarction: A Systematic Review and Meta-analysis. JAMA Cardiol. 2020, 5, 881–888. [Google Scholar] [CrossRef]
- Pavasini, R.; Biscaglia, S.; Barbato, E.; Tebaldi, M.; Dudek, D.; Escaned, J.; Casella, G.; Santarelli, A.; Guiducci, V.; Gutierrez-Ibanes, E.; et al. Complete revascularization reduces cardiovascular death in patients with ST-segment elevation myocardial infarction and multivessel disease: Systematic review and meta-analysis of randomized clinical trials. Eur. Heart J. 2020, 41, 4103–4110. [Google Scholar] [CrossRef]
- Kyhl, K.; Ahtarovski, K.A.; Nepper-Christensen, L.; Ekstrom, K.; Ghotbi, A.A.; Schoos, M.; Goransson, C.; Bertelsen, L.; Helqvist, S.; Holmvang, L.; et al. Complete Revascularization Versus Culprit Lesion Only in Patients With ST-Segment Elevation Myocardial Infarction and Multivessel Disease: A DANAMI-3-PRIMULTI Cardiac Magnetic Resonance Substudy. JACC Cardiovasc. Interv. 2019, 12, 721–730. [Google Scholar] [CrossRef]
- Mangion, K.; Carrick, D.; Hennigan, B.W.; Payne, A.R.; McClure, J.; Mason, M.; Das, R.; Wilson, R.; Edwards, R.J.; Petrie, M.C.; et al. Infarct size and left ventricular remodelling after preventive percutaneous coronary intervention. Heart 2016, 102, 1980–1987. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No LV Remodeling (N = 236) | LV Remodeling (N = 26) | p Value | |
|---|---|---|---|
| Age | 68.0 ± 11.9 | 71.5 ± 10.1 | 0.157 |
| Male | 173 (73.3%) | 18 (69.2%) | 0.833 |
| SBP (mmHg) | 130.0 [120.0; 150.0] | 130.0 [120.0; 140.0] | 0.187 |
| DBP (mmHg) | 80.0 [80.0; 90.0] | 80.0 [70.0; 90.0] | 0.21 |
| HR (/min) | 72.0 [64.0; 80.0] | 79.0 [68.0; 88.0] | 0.089 |
| Killip 1 | 197 (83.5%) | 20 (76.9%) | 0.571 |
| Killip 2 | 29 (12.3%) | 1 (3.8%) | 0.338 |
| Killip 3 | 10 (4.2%) | 5 (19.2%) | 0.007 |
| Previous CAD | 16 (6.8%) | 3 (11.5%) | 0.624 |
| Hypertension | 112 (47.5%) | 11 (42.3%) | 0.77 |
| DM | 67 (28.4%) | 11 (42.3%) | 0.212 |
| Smoking history | 149 (63.1%) | 16 (61.5%) | 1 |
| Previous CVA | 8 (3.4%) | 3 (11.5%) | 0.147 |
| LVEF (%) | 57.8 ± 10.4 | 47.3 ± 10.5 | <0.001 |
| LVEDD (mm) | 49.0 [46.0; 52.0] | 53.0 [50.0; 54.0] | 0.001 |
| Hemoglobin (mg/dL) | 13.1 [10.3; 14.8] | 13.3 [12.6; 14.8] | 0.515 |
| Glucose (mg/dL) | 155.0 [120.5; 187.0] | 162.5 [129.0; 197.0] | 0.592 |
| Creatinine (mg/dL) | 0.9 [ 0.8; 1.1] | 0.9 [ 0.8; 1.0] | 0.665 |
| CK-MB (ng/mL) | 55.9 [18.1; 109.2] | 89.2 [33.2; 169.3] | 0.06 |
| Peak Troponin-I (mg/dL) | 41.6 [16.3; 75.5] | 72.0 [28.1; 119.8] | 0.032 |
| NT-proBNP (pg/mL) | 216.0 [73.0; 511.0] | 310.5 [62.0; 632.0] | 0.789 |
| Total cholesterol (mg/dL) | 186.0 [161.0; 214.0] | 172.5 [155.0; 214.0] | 0.276 |
| LDL cholesterol (mg/dL) | 124.5 [103.0; 146.0] | 119.0 [103.0; 143.0] | 0.607 |
| HDL Cholesterol(mg/dL) | 44.0 [38.0; 52.0] | 39.5 [34.0; 50.0] | 0.064 |
| Triglyceride (mg/dL) | 106.0 [76.0; 142.0] | 81.5 [61.0; 132.0] | 0.034 |
| No LV Remodeling (N = 236) | LV Remodeling (N = 26) | p Value | |
|---|---|---|---|
| Door to balloon time (mins) | 78.0 [61.0;92.0] | 83.5 [53.0; 101.0] | 0.279 |
| Culpri | 0.739 | ||
| LM | 2 (0.8%) | 0 (0.0%) | |
| LAD | 95 (40.3%) | 13 (50.0%) | |
| LCX | 25 (10.6%) | 3 (11.5%) | |
| RCA | 114 (48.3%) | 10 (38.5%) | |
| Two-vessel disease | 156 (66.1%) | 17 (65.4%) | 1 |
| Three-vessel disease | 80 (33.9%) | 9 (34.6%) | 1 |
| Lesion types of a culprit lesion | 0.121 | ||
| Type B1 | 50 (21.2%) | 9 (34.6%) | |
| Type B2 | 121 (51.3%) | 14 (53.8%) | |
| Type C | 65 (27.5%) | 3 (11.5%) | |
| PCI | |||
| PCI using stent(s) | 234 (99.2%) | 26 (100.0%) | 1 |
| Thrombus aspiration | 15 (6.4%) | 2 (7.7%) | 1 |
| TIMI 3 flow after PCI for a culprit artery | 235 (99.6%) | 25 (96.2%) | 0.474 |
| Multivessel PCI | 169 (71.6%) | 17 (65.4%) | 0.663 |
| Staged PCI | 133 (56.4%) | 17 (65.4%) | 0.5 |
| CR | 133 (56.4%) | 13 (50.0%) | 0.681 |
| Complications during hospitalization | |||
| AKI | 2 (0.8%) | 0 (0.0%) | 1 |
| AV block | 12 (5.1%) | 1 (3.8%) | 1 |
| VF or Pulseless VT | 8 (3.4%) | 0 (0.0%) | 0.724 |
| TPM | 19 (8.1%) | 2 (7.7%) | 1 |
| IABP | 5 (2.1%) | 0 (0.0%) | 1 |
| Discharge medication | |||
| Aspirin | 236(100%) | 26(100%) | |
| Clopidogrel | 235 (99.6%) | 26 (100.0%) | 1 |
| Cilostazole | 149 (63.1%) | 15 (57.7%) | 0.741 |
| Beta-blocker | 210 (89.0%) | 22 (84.6%) | 0.734 |
| ACE inhibitor or ARB | 186 (78.8%) | 21 (80.8%) | 1 |
| Statin | 200 (85.1%) | 20 (76.9%) | 0.421 |
| Spironolactone | 19 (8.2%) | 6 (23.1%) | 0.038 |
| Medication at 1 y | |||
| Beta-blocker | 167 (78.8%) | 19 (76.0%) | 0.951 |
| ACE inhibitor or ARB | 183 (86.3%) | 22 (88.0%) | 1.000 |
| Spironolactone | 10 (4.7%) | 6 (24.0%) | 0.001 |
| Statin | 186 (87.7%) | 20 (80.0%) | 0.440 |
| Factors | Univariable | Multivariable | ||
|---|---|---|---|---|
| Unadjusted OR (95% CI) | p Value | Adjusted OR (95% CI) | p Value | |
| Age > 65 | 2.05 (0.80–5.31) | 0.137 | ||
| Male | 0.82 (0.34–1.98) | 0.657 | ||
| Initial LVEF < 50% | 5.20 (2.25–12.04) | <0.001 | 3.62 (1.45–9.07) | 0.006 |
| LVEDD > 50 mm | 3.34 (1.40–7.99) | 0.006 | 2.47 (0.97–6.26) | 0.056 |
| Killip 2 | 0.29 (0.04–2.19) | 0.227 | ||
| Killip 3 | 5.38 (1.68–17.21) | 0.004 | 4.89 (1.31–18.30) | 0.018 |
| Hypertension | 0.81 (0.36–1.84) | 0.618 | ||
| DM | 1.85 (0.81–4.23) | 0.145 | ||
| Creatinine > 1.5 mg/dL | 1.32 (0.28–6.17) | 0.722 | ||
| Hemoglobin < 10 (mg/dL) | 0.43 (0.12–1.48) | 0.181 | ||
| Beta-blocker at discharge | 0.68 (0.22–2.13) | 0.509 | ||
| ACE inhibitor or ARB at discharge | 1.13 (0.41–3.14) | 0.816 | ||
| Statin at discharge | 0.58(0.22–1.55) | 0.276 | ||
| LAD or LM as a culprit | 1.43 (0.64–3.23) | 0.384 | ||
| Three-vessel disease | 1.03 (0.44–2.42) | 0.941 | ||
| Complete revascularization | 0.77 (0.34–1.74) | 0.536 | ||
| Peak Troponin I > 70 mg/dL | 2.58 (1.13–5.85) | 0.023 | 2.79 (1.09–7.17) | 0.032 |
| LDL cholesterol > 100 mg/dL | 1.06 (0.41–2.77) | 0.903 | ||
| NT pro-BNP > 400 pg/mL | 3.04 (1.33–6.95) | 0.008 | 2.40 (0.96–6.00) | 0.061 |
| HbA1c > 8% | 2.01 (0.70–5.80) | 0.196 |
| Total | |||
|---|---|---|---|
| No LV remodeling (N = 236) | LV remodeling (N = 26) | p value | |
| MACE | 30 (12.7%) | 9 (34.6%) | 0.007 |
| AD | 19 (8.1%) | 5 (19.2%) | 0.129 |
| MI | 24 (10.2%) | 4 (15.4%) | 0.629 |
| HF | 12 (5.1%) | 7 (26.9%) | <0.001 |
| Complete revascularization | |||
| No LV remodeling (N = 133) | LV remodeling (N = 13) | p value | |
| MACE | 12 (9.0%) | 2 (15.4%) | 0.803 |
| AD | 5 (3.8%) | 1 (7.7%) | 1 |
| MI | 14 (10.5%) | 2 (15.4%) | 0.944 |
| HF | 8 (6.0%) | 1 (7.7%) | 1 |
| Incomplete revascularization | |||
| No LV remodeling (N = 103) | LV remodeling (N = 13) | p value | |
| MACE | 18 (17.5%) | 7 (53.8%) | 0.008 |
| AD | 14 (13.6%) | 4 (30.8%) | 0.228 |
| MI | 10 (9.7%) | 2 (15.4%) | 0.881 |
| HF | 4 (3.9%) | 6 (46.2%) | 0.001 |
| Total | ||||||
|---|---|---|---|---|---|---|
| Unadjusted HR (95% CI) | p value | Adjusted HR (95% CI) | p value | IPTW-Adjusted HR (95% CI) | p value | |
| MACE | 3.54 (1.68–7.47) | 0.001 | 2.09 (0.86–5.08) | 0.10 | 2.19 (0.96–4.96) | 0.059 |
| AD | 2.84 (1.06–7.61) | 0.038 | 1.95 (0.71–5.32) | 0.191 | 1.66 (0.72–3.83) | 0.23 |
| MI | 1.80 (0.62–5.20) | 0.278 | 1.68 (0.55–5.06) | 0.356 | 1.41 (0.42–4.69) | 0.569 |
| HF | 6.66 (2.62–16.95) | <0.001 | 3.98 (1.44–11.02) | 0.004 | 2.61 (0.95–7.11) | 0.06 |
| Complete revascularization | ||||||
| Unadjusted HR (95% CI) | p value | Adjusted HR (95% CI) | p value | IPTW-adjusted HR (95% CI) | p value | |
| MACE | 1.93 (0.43–8.68) | 0.39 | 1.79 (0.39–8.21) | 0.44 | 1.26 (0.27–5.89) | 0.76 |
| AD | 2.13 (0.25–18.26) | 0.49 | 0.86 (0.09–8.14) | 0.89 | 0.73 (0.068–8.58) | 0.80 |
| MI | 1.84 (0.41–8.14) | 0.424 | 1.33(0.27–6.33) | 0.77 | 1.19 (0.34–4.08) | 0.71 |
| HF | 1.44 (0.18–11.53) | 0.732 | 0.98 (0.11–8.59) | 0.99 | 0.80 (0.10–6.00) | 0.83 |
| Incomplete revascularization | ||||||
| Unadjusted HR (95% CI) | p value | Adjusted HR (95% CI) | p value | IPTW-adjusted HR (95% CI) | p value | |
| MACE | 4.49 (1.87–10.80) | 0.001 | 3.51 (1.34–9.18) | 0.01 | 3.22 (1.19–8.71) | 0.02 |
| AD | 2.81 (0.92–8.56) | 0.07 | 1.91 (0.58–6.25) | 0.33 | 2.09 (0.66–6.58) | 0.20 |
| MI | 1.83 (0.39–8.59) | 0.44 | 1.66 (0.31–8.83) | 0.55 | 1.71 (0.32–8.99) | 0.52 |
| HF | 16.59 (4.64–59.29) | <0.001 | 23.65 (5.64–99.06) | <0.001 | 18.98 (4.79–75.10) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, M.C.; Lim, Y.; Ahn, Y.; Ahn, J.H.; Lee, S.H.; Hyun, D.Y.; Cho, K.H.; Sim, D.S.; Hong, Y.J.; Kim, J.H.; et al. Incidence, Predictive Factors and Long-Term Clinical Impact of Left Ventricular Remodeling According to the Completeness of Revascularization in Patients with ST-Elevation Myocardial Infarction and Multivessel Disease. J. Clin. Med. 2022, 11, 6252. https://doi.org/10.3390/jcm11216252
Kim MC, Lim Y, Ahn Y, Ahn JH, Lee SH, Hyun DY, Cho KH, Sim DS, Hong YJ, Kim JH, et al. Incidence, Predictive Factors and Long-Term Clinical Impact of Left Ventricular Remodeling According to the Completeness of Revascularization in Patients with ST-Elevation Myocardial Infarction and Multivessel Disease. Journal of Clinical Medicine. 2022; 11(21):6252. https://doi.org/10.3390/jcm11216252
Chicago/Turabian StyleKim, Min Chul, Yongwhan Lim, Youngkeun Ahn, Joon Ho Ahn, Seung Hun Lee, Dae Young Hyun, Kyung Hoon Cho, Doo Sun Sim, Young Joon Hong, Ju Han Kim, and et al. 2022. "Incidence, Predictive Factors and Long-Term Clinical Impact of Left Ventricular Remodeling According to the Completeness of Revascularization in Patients with ST-Elevation Myocardial Infarction and Multivessel Disease" Journal of Clinical Medicine 11, no. 21: 6252. https://doi.org/10.3390/jcm11216252
APA StyleKim, M. C., Lim, Y., Ahn, Y., Ahn, J. H., Lee, S. H., Hyun, D. Y., Cho, K. H., Sim, D. S., Hong, Y. J., Kim, J. H., & Jeong, M. H. (2022). Incidence, Predictive Factors and Long-Term Clinical Impact of Left Ventricular Remodeling According to the Completeness of Revascularization in Patients with ST-Elevation Myocardial Infarction and Multivessel Disease. Journal of Clinical Medicine, 11(21), 6252. https://doi.org/10.3390/jcm11216252