
Long-Term Follow-Up of Catheter Ablation for Premature Ventricular Complexes in the Modern Era: The Importance of Localization and Substrate

 ,
,  ,
,  , , ,
, , ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Procedural Details
2.3. Data Collection and Follow-Up Strategies
2.4. Variable Definitions and Study Outcomes
2.5. Statistical Analysis
3. Results
3.1. Patient Population
3.2. Procedural Data
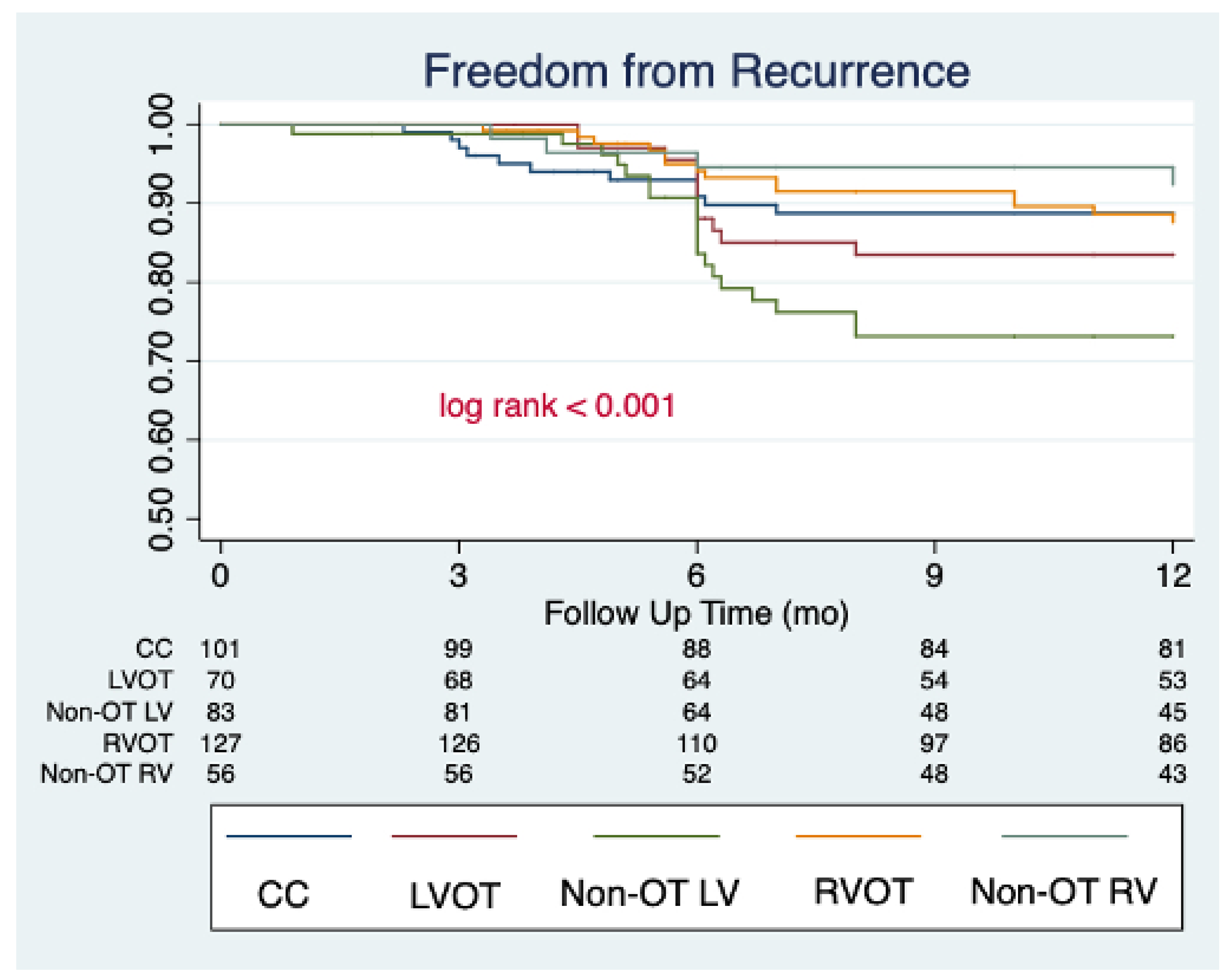
3.3. Study Outcomes and Outcome Predictors
4. Discussion
4.1. PVC Ablation and Clinical Outcomes
4.2. Ablation Index Use in PVC Ablation
4.3. Safety Endpoints
4.4. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baman, T.S.; Lange, D.C.; Ilg, K.J.; Gupta, S.K.; Liu, T.-Y.; Alguire, C.; Armstrong, W.; Good, E.; Chugh, A.; Jongnarangsin, K.; et al. Relationship between burden of premature ventricular complexes and left ventricular function. Heart Rhythm 2010, 7, 865–869. [Google Scholar] [CrossRef] [PubMed]
- Ling, Z.; Liu, Z.; Su, L.; Zipunnikov, V.; Wu, J.; Du, H.; Woo, K.; Chen, S.; Zhong, B.; Lan, X.; et al. Radiofrequency ablation versus antiarrhythmic medication for treatment of ventricular premature beats from the right ventricular outflow tract prospective randomized study. Circ. Arrhythmia Electrophysiol. 2014, 7, 237–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhong, L.; Lee, Y.-H.; Huang, X.-M.; Asirvatham, S.J.; Shen, W.-K.; Friedman, P.A.; Hodge, D.O.; Slusser, J.P.; Song, Z.-Y.; Packer, D.L.; et al. Relative efficacy of catheter ablation vs antiarrhythmic drugs in treating premature ventricular contractions: A single-center retrospective study. Heart Rhythm 2014, 11, 187–193. [Google Scholar] [CrossRef]
- Zang, M.; Zhang, T.; Mao, J.; Zhou, S.; He, B. Beneficial effects of catheter ablation of frequent premature ventricular complexes on left ventricular function. Heart 2014, 100, 787–793. [Google Scholar] [CrossRef] [PubMed]
- Latchamsetty, R.; Yokokawa, M.; Morady, F.; Kim, H.M.; Mathew, S.; Tilz, R.; Kuck, K.-H.; Nagashima, K.; Tedrow, U.; Stevenson, W.G.; et al. Multicenter Outcomes for Catheter Ablation of Idiopathic Premature Ventricular Complexes. JACC Clin. Electrophysiol. 2015, 1, 116–123. [Google Scholar] [CrossRef]
- Yamada, T.; Mcelderry, T.H.; Doppalapudi, H.; Okada, T.; Murakami, Y.; Yoshida, Y.; Yoshida, N.; Inden, Y.; Murohara, T.; Plumb, V.J.; et al. Idiopathic Ventricular Arrhythmias Originating From the Left Ventricular Summit Anatomic Concepts Relevant to Ablation. Circ. Arrhythmia Electrophysiol. 2010, 3, 616–623. [Google Scholar] [CrossRef] [Green Version]
- Van Herendael, H.; Zado, E.S.; Haqqani, H.; Tschabrunn, C.; Callans, D.J.; Frankel, D.S.; Lin, D.; Garcia, F.; Hutchinson, M.; Riley, M.; et al. Catheter ablation of ventricular fibrillation: Importance of left ventricular outflow tract and papillary muscle triggers. Heart Rhythm 2014, 11, 566–573. [Google Scholar] [CrossRef]
- Takemoto, M.; Yoshimura, H.; Ohba, Y.; Matsumoto, Y.; Yamamoto, U.; Mohri, M.; Yamamoto, H.; Origuchi, H. Radiofrequency catheter ablation of premature ventricular complexes from right ventricular outflow tract improves left ventricular dilation and clinical status in patients without structural heart disease. J. Am. Coll. Cardiol. 2005, 45, 1259–1265. [Google Scholar] [CrossRef] [Green Version]
- Penela, D.; Taxis, C.V.H.V.; Aguinaga, L.; Fernández-Armenta, J.; Mont, L.; Castel, M.A.; Heras, M.; Tolosana, J.M.; Sitges, M.; Ordóñez, A.; et al. Neurohormonal, structural, and functional recovery pattern after premature ventricular complex ablation is independent of structural heart disease status in patients with depressed left ventricular ejection fraction: A prospective multicenter study. J. Am. Coll. Cardiol. 2013, 62, 1195–1202. [Google Scholar] [CrossRef] [Green Version]
- Han, J.; Lee, J.Z.; Padmanabhan, D.; Naksuk, N.; Asirvatham, S.J.; Munger, T.M.; Killu, A.M.; Madhavan, M.; Xiao, P.; Zheng, L. Catheter ablation of premature ventricular contractions originating from periprosthetic aortic valve regions. J. Cardiovasc. Electrophysiol. 2021, 32, 400–408. [Google Scholar] [CrossRef]
- Voskoboinik, A.; Hadjis, A.; Alhede, C.; Im, S.I.; Park, H.; Moss, J.; Marcus, G.M.; Hsia, H.; Lee, B.; Tseng, Z.; et al. Predictors of adverse outcome in patients with frequent premature ventricular complexes: The ABC-VT risk score. Heart Rhythm 2020, 17, 1066–1074. [Google Scholar] [CrossRef] [PubMed]
- Im, S.; Voskoboinik, A.; Lee, B.; Higuchi, S.; Moss, J.D.; Hsia, H.; Tseng, Z.H.; Lee, R.; Marcus, G.M.; Vedantham, V.; et al. Predictors of long-term success after catheter ablation of premature ventricular complexes. J. Cardiovasc. Electrophysiol. 2021, 32, 2254–2261. [Google Scholar] [CrossRef] [PubMed]
- Good, E.; Desjardins, B.; Jongnarangsin, K.; Oral, H.; Chugh, A.; Ebinger, M.; Pelosi, F.; Morady, F.; Bogun, F. Ventricular arrhythmias originating from a papillary muscle in patients without prior infarction: A comparison with fascicular arrhythmias. Heart Rhythm 2008, 5, 1530–1537. [Google Scholar] [CrossRef] [PubMed]
- Lin, A.N.; Shirai, Y.; Liang, J.J.; Chen, S.; Kochar, A.; Hyman, M.C.; Santangeli, P.; Schaller, R.D.; Frankel, D.S.; Arkles, J.S.; et al. Strategies for Catheter Ablation of Left Ventricular Papillary Muscle Arrhythmias: An Institutional Experience. JACC Clin. Electrophysiol. 2020, 6, 1381–1392. [Google Scholar] [CrossRef] [PubMed]
- Enriquez, A.; Supple, G.E.; Marchlinski, F.E.; Garcia, F.C. How to map and ablate papillary muscle ventricular arrhythmias. Heart Rhythm 2017, 14, 1721–1728. [Google Scholar] [CrossRef]
- Romero, J.; Shivkumar, K.; Valderrabano, M.; Diaz, J.C.; Alviz, I.; Briceno, D.; Natale, A.; Di Biase, L. Modern mapping and ablation techniques to treat ventricular arrhythmias from the left ventricular summit and interventricular septum. Heart Rhythm 2020, 17, 1609–1620. [Google Scholar] [CrossRef]
- Obel, O.A.; d’Avila, A.; Neuzil, P.; Saad, E.B.; Ruskin, J.N.; Reddy, V.Y. Ablation of Left Ventricular Epicardial Outflow Tract Tachycardia From the Distal Great Cardiac Vein. J. Am. Coll. Cardiol. 2006, 48, 1813–1817. [Google Scholar] [CrossRef] [Green Version]
- El Kadri, M.; Yokokawa, M.; Labounty, T.; Mueller, G.; Crawford, T.; Good, E.; Jongnarangsin, K.; Chugh, A.; Ghanbari, H.; Latchamsetty, R.; et al. Effect of ablation of frequent premature ventricular complexes on left ventricular function in patients with nonischemic cardiomyopathy. Heart Rhythm 2015, 12, 706–713. [Google Scholar] [CrossRef]
- Edward, J.A.; Zipse, M.M.; Tompkins, C.; Varosy, P.D.; Sandhu, A.; Rosenberg, M.; Aleong, R.; Tzou, W.S.; Borne, R.T.; Sauer, W.H.; et al. Follow-Up After Catheter Ablation of Papillary Muscles and Valve Cusps. JACC Clin. Electrophysiol. 2019, 5, 1185–1196. [Google Scholar] [CrossRef]
- Castao, A.; Crawford, T.; Yamazaki, M.; Avula, U.M.R.; Kalifa, J. Coronary artery pathophysiology after radiofrequency catheter ablation: Review and perspectives. Heart Rhythm 2011, 8, 1975–1980. [Google Scholar] [CrossRef]
- Enriquez, A.; Baranchuk, A.; Briceno, D.; Saenz, L.; Garcia, F. How to use the 12-lead ECG to predict the site of origin of idiopathic ventricular arrhythmias. Heart Rhythm 2019, 16, 1538–1544. [Google Scholar] [CrossRef] [PubMed]
- Casella, M.; Gasperetti, A.; Gianni, C.; Zucchelli, G.; Notarstefano, P.; Al-Ahmad, A.; Burkhardt, J.D.; Soldati, E.; Della Rocca, D.; Catto, V.; et al. Ablation Index as a predictor of long-term efficacy in premature ventricular complex ablation: A regional target value analysis. Heart Rhythm 2019, 16, 888–895. [Google Scholar] [CrossRef] [PubMed]
- Gasperetti, A.; Sicuso, R.; Russo, A.D.; Zucchelli, G.; Saguner, A.M.; Notarstefano, P.; Soldati, E.; Bongiorni, M.G.; Della Rocca, D.G.; Mohanty, S.; et al. Prospective use of ablation index for the ablation of right ventricle outflow tract premature ventricular contractions: A proof of concept study. Europace 2021, 23, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Casella, M.; Russo, A.D.; Riva, S.; Catto, V.; Negro, G.; Sicuso, R.; Cellucci, S.; Gasperetti, A.; Zucchetti, M.; Ribatti, V.; et al. An ablation index operator-independent approach to improve efficacy in atrial fibrillation ablation at 24-month follow-up: A single center experience. J. Interv. Card. Electrophysiol. 2020, 57, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Kis, Z.; Pal, M.; Szabo, Z.; Kardos, A. Aortic Valve Rupture Due to Radiofrequency Ablation of Left Ventricular Outflow Tract Extrasystole. J. Cardiovasc. Electrophysiol. 2016, 27, 992. [Google Scholar] [CrossRef]
- Bianchini, L.; Zanchi, S.; Bordignon, S.; Tohoku, S.; Chen, S.; Bologna, F.; Schmidt, B.; Chun, K.J. EP Laboratory Nightmare: Catheter Ablation of Malignant Premature Ventricular Complex Complicated by Left Main Injury. JACC Case Rep. 2020, 2, 2331–2335. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Study Population (n = 437) | |
|---|---|
| Age (years), median [IQR] | 51 [36–62] |
| Male, n (%) | 286 (65.5) |
| Diabetes, n (%) | 42 (26.9) |
| HF, n (%) | 26 (6.0) |
| Hypertension, n (%) | 87 (19.9) |
| CKD, n (%) | 10 (2.9) |
| AF, n (%) | 23 (5.3) |
| Sport practice, n (%) | 57 (13.0) |
| LVEF (%), mean ± s.d. | 54.1 ± 9.9 |
| Structural heart disease, n (%) | 109 (24.9) |
| PVC localization | |
| CC, n (%) | 101 (23.1) |
| LVOT, n (%) | 70 (16.0) |
| Non-OT LV, n (%) | 83 (19.0) |
| RVOT, n (%) | 127 (29.1) |
| Non-OT RV, n (%) | 56 (12.8) |
| PVC QRS length, median [IQR] | 148 [136–157] |
| PVC coupling, median [IQR] | 478 [427–538] |
| Arrhythmic burden | |
| 24 h PVC burden %, median [IQR] | 20.1 [11.6–34.5] |
| N of Couplets, median [IQR] | 377 [128–668] |
| N of Triplets, median [IQR] | 57 [24–92] |
| Palpitations, n (%) | 274 (62.7) |
| Pharmacological therapy | |
| Beta-blockers, n (%) | 216 (49.4) |
| Class Ic, n (%) | 140 (32.0) |
| Class III, n (%) | 110 (25.2) |
| Overall (n = 437) | CC (n = 101) | LVOT (n = 70) | Non-OT LV (n = 83) | RVOT (n = 127) | Non-OT RV (n = 56) | p Value | |
|---|---|---|---|---|---|---|---|
| Procedure time (min), mean ± s.d. | 118.9 ± 45.5 | 107.5 ± 42.0 | 124.7 ± 55.0 | 129.1 ± 44.3 | 117.6 ± 41.9 | 120.0 ± 48.1 | 0.043 |
| Fluoroscopic time (min), median [IQR] | 30 [20–35] | 25 [20–30] | 28 [15–40] | 30 [25–45] | 30 [20–35] | 20 [15–35] | 0.002 |
| Radiofrequency time (s), median [IQR] | 317 [180–570] | 279 [180–600] | 345 [179–575] | 378 [200–721] | 300 [188–515] | 280 [176–580] | 0.573 |
| Power (W), mean ± s.d. | 42.1 ± 10.6 | 46.9 ± 9.9 | 49.2 ± 8.0 | 43.8 ± 9.9 | 35.2 ± 8.4 | 37.3 ± 9.4 | <0.001 |
| Ablation-index-guided, n (%) | 206 (47.1) | 51 (50.5) | 21 (30.0) | 37 (44.6) | 77 (60.6) | 20 (35.7) | <0.001 |
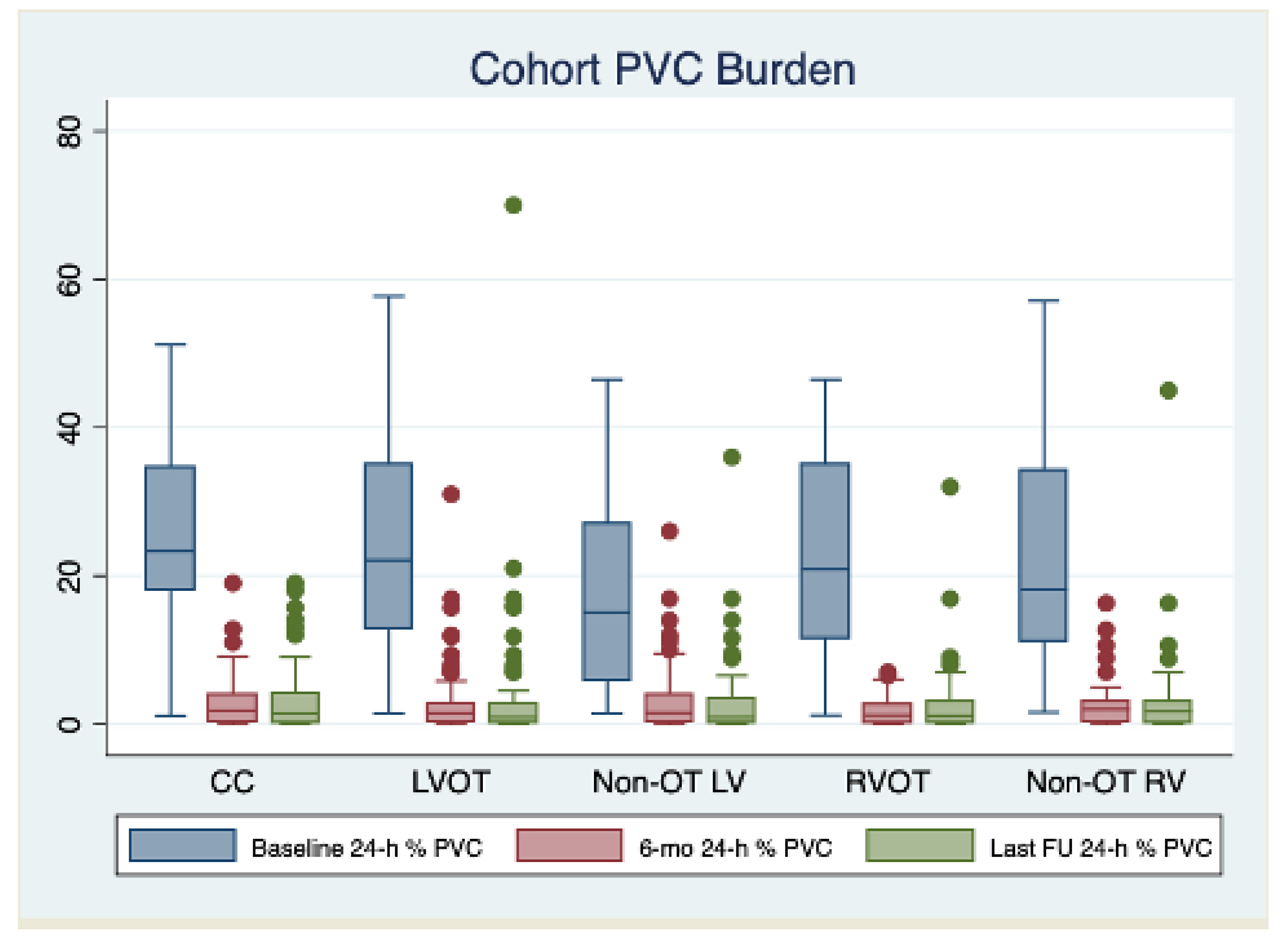
| Baseline | 6-mo F.U. | Last F.U. | |||||
|---|---|---|---|---|---|---|---|
| Burden % Median [IQR] | Burden % Median [IQR] | p | Procedure Success (%) | Burden % Median [IQR] | p | Procedure Success (%) | |
| Overall Cohort (n = 437) | 20.1 [11.6–34.5] | 1.5 [0.3–3.0] | <0.001 | 372 (85.1) | 1.1 [0.1–3.1] | 0.402 | 359 (82.1) |
| CC (n = 101) | 23.3 [18.0 –34.7] | 1.8 [0.4–4.0] | <0.001 | 89 (88.1) | 1.8 [0.3–4.0] | 0.167 | 84 (83.2) |
| LVOT (n = 70) | 22.1 [12.8–34.9] | 1.5 [0.3–2.8] | <0.001 | 57 (81.4) | 1.4 [0.2–2.6] | 0.330 | 56 (80.0) |
| Non-OT LV (n = 83) | 15.1 [5.8–26.9] | 1.5 [0.3–4.0] | <0.001 | 58 (70.0) | 1.6 [0.3–3.8] | 0.403 | 57 (68.7) |
| RVOT (n = 127) | 20.9 [11.6–34.9] | 1.2 [0.2–2.6] | <0.001 | 116 (91.3) | 1.2 [0.3–2.6] | 0.108 | 112 (88.2) |
| Non-OT RV (n = 56) | 18.2 [11.2–34.2] | 2.0 [0.4–2.9] | <0.001 | 52 (92.9) | 2.1 [0.4–2.9] | 0.345 | 50 (89.3) |
| HR [IQR] | p | aHR [IQR] | p | |
|---|---|---|---|---|
| Sex | 0.79 [0.50–1.25] | 0.319 | ||
| Age (/year) | 1.01 [0.98–1.02] | 0.628 | ||
| Sport | 0.63 [0.29–1.37] | 0.244 | ||
| HF | 0.95 [0.70–1.29] | 0.739 | ||
| LVEF (/%) | 1.01 [0.97–1.03] | 0.872 | ||
| Structural heart disease | 2.15 [1.37–3.38] | <0.001 | 1.96 [1.22–3.14] | 0.005 |
| AAD use during follow-up | 1.12 [0.67–1.87] | 0.656 | ||
| PVC burden | 0.96 [0.94–0.97] | <0.001 | 0.96 [0.95–0.98] | <0.001 |
| PVC QRS length (/ms) | 0.98 [0.97–1.01] | 0.118 | ||
| PVC coupling (/ms) | 0.99 [0.99–1.01] | 0.283 | ||
| CC origin | 0.85 [0.50–1.46] | 0.557 | ||
| LVOT origin | 1.06 [0.60–1.90] | 0.830 | ||
| Non-OT LV origin | 2.60 [1.62–4.17] | <0.001 | 1.77 [1.07–2.93] | 0.027 |
| Non-OT RV origin | 0.61 [0.35–1.07] | 0.084 | ||
| RVOT origin | 0.51 [0.22–1.17] | 0.112 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gulletta, S.; Gasperetti, A.; Schiavone, M.; Paglino, G.; Vergara, P.; Compagnucci, P.; Bisceglia, C.; Cireddu, M.; Fierro, N.; D’Angelo, G.; et al. Long-Term Follow-Up of Catheter Ablation for Premature Ventricular Complexes in the Modern Era: The Importance of Localization and Substrate. J. Clin. Med. 2022, 11, 6583. https://doi.org/10.3390/jcm11216583
Gulletta S, Gasperetti A, Schiavone M, Paglino G, Vergara P, Compagnucci P, Bisceglia C, Cireddu M, Fierro N, D’Angelo G, et al. Long-Term Follow-Up of Catheter Ablation for Premature Ventricular Complexes in the Modern Era: The Importance of Localization and Substrate. Journal of Clinical Medicine. 2022; 11(21):6583. https://doi.org/10.3390/jcm11216583
Chicago/Turabian StyleGulletta, Simone, Alessio Gasperetti, Marco Schiavone, Gabriele Paglino, Pasquale Vergara, Paolo Compagnucci, Caterina Bisceglia, Manuela Cireddu, Nicolai Fierro, Giuseppe D’Angelo, and et al. 2022. "Long-Term Follow-Up of Catheter Ablation for Premature Ventricular Complexes in the Modern Era: The Importance of Localization and Substrate" Journal of Clinical Medicine 11, no. 21: 6583. https://doi.org/10.3390/jcm11216583
APA StyleGulletta, S., Gasperetti, A., Schiavone, M., Paglino, G., Vergara, P., Compagnucci, P., Bisceglia, C., Cireddu, M., Fierro, N., D’Angelo, G., Sala, S., Rampa, L., Casella, M., Mazzone, P., Dello Russo, A., Forleo, G. B., & Della Bella, P. (2022). Long-Term Follow-Up of Catheter Ablation for Premature Ventricular Complexes in the Modern Era: The Importance of Localization and Substrate. Journal of Clinical Medicine, 11(21), 6583. https://doi.org/10.3390/jcm11216583