
Improvement of Mucosal Lesion Diagnosis with Machine Learning Based on Medical and Semiological Data: An Observational Study

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Selection Criteria
2.2. Data Collection and Annotation
2.3. Model Development and Data Analysis
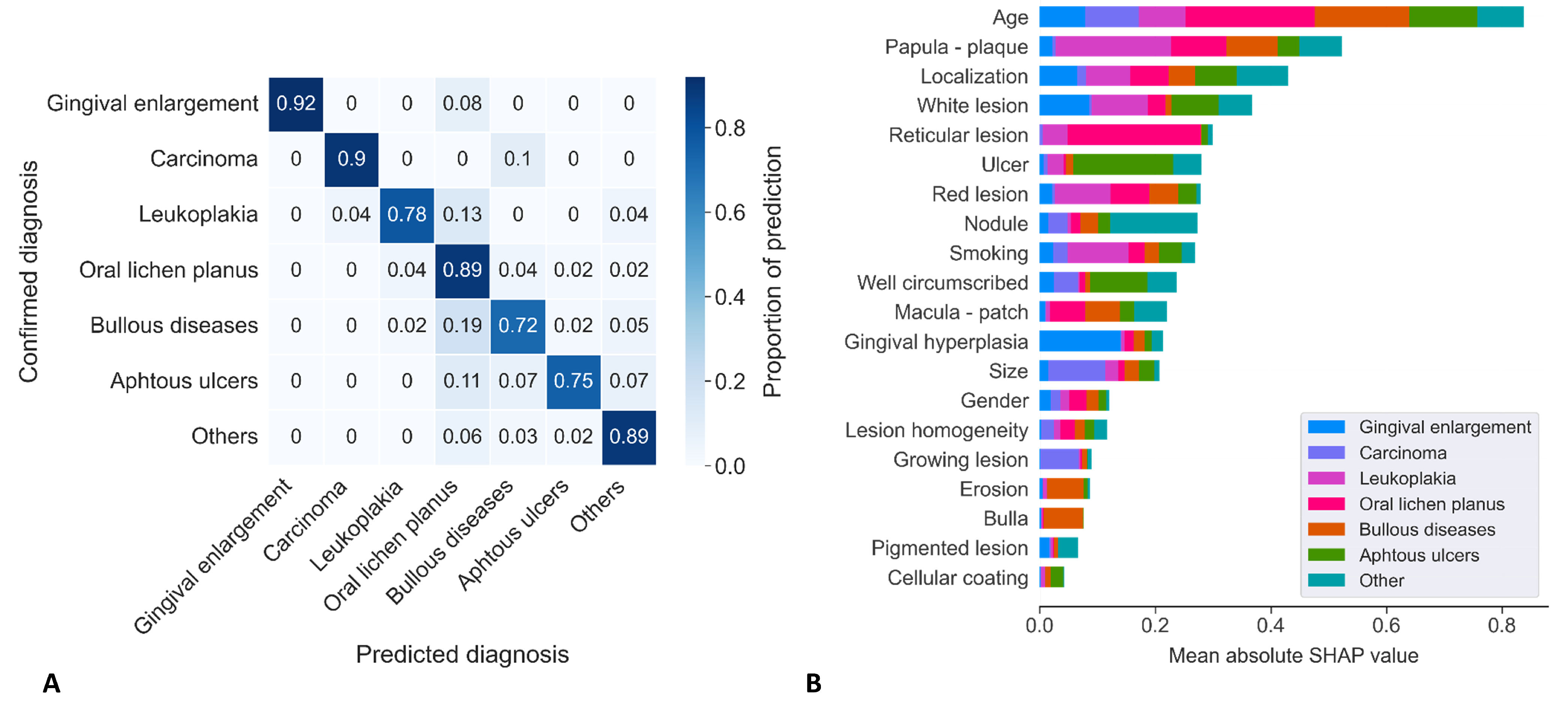
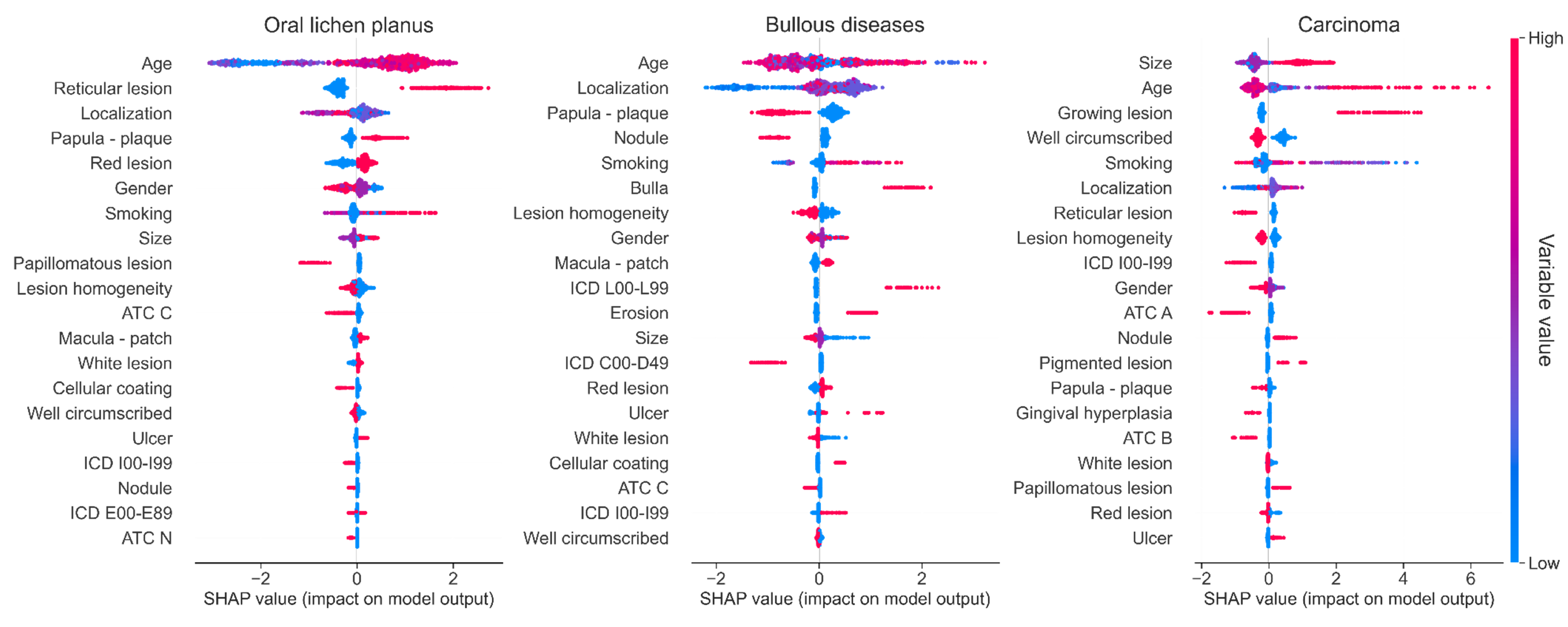
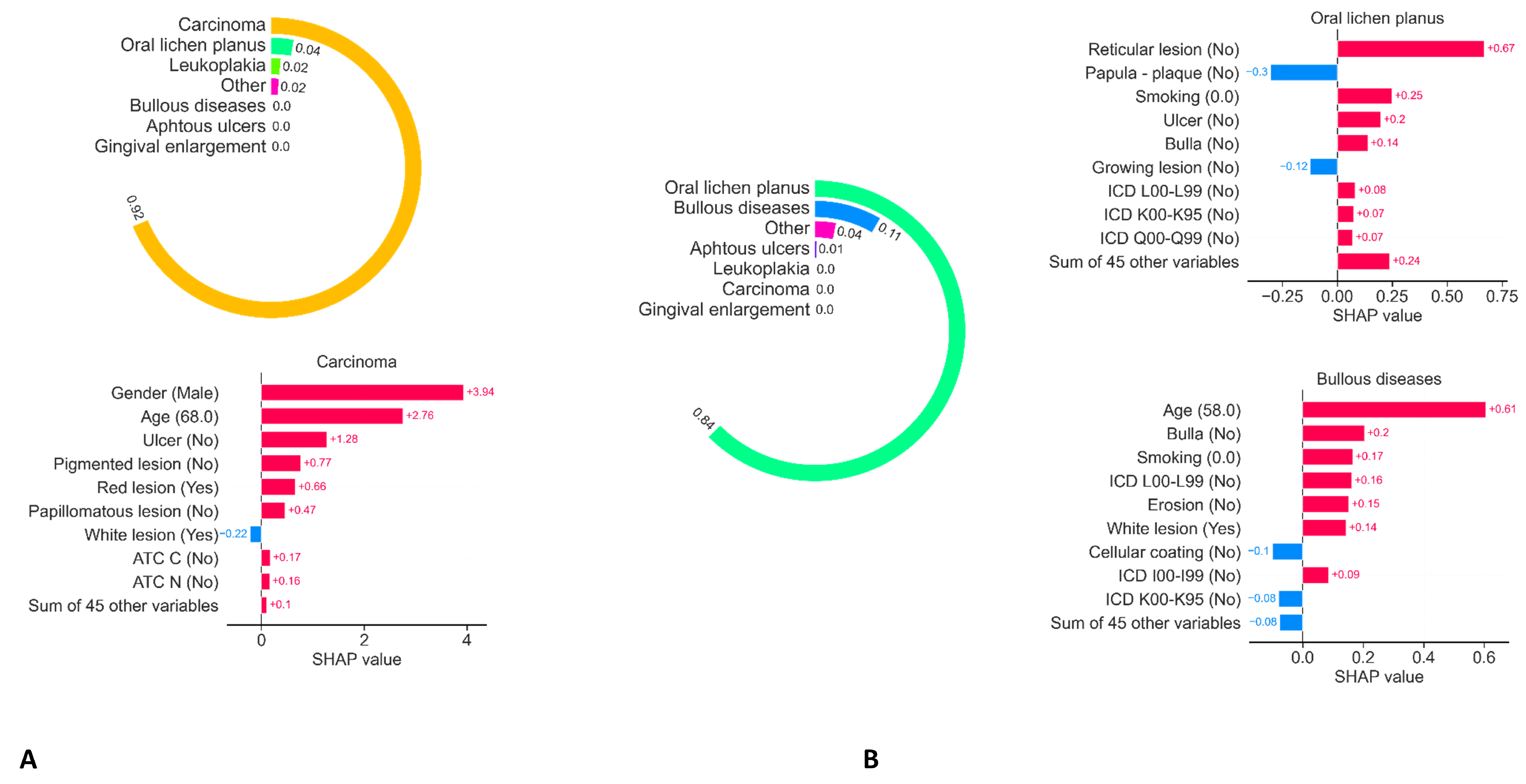
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AI | Artificial intelligence |
| ML | Machine learning |
| CNN | Convolutional neural network |
| DL | Deep learning |
| ICD | International classification of diseases |
| ATC | Anatomical therapeutic chemical classification system |
| CNIL | Commission for informatics and liberties |
| LR | Logistic regression |
| KNN | K-nearest neighbors |
| DTR | Decision tree regressor |
| MLP | Multilayer perceptron |
| TNR | True negative rate |
| TPR | True positive rate |
| PPV | Predictive positive value |
| PNV | Predictive negative value |
| ROC | Receiver Operator Characteristic |
| AUC | Area under curve |
References
- Hogarty, D.T.; Su, J.C.; Phan, K.; Attia, M.; Hossny, M.; Nahavandi, S.; Lenane, P.; Moloney, F.J.; Yazdabadi, A. Artificial Intelligence in Dermatology—Where We Are and the Way to the Future: A Review. Am. J. Clin. Dermatol. 2019, 21, 41–47. [Google Scholar] [CrossRef]
- Olsen, T.G.; Jackson, B.H.; Feeser, T.A.; Kent, M.N.; Moad, J.C.; Krishnamurthy, S.; Lunsford, D.D.; Soans, R.E. Diagnostic Performance of Deep Learning Algorithms Applied to Three Common Diagnoses in Dermatopathology. J. Pathol. Inform. 2018, 9, 32. [Google Scholar] [CrossRef] [PubMed]
- Zahia, S.; Zapirain, M.B.G.; Sevillano, X.; González, A.; Kim, P.J.; Elmaghraby, A. Pressure injury image analysis with machine learning techniques: A systematic review on previous and possible future methods. Artif. Intell. Med. 2020, 102, 101742. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Chen, H.; Weng, L.; Shao, J.; Lin, J. Automatic detection of oral cancer in smartphone-based images using deep learning for early diagnosis. J. Biomed. Opt. 2021, 26, 086007. [Google Scholar] [CrossRef]
- Day, G.R.; Barbour, R.H. Automated skin lesion screening—A new approach. Melanoma Res. 2001, 11, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Han, S.S.; Lim, W.; Kim, M.S.; Park, I.; Park, G.H.; Chang, S.E. Interpretation of the Outputs of a Deep Learning Model Trained with a Skin Cancer Dataset. J. Investig. Dermatol. 2018, 138, 2275–2277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burki, T.K. Machine learning model in melanoma. Lancet. Oncol. 2018, 19, e340. [Google Scholar] [CrossRef]
- Alkhadar, H.; Macluskey, M.; White, S.; Ellis, I.; Gardner, A. Comparison of machine learning algorithms for the prediction of five-year survival in oral squamous cell carcinoma. J. Oral Pathol. Med. 2021, 50, 378–384. [Google Scholar] [CrossRef]
- Thomsen, K.; Iversen, L.; Titlestad, T.L.; Winther, O. Systematic review of machine learning for diagnosis and prognosis in dermatology. J. Dermatol. Treat. 2020, 31, 496–510. [Google Scholar] [CrossRef]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef]
- Brinker, T.J.; Hekler, A.; Enk, A.H.; Berking, C.; Haferkamp, S.; Hauschild, A.; Weichenthal, M.; Klode, J.; Schadendorf, D.; Holland-Letz, T.; et al. Deep neural networks are superior to dermatologists in melanoma image classification. Eur. J. Cancer 2019, 119, 11–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amann, J.; Blasimme, A.; Vayena, E.; Frey, D.; Madai, V.I.; Precise4Q Consortium. Explainability for artificial intelligence in healthcare: A multidisciplinary perspective. BMC Med. Inform. Decis. Mak. 2020, 20, 310. [Google Scholar] [CrossRef]
- Diprose, W.K.; Buist, N.; Hua, N.; Thurier, Q.; Shand, G.; Robinson, R. Physician understanding, explainability, and trust in a hypothetical machine learning risk calculator. J. Am. Med. Inform. Assoc. JAMIA 2020, 27, 592–600. [Google Scholar] [CrossRef] [PubMed]
- Adeoye, J.; Tan, J.Y.; Choi, S.W.; Thomson, P. Prediction models applying machine learning to oral cavity cancer outcomes: A systematic review. Int. J. Med. Inform. 2021, 154, 104557. [Google Scholar] [CrossRef]
- Idrees, M.; Farah, C.S.; Shearston, K.; Kujan, O. A machine-learning algorithm for the reliable identification of oral lichen planus. J. Oral Pathol. Med. 2021, 50, 946–953. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Chu, C.S.; Lee, N.P.; Adeoye, J.; Thomson, P.; Choi, S.W. Machine learning and treatment outcome prediction for oral cancer. J. Oral Pathol. Med. 2020, 49, 977–985. [Google Scholar] [CrossRef]
- Ilhan, B.; Lin, K.; Guneri, P.; Wilder-Smith, P. Improving Oral Cancer Outcomes with Imaging and Artificial Intelligence. J. Dent. Res. 2020, 99, 241–248. [Google Scholar] [CrossRef]
- Pan, X.; Zhang, T.; Yang, Q.; Yang, D.; Rwigema, J.C.; Qi, X.S. Survival prediction for oral tongue cancer patients via probabilistic genetic algorithm optimized neural network models. Br. J. Radiol. 2020, 93, 20190825. [Google Scholar] [CrossRef]
- Jeyaraj, P.R.; Samuel Nadar, E.R. Computer-assisted medical image classification for early diagnosis of oral cancer employing deep learning algorithm. J. Cancer Res. Clin. Oncol. 2019, 145, 829–837. [Google Scholar] [CrossRef]
- Howard, F.M.; Kochanny, S.; Koshy, M.; Spiotto, M.; Pearson, A.T. Machine Learning-Guided Adjuvant Treatment of Head and Neck Cancer. JAMA Netw. Open 2020, 3, e2025881. [Google Scholar] [CrossRef] [PubMed]
- Gorphe, P.; Jannin, C. Regulatory aspects of prospective and retrospective clinical research in France in 2018. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2019, 136, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Buuren, S.V.; Groothuis-Oudshoorn, K. Mice: Multivariate Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef] [Green Version]
- Lundberg, S.; Lee, S.I. A Unified Approach to Interpreting Model Predictions. arXiv 2017, arXiv:1705.07874. [Google Scholar]
- Doumard, E.; Aligon, J.; Escriva, E.; Excoffier, J.; Monsarrat, P.; Soulé-Dupuy, C. A Comparative Study of Additive Local Explanation Methods based on Feature Influences. In Proceedings of the 24th International Workshop on Design, Optimization, Languages and Analytical Processing of Big Data (DOLAP) Co-Located with the 25th International Conference on Extending Database Technology and the 25th International Conference on Database Theory (EDBT/ICDT 2022), Edinburgh, UK, 29 March 2022; Stefanidis, K., Golab, L., Eds.; Volume 3130, pp. 31–40. [Google Scholar]
- Abati, S.; Bramati, C.; Bondi, S.; Lissoni, A.; Trimarchi, M. Oral Cancer and Precancer: A Narrative Review on the Relevance of Early Diagnosis. Int. J. Environ. Res. Public Health 2020, 17, 9160. [Google Scholar] [CrossRef] [PubMed]
- Seoane, J.; Alvarez-Novoa, P.; Gomez, I.; Takkouche, B.; Diz, P.; Warnakulasiruya, S.; Seoane-Romero, J.M.; Varela-Centelles, P. Early oral cancer diagnosis: The Aarhus statement perspective. A systematic review and meta-analysis. Head Neck 2016, 38 (Suppl. 1), 2182–2189. [Google Scholar] [CrossRef]
- Heelan, K.; McKenna, D. A survey of oral medicine education, training and practice among dermatologists in the UK and Ireland. Br. Dent. J. 2016, 220, 17–20. [Google Scholar] [CrossRef]
- Khanagar, S.B.; Al-Ehaideb, A.; Maganur, P.C.; Vishwanathaiah, S.; Patil, S.; Baeshen, H.A.; Sarode, S.C.; Bhandi, S. Developments, application, and performance of artificial intelligence in dentistry—A systematic review. J. Dent. Sci. 2021, 16, 508–522. [Google Scholar] [CrossRef]
- Pacheco, A.G.C.; Krohling, R.A. The impact of patient clinical information on automated skin cancer detection. Comput. Biol. Med. 2020, 116, 103545. [Google Scholar] [CrossRef]
- Abbott, L.M.; Smith, S.D. Smartphone apps for skin cancer diagnosis: Implications for patients and practitioners. Australas. J. Dermatol. 2018, 59, 168–170. [Google Scholar] [CrossRef]
- Chuchu, N.; Takwoingi, Y.; Dinnes, J.; Matin, R.N.; Bassett, O.; Moreau, J.F.; Bayliss, S.E.; Davenport, C.; Godfrey, K.; O’Connell, S.; et al. Smartphone applications for triaging adults with skin lesions that are suspicious for melanoma. Cochrane Database Syst. Rev. 2018, 12, CD013192. [Google Scholar] [CrossRef] [PubMed]
- Udrea, A.; Mitra, G.D.; Costea, D.; Noels, E.C.; Wakkee, M.; Siegel, D.M.; de Carvalho, T.M.; Nijsten, T.E.C. Accuracy of a smartphone application for triage of skin lesions based on machine learning algorithms. J. Eur. Acad. Dermatol. Venereol. JEADV 2020, 34, 648–655. [Google Scholar] [CrossRef] [PubMed]
- El-Khatib, H.; Popescu, D.; Ichim, L. Deep Learning–Based Methods for Automatic Diagnosis of Skin Lesions. Sensors 2020, 20, 1753. [Google Scholar] [CrossRef] [Green Version]
- Nasiri, S.; Helsper, J.; Jung, M.; Fathi, M. DePicT Melanoma Deep-CLASS: A deep convolutional neural networks approach to classify skin lesion images. BMC Bioinform. 2020, 21, 84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winkler, J.K.; Sies, K.; Fink, C.; Toberer, F.; Enk, A.; Deinlein, T.; Hofmann-Wellenhof, R.; Thomas, L.; Lallas, A.; Blum, A.; et al. Melanoma recognition by a deep learning convolutional neural network-Performance in different melanoma subtypes and localisations. Eur. J. Cancer 2020, 127, 21–29. [Google Scholar] [CrossRef] [PubMed]
- D, S.R.; A, S. Deep Learning Based Skin Lesion Segmentation and Classification of Melanoma Using Support Vector Machine (SVM). Asian Pac. J. Cancer Prev. APJCP 2019, 20, 1555–1561. [Google Scholar] [CrossRef] [Green Version]
- Bajwa, M.N.; Muta, K.; Malik, M.I.; Siddiqui, S.A.; Braun, S.A.; Homey, B.; Dengel, A.; Ahmed, S. Computer-Aided Diagnosis of Skin Diseases Using Deep Neural Networks. Appl. Sci. 2020, 10, 2488. [Google Scholar] [CrossRef] [Green Version]
- Rotemberg, V.; Kurtansky, N.; Betz-Stablein, B.; Caffery, L.; Chousakos, E.; Codella, N.; Combalia, M.; Dusza, S.; Guitera, P.; Gutman, D.; et al. A patient-centric dataset of images and metadata for identifying melanomas using clinical context. Sci. Data 2021, 8, 34. [Google Scholar] [CrossRef]
- Cullell-Dalmau, M.; Otero-Viñas, M.; Manzo, C. Research Techniques Made Simple: Deep Learning for the Classification of Dermatological Images. J. Investig. Dermatol. 2020, 140, 507–514.e1. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Lichen Planus | Leukoplakia | Aphthous Ulcer | Bullous Diseases | Gingival Enlargement | Carcinoma | Others | p-Value a | |
|---|---|---|---|---|---|---|---|---|
| Number of Subjects | (n = 77) | (n = 41) | (n = 37) | (n = 26) | (n = 12) | (n = 11) | (n = 95) | |
| Gender (n,%) | 0.03 | |||||||
| Male | 22 (29%) | 20 (49%) | 19 (51%) | 9 (35%) | 5 (42%) | 5 (45%) | 42 (44%) | |
| Female | 51 (66%) | 16 (39%) | 14 (38%) | 15 (58%) | 3 (25%) | 4 (36%) | 53 (56%) | |
| Mean age | 65 | 65 | 50 | 65 | 43 | 54 | 50 | <0.001 |
| Alcohol (n,%) | 2 (3%) | 4 (10%) | 1 (3%) | - | - | 2 (18%) | 2 (2%) | 0.007 |
| Smoking (n,%) | 21 (27%) | 18 (44%) | 8 (22%) | 3 (12%) | 1 (8%) | 5 (45%) | 16 (17%) | 0.002 |
| Number of lesions (n) | 497 | 91 | 110 | 173 | 46 | 41 | 252 | |
| Localization (n,%) | 0.002 | |||||||
| Vermilion | 19 (3.8 %) | 6 (6.5%) | 5 (4.5%) | 3 (1.7%) | - | - | 16 (6.3%) | |
| Commissure | 1 (0.2%) | - | - | 1 (9.6%) | - | - | 8 (3%) | |
| Labial mucosa | 8 (1.7%) | 3 (3%) | 15 (13.6%) | 16 (9.2%) | - | 1 (2.4%) | 21 (8.3%) | |
| Muco-buccal fold | 136 (27.3%) | 25 (27.5%) | 18 (16.4%) | 16 (9.2%) | - | 5 (12%) | 21 (8.3%) | |
| Attached gingiva | 172 (34.6%) | 12 (13.1%) | 12 (10.9%) | 91 (52.6%) | 45 (98%) | 16 (39%) | 85 (33.7%) | |
| Buccal mucosa | 37 (7.4%) | 3 (3.3%) | 10 (9.0%) | 14 (8.0%) | 1 (2.0%) | 2 (4.8%) | 11 (4.4%) | |
| Hard palate | 22 (4.4%) | 13 (14.3%) | 5 (4.5%) | 10 (5.7%) | - | 11 (26.8%) | 20 (7.9%) | |
| Soft palate | 1 (0.2%) | 4 (4.4%) | 5 (4.5%) | 19 (10.9%) | - | - | 2 (0.7%) | |
| Tonsillar pillar | 3 (0.6%) | 1 (1.1%) | 1 (0.9%) | 1 (0.5%) | - | - | 2 (0.7%) | |
| Dorsal tongue | 60 (12.0%) | 7 (1.8%) | 3 (2.7%) | 2 (1.2%) | - | 2 (4.8%) | 51 (20.2%) | |
| Ventral tongue | 9 (1.8%) | 1 (1.0%) | 10 (9.0%) | 6 (3.5%) | - | 1 (2.4%) | 2 (0.7%) | |
| Lateral tongue | 24 (4.8%) | 14 (15.4%) | 13 (11.8%) | - | - | 1 (2.4%) | 11 (4.4%) | |
| Floor of mouth | 5 (1.0%) | 2 (2.2%) | 2 (1.8%) | - | - | 2 (4.8%) | 2 (0.7%) | |
| Lesion color (n,%) | <0.001 | |||||||
| White | 160 (32.0%) | 70 (7.8%) | 33 (30.0%) | 46 (26.6%) | - | 13 (31.7%) | 50 (18.8%) | |
| Red | 55 (11.0%) | 2 (2.2%) | 9 (8.1%) | 55 (31.8%) | 15 (32,6%) | 8 (19.5%) | 51 (20.2%) | |
| Mixt (red and white) | 268 (54%) | 19 (20.8%) | 66 (60.0%) | 69 (39.9%) | 5 (11.8%) | 16 (39.0%) | 79 (31.3%) | |
| Pigmented | 10 (2.0%) | - | 1 (0.9%) | - | 5 (11.8%) | 3 (2.3%) | 40 (15.8%) | |
| No color changes | 4 (0.8%) | - | 1 (0.9%) | - | 21 (46.0%) | 1 (2.4%) | 32 (12.7%) | |
| Lesion size (n,%) | <0.001 | |||||||
| <5 mm | 39 (7.8%) | 13 (14.3%) | 27 (24.5%) | 32 (18.5%) | 27 (58.6%) | 1 (2.4%) | 41 (16.2%) | |
| 5 to 10 mm | 268 (54.0%) | 41 (45.1%) | 66 (60.0%) | 116 (67.0%) | 38 (82.6%) | 9 (21.9%) | 135 (53.1%) | |
| 10 to 50 mm | 188 (38.0%) | 37 (40.7%) | 17 (15.5%) | 25 (14.5%) | 6 (13.0%) | 27 (65.8%) | 75 (29.7%) | |
| >50 mm | 2 (0.4%) | - | - | - | - | 4 (9.7%) | 1 (0.4%) | |
| Elementary Lesion (n,%) | <0.001 | |||||||
| Gingival hyperplasia | 3 (0.6%) | - | - | 1 (0.5%) | 40 (86.9%) | - | 9 (3.5%) | |
| Bulla | 7 (1.4%) | 2 (2.2%) | 2 (1.8%) | 31 (18.0%) | - | - | 16 (6.3%) | |
| Cellular coating | 11 (2.2%) | 1 (1.1%) | 13 (11.8%) | 16 (9.2%) | - | 2 (4.8%) | 12 (4.7%) | |
| Erosion | 18 (3.6%) | 3 (3.3%) | 6 (5.5%) | 30 (18.3%) | - | 1 (2.4%) | 8 (3.1%) | |
| Macula/patch | 184 (37.0%) | 12 (13.2%) | 11 (10.0%) | 79 (45.7%) | 6 (13.0%) | 4 (9.7%) | 78 (30.9%) | |
| Nodule | 13 (2.6%) | 2 (2.2%) | 2 (1.8%) | - | - | 18 (43.9%) | 100 (39.6%) | |
| Papula/plaque | 220 (44.3%) | 70 (77.0%) | 8 (7.3%) | 7 (4.0%) | - | 13 (31.7%) | 23 (9.1%) | |
| Ulcer | 40 (8.0%) | 1 (1.1%) | 68 (61.8%) | 9 (5.2%) | - | 3 (7.3%) | 4 (1.5%) | |
| Lesion homogeneity (n,%) | 187 (37.6%) | 52 (75.1%) | 77 (70.0%) | 71 (41.0%) | 32 (69.5%) | 5 (12.1%) | 142 (56.4%) | <0.001 |
| Well circumscribed lesion (n,%) | 230 (46.3%) | 55 (60.4%) | 93 (84.5%) | 81 (46.8%) | 19 (41.3%) | 7 (17.0%) | 166 (65.8%) | <0.001 |
| Elevated edges of the lesion (n,%) | 5 (1.0%) | - | 13 (11.8%) | 2 (1.2%) | 1 (2.0%) | 1 (2.4%) | 4 (1.6%) | 0.29 |
| Reticular lesion (n,%) | 175 (35.2%) | 3 (3.3%) | 1 (0.9%) | 5 (2.9%) | - | - | 5 (1.9%) | <0.001 |
| Growing lesion (n,%) | 13 (2.6%) | 2 (2.2%) | - | 1 (0.5%) | 3 (6.5%) | 24 (58.5%) | 25 (9.9%) | <0.001 |
| Papillomatus lesion (n,%) | 3 (0.6%) | 8 (8.8%) | 1 (0.9%) | 1 (0.5%) | 1 (2.0%) | 8 (19.5%) | 41 (16.2%) | 0.007 |
| LightGBM | Elastic Net Regression | K-Nearest Neighbors | Decision Tree | Multilayer Perceptron | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Diagnostics | TPR | TNR | PPV | NPV | F1 | TPR | TNR | PPV | NPV | F1 | TPR | TNR | PPV | NPV | F1 | TPR | TNR | PPV | NPV | F1 | TPR | TNR | PPV | NPV | F1 |
| Gingival enlargement | 0.92 | 1.00 | 1.00 | 1.00 | 0.96 | 0.92 | 0.99 | 0.85 | 1.00 | 0.88 | 0.83 | 0.99 | 0.71 | 0.99 | 0.77 | 0.67 | 0.97 | 0.47 | 0.99 | 0.55 | 0.83 | 1.00 | 1.00 | 0.99 | 0.91 |
| Carcinoma | 0.90 | 1.00 | 0.90 | 1.00 | 0.90 | 0.60 | 0.92 | 0.21 | 0.99 | 0.32 | 0.70 | 0.99 | 0.64 | 0.99 | 0.67 | 0.80 | 0.96 | 0.40 | 0.99 | 0.53 | 0.50 | 0.98 | 0.50 | 0.98 | 0.50 |
| Leukoplakia | 0.78 | 0.98 | 0.75 | 0.98 | 0.77 | 0.74 | 0.91 | 0.40 | 0.98 | 0.52 | 0.57 | 0.94 | 0.42 | 0.96 | 0.48 | 0.74 | 0.89 | 0.36 | 0.98 | 0.49 | 0.35 | 0.98 | 0.62 | 0.95 | 0.44 |
| Oral lichen planus | 0.89 | 0.89 | 0.85 | 0.92 | 0.87 | 0.38 | 0.92 | 0.77 | 0.68 | 0.51 | 0.85 | 0.88 | 0.83 | 0.89 | 0.84 | 0.27 | 0.98 | 0.92 | 0.66 | 0.42 | 0.84 | 0.70 | 0.66 | 0.86 | 0.74 |
| Bullous diseases | 0.72 | 0.96 | 0.76 | 0.95 | 0.74 | 0.70 | 0.81 | 0.38 | 0.94 | 0.49 | 0.70 | 0.96 | 0.75 | 0.95 | 0.72 | 0.74 | 0.76 | 0.34 | 0.95 | 0.46 | 0.35 | 0.95 | 0.56 | 0.90 | 0.43 |
| Aphthous ulcers | 0.75 | 0.99 | 0.84 | 0.97 | 0.79 | 0.54 | 0.96 | 0.56 | 0.95 | 0.55 | 0.46 | 0.97 | 0.59 | 0.95 | 0.52 | 0.75 | 0.92 | 0.50 | 0.97 | 0.60 | 0.50 | 0.98 | 0.74 | 0.95 | 0.60 |
| Other lesions | 0.89 | 0.97 | 0.89 | 0.97 | 0.89 | 0.60 | 0.94 | 0.72 | 0.90 | 0.66 | 0.67 | 0.93 | 0.72 | 0.91 | 0.69 | 0.46 | 0.93 | 0.64 | 0.87 | 0.54 | 0.73 | 0.92 | 0.70 | 0.93 | 0.71 |
| Mean accuracy | 0.84 | 0.54 | 0.73 | 0.49 | 0.67 | ||||||||||||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dubuc, A.; Zitouni, A.; Thomas, C.; Kémoun, P.; Cousty, S.; Monsarrat, P.; Laurencin, S. Improvement of Mucosal Lesion Diagnosis with Machine Learning Based on Medical and Semiological Data: An Observational Study. J. Clin. Med. 2022, 11, 6596. https://doi.org/10.3390/jcm11216596
Dubuc A, Zitouni A, Thomas C, Kémoun P, Cousty S, Monsarrat P, Laurencin S. Improvement of Mucosal Lesion Diagnosis with Machine Learning Based on Medical and Semiological Data: An Observational Study. Journal of Clinical Medicine. 2022; 11(21):6596. https://doi.org/10.3390/jcm11216596
Chicago/Turabian StyleDubuc, Antoine, Anissa Zitouni, Charlotte Thomas, Philippe Kémoun, Sarah Cousty, Paul Monsarrat, and Sara Laurencin. 2022. "Improvement of Mucosal Lesion Diagnosis with Machine Learning Based on Medical and Semiological Data: An Observational Study" Journal of Clinical Medicine 11, no. 21: 6596. https://doi.org/10.3390/jcm11216596
APA StyleDubuc, A., Zitouni, A., Thomas, C., Kémoun, P., Cousty, S., Monsarrat, P., & Laurencin, S. (2022). Improvement of Mucosal Lesion Diagnosis with Machine Learning Based on Medical and Semiological Data: An Observational Study. Journal of Clinical Medicine, 11(21), 6596. https://doi.org/10.3390/jcm11216596