
BSSRO Improves Mandibular Morphology Mainly through Correction of Body Length and Volume in Patients with Asymmetric Mandibular Prognathism

Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
- (1)
- Adult patients diagnosed with asymmetric mandibular prognathism;
- (2)
- ANB angle was less than 0 degree;
- (3)
- The distance between the submental point and the midsagittal plane on the 3D reconstruction model was ≥4 mm;
- (4)
- Patients were treated with orthodontic appliance and orthognathic surgery;
- (5)
- Patients who accepted BSSRO with or without genioplasty.
- (1)
- Patients with maxillofacial trauma or jaw deformity secondary to cleft lip and palate;
- (2)
- Patients with condylar tumor;
- (3)
- Patients with systemic diseases;
- (4)
- Patients with a history of camouflaged orthognathic surgery;
- (5)
- Patients who underwent maxillary orthognathic surgery at the same time (some studies have shown that the change of the condyle and the ramus angle after single mandibular surgery is different from that of bimaxillary surgery [9]. In order to minimize this system error, we chose patients who had mandibular surgery only).
2.2. Data Collection and Processing
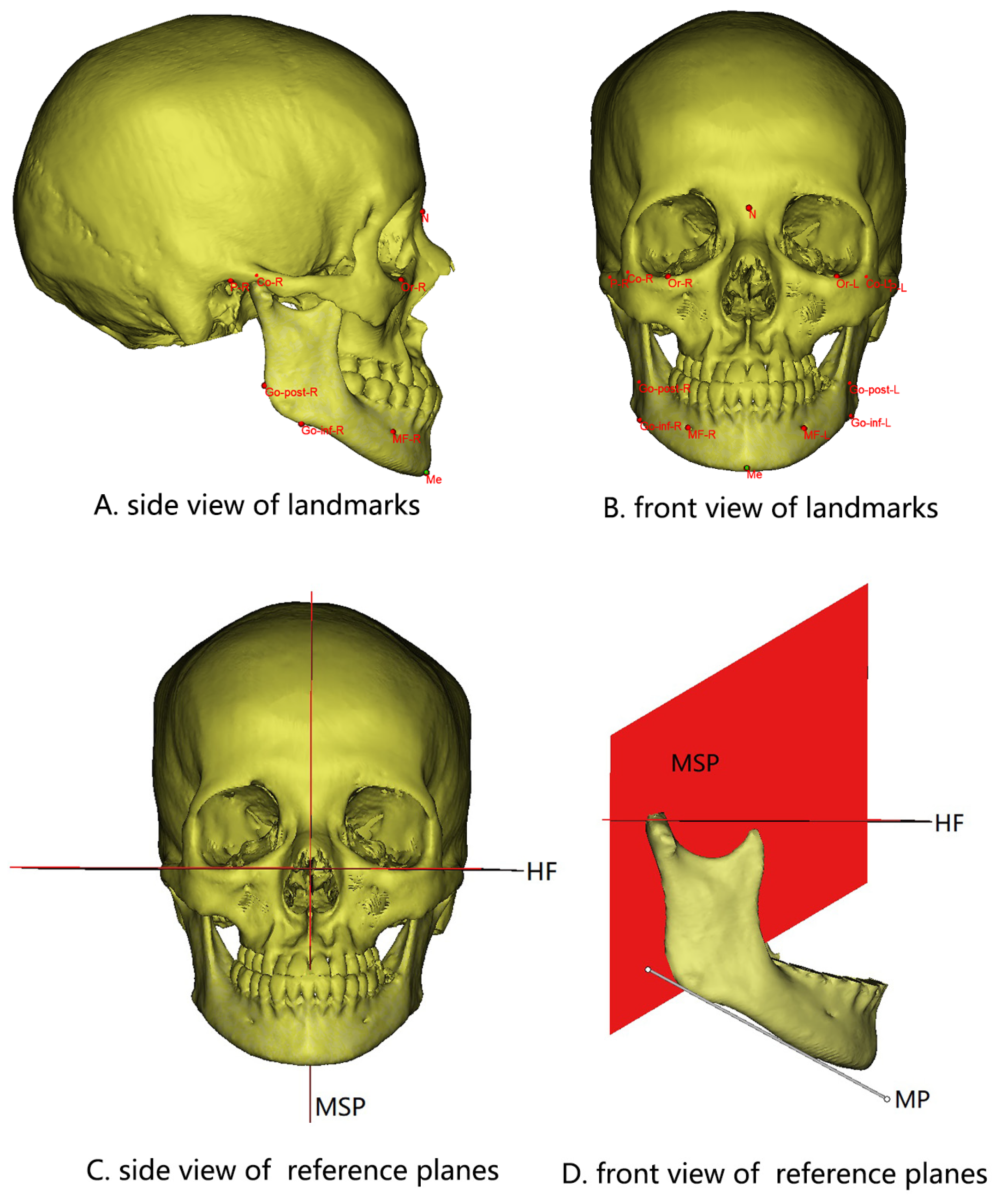
2.3. Selection of Marker Points and Reference Planes
2.4. Measurement Items (Figure 1 and Figure 2)
- (1)
- Condyle volume: the volume of the part above the plane which is parallel to the HF and passes through the lowest point of the sigmoid notch.
- (2)
- Medial–lateral diameter of the condyle: the distance from the innermost point to the outermost point of the condyle.
- (3)
- Anterior–posterior diameter of the condyle: the distance from the most anterior point to the last point of the condyle.
- (4)
- Ramus height: the distance from Co to Go-inf.
- (5)
- Ramus volume: the volume of the part of the mandible above the plane established by J-lat, J-med, and Go-inf.
- (6)
- Body volume: after making a plane parallel to the MSP through the MF, the body volume is the volume of the distal part of this plane, excluding the ramus volume.
- (7)
- Body length: the distance from Go-post to MF.
- (8)
- Body height: the vertical distance between MP and the margin of the distal alveolar bone of the first molar.


2.5. Statistical Analysis
3. Results
3.1. Symmetric Analysis of Bilateral Mandible before Operation (T0)
3.2. Changes in the Long and Short Sides Immediately after Surgery (T1)
3.3. Symmetric Analysis of Bilateral Mandible after Surgery (T1)
3.4. Morphological Changes of Bilateral Mandible over Six Months after Surgery (T2)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Proothi, M.; Drew, S.J.; Sachs, S.A. Motivating factors for patients undergoing orthognathic surgery evaluation. J. Oral Maxillofac. Surg. 2010, 68, 1555–1559. [Google Scholar] [CrossRef] [PubMed]
- Eslamipour, F.; Najimi, A.; Tadayonfard, A.; Azamian, Z. Impact of Orthognathic Surgery on Quality of Life in Patients with Dentofacial Deformities. Int. J. Dentistry. 2017, 2017, 4103905. [Google Scholar] [CrossRef] [PubMed]
- Ming, T.C. Spectrum and management of dentofacial deformities in a multiethnic Asian population. Angle Orthod. 2006, 76, 806. [Google Scholar]
- Li, J.; Ryu, S.Y.; Park, H.J.; Kook, M.S.; Jung, S.; Han, J.J.; Oh, H.K. Changes in condylar position after BSSRO with and without Le Fort I osteotomy via surgery-first approach in mandibular prognathism with facial asymmetry. Oral Surg. Oral Med. Oral Pathol. Oral Radio 2017, 123, 661–669. [Google Scholar] [CrossRef]
- Borstlap, W.A.; Stoelinga, P.J.W.; Hoppenreijs, T.J.M.; Van’t Hof, M.A. Stabilisation of sagittal split set-back osteotomies with miniplates: A prospective, multicentre study with 2-year follow-up. Int. J. Oral Maxillofac. Surg. 2005, 34, 487–494. [Google Scholar] [CrossRef]
- Je, F.; Van Sickels, J.E.; Thrash, W.J. Factors contributing to relapse in rigidly fixed mandibular setbacks. J. Oral Maxillofac. Surg. 1989, 47, 451–456. [Google Scholar]
- Hwang, H.S.; Hwang, C.H.; Lee, K.H.; Kang, B.C. Maxillofacial 3-dimensional Image Analysis for the Diagnosis of Facial Asymmetry. Am. J. Orthod. Dentofac. 2006, 130, 779–785. [Google Scholar] [CrossRef]
- Yun, H.S.; Jang, T.J.; Lee, S.M.; Lee, S.H.; Seo, J.K. Learning-based local-to-global landmark annotation for automatic 3D cephalometry. Phys. Med. Bio. 2020, 65, 085018. [Google Scholar] [CrossRef]
- Kim, Y.J.; Oh, K.M.; Hong, J.S.; Lee, J.H.; Kim, H.M.; Reyes, M.; Cevidanes, L.H.S.; Park, Y.-H. Do Patients Treated with Bimaxillary Surgery Have More Stable Condylar Positions than Those Who Have Undergone Single-Jaw Surgery? J. Oral Maxillofac. Surg. 2012, 70, 2143–2152. [Google Scholar] [CrossRef]
- You, K.H.; Kim, K.H.; Lee, K.J.; Baik, H.S. Three-dimensional computed tomography analysis of mandibular morphology in patients with facial a symmetry and mandibular retrognathism. Am. J. Orthod. Dentofac. 2018, 153, 685–691. [Google Scholar] [CrossRef]
- Guijarro-Martínez, R.; Swennen, G. Three-dimensional cone beam computed tomography definition of the anatomical subregions of the upper airway: A validation study. Int. J. Oral Max Surg. 2013, 42, 1140–1149. [Google Scholar] [CrossRef] [PubMed]
- Ueki, K.; Moroi, A.; Sotobori, M.; Ishihara, Y.; Marukawa, K.; Yoshizawa, K.; Kato, K.; Kawashiri, S. Changes in temporomandibular joint and ramus after sagittal split ramus osteotomy in mandibular prognathism patients with and without asymmetry. J. Cranio. Maxill Surg. 2012, 40, 821–827. [Google Scholar] [CrossRef] [PubMed]
- Ueki, K.; Moroi, A.; Sotobori, M.; Ishihara, Y.; Marukawa, K.; Yoshizawa, K.; Kato, K.; Kawashiri, S. Evaluating the mandible with cone-beam computed tomography. Am. J. Orthod. Dentofac. 2010, 137, S58–S70. [Google Scholar]
- Berger, J.L.; Pangrazio-Kulbersh, V.; Bacchus, S.N.; Kaczynski, R. Stability of bilateral sagittal split ramus osteotomy: Rigid fixation versus transosseous wiring. Am. J. Orthod. Dentofac. 2000, 118, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Lee, K. Three-Dimensional Evaluation of the Postsurgical Stability of Mandibular Setback with the Surgery-First Approach: Comparison between Patients With Symmetry and Asymmetry. J. Oral Maxillofac. Surg. 2019, 77, 1461–1469. [Google Scholar] [CrossRef]
- Hågensli, N.; Stenvik, A.; Espeland, L. Asymmetric mandibular prognathism: Outcome, stability and patient satisfaction after BSSRO surgery. A retrospective study. J. Cranio-Maxillofac. Surg. 2014, 42, 1735–1741. [Google Scholar] [CrossRef]
- Lin, H.; Zhu, P.; Lin, Q.; Huang, X.; Xu, Y.; Yang, X. Comprehensive Analysis of Mandibular Residual Asymmetry after Bilateral Sagittal Split Ramus Osteotomy Correction of Menton Point Deviation. PLoS ONE 2016, 11, e161601. [Google Scholar] [CrossRef]
- Abotaleb, B.M.; Bi, R.; Liu, Y.; Jiang, N.; Telha, W.; Zhu, S. Three-dimensional condylar displacement and remodelling in patients with asymmetrical mandibular prognathism following bilateral sagittal split osteotomy. Int. J. Oral Maxillofac. Surg. 2021, 51, 509–517. [Google Scholar] [CrossRef]
- Kim, H.O.; Lee, W.; Kook, Y.A.; Kim, Y. Comparison of the condyle-fossa relationship between skeletal class III malocclusion patients with and without asymmetry: A retrospective three-dimensional cone-beam computed tomograpy study. Korean J. Orthod. 2013, 43, 209–217. [Google Scholar] [CrossRef] [Green Version]
- Baek, S.H.; Kim, T.K.; Kim, M.J. Is there any difference in the condylar position and angulation after asymmetric mandibular setback? Oral Surg. Oral Med. Oral Pathol. Oral Radio 2006, 101, 155–163. [Google Scholar] [CrossRef]
- Ueki, K.; Nakagawa, K.; Marukawa, K.; Yamamoto, E.; Takeuchi, N. Stress change on the temporomandibular joint in mandibular prognathism subjects with asymmetry after orthognathic surgery. Eur. J. Orthodont. 2010, 32, 522–529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shu, J.; Zhang, Y.; Chong, D.Y.; Liu, Z. Effects on loads in temporomandibular joints for patients with mandibular asymmetry before and after orthognathic surgeries under the unilateral molar clenching. Biomech. Model Mechan. 2020, 19, 533–541. [Google Scholar] [CrossRef] [PubMed]
- Moroi, A.; Yoshizawa, K.; Iguchi, R.; Kosaka, A.; Ikawa, H.; Saida, Y.; Hotta, A.; Tsutsui, T.; Ueki, K. Comparison of the computed tomography values of the bone fragment gap after sagittal split ramus osteotomy in mandibular prognathism with and without asymmetry. Int. J. Oral Maxillofac. Surg. 2016, 45, 1520–1525. [Google Scholar] [CrossRef] [PubMed]
- Ueki, K.; Yoshizawa, K.; Moroi, A.; Iguchi, R.; Kosaka, A.; Ikawa, H.; Tsutsui, T.; Saida, Y.; Hotta, A. Change in mandibular body height at the site of a fixation plate in the advance (lengthening) and setback (shortening) sides after sagittal split ramus osteotomy. J. Cranio-Maxillofac. Surg. 2016, 44, 279–284. [Google Scholar] [CrossRef]
- Aneja, V.; Raval, R.; Aneja, P.; Rai, K.K.; Agarwal, S.; Chuadhary, S. Evaluation of Mandibular Condylar Changes in Patients following Orthognathic Surgery: A Retrospective Study. Niger. J. Surg. 2017, 23, 37–41. [Google Scholar]
- Ayoub, A.F.; Millett, D.T.; Hasan, S. Evaluation of skeletal stability following surgical correction of mandibular prognathism. Br. J. Oral Maxillofac. Surg. 2000, 38, 305–311. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Landmarks and Reference Planes | Definition |
|---|---|
| Or, R/L | The most inferior point of the bony orbitale |
| P, R/L | The most superior point of the external auditory meatus |
| Ba | Midpoint of the anterior margin of the foramen magnum on the occipital point |
| N | The junction of the nasal and frontal bones in the midline |
| Me | The most inferior midpoint of the mandibular symphysis |
| Go-inf, R/L | The most inferior point on the mandibular angle |
| Go-post, R/L | The most posterior point on the mandibular angle |
| Co, R/L | The most superior point of the condylar head |
| MF, R/L | Mental foramen |
| J-lat, R/L | The most lateral and deepest point of the curvature at the junction of the mandibular ramus and body |
| J-med, R/L | The most medial and deepest point of the curvature formed at the junction of the mandibular ramus and body |
| HF | Frankfort horizontal plane |
| MSP | Plane passing through N and Ba perpendicular to HF |
| MP | Tangent to the lowest part of the mandibular inferior border |
| Measurement | Long Side | Short Side | Difference | p (Long Side-Short Side) |
|---|---|---|---|---|
| Condyle volume (mm3) | 1991.30 ± 506.22 | 1708.05 ± 499.37 | 283.25 ± 380.96 | 0.000 ** |
| Medial–lateral diameter of condyle (mm) | 19.49 ± 2.46 | 18.82 ± 2.22 | 0.67 ± 2.12 | 0.030 * |
| Anterior–posterior diameter of condyle (mm) | 8.25 ± 1.41 | 8.11 ± 1.66 | 0.14 ± 1.17 | 0.398 |
| Ramus height (mm) | 69.91 ± 5.81 | 66.39 ± 5.50 | 3.51 ± 4.85 | 0.000 ** |
| Ramus volume (mm3) | 10,399.23 ± 1919.99 | 9912.39 ± 1947.23 | 486.85 ± 1056.21 | 0.002 ** |
| Body volume (mm3) | 10,378.98 ± 1775.21 | 10,086.02 ± 1759.39 | 292.96 ± 899.77 | 0.026 * |
| Body length (mm) | 67.24 ± 4.49 | 65.11 ± 4.82 | 2.13 ± 2.59 | 0.000 ** |
| Body height (mm) | 26.42 ± 2.73 | 26.89 ± 2.59 | −0.47 ± 1.64 | 0.051 |
| Measurement | T0 | T1 | Difference | p (T1-T0) | |
|---|---|---|---|---|---|
| Long Side | Ramus height (mm) | 69.91 ± 5.81 | 69.65 ± 5.57 | −0.26 ± 1.59 | 0.260 |
| Ramus volume (mm3) | 10,399.23 ± 1919.99 | 10,675.08 ± 1915.72 | 275.85 ± 565.35 | 0.001 ** | |
| Body volume (mm3) | 10,378.98 ± 1775.21 | 10,098.15 ± 1804.49 | −280.83 ± 710.88 | 0.007 ** | |
| Body length (mm) | 67.24 ± 4.49 | 63.60 ± 4.54 | −3.64 ± 2.34 | 0.000 ** | |
| Body height (mm) | 26.42 ± 2.73 | 26.54 ± 2.62 | 0.12 ± 0.67 | 0.226 | |
| Short Side | Ramus height (mm) | 66.39 ± 5.50 | 66.56 ± 5.61 | 0.17 ± 1.61 | 0.458 |
| Ramus volume (mm3) | 9912.39 ± 1947.23 | 10,005.36 ± 1957.10 | 92.97 ± 564.33 | 0.250 | |
| Body volume (mm3) | 10,086.02 ± 1759.39 | 10,257.40 ± 1815.77 | 171.38 ± 595.18 | 0.051 | |
| Body length (mm) | 65.11 ± 4.82 | 64.94 ± 4.62 | −0.17 ± 2.11 | 0.567 | |
| Body height (mm) | 26.89 ± 2.59 | 26.87 ± 2.59 | −0.02 ± 0.69 | 0.833 |
| Measurement | Long Side | Short Side | Difference | p (Long Side-Short Side) |
|---|---|---|---|---|
| Ramus height (mm) | 69.65 ± 5.57 | 66.56 ± 5.61 | 3.09 ± 4.68 | 0.000 ** |
| Ramus volume (mm3) | 10,675.08 ± 1915.72 | 10,005.36 ± 1957.10 | 669.72 ± 1052.14 | 0.000 ** |
| Body volume (mm3) | 10,098.15 ± 1804.49 | 10,257.40 ± 1815.77 | −159.25 ± 1121.66 | 0.320 |
| Body length (mm) | 63.60 ± 4.54 | 64.94 ± 4.62 | −1.34 ± 3.06 | 0.003 ** |
| Body height (mm) | 26.54 ± 2.62 | 26.87 ± 2.59 | −0.33 ± 1.75 | 0.188 |
| Measurement | T1 | T2 | Difference | p (T2-T1) | |
|---|---|---|---|---|---|
| Long Side | Condyle volume (mm3) | 2040.25 ± 506.47 | 1989.49 ± 523.03 | −50.77 ± 202.40 | 0.082 |
| Medial–lateral diameter of condyle (mm) | 19.47 ± 2.44 | 19.73 ± 2.78 | 0.25 ± 1.09 | 0.106 | |
| Anterior–posterior diameter of condyle (mm) | 8.35 ± 1.42 | 8.38 ± 1.43 | 0.03 ± 0.63 | 0.739 | |
| Ramus height (mm) | 69.65 ± 5.57 | 69.08 ± 6.05 | −0.57 ± 1.82 | 0.031 * | |
| Ramus volume (mm3) | 10,675.08 ± 1915.72 | 11,266.45 ± 1987.58 | 591.37 ± 688.78 | 0.000 ** | |
| Body volume (mm3) | 10,098.15 ± 1804.49 | 10,599.45 ± 1893.86 | 501.31 ± 762.77 | 0.000 ** | |
| Body length (mm) | 63.60 ± 4.54 | 63.99 ± 4.27 | 0.39 ± 1.37 | 0.052 | |
| Body height (mm) | 26.54 ± 2.62 | 25.85 ± 2.90 | −0.69 ± 1.08 | 0.000 ** | |
| Short Side | Condyle volume (mm3) | 1744.72 ± 515.87 | 1681.99 ± 569.73 | −62.73 ± 235.78 | 0.066 |
| Medial–lateral diameter of condyle (mm) | 18.76 ± 2.17 | 18.81 ± 2.39 | 0.04 ± 0.82 | 0.724 | |
| Anterior–posterior diameter of condyle (mm) | 8.18 ± 1.74 | 8.05 ± 1.78 | −0.13 ± 0.77 | 0.230 | |
| Ramus height (mm) | 66.56 ± 5.61 | 65.87 ± 5.67 | −0.69 ± 1.62 | 0.004 ** | |
| Ramus volume (mm3) | 10,005.36 ± 1957.10 | 10,352.99 ± 1895.42 | 347.63 ± 699.86 | 0.001 ** | |
| Body volume (mm3) | 10,257.40 ± 1815.77 | 10,891.46 ± 2164.02 | 634.06 ± 822.44 | 0.000 ** | |
| Body length (mm) | 64.94 ± 4.62 | 64.92 ± 4.81 | −0.02 ± 1.51 | 0.937 | |
| Body height (mm) | 26.87 ± 2.59 | 26.07 ± 3.00 | −0.80 ± 1.20 | 0.000 ** |
| Measurement | T1 | T2 | p |
|---|---|---|---|
| Ramus height difference (mm) | 3.09 ± 4.68 | 3.21 ± 4.70 | 0.717 |
| Ramus volume difference (mm) | 669.72 ± 1052.14 | 913.46 ± 1152.58 | 0.019 * |
| Body volume difference (mm3) | −159.25 ± 1121.66 | −292.01 ± 1224.09 | 0.283 |
| Body length difference (mm) | −1.34 ± 3.06 | −0.93 ± 3.23 | 0.130 |
| Body height difference (mm) | −0.33 ± 1.75 | −0.22 ± 1.76 | 0.469 |
| Condyle volume difference (mm3) | 295.53 ± 415.80 | 307.49 ± 497.44 | 0.723 |
| Medial–lateral diameter of condyle difference (mm) | 0.71± 2.05 | 0.92 ± 2.39 | 0.165 |
| Anterior–posterior diameter of condyle difference (mm) | 0.16 ± 1.34 | 0.33 ± 1.38 | 0.273 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, Y.; Li, Y. BSSRO Improves Mandibular Morphology Mainly through Correction of Body Length and Volume in Patients with Asymmetric Mandibular Prognathism. J. Clin. Med. 2022, 11, 7131. https://doi.org/10.3390/jcm11237131
Liu Y, Li Y. BSSRO Improves Mandibular Morphology Mainly through Correction of Body Length and Volume in Patients with Asymmetric Mandibular Prognathism. Journal of Clinical Medicine. 2022; 11(23):7131. https://doi.org/10.3390/jcm11237131
Chicago/Turabian StyleLiu, Yanfei, and Yunfeng Li. 2022. "BSSRO Improves Mandibular Morphology Mainly through Correction of Body Length and Volume in Patients with Asymmetric Mandibular Prognathism" Journal of Clinical Medicine 11, no. 23: 7131. https://doi.org/10.3390/jcm11237131
APA StyleLiu, Y., & Li, Y. (2022). BSSRO Improves Mandibular Morphology Mainly through Correction of Body Length and Volume in Patients with Asymmetric Mandibular Prognathism. Journal of Clinical Medicine, 11(23), 7131. https://doi.org/10.3390/jcm11237131