
The Effect of Pharyngeal Surgery on Positive Airway Pressure Therapy in Obstructive Sleep Apnea: A Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
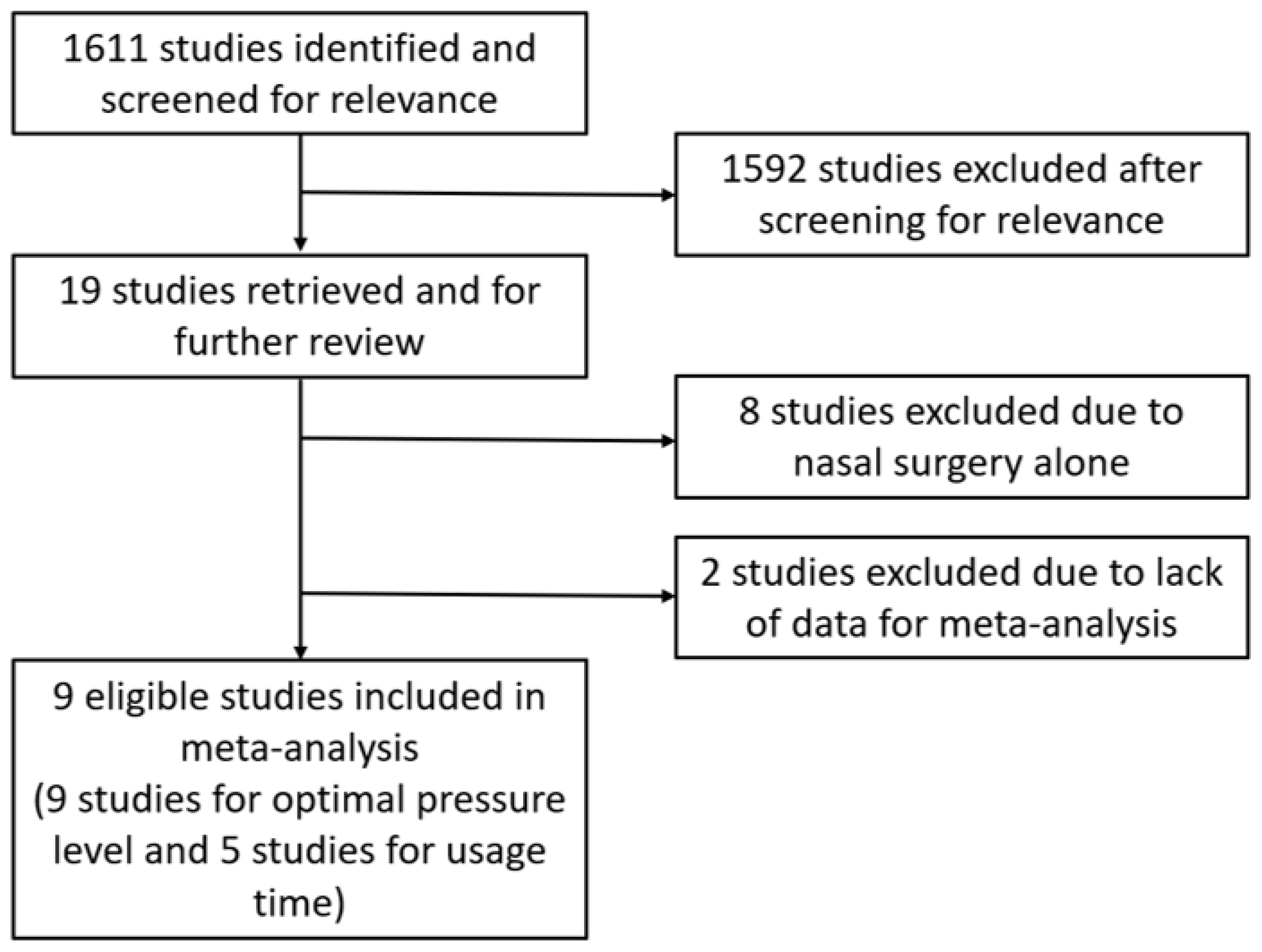
2.1. Search Strategy
2.2. Eligibility Criteria and Study Selection
2.3. Data Extraction
2.4. Quality Assessment
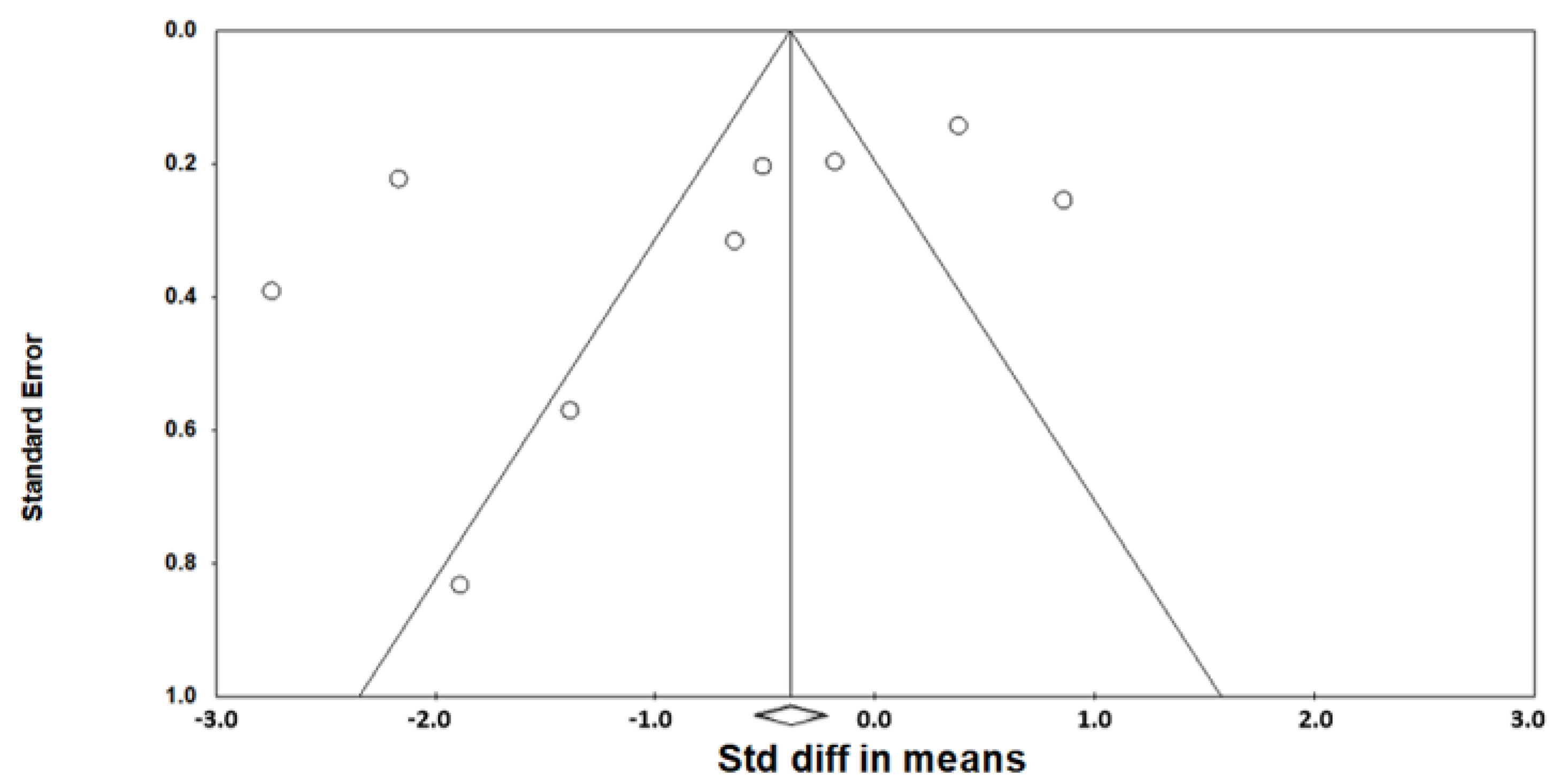
2.5. Statistical Analysis
3. Results
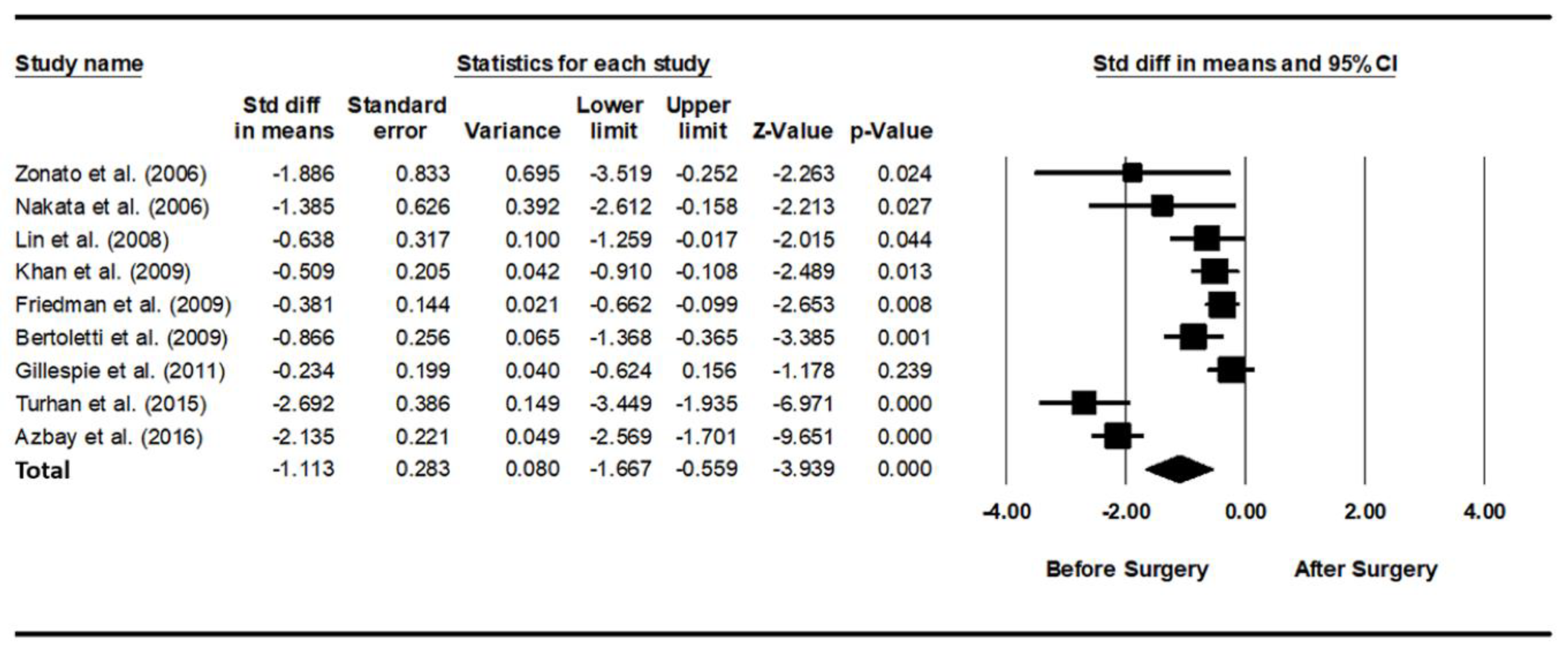
3.1. Optimal PAP Level before and after Pharyngeal OSA Surgery
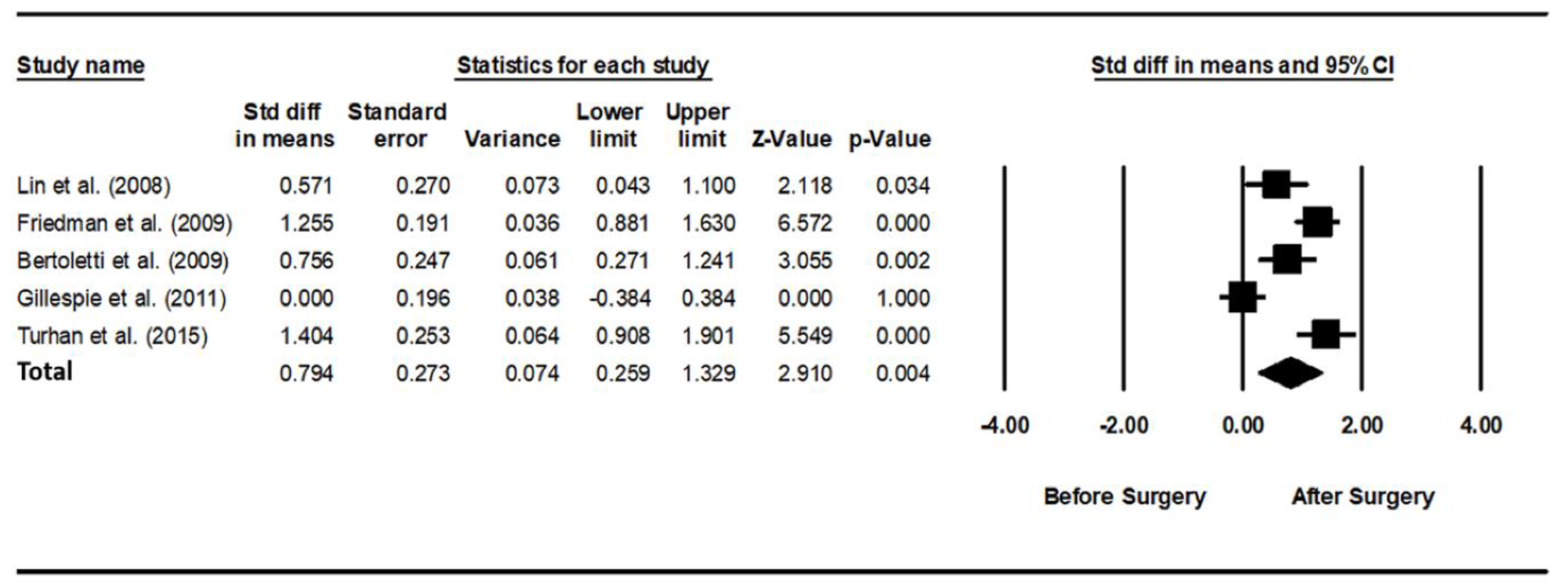
3.2. Usage Time of PAP before and after Pharyngeal OSA Surgery
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Guilleminault, C.; Tilkian, A.; Dement, W.C. The sleep apnea syndromes. Annu. Rev. Med. 1976, 27, 465–484. [Google Scholar] [CrossRef]
- Epstein, L.J.; Kristo, D.; Strollo, P.J., Jr.; Friedman, N.; Malhotra, A.; Patil, S.P.; Ramar, K.; Rogers, R.; Schwab, R.J.; Weaver, E.M.; et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J. Clin. Sleep Med. 2009, 5, 263–276. [Google Scholar] [PubMed]
- American Academy of Sleep Medicine. International Classification of Sleep Disorders; American Academy of Sleep Medicine: Darien, IL, USA, 2014. [Google Scholar]
- Gottlieb, D.J.; Punjabi, N.M. Diagnosis and Management of Obstructive Sleep Apnea: A Review. JAMA 2020, 323, 1389–1400. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.H. Treatments for adult obstructive sleep apnea. Sleep Med. Res. 2021, 12, 9–14. [Google Scholar] [CrossRef]
- Sullivan, C.E.; Issa, F.G.; Berthon-Jones, M.; Eves, L. Reversal of obstructive sleep apnoea by continuous positive airway pressure applied through the nares. Lancet 1981, 1, 862–865. [Google Scholar] [CrossRef]
- Kushida, C.A.; Littner, M.R.; Hirshkowitz, M.; Morgenthaler, T.I.; Alessi, C.A.; Bailey, D.; Boehlecke, B.; Brown, T.M.; Coleman, J., Jr.; Friedman, L.; et al. Practice parameters for the use of continuous and bilevel positive airway pressure devices to treat adult patients with sleep-related breathing disorders. Sleep 2006, 29, 375–380. [Google Scholar] [CrossRef] [PubMed]
- Ballester, E.; Badia, J.R.; Hernández, L.; Carrasco, E.; de Pablo, J.; Fornas, C.; Rodriguez-Roisin, R.; Montserrat, J.M. Evidence of the effectiveness of continuous positive airway pressure in the treatment of sleep apnea/hypopnea syndrome. Am. J. Respir. Crit. Care Med. 1999, 159, 495–501. [Google Scholar] [CrossRef]
- Jenkinson, C.; Davies, R.J.; Mullins, R.; Stradling, J.R. Comparison of therapeutic and subtherapeutic nasal continuous positive airway pressure for obstructive sleep apnoea: A randomised prospective parallel trial. Lancet 1999, 353, 2100–2105. [Google Scholar] [CrossRef]
- Becker, H.F.; Jerrentrup, A.; Ploch, T.; Grote, L.; Penzel, T.; Sullivan, C.E.; Peter, J.H. Effect of nasal continuous positive airway pressure treatment on blood pressure in patients with obstructive sleep apnea. Circulation 2003, 107, 68–73. [Google Scholar] [CrossRef]
- Kakkar, R.K.; Berry, R.B. Positive airway pressure treatment for obstructive sleep apnea. Chest 2007, 132, 1057–1072. [Google Scholar] [CrossRef]
- Liu, S.Y.; Riley, R.W.; Yu, M.S. Surgical Algorithm for Obstructive Sleep Apnea: An Update. Clin. Exp. Otorhinolaryngol. 2020, 13, 215–224. [Google Scholar] [PubMed]
- Smith, D.F.; Cohen, A.P.; Ishman, S.L. Surgical management of OSA in adults. Chest 2015, 147, 1681–1690. [Google Scholar] [CrossRef] [PubMed]
- Reilly, E.K.; Boon, M.S.; Vimawala, S.; Chitguppi, C.; Patel, J.; Murphy, K.; Doghramji, K.; Nyquist, G.G.; Rosen, M.R.; Rabinowitz, M.R.; et al. Tolerance of Continuous Positive Airway Pressure After Sinonasal Surgery. Laryngoscope 2021, 131, E1013–E1018. [Google Scholar] [PubMed]
- Chandrashekariah, R.; Shaman, Z.; Auckley, D. Impact of upper airway surgery on CPAP compliance in difficult-to-manage obstructive sleep apnea. Arch. Otolaryngol. Head Neck Surg. 2008, 134, 926–930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camacho, M.; Riaz, M.; Capasso, R.; Ruoff, C.M.; Guilleminault, C.; Kushida, C.A.; Certal, V. The effect of nasal surgery on continuous positive airway pressure device use and therapeutic treatment pressures: A systematic review and meta-analysis. Sleep 2015, 38, 279–286. [Google Scholar]
- Ayers, C.M.; Lohia, S.; Nguyen, S.A.; Gillespie, M.B. The Effect of Upper Airway Surgery on Continuous Positive Airway Pressure Levels and Adherence: A Systematic Review and Meta-Analysis. ORL J. Otorhinolaryngol. Relat. Spec. 2016, 78, 119–125. [Google Scholar] [CrossRef]
- Han, F.; Song, W.; Li, J.; Zhang, L.; Dong, X.; He, Q. Influence of UPPP surgery on tolerance to subsequent continuous positive airway pressure in patients with OSAHS. Sleep Breath. 2006, 10, 37–42. [Google Scholar]
- Mayer-Brix, J.; Müller-Marschhausen, U.; Becker, H.; Peter, J.H. How frequent are pathologic ENT findings in patients with obstructive sleep apnea syndrome? HNO 1989, 37, 511–516. [Google Scholar]
- Friedman, M.; Tanyeri, H.; Lim, J.W.; Landsberg, R.; Vaidyanathan, K.; Caldarelli, D. Effect of improved nasal breathing on obstructive sleep apnea. Otolaryngol. Head Neck Surg. 2000, 122, 71–74. [Google Scholar] [CrossRef]
- Dorn, M.; Pirsig, W.; Verse, T. Postoperative management following rhinosurgery interventions in severe obstructive sleep apnea. A pilot study. HNO 2001, 49, 642–645. [Google Scholar]
- Nowak, C.; Bourgin, P.; Portier, F.; Genty, E.; Escourrou, P.; Bobin, S. Nasal obstruction and compliance to nasal positive airway pressure. Ann. Otolaryngol. Chir. Cervicofac. 2003, 120, 161–166. [Google Scholar] [PubMed]
- Nakata, S.; Noda, A.; Yagi, H.; Yanagi, E.; Mimura, T.; Okada, T.; Misawa, H.; Nakashima, T. Nasal resistance for determinant factor of nasal surgery in CPAP failure patients with obstructive sleep apnea syndrome. Rhinology 2005, 43, 296–299. [Google Scholar] [PubMed]
- Sufioğlu, M.; Ozmen, O.A.; Kasapoglu, F.; Demir, U.L.; Ursavas, A.; Erişen, L.; Onart, S. The efficacy of nasal surgery in obstructive sleep apnea syndrome: A prospective clinical study. Eur. Arch. Otorhinolaryngol. 2012, 269, 487–494. [Google Scholar] [CrossRef] [PubMed]
- Poirier, J.; George, C.; Rotenberg, B. The effect of nasal surgery on nasal continuous positive airway pressure compliance. Laryngoscope 2014, 124, 317–319. [Google Scholar] [CrossRef]
- Zonato, A.I.; Bittencourt, L.R.; Martinho, F.L.; Gregório, L.C.; Tufik, S. Upper airway surgery: The effect on nasal continuous positive airway pressure titration on obstructive sleep apnea patients. Eur. Arch. Otorhinolaryngol. 2006, 263, 481–486. [Google Scholar] [CrossRef]
- Nakata, S.; Noda, A.; Yanagi, E.; Suzuki, K.; Yamamoto, H.; Nakashima, T. Tonsil size and body mass index are important factors for efficacy of simple tonsillectomy in obstructive sleep apnoea syndrome. Clin. Otolaryngol. 2006, 31, 41–45. [Google Scholar] [CrossRef]
- Lin, H.S.; Toma, R.; Glavin, C.; Toma, M.; Badr, M.S.; Rowley, J.A. Tolerance of positive airway pressure following site-specific surgery of upper airway. Open Sleep J. 2008, 1, 34–39. [Google Scholar]
- Khan, A.; Ramar, K.; Maddirala, S.; Friedman, O.; Pallanch, J.F.; Olson, E.J. Uvulopalatopharyngoplasty in the management of obstructive sleep apnea: The mayo clinic experience. Mayo Clin. Proc. 2009, 84, 795–800. [Google Scholar]
- Friedman, M.; Soans, R.; Joseph, N.; Kakodkar, S.; Friedman, J. The effect of multilevel upper airway surgery on continuous positive airway pressure therapy in obstructive sleep apnea/hypopnea syndrome. Laryngoscope 2009, 119, 193–196. [Google Scholar] [CrossRef]
- Bertoletti, F.; Indelicato, A.; Banfi, P.; Capolunghi, B. Sleep apnoea/hypopnoea syndrome: Combination therapy with the Pillar palatal implant technique and continuous positive airway pressure (CPAP). A preliminary report. B-ENT 2009, 5, 251–257. [Google Scholar]
- Gillespie, M.B.; Wylie, P.E.; Lee-Chiong, T.; Rapoport, D.M. Effect of palatal implants on continuous positive airway pressure and compliance. Otolaryngol. Head Neck Surg. 2011, 144, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Turhan, M.; Bostanci, A.; Akdag, M. The impact of modified tongue base suspension on CPAP levels in patients with severe OSA. Eur. Arch. Otorhinolaryngol. 2015, 272, 995–1000. [Google Scholar] [CrossRef] [PubMed]
- Azbay, S.; Bostanci, A.; Aysun, Y.; Turhan, M. The influence of multilevel upper airway surgery on CPAP tolerance in non-responders to obstructive sleep apnea surgery. Eur. Arch. Otorhinolaryngol. 2016, 273, 2813–2818. [Google Scholar] [CrossRef] [PubMed]
- Caples, S.M.; Rowley, J.A.; Prinsell, J.R.; Pallanch, J.F.; Elamin, M.B.; Katz, S.G.; Harwick, J.D. Surgical modifications of the upper airway for obstructive sleep apnea in adults: A systematic review and meta-analysis. Sleep 2010, 33, 1396–1407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, H.Y.; Wang, P.C.; Chen, Y.P.; Lee, L.A.; Fang, T.J.; Lin, H.C. Critical appraisal and meta-analysis of nasal surgery for obstructive sleep apnea. Am. J. Rhinol. Allergy 2011, 25, 45–49. [Google Scholar] [CrossRef]
- Wu, J.; Zhao, G.; Li, Y.; Zang, H.; Wang, T.; Wang, D.; Han, D. Apnea-hypopnea index decreased significantly after nasal surgery for obstructive sleep apnea: A meta-analysis. Medicine 2017, 96, e6008. [Google Scholar] [CrossRef]
- Millman, R.P.; Carlisle, C.C.; Rosenberg, C.; Kahn, D.; McRae, R.; Kramer, N.R. Simple predictors of uvulopalatopharyngoplasty outcome in the treatment of obstructive sleep apnea. Chest 2000, 118, 1025–1030. [Google Scholar] [CrossRef]
- Wilhelmsson, B.; Tegelberg, A.; Walker-Engström, M.L.; Ringqvist, M.; Andersson, L.; Krekmanov, L.; Ringqvist, I. A prospective randomized study of a dental appliance compared with uvulopalatopharyngoplasty in the treatment of obstructive sleep apnoea. Acta Otolaryngol. 1999, 119, 503–509. [Google Scholar]
- Choi, J.H.; Lee, J.Y.; Cha, J.; Kim, K.; Hong, S.N.; Lee, S.H. Predictive models of objective oropharyngeal OSA surgery outcomes: Success rate and AHI reduction ratio. PLoS ONE 2017, 12, e0185201. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| References | Year | Level of Evidence (Study Design) | Total No. of Subjects | Age (Years) | Sex (M:F) | BMI (kg/m²) | AHI (Events/Hour) | Surgical Procedures | PAP Therapy Related Outcomes Measures |
|---|---|---|---|---|---|---|---|---|---|
| Zonato et al. [26] | 2006 | Level IV (retrospective) | 17 | 49.0 ± 9.0 | 16:1 | 30.0 ± 4.0 | 38.0 ± 19.0 | Tonsillectomy ± nasal surgery | Optimal PAP level |
| Nakata et al. [27] | 2006 | Level II-2 (prospective) | 30 | 33.2 ± 6.8 | 28:2 | 30.7 ± 6.0 | 69.0 ± 28.4 | Tonsillectomy | Optimal PAP level |
| Lin et al. [28] | 2008 | Level IV (retrospective) | 16 | 34.1 ± 4.7 | 65.2 ± 49.2 | Site-specific upper airway surgery (UPPP, pillar palatoplasty, GA, HMA, and repose tongue suspension) | Optimal PAP level PAP usage time | ||
| Khan et al. [29] | 2009 | Level IV (retrospective) | 63 | 42.1 ± 13.9 | 51:12 | 34.9 ± 7.2 | 62.0 ± 35.4 | UPPP ± tongue base surgery ± nasal surgery | Optimal PAP level |
| Friedman et al. [30] | 2009 | Level IV (retrospective) | 52 | 43.1 ± 9.1 | 42:10 | 31.2 ± 5.0 | 63.2 ± 22.0 | Multi-level surgery (UPPP, RFBOT, and nasal surgery) | Optimal PAP level PAP usage time |
| Bertoletti et al. [31] | 2009 | Level II-2 (prospective) | 21 | 49.6 ± 11.2 | 16:5 | 31.4 ± 3.2 | 41.1 ± 5.8 | Pillar palatal implants | Optimal PAP level PAP usage time |
| Gillespie et al. [32] | 2011 | Level I (RCT) | 26 | 52.3 ± 10.3 | 22:4 | 34.7 ± 5.0 | 42.0 ± 21.0 | Pillar palatal implants | Optimal PAP level PAP usage time |
| Turhan et al. [33] | 2015 | Level II-2 (prospective) | 31 | 48 (31–66) | 27:4 | 31.0 ± 2.4 | 44.7 ± 17.1 | Modified tongue base suspension | Optimal PAP level PAP usage time |
| Azbay et al. [34] | 2016 | Level IV (retrospective) | 67 | 47.0 ± 9.8 | 59:8 | 31.6 ± 4.2 | 45.0 ± 19.8 | Modified UPPP + septoplasty ± modified tongue base suspension | Optimal PAP level |
| References | Year | Final No. of Patients | Preoperative Optimal Pressure (cmH2O) | Postoperative Optimal Pressure (cmH2O) | p Value | Final No. of Patients | Preoperative Usage Time (Hours/Night) | Postoperative Usage Time (Hours/Night) | p Value |
|---|---|---|---|---|---|---|---|---|---|
| Zonato et al. [26] | 2006 | 4 | 13.8 ± 1.5 | 10.4 ± 2.0 | <0.05 | ||||
| Nakata et al. [27] | 2006 | 5 | 13.6 ± 2.5 | 10.6 ± 1.3 | <0.05 | ||||
| Lin et al. [28] | 2008 | 12 | 11.5 ± 3.7 | 9.4 ± 2.6 | <0.05 | 16 | 4.1 ± 2.4 | 5.5 ± 2.5 | <0.05 |
| Khan et al. [29] | 2009 | 27 | 9.7 ± 3.0 | 8.3 ± 2.4 | <0.05 | ||||
| Friedman et al. [30] | 2009 | 52 | 10.6 ± 2.1 | 9.8 ± 2.1 | <0.05 | 49 | 0.02 ± 0.14 | 3.2 ± 2.6 | <0.001 |
| Bertoletti et al. [31] | 2009 | 21 | 11.2 ± 1.6 | 9.3 ± 2.5 | <0.05 | 21 | 5.7 ± 0.9 | 6.3 ± 0.6 | <0.05 |
| Gillespie et al. [32] | 2011 | 26 | 10.9 ± 2.7 | 10.3 ± 2.4 | NS | 26 | 6.0 ± 2.5 | 6.0 ± 2.4 | NS |
| Turhan et al. [33] | 2015 | 31 | 12.6 ± 1.6 | 8.0 ± 1.8 | <0.001 | 31 | 5.3 ± 0.8 | 6.5 ± 0.9 | <0.001 |
| Azbay et al. [34] | 2016 | 67 | 11.8 ± 1.4 | 9.0 ± 1.2 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwak, K.H.; Lee, Y.J.; Lee, J.Y.; Cho, J.H.; Choi, J.H. The Effect of Pharyngeal Surgery on Positive Airway Pressure Therapy in Obstructive Sleep Apnea: A Meta-Analysis. J. Clin. Med. 2022, 11, 6443. https://doi.org/10.3390/jcm11216443
Kwak KH, Lee YJ, Lee JY, Cho JH, Choi JH. The Effect of Pharyngeal Surgery on Positive Airway Pressure Therapy in Obstructive Sleep Apnea: A Meta-Analysis. Journal of Clinical Medicine. 2022; 11(21):6443. https://doi.org/10.3390/jcm11216443
Chicago/Turabian StyleKwak, Ki Hwan, Young Jeong Lee, Jae Yong Lee, Jae Hoon Cho, and Ji Ho Choi. 2022. "The Effect of Pharyngeal Surgery on Positive Airway Pressure Therapy in Obstructive Sleep Apnea: A Meta-Analysis" Journal of Clinical Medicine 11, no. 21: 6443. https://doi.org/10.3390/jcm11216443
APA StyleKwak, K. H., Lee, Y. J., Lee, J. Y., Cho, J. H., & Choi, J. H. (2022). The Effect of Pharyngeal Surgery on Positive Airway Pressure Therapy in Obstructive Sleep Apnea: A Meta-Analysis. Journal of Clinical Medicine, 11(21), 6443. https://doi.org/10.3390/jcm11216443