

Suicidality as a Predictor of Overdose among Patients with Substance Use Disorders
 , , ,
, , ,  , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Independent Variable: Suicidality
2.3. Dependent Variable and Adjudication Process: Overdose Events
2.4. Covariates
2.5. Analytic Plan
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- O’Donnell, J.; Tanz, L.J.; Gladden, R.M.; Davis, N.L.; Bitting, J. Trends in and Characteristics of Drug Overdose Deaths Involving Illicitly Manufactured Fentanyls—United States, 2019–2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1740–1746. [Google Scholar] [CrossRef]
- Han, B.; Compton, W.M.; Jones, C.M.; Einstein, E.B.; Volkow, N.D. Methamphetamine Use, Methamphetamine Use Disorder, and Associated Overdose Deaths Among US Adults. JAMA Psychiatry 2021, 78, 1329–1342. [Google Scholar] [CrossRef]
- Ellis, M.S.; Kasper, Z.A.; Cicero, T.J. Polysubstance use trends and variability among individuals with opioid use disorder in rural versus urban settings. Prev. Med. 2021, 152, 106729. [Google Scholar] [CrossRef]
- Compton, W.M.; Valentino, R.J.; DuPont, R.L. Polysubstance use in the U.S. opioid crisis. Mol. Psychiatry 2021, 26, 41–50. [Google Scholar] [CrossRef]
- WHO. Lexicon of Alcohol and Drug Terms; World Health Organization: Geneva, Switzerland, 1994. [Google Scholar]
- Vekaria, V.; Bose, B.; Murphy, S.M.; Avery, J.; Alexopoulos, G.; Pathak, J. Association of co-occurring opioid or other substance use disorders with increased healthcare utilization in patients with depression. Transl. Psychiatry 2021, 11, 265. [Google Scholar] [CrossRef]
- Tormohlen, K.N.; Mojtabai, R.; Seiwell, A.; McGinty, E.E.; Stuart, E.A.; Tobin, K.E.; Troiani, V. Co-Occurring Opioid Use and Depressive Disorders: Patient Characteristics and Co-Occurring Health Conditions. J. Dual Diagn. 2021, 17, 296–303. [Google Scholar] [CrossRef]
- Conway, K.P.; Compton, W.; Stinson, F.S.; Grant, B.F. Lifetime comorbidity of DSM-IV mood and anxiety disorders and specific drug use disorders: Results from the National Epidemiologic Survey on Alcohol and Related Conditions. J. Clin. Psychiatry 2006, 67, 247–257. [Google Scholar] [CrossRef]
- Meier, A.; Lambert-Harris, C.; McGovern, M.P.; Xie, H.; An, M.; McLeman, B. Co-occurring prescription opioid use problems and posttraumatic stress disorder symptom severity. Am. J. Drug Alcohol Abuse 2014, 40, 304–311. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Nwabueze, C.; Pan, Y.; Walter, S.M.; Su, B.; Xu, C.; Winstanley, E.L.; Wang, K. Polysubstance Use, Mood Disorders, and Chronic Conditions With Anxiety in Opioid Patients. West. J. Nurs. Res. 2021. [Google Scholar] [CrossRef] [PubMed]
- Chakravorty, S.; Vandrey, R.G.; He, S.; Stein, M.D. Sleep Management Among Patients with Substance Use Disorders. Med. Clin. N. Am. 2018, 102, 733–743. [Google Scholar] [CrossRef]
- Saunders, E.C.; Lambert-Harris, C.; McGovern, M.P.; Meier, A.; Xie, H. The Prevalence of Posttraumatic Stress Disorder Symptoms among Addiction Treatment Patients with Cocaine Use Disorders. J. Psychoact. Drugs 2015, 47, 42–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keen, C.; Kinner, S.A.; Young, J.T.; Jang, K.; Gan, W.; Samji, H.; Zhao, B.; Krausz, M.; Slaunwhite, A. Prevalence of co-occurring mental illness and substance use disorder and association with overdose: A linked data cohort study among residents of British Columbia, Canada. Addiction 2022, 117, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Keen, C.; Young, J.T.; Borschmann, R.; Kinner, S.A. Non-fatal drug overdose after release from prison: A prospective data linkage study. Drug Alcohol Depend. 2020, 206, 107707. [Google Scholar] [CrossRef]
- Hedegaard, H.; Curtin, S.C.; Warner, M. Suicide Mortality in the United States, 1999–2019. NCHS Data Brief 2020, 1–8. [Google Scholar] [CrossRef]
- Gicquelais, R.E.; Jannausch, M.; Bohnert, A.S.B.; Thomas, L.; Sen, S.; Fernandez, A.C. Links between suicidal intent, polysubstance use, and medical treatment after non-fatal opioid overdose. Drug Alcohol Depend. 2020, 212, 108041. [Google Scholar] [CrossRef]
- Bohnert, A.S.B.; Walton, M.A.; Cunningham, R.M.; Ilgen, M.A.; Barry, K.; Chermack, S.T.; Blow, F.C. Overdose and adverse drug event experiences among adult patients in the emergency department. Addict. Behav. 2018, 86, 66–72. [Google Scholar] [CrossRef]
- Connery, H.S.; Taghian, N.; Kim, J.; Griffin, M.; Rockett, I.R.H.; Weiss, R.D.; Kathryn McHugh, R. Suicidal motivations reported by opioid overdose survivors: A cross-sectional study of adults with opioid use disorder. Drug Alcohol Depend. 2019, 205, 107612. [Google Scholar] [CrossRef]
- Stover, A.N.; Rockett, I.R.H.; Smith, G.S.; LeMasters, T.; Scott, V.G.; Kelly, K.M.; Winstanley, E.L. Distinguishing clinical factors associated with unintentional overdose, suicidal ideation, and attempted suicide among opioid use disorder in-patients. J. Psychiatr. Res. 2022, 153, 245–253. [Google Scholar] [CrossRef]
- Bohnert, A.S.B.; Ilgen, M.A. Understanding Links among Opioid Use, Overdose, and Suicide. N. Engl. J. Med. 2019, 380, 71–79. [Google Scholar] [CrossRef]
- Abroms, M.; Sher, L. Dual Disorders and Suicide. J. Dual Diagn. 2016, 12, 148–149. [Google Scholar] [CrossRef]
- Ponizovsky, A.M.; Rosca, P.; Haklai, Z.; Goldberger, N. Trends in dual diagnosis of severe mental illness and substance use disorders, 1996–2010, Israel. Drug Alcohol Depend. 2015, 148, 203–208. [Google Scholar] [CrossRef]
- Szerman, N.; Lopez-Castroman, J.; Arias, F.; Morant, C.; Babin, F.; Mesias, B.; Basurte, I.; Vega, P.; Baca-Garcia, E. Dual diagnosis and suicide risk in a Spanish outpatient sample. Subst. Use Misuse 2012, 47, 383–389. [Google Scholar] [CrossRef]
- Trivedi, M.H.; Wisniewski, S.R.; Morris, D.W.; Fava, M.; Gollan, J.K.; Warden, D.; Nierenberg, A.A.; Gaynes, B.N.; Husain, M.M.; Luther, J.F.; et al. Concise Health Risk Tracking scale: A brief self-report and clinician rating of suicidal risk. J. Clin. Psychiatry 2011, 72, 757–764. [Google Scholar] [CrossRef] [Green Version]
- Posner, K.; Brown, G.K.; Stanley, B.; Brent, D.A.; Yershova, K.V.; Oquendo, M.A.; Currier, G.W.; Melvin, G.A.; Greenhill, L.; Shen, S.; et al. The Columbia-Suicide Severity Rating Scale: Initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am. J. Psychiatry 2011, 168, 1266–1277. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Villegas, A.C.; DuBois, C.M.; Celano, C.M.; Beale, E.E.; Mastromauro, C.A.; Stewart, J.G.; Auerbach, R.P.; Huffman, J.C.; Hoeppner, B.B. A longitudinal investigation of the Concise Health Risk Tracking Self-Report (CHRT-SR) in suicidal patients during and after hospitalization. Psychiatry Res. 2018, 262, 558–565. [Google Scholar] [CrossRef]
- Ostacher, M.J.; Nierenberg, A.A.; Rabideau, D.; Reilly-Harrington, N.A.; Sylvia, L.G.; Gold, A.K.; Shesler, L.W.; Ketter, T.A.; Bowden, C.L.; Calabrese, J.R.; et al. A clinical measure of suicidal ideation, suicidal behavior, and associated symptoms in bipolar disorder: Psychometric properties of the Concise Health Risk Tracking Self-Report (CHRT-SR). J. Psychiatr. Res. 2015, 71, 126–133. [Google Scholar] [CrossRef]
- Sanchez, K.; Killian, M.O.; Mayes, T.L.; Greer, T.L.; Trombello, J.M.; Lindblad, R.; Grannemann, B.D.; Carmody, T.J.; Rush, A.J.; Walker, R.; et al. A psychometric evaluation of the Concise Health Risk Tracking Self-Report (CHRT-SR)- a measure of suicidality-in patients with stimulant use disorder. J. Psychiatr. Res. 2018, 102, 65–71. [Google Scholar] [CrossRef]
- NIDA. About the CTN. Available online: https://nida.nih.gov/about-nida/organization/cctn/ctn/about-ctn (accessed on 20 April 2022).
- NIDA. Data Share Website: Home. Available online: https://datashare.nida.nih.gov/ (accessed on 20 May 2022).
- Trivedi, M.H.; Greer, T.L.; Rethorst, C.D.; Carmody, T.; Grannemann, B.D.; Walker, R.; Warden, D.; Shores-Wilson, K.; Stoutenberg, M.; Oden, N.; et al. Randomized Controlled Trial Comparing Exercise to Health Education for Stimulant Use Disorder: Results From the CTN-0037 STimulant Reduction Intervention Using Dosed Exercise (STRIDE) Study. J. Clin. Psychiatry 2017, 78, 1075–1082. [Google Scholar] [CrossRef]
- Metsch, L.R.; Feaster, D.J.; Gooden, L.; Matheson, T.; Stitzer, M.; Das, M.; Jain, M.K.; Rodriguez, A.E.; Armstrong, W.S.; Lucas, G.M.; et al. Effect of Patient Navigation With or Without Financial Incentives on Viral Suppression Among Hospitalized Patients With HIV Infection and Substance Use: A Randomized Clinical Trial. JAMA 2016, 316, 156–170. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.D.; Nunes, E.V., Jr.; Novo, P.; Bachrach, K.; Bailey, G.L.; Bhatt, S.; Farkas, S.; Fishman, M.; Gauthier, P.; Hodgkins, C.C.; et al. Comparative effectiveness of extended-release naltrexone versus buprenorphine-naloxone for opioid relapse prevention (X:BOT): A multicentre, open-label, randomised controlled trial. Lancet 2018, 391, 309–318. [Google Scholar] [CrossRef]
- Gray, K.M.; Sonne, S.C.; McClure, E.A.; Ghitza, U.E.; Matthews, A.G.; McRae-Clark, A.L.; Carroll, K.M.; Potter, J.S.; Wiest, K.; Mooney, L.J.; et al. A randomized placebo-controlled trial of N-acetylcysteine for cannabis use disorder in adults. Drug Alcohol Depend. 2017, 177, 249–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mooney, L.J.; Hillhouse, M.P.; Thomas, C.; Ang, A.; Sharma, G.; Terry, G.; Chang, L.; Walker, R.; Trivedi, M.; Croteau, D.; et al. Utilizing a Two-stage Design to Investigate the Safety and Potential Efficacy of Monthly Naltrexone Plus Once-daily Bupropion as a Treatment for Methamphetamine Use Disorder. J. Addict. Med. 2016, 10, 236–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Metsch, L.R.; Feaster, D.J.; Gooden, L.K.; Masson, C.; Perlman, D.C.; Jain, M.K.; Matheson, T.; Nelson, C.M.; Jacobs, P.; Tross, S.; et al. Care Facilitation Advances Movement Along the Hepatitis C Care Continuum for Persons With Human Immunodeficiency Virus, Hepatitis C, and Substance Use: A Randomized Clinical Trial (CTN-0064). Open Forum Infect. Dis. 2021, 8, ofab334. [Google Scholar] [CrossRef]
- Korthuis, P.T.; Cook, R.R.; Lum, P.J.; Waddell, E.N.; Tookes, H.; Vergara-Rodriguez, P.; Kunkel, L.E.; Lucas, G.M.; Rodriguez, A.E.; Bielavitz, S.; et al. HIV clinic-based extended-release naltrexone versus treatment as usual for people with HIV and opioid use disorder: A non-blinded, randomized non-inferiority trial. Addiction 2022, 117, 1961–1971. [Google Scholar] [CrossRef]
- Trivedi, M.H.; Walker, R.; Ling, W.; Dela Cruz, A.; Sharma, G.; Carmody, T.; Ghitza, U.E.; Wahle, A.; Kim, M.; Shores-Wilson, K.; et al. Bupropion and Naltrexone in Methamphetamine Use Disorder. N. Engl. J. Med. 2021, 384, 140–153. [Google Scholar] [CrossRef]
- NIDA. Protocol NIDA-CTN-0037: Stimulant Reduction Intervention Using Dosed Exercise (STRIDE). Available online: http://ctndisseminationlibrary.org/protocols/ctn0037.htm (accessed on 10 July 2022).
- NIDA. Protocol NIDA-CTN-0049: Project HOPE Hospital Visit as Oopportunity for Prevention and Engagement for HIV-Infected Drug Users. Available online: http://ctndisseminationlibrary.org/protocols/ctn0049.htm (accessed on 10 July 2022).
- NIDA. Protocol NIDA-CTN-0051: Extended-Release Naltrexone vs. Buprenorphone for Opioid Treatment (X:BOT). Available online: http://ctndisseminationlibrary.org/protocols/ctn0051.htm (accessed on 10 July 2022).
- NIDA. Protocol NIDA-CTN-0053: Achieving Cannabis Cessation- Evaluating N-Acetylcysteine Treatment (ACCENT). Available online: http://ctndisseminationlibrary.org/protocols/ctn0053.htm (accessed on 10 July 2022).
- NIDA. Protcol NIDA-CTN-0054: Accelerated Development of Additive Pharmacotherapy Treatment (ADAPT) for Methamphetamine Use Disorder. Available online: http://ctndisseminationlibrary.org/protocols/ctn0054.htm (accessed on 10 July 2022).
- NIDA. Protocol NIDA-CTN-0064: Linkage to Hepatitis C Virus (HCV) Care Among HIV/HCV Co-infected Substance Users. Available online: http://ctndisseminationlibrary.org/protocols/ctn0064.htm (accessed on 10 July 2022).
- NIDA. Protocol NIDA-CTN-0067: Comparing Treatments for HIV-Positive Opioid Users in an Integrated Care Effectiveness Study (CHOICES: Scale-Up. Available online: http://ctndisseminationlibrary.org/protocols/ctn0067.htm (accessed on 10 July 2022).
- NIDA. Protocol NIDA-CTN-0068: Accelerated Development of Additive Pharmacotherapy Treatment (ADAPT-2) for Methamphetamine Use Disorder. Available online: http://ctndisseminationlibrary.org/protocols/ctn0068.htm (accessed on 10 July 2022).
- Derogatis, L. Brief Symptom Inventory (BSI) 18: Administration, Scoring, and Procedures Manual, 3rd ed.; National Computer Systems: Minneapolis, MN, USA, 2000. [Google Scholar]
- McLellan, A.T.; Kushner, H.; Metzger, D.; Peters, R.; Smith, I.; Grissom, G.; Pettinati, H.; Argeriou, M. The Fifth Edition of the Addiction Severity Index. J. Subst. Abuse Treat. 1992, 9, 199–213. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Siegler, A.; Tuazon, E.; Bradley O’Brien, D.; Paone, D. Unintentional opioid overdose deaths in New York City, 2005–2010: A place-based approach to reduce risk. Int. J. Drug Policy 2014, 25, 569–574. [Google Scholar] [CrossRef]
- Riley, E.D.; Evans, J.L.; Hahn, J.A.; Briceno, A.; Davidson, P.J.; Lum, P.J.; Page, K. A Longitudinal Study of Multiple Drug Use and Overdose Among Young People Who Inject Drugs. Am. J. Public Health 2016, 106, 915–917. [Google Scholar] [CrossRef]
- Zedler, B.; Xie, L.; Wang, L.; Joyce, A.; Vick, C.; Brigham, J.; Kariburyo, F.; Baser, O.; Murrelle, L. Development of a Risk Index for Serious Prescription Opioid-Induced Respiratory Depression or Overdose in Veterans’ Health Administration Patients. Pain Med. 2015, 16, 1566–1579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Association, A.P. Diagnostic and Statistical Manual of Mental Disorders (DSM-5) Fifth Edition, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59 (Suppl. 20), 22–33. [Google Scholar] [PubMed]
- SAS Institute Inc. SAS® OnDemand for Academics: User’s Guide; SAS Institute Inc.: Cary, NC, USA, 2014. [Google Scholar]
- Esang, M.; Ahmed, S. A Closer Look at Substance Use and Suicide. Am. J. Psychiatry 2018, 13, 6–8. [Google Scholar] [CrossRef] [Green Version]
- Brandt, L.; Hu, M.; Liu, Y.; Castillo, F.; Odom, G.; Balise, R.; Feaster, D.; Nunes, E.; Luo, S. Risks of Overdose Events for Patients Undergoing Opioid Use Disorder Treatment; The College on Problems of Drug Dependence: Minneapolis, MN, USA, 2022. [Google Scholar]
- De La Garza, N.; Rush, A.J.; Killian, M.O.; Grannemann, B.D.; Carmody, T.J.; Trivedi, M.H. The Concise Health Risk Tracking Self-Report (CHRT-SR) assessment of suicidality in depressed outpatients: A psychometric evaluation. Depress. Anxiety 2019, 36, 313–320. [Google Scholar] [CrossRef]
- Mohamed, I.I.; Ahmad, H.E.K.; Hassaan, S.; Hassan, S. Assessment of anxiety and depression among substance use disorder patients: A case-control study. Middle East Curr. Psychiatry 2020, 27, 22. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Trial | Study Title | Study Type | Sample Size | Main Target Substance | Recruitment Setting | Intervention Period/Follow Up Period |
|---|---|---|---|---|---|---|
| CTN 0037 [32,40] | Stimulant Reduction Intervention Using Dosed Exercise (STRIDE) | 2-arm RCT | 302 | Stimulants (Cocaine and Methamphetamine) | Residential substance use treatment programs | 12 weeks/ 36 weeks |
| CTN 0049 [33,41] | Project HOPE: Hospital Visit as Opportunity for Prevention and Engagement for HIV-Infected Drug Users | 3-arm RCT | 801 * | Any substance | Inpatient, Hospitalized, enrolled at bedside | 26 weeks/ 52 weeks |
| CTN 0051 [34,42] | Extended-Release Naltrexone vs. Buprenorphine for Opioid Treatment (X:BOT) | 2-arm comparative effectiveness RCT | 570 | Opioids | Community based treatment programs | 24 weeks/ 36 weeks |
| CTN 0053 [35,43] | Achieving Cannabis Cessation: Evaluating N-Acetylcysteine Treatment (ACCENT) | Double-blind, placebo controlled 2-arm RCT | 302 | Cannabis | Multicenter, “treatment-seeking cannabis-dependent adults who submit positive urine cannabinoid testing during screening” | 12 weeks/ 16 weeks |
| CTN 0054 [36,44] | Accelerated Development of Additive Pharmacotherapy Treatment (ADAPT) | 2-stage pilot study | 49 | Methamphetamine | Outpatient, community treatment programs | 8 weeks/ 9 weeks |
| CTN 0064 [37,45] | Linkage to Hepatitis C Virus (HCV) Care among HIV/HCV Co-infected Substance Users | 2-arm RCT | 113 | Any substance | Follow up population of CTN 0049 | 26 weeks/ 52 weeks |
| CTN 0067 [38,46] | Comparing Treatments for HIV-Infected Opioid Users in an Integrated Care Effectiveness Study (CHOICES) Scale-Up | 2-arm RCT | 116 | Opioids | Primary Care | 24 weeks/ 24 weeks |
| CTN 0068 [39,47] | Accelerated Development of Additive Pharmacotherapy Treatment (ADAPT-2) for Methamphetamine Use Disorder | Double-blind, placebo controlled 2-arm RCT with adaptive design | 403 | Methamphetamine | Adults 18–65 were recruited from communities near the trial sites with the use of ads and direct referrals | 12 weeks/ 16 weeks |
| Overall (N = 2541) | Suicidal * (N = 122) | Non-Suicidal (N = 2418) | Mean CHRT-SR Score | Yes Overdose (N = 75) | No Overdose (N = 2466) | ||
|---|---|---|---|---|---|---|---|
| Mean (Standard Deviation) or N (%) | M (SD) or N (%) | M (SD) or N (%) | M (SD) | M (SD) or N (%) | M (SD) or N (%) | ||
| Age | 39.4 (11.4) | 42.4 (10.5) | 39.2 (11.5) | - | 39.1 (11.8) | 39.4 (11.4) | |
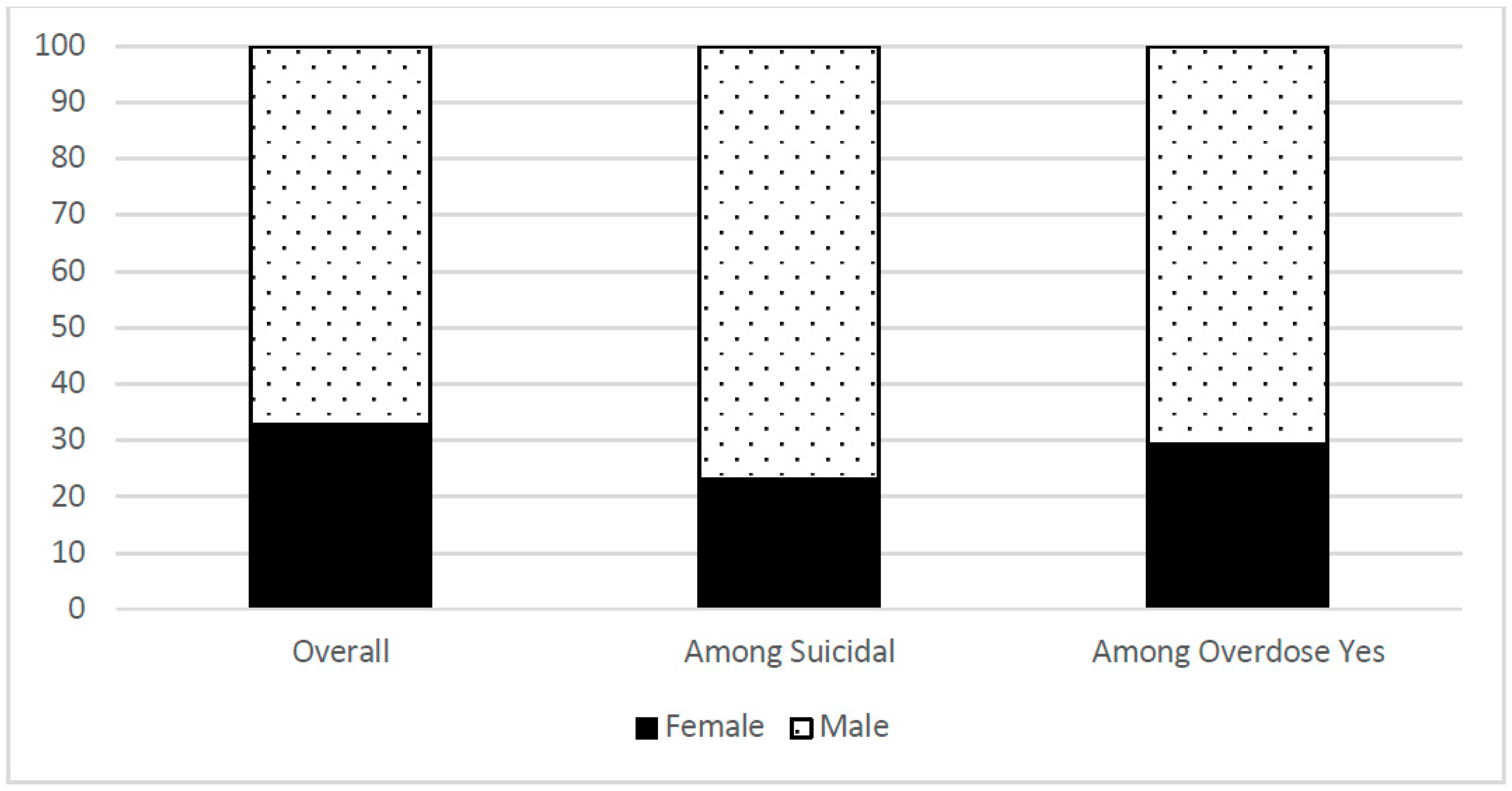
| Sex | Female | 829 (32.6%) | 28 (23.0%) | 800 (33.1%) | 23.8 (8.3) | 22 (29.3%) | 806 (32.7%) |
| Male | 1712 (67.4%) | 94 (77.0%) | 1618 (66.9%) | 23.9 (8.6) | 53 (70.7%) | 1659 (67.3%) | |
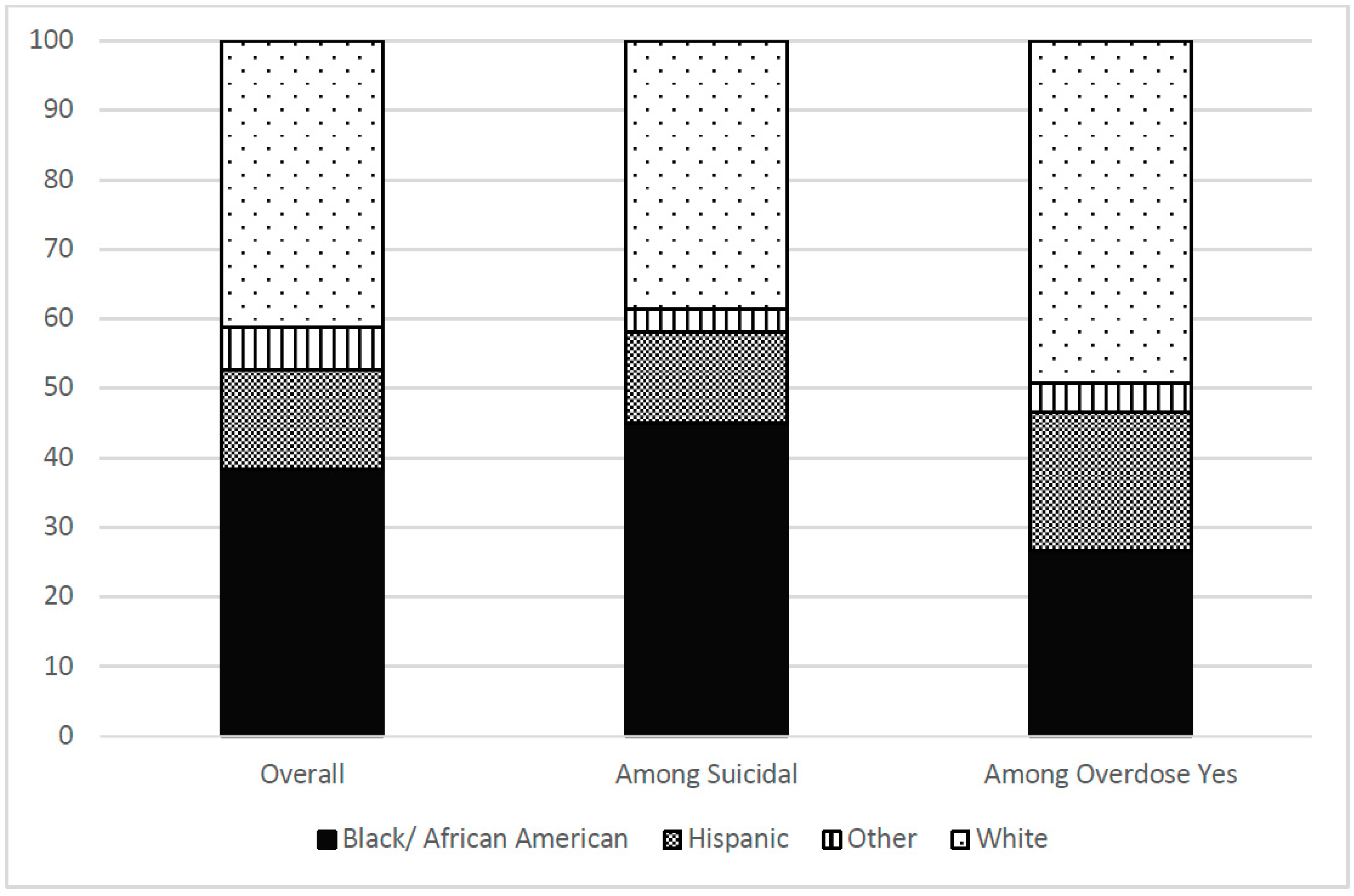
| Race/Ethnicity | Black/Af Am | 972 (38.3%) | 55 (45.1%) | 916 (37.9%) | 23.5 (8.6) | 20 (26.7%) | 951 (38.6%) |
| Hispanic | 366 (14.4%) | 16 (13.1%) | 350 (14.5%) | 24.0 (8.4) | 15 (20.0%) | 351 (14.2%) | |
| Other | 153 (6.0%) | 4 (3.3%) | 149 (6.2%) | 25.0 (8.0) | 3 (4.0%) | 150 (6.1%) | |
| White | 1050 (41.3%) | 47 (38.5%) | 1003 (41.5%) | 23.9 (8.6) | 37 (49.3%) | 1013 (41.1%) | |
| Treatment Arm Assignment | Experimental | 1310 (51.6%) | 64 (52.5%) | 1245 (51.5%) | 24.0 (8.5) | 45 (60.0%) | 1265 (51.3%) |
| Control | 1231 (48.5%) | 58 (47.5%) | 1173 (48.5%) | 23.7 (8.6) | 30 (40.0%) | 1200 (48.7%) | |
| Depressed | Yes | 1310 (51.6%) | 112 (91.8%) | 1197 (49.5%) | 27.0 (8.7) | 37 (49.3%) | 1273 (51.7%) |
| No | 1230 (48.4%) | 10 (8.2%) | 1220 (50.5%) | 20.5 (6.9) | 38 (50.7%) | 1191 (48.3%) | |
| History of Psychiatric Diagnosis | Yes | 1276 (50.2%) | 75 (61.5%) | 1200 (49.6%) | 25.2 (8.7) | 42 (56.0%) | 1233 (50.0%) |
| No | 1265 (49.8%) | 47 (38.5%) | 1218 (50.4%) | 22.5 (8.1) | 33 (44.0%) | 1232 (50.0%) | |
| Recent Alcohol Use | Yes | 1523 (60.0%) | 72 (60.0%) | 1450 (60.0%) | 23.5 (8.6) | 37 (49.3%) | 1485 (60.3%) |
| No | 1016 (40.0%) | 48 (40.0%) | 968 (40.0%) | 24.4 (8.4) | 38 (50.7%) | 978 (39.7%) | |
| Recent Benzo Use | Yes | 400 (15.8%) | 19 (15.8%) | 381 (15.8%) | 25.2 (8.6) | 18 (24.0%) | 382 (15.5%) |
| No | 2139 (84.2%) | 101 (84.2%) | 2037 (84.2%) | 23.6 (8.5) | 57 (76.0%) | 2081 (84.5%) | |
| Lifetime Heroin Use | Yes | 992 (39.0%) | 41 (33.6%) | 951 (39.3%) | 25.4 (8.0) | 53 (70.7%) | 939 (38.1%) |
| No | 1245 (49.0%) | 74 (60.7%) | 1170 (48.4%) | 23.8 (8.9) | 21 (28.0%) | 1223 (49.6%) | |
| Missing | 304 (12.0%) | 7 (5.7%) | 297 (12.3%) | 19.1 (7.0) | 1 (1.3%) | 303 (12.3%) | |
| Suicidal | Yes | 122 (4.8%) | 122 (4.8%) | - | 39.8 (7.9) | 6 (8.0%) | 116 (4.7%) |
| No | 2418 (95.2%) | - | 2418 (95.2%) | 23.1 (7.8) | 69 (92.0%) | 2348 (95.2%) | |
| Overdose | Yes | 75 (3.0%) | 6 (4.9%) | 69 (2.9%) | 25.8 (8.8) | 75 (3.0%) | - |
| No | 2465 (97.0%) | 116 (95.1%) | 2348 (97.1%) | 23.8 (8.5) | - | 2465 (97.1%) | |
| CHRT-SR Score | 23.9 (8.5) | 39.8 (7.8) | 23.1 (7.8) | - | 25.8 (8.8) | 23.8 (8.5) | |
| Odds Ratio | 95% Confidence Limits | p-Value | |||
|---|---|---|---|---|---|
| CHRT-SR Score | 1.02 | 1.00 | 1.04 | 0.03 | |
| Depressed | Yes | 0.76 | 0.32 | 1.83 | 0.54 |
| No | 0 | 0 | 0 | ||
| Recent Alcohol Use | Yes | 0.81 | 0.63 | 1.05 | 0.11 |
| No | 0 | 0 | 0 | ||
| Recent Benzo Use | Yes | 1.40 | 0.77 | 2.54 | 0.27 |
| No | 0 | 0 | 0 | ||
| Lifetime Heroin Use | Missing | 0.19 | 0.11 | 0.32 | <0.01 |
| Yes | 3.08 | 1.93 | 4.92 | <0.01 | |
| No | 0 | 0 | 0 | ||
| History of Psychiatric Diagnosis | Yes | 0.85 | 0.65 | 1.11 | 0.23 |
| No | 0 | 0 | 0 | ||
| Treatment Arm | Experimental | 1.48 | 0.81 | 2.70 | 0.20 |
| Control | 0 | 0 | 0 | . | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Horigian, V.E.; Schmidt, R.D.; Shmueli-Blumberg, D.; Hefner, K.; Feinberg, J.; Kondapaka, R.; Feaster, D.J.; Duan, R.; Gonzalez, S.; Davis, C.; et al. Suicidality as a Predictor of Overdose among Patients with Substance Use Disorders. J. Clin. Med. 2022, 11, 6400. https://doi.org/10.3390/jcm11216400
Horigian VE, Schmidt RD, Shmueli-Blumberg D, Hefner K, Feinberg J, Kondapaka R, Feaster DJ, Duan R, Gonzalez S, Davis C, et al. Suicidality as a Predictor of Overdose among Patients with Substance Use Disorders. Journal of Clinical Medicine. 2022; 11(21):6400. https://doi.org/10.3390/jcm11216400
Chicago/Turabian StyleHorigian, Viviana E., Renae D. Schmidt, Dikla Shmueli-Blumberg, Kathryn Hefner, Judith Feinberg, Radhika Kondapaka, Daniel J. Feaster, Rui Duan, Sophia Gonzalez, Carly Davis, and et al. 2022. "Suicidality as a Predictor of Overdose among Patients with Substance Use Disorders" Journal of Clinical Medicine 11, no. 21: 6400. https://doi.org/10.3390/jcm11216400
APA StyleHorigian, V. E., Schmidt, R. D., Shmueli-Blumberg, D., Hefner, K., Feinberg, J., Kondapaka, R., Feaster, D. J., Duan, R., Gonzalez, S., Davis, C., Marín-Navarrete, R., & Tross, S. (2022). Suicidality as a Predictor of Overdose among Patients with Substance Use Disorders. Journal of Clinical Medicine, 11(21), 6400. https://doi.org/10.3390/jcm11216400