
Doll Therapy Intervention Reduces Challenging Behaviours of Women with Dementia Living in Nursing Homes: Results from a Randomized Single-Blind Controlled Trial

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Ethical Consideration and Consent to Participate
2.3. Intervention
2.4. Primary Outcomes’ Measurements
2.4.1. Patient’s BPSD
2.4.2. Professional Caregivers’ Distress
2.4.3. Patient’s Biomarkers of Stress
2.4.4. Patient’s Interaction with the Object
2.5. Statistical Analysis
2.5.1. Sample Size
2.5.2. Analysis
3. Results
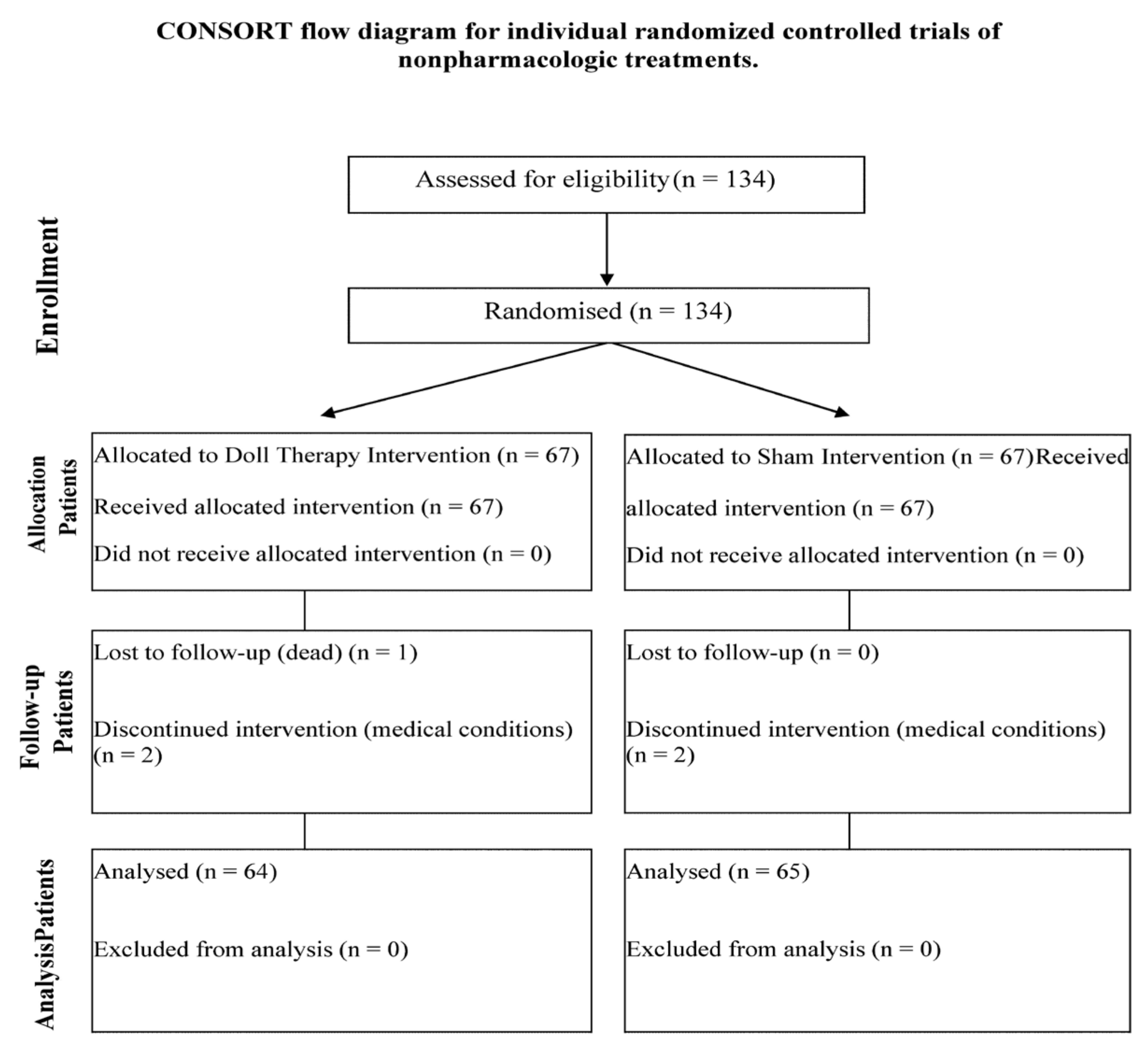
3.1. Participants
3.2. Baseline Characteristics
3.3. Patient’s BPSD and Caregivers’ Distress
3.4. Patient’s Biomarkers of Stress
3.5. Patient’s Interaction with the Object
3.5.1. Object Presentation
3.5.2. Separation from the Nurse
3.5.3. Interaction with the Object
3.5.4. Separation from the Object
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- International Psychogeriatric Association IPA Complete Guides to Behavioral and Psychological Symptoms of Dementia (BPSD). Available online: https://www.ipa-online.org/publications/guides-to-bpsd (accessed on 2 March 2022).
- Van der Linde, R.M.; Dening, T.; Stephan, B.C.M.; Prina, A.M.; Evans, E.; Brayne, C. Longitudinal Course of Behavioural and Psychological Symptoms of Dementia: Systematic Review. Br. J. Psychiatry 2016, 209, 366–377. [Google Scholar] [CrossRef]
- Zhao, Q.; Tan, L.; Wang, H.; Jiang, T.; Tan, M.; Tan, L.; Xu, W.; Li, J.; Wang, J.; Lai, T.; et al. The Prevalence of Neuropsychiatric Symptoms in Alzheimer’s Disease: Systematic Review and Meta-Analysis. J. Affect. Disord. 2016, 190, 264–271. [Google Scholar] [CrossRef] [PubMed]
- Hazelhof, T.; Schoonhoven, L.; van Gaal, B.; Koopmans, R.; Gerritsen, D. Nursing Staff Stress from Challenging Behaviour of Residents with Dementia: A Concept Analysis. Int. Nurs. Rev. Rev. 2016, 63, 507–516. [Google Scholar] [CrossRef] [PubMed]
- Hongisto, K.; Hallikainen, I.; Selander, T.; Törmälehto, S.; Väätäinen, S.; Martikainen, J.; Välimäki, J.; Hartikainen, S.; Suhonen, J.; Koivisto, A. Quality of Life in Relation to Neuropsychiatric Symptoms in Alzheimer’s Disease: 5-Year Prospective ALSOVA Cohort Study. Int. J. Geriatr. Psychiatry 2018, 33, 47–57. [Google Scholar] [CrossRef] [PubMed]
- Ng, Q.X.; Ho, C.Y.X.; Koh, S.S.H.; Tan, W.C.; Chan, H.W. Doll Therapy for Dementia Sufferers: A Systematic Review. Complement. Ther. Clin. Pract. 2017, 26, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Pezzati, R.; Molteni, V.; Bani, M.; Settanta, C.; Di Maggio, M.G.; Villa, I.; Poletti, B.; Ardito, R.B. Can Doll Therapy Preserve or Promote Attachment in People with Cognitive, Behavioral, and Emotional Problems? A Pilot Study in Institutionalized Patients with Dementia. Front. Psychol. 2014, 5, 342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mackenzie, L.; James, I.A.; Morse, R.; Mukaetova-Ladinska, E.; Reichelt, F.K. A Pilot Study on the Use of Dolls for People with Dementia. Age Ageing 2006, 35, 441–444. [Google Scholar] [CrossRef] [Green Version]
- Ellingford, L.; Mackenzie, L.; Marsland, L. Using Dolls to Alter Behavior in People with Dementia. Nurs. Times 2007, 103, 36–37. [Google Scholar]
- Fraser, F.; James, I. Why Does Doll Therapy Improve the Well-Being of Some Older Adults with Dementia? PSIGE Newsl. 2008, 105, 55–63. [Google Scholar]
- Braden, B.A.; Gaspar, P.M. Implementation of a Baby Doll Therapy Protocol for People with Dementia: Innovative Practice. Dementia 2015, 14, 696–706. [Google Scholar] [CrossRef]
- Mitchell, G.; McCormack, B.; McCance, T. Therapeutic Use of Dolls for People Living with Dementia: A Critical Review of the Literature. Dementia 2014, 15, 976–1001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cantarella, A.; Borella, E.; Faggian, S.; Navuzzi, A.; De Beni, R. Using Dolls for Therapeutic Purposes: A Study on Nursing Home Residents with Severe Dementia. Int. J. Geriatr. Psychiatry 2018, 33, 915–925. [Google Scholar] [CrossRef] [PubMed]
- Santagata, F.; Massaia, M.; D’Amelio, P. The Doll Therapy as a First Line Treatment for Behavioral and Psychologic Symptoms of Dementia in Nursing Homes Residents: A Randomized, Controlled Study. BMC Geriatr. 2021, 21, 545. [Google Scholar] [CrossRef] [PubMed]
- Balzotti, A.; Filograsso, M.; Altamura, C.; Fairfield, B.; Bellomo, A.; Daddato, F.; Vacca, R.A.; Altamura, M. Comparison of the Efficacy of Gesture-Verbal Treatment and Doll Therapy for Managing Neuropsychiatric Symptoms in Older Patients with Dementia. Int. J. Geriatr. Psychiatry 2019, 34, 1308–1315. [Google Scholar] [CrossRef] [PubMed]
- Xiang, Q.; Yih, C.; Ho, X.; Shao, S.; Koh, H.; Chuan, W.; Wuen, H. Complementary Therapies in Clinical Practice Doll Therapy for Dementia Sufferers: A Systematic Review. Complement. Ther. Clin. Pract. 2017, 26, 42–46. [Google Scholar] [CrossRef]
- Bowlby, J. The Making and Breaking of Affectional Bonds. I. Aetiology and Psychopathology in the Light of Attachment Theory. An Expanded Version of the Fiftieth Maudsley Lecture, Delivered before the Royal College of Psychiatrists, 19 November 1976. Br. J. Psychiatry 1977, 130, 201–210. [Google Scholar] [CrossRef] [Green Version]
- Bisiani, L.; Angus, J. Doll Therapy: A Therapeutic Means to Meet Past Attachment Needs and Diminish Behaviours of Concern in a Person Living with Dementia-a Case Study Approach. Dementia 2013, 12, 447–462. [Google Scholar] [CrossRef]
- Bradley, J.M.; Cafferty, T.P. Attachment among Older Adults: Current Issues and Directions for Future Research. Attach. Hum. Dev. 2001, 3, 200–221. [Google Scholar] [CrossRef]
- Consedine, N.S.; Magai, C. Attachment and Emotion Experience in Later Life: The View from Emotions Theory. Attach. Hum. Dev. 2003, 5, 1651–1687. [Google Scholar] [CrossRef]
- Miesen, B.; Jones, G. Care-Giving in Dementia: Contours of a Curriculum. Dementia 2010, 9, 473–489. [Google Scholar] [CrossRef]
- Alander, H.; Prescott, T.; James, I.A. Older Adults’ Views and Experiences of Doll Therapy in Residential Care Homes. Dementia 2015, 14, 574–588. [Google Scholar] [CrossRef] [PubMed]
- Tsigos, C.; Chrousos, G.P. Hypothalamic-Pituitary-Adrenal Axis, Neuroendocrine Factors and Stress. J. Psychosom. Res. 2002, 53, 865–871. [Google Scholar] [CrossRef]
- Lupien, S.J.; Lepage, M. Stress, Memory, and the Hippocampus: Can’t Live with It, Can’t Live without It. Behav. Brain Res. 2001, 127, 137–158. [Google Scholar] [CrossRef]
- Vreeburg, S.A.; Zitman, F.G.; van Pelt, J.; Derijk, R.H.; Verhagen, J.C.M.; van Dyck, R.; Hoogendijk, W.J.G.; Smit, J.H.; Penninx, B.W.J.H. Salivary Cortisol Levels in Persons with and without Different Anxiety Disorders. Psychosom. Med. 2010, 72, 340–347. [Google Scholar] [CrossRef]
- Ng, T.K.S.; Feng, L.; Fam, J.; Rawtaer, I.; Kumar, A.P.; Rane, G.; Cheah, I.K.M.; Mahendran, R.; Lee, Y.K.; Tan, E.C.; et al. Mindfulness Awareness Practice (MAP) to Prevent Dementia in Older Adults with Mild Cognitive Impairment: Protocol of a Randomized Controlled Trial and Implementation Outcomes. Int. J. Environ. Res. Public Health 2021, 18, 10205. [Google Scholar] [CrossRef]
- Randomizer Research Randomizer. Available online: https://www.randomizer.org/ (accessed on 1 February 2017).
- Reisberg, B.; Ferris, S.H.; de Leon, M.J.; Crook, T. The Global Deterioration Scale for assessment of primary degenerative dementia. Am. J. Psychiatry 1982, 139, 1136–1139. [Google Scholar]
- Vaccaro, R.; Ballabio, R.; Molteni, V.; Ceppi, L.; Ferrari, B.; Cantù, M.; Zaccaria, D.; Vandoni, C.; Ardito, R.B.; Adenzato, M.; et al. Doll Therapy Intervention for Women with Dementia Living in Nursing Homes: A Randomized Single-Blind Controlled Trial Protocol. Trials 2020, 21, 133. [Google Scholar] [CrossRef] [Green Version]
- Dusyma GmbH Joyk®-Empathy Dolls Made by Dusyma. Available online: https://www.dusyma.com/en/--cms-page.blog.joyk-empathiepuppen (accessed on 13 September 2022).
- Cummings, J.L.; Mega, M.; Gray, K.; Rosenberg-Thompson, S.; Carusi, D.A.; Gornbein, J. The Neuropsychiatric Inventory: Comprehensive Assessment of Psychopathology in Dementia. Neurology 1994, 44, 2308–2314. [Google Scholar] [CrossRef] [Green Version]
- Baranzini, F.; Grecchi, A.; Berto, E.; Costantini, C.; Ceccon, F.; Cazzamalli, S.; Callegari, C. Factor Analysis and Psychometric Properties of the Italian Version of the Neuropsychiatric Inventory-Nursing Home in a Population of Institutionalized Elderly in Psychiatric Comorbidity. Riv. Psichiatr. 2013, 48, 335–344. [Google Scholar]
- Lehrer, P.; Eddie, D. Dynamic Processes in Regulation and Some Implications for Biofeedback and Biobehavioral Interventions. Appl. Psychophysiol. Biofeedback 2013, 38, 143–155. [Google Scholar] [CrossRef] [Green Version]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A Flexible Statistical Power Analysis Program for the Social, Behavioral, and Biomedical Sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. A Power Primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Lanctôt, K.L.; Amatniek, J.; Ancoli-Israel, S.; Arnold, S.E.; Ballard, C.; Cohen-Mansfield, J.; Ismail, Z.; Lyketsos, C.; Miller, D.S.; Musiek, E.; et al. Neuropsychiatric signs and symptoms of Alzheimer’s disease: New treatment paradigms. Alzheimers Dement. 2017, 3, 440–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kales, H.C.; Gitlin, L.N.; Lyketsos, C.G. Management of Neuropsychitric Symptoms of Dementia in Clinical Setting: Recommendations from a Multidisciplinary Expert Panel. J. Am. Geriatr. Soc. 2015, 62, 762–769. [Google Scholar] [CrossRef] [PubMed]
- Moyle, W.; Murfield, J.; Jones, C.; Beattie, E.; Draper, B.; Moyle, W.; Murfield, J.; Jones, C.; Beattie, E.; Draper, B. Can Lifelike Baby Dolls Reduce Symptoms of Anxiety, Agitation, or Aggression for People with Dementia in Long-Term Care? Findings from a Pilot Randomised Controlled Trial. Aging Ment. Health 2018, 23, 1442–1450. [Google Scholar] [CrossRef]
- Losada-Baltar, A.; Jiménez-Gonzalo, L. Translating Evidence into Practice: Nonpharmacological Interventions for BPSD. Int. Psychogeriatr. 2021, 33, 867–869. [Google Scholar] [CrossRef]
- Bennett, S.; Laver, K.; MacAndrew, M.; Beattie, E.; Clemson, L.; Runge, C.; Richardson, L. Implementation of Evidence-Based, Non-Pharmacological Interventions Addressing Behavior and Psychological Symptoms of Dementia: A Systematic Review Focused on Implementation Strategies. Int. Psychogeriatr. 2021, 33, 947–975. [Google Scholar] [CrossRef]
- Mitchell, G.; O’Donnell, H. The Therapeutic Use of Doll Therapy in Dementia. Br. J. Nurs. 2013, 22, 329–334. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, G.; Templeton, M. Ethical Considerations of Doll Therapy for People with Dementia. Nurs. Ethics 2014, 21, 720–730. [Google Scholar] [CrossRef] [Green Version]
- Minshull, K. The Impact of Doll Therapy on Well-Being of People with Dementia. J. Dement. Care 2009, 17, 35–38. [Google Scholar]
- Hestad, K.A.; Engedal, K.; Selbæk, G.; Strand, B.H. Blood Pressure in Dementia, Mild Cognitive Impairment, and Subjective Cognitive Decline Related to Time of Death. Brain Behav. 2021, 11, e02166. [Google Scholar] [CrossRef] [PubMed]
- Ardito, R.B.; Adenzato, M.; Dell’Osbell, G.; Izard, E.; Veglia, F. Attachment Representations in Adults with Congenital Blindness: Association with Maternal Interactive Behaviors During Childhood. Psychol. Rep. 2004, 95, 263–274. [Google Scholar] [CrossRef] [PubMed]
- Adenzato, M.; Ardito, R.B.; Izard, E. Impact of Maternal Directiveness and Overprotectiveness on the Personality Development of a Sample of Individuals with Acquired Blindness. Soc. Behav. Pers. 2006, 34, 17–26. [Google Scholar] [CrossRef] [Green Version]
- Cohen-Mansfield, J. Nonpharmacological Treatment of Behavioral Disorders in Dementia. Curr. Treat. Options Neurol. 2013, 15, 765–785. [Google Scholar] [CrossRef]


{kind=link}
| DTI (n = 64) | SI (n = 65) | |
|---|---|---|
| Age, mean (SD) | 86.9 (5.9) | 88.4 (5.5) |
| Pre-intervention # NPI-NH total score (range 0–144), mean (SD) | 33.84 (13.28) | 31.55 (12.1) |
| Pre-intervention ¥ NPI-NH Distress score (range 0–60), mean (SD) | 12.08 (5.4) | 10.6 (5.04) |
| Pre-intervention psychotropic medications, mean (SD) | 1.87 (1.11) | 1.81 (1.08) |
| Mini Mental State Examination (range 1–30), mean (SD) | 7.92 (4.95) | 10.27 (5.32) |
| Global Deterioration Scale (range 1–7), median (iqr) | 6 (5–7) | 6 (5–7) |
| Diagnosis, n (%) | ||
| Alzheimer | 23 (35.9) | 24 (36.9) |
| Vascular | 2 (3.1) | 4 (6.2) |
| Mixed | 7 (10.7) | 9 (13.8) |
| Other | 8 (12.5) | 3 (4.6) |
| Non specified dementia | 24 (37.5) | 25 (38.5) |
| DTI (n = 64) | SI (n = 65) | ||||||
|---|---|---|---|---|---|---|---|
| Post-Intervention | Adjusted Mean (SE) | 95% CI | Adjusted Mean (SE) | 95% CI | ¶ F | p-Value | § Partial Ƞ2 |
| NPI-NH total score | 21.067 (1.014) | 19.061–23.073 | 28.508 (1.018) | 26.492–30.523 | 43.433 | <0.001 | 0.638 |
| NPI-NH Distress score | 7.612 (0.435) | 6.751–8.473 | 10.093 (0.432) | 9.237–10.948 | 40.970 | <0.001 | 0.625 |
| DTI | SI | ¶ z | |
|---|---|---|---|
| Systolic pressure ratio at the 1st session | 1 (0.95–1.07) | 1 (0.94–1.08) | −0.069 |
| Systolic pressure ratio at the 30th session | 1 (0.95–1.08) | 1 (0.94–1.08) | −1.180 |
| Diastolic pressure ratio at the 1st session | 1 (0.97–1.07) | 1 (0.93–1.11) | −0.687 |
| Diastolic pressure ratio at the 30th session | 1 (0.93–1.07) | 1 (0.92–1.05) | −0.661 |
| Heart rate ratio at the 1st session | 1 (0.94–1.09) | 1 (0.93–1.04) | −1.147 |
| Heart rate ratio at the 30th session | 1 (0.97–1.11) | 0.98 (0.93–1.05) | −1.946 |
| Post-intervention | |||||
|---|---|---|---|---|---|
| Irrelevant # | Effective ¥ | Negative ¶ | |||
| Pre-intervention | Irrelevant # | 2 (28.6) | 2 (22.2) | 0 (0) | |
| DTI (n = 19) | Effective ¥ | 3 (42.9) | 6 (66.7) | 3 (100) | |
| Negative ¶ | 2 (28.6) | 1 (11.1) | 0 (0) | ||
| Pre-intervention | Irrelevant # | 4 (36.4) | 2 (25) | 2 (28.6) | |
| SI (n = 26) | Effective ¥ | 3 (27.3) | 6 (75) | 4 (57.1) | |
| Negative ¶ | 4 (36.4) | 0 (0) | 1 (14.3) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Molteni, V.; Vaccaro, R.; Ballabio, R.; Ceppi, L.; Cantù, M.; Ardito, R.B.; Adenzato, M.; Poletti, B.; Guaita, A.; Pezzati, R. Doll Therapy Intervention Reduces Challenging Behaviours of Women with Dementia Living in Nursing Homes: Results from a Randomized Single-Blind Controlled Trial. J. Clin. Med. 2022, 11, 6262. https://doi.org/10.3390/jcm11216262
Molteni V, Vaccaro R, Ballabio R, Ceppi L, Cantù M, Ardito RB, Adenzato M, Poletti B, Guaita A, Pezzati R. Doll Therapy Intervention Reduces Challenging Behaviours of Women with Dementia Living in Nursing Homes: Results from a Randomized Single-Blind Controlled Trial. Journal of Clinical Medicine. 2022; 11(21):6262. https://doi.org/10.3390/jcm11216262
Chicago/Turabian StyleMolteni, Valentina, Roberta Vaccaro, Roberta Ballabio, Laura Ceppi, Marco Cantù, Rita B. Ardito, Mauro Adenzato, Barbara Poletti, Antonio Guaita, and Rita Pezzati. 2022. "Doll Therapy Intervention Reduces Challenging Behaviours of Women with Dementia Living in Nursing Homes: Results from a Randomized Single-Blind Controlled Trial" Journal of Clinical Medicine 11, no. 21: 6262. https://doi.org/10.3390/jcm11216262
APA StyleMolteni, V., Vaccaro, R., Ballabio, R., Ceppi, L., Cantù, M., Ardito, R. B., Adenzato, M., Poletti, B., Guaita, A., & Pezzati, R. (2022). Doll Therapy Intervention Reduces Challenging Behaviours of Women with Dementia Living in Nursing Homes: Results from a Randomized Single-Blind Controlled Trial. Journal of Clinical Medicine, 11(21), 6262. https://doi.org/10.3390/jcm11216262