
BDNF and proBDNF Serum Protein Levels in Obstructive Sleep Apnea Patients and Their Involvement in Insomnia and Depression Symptoms

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Polysomnography
2.3. Questionnaires
2.3.1. Pittsburgh Sleep Quality Index (PSQI)
2.3.2. Beck Depression Inventory (BDI)
2.3.3. Athens Insomnia Scale (AIS)
2.4. Blood Collection and Protein Level Assessment
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| Abbreviations | Full Name |
| 7:8-DHF | 7,8-dihydroxyflavone |
| AHI | apnea-hypopnea index |
| AIS | Athens Insomnia Scale |
| Akt | AKT serine/threonine kinase |
| BDI | Beck Depression Inventory |
| BDNF | brain-derived neurotrophic factor |
| BMAL1 | aryl hydrocarbon receptor nuclear translocator-like protein 1 |
| CIH | chronic intermittent hypoxia |
| CPAP | continous positive airway pressure |
| CREB | CREB binding protein |
| EDS | excessive daytime sleepiness |
| HIF-1 | hypoxia-inducable factor 1 |
| HPA | hypothalamus-pituitary-adrenal glands axis |
| IH | intermittent hypoxia |
| IL1 | interleukin 1 |
| IQR | interquartile range |
| JNK | mitogen-activated protein kinase 8 |
| LTP | long-term potentiation |
| MAPK | mitogen-activated protein kinase 1 |
| MDD | major depressive disorder |
| NREM | non-rapid eye movement |
| NT | neurotrophin |
| OSA | obstructive sleep apnea |
| PER1 | period 1 protein |
| PI3K | -4,5-bisphosphate 3-kinase catalytic subunit |
| PKC | protein kinase C |
| PLC | phospholipase C |
| proBDNF | premature BDNF |
| PSG | polysomnography |
| PSQI | Pittsburgh Sleep Quality Index |
| Ras | KRAS proto-oncogene |
| REM | rapid eye movement |
| ROS | reactive oxygen species |
| SAPK | mitogen-activated protein kinase 4 |
| SpO2 | hemoglobin oxygen saturation |
| TrkB | neurotrophic receptor tyrosine kinase 2 |
References
- Gottlieb, D.J.; Punjabi, N.M. Diagnosis and Management of Obstructive Sleep Apnea: A Review. JAMA 2020, 323, 1389–1400. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, H.; Homayouni-Tabrizi, M.; Amiri, H.; Safari-Faramani, R.; Moradi, M.-T.; Fadaei, R.; Khazaie, H. The effect of continuous positive airway pressure on total antioxidant capacity in obstructive sleep apnea: A systematic review and meta-analysis. Sleep Breath. 2022. [Google Scholar] [CrossRef] [PubMed]
- Gabryelska, A.; Chrzanowski, J.; Sochal, M.; Kaczmarski, P.; Turkiewicz, S.; Ditmer, M.; Karuga, F.F.; Czupryniak, L.; Białasiewicz, P. Nocturnal Oxygen Saturation Parameters as Independent Risk Factors for Type 2 Diabetes Mellitus among Obstructive Sleep Apnea Patients. J. Clin. Med. 2021, 10, 3770. [Google Scholar] [CrossRef] [PubMed]
- Heinzer, R.; Vat, S.; Marques-Vidal, P.; Marti-Soler, H.; Andries, D.; Tobback, N.; Mooser, V.; Preisig, M.; Malhotra, A.; Waeber, G.; et al. Prevalence of sleep-disordered breathing in the general population: THE HypnoLaus study. Lancet Respir. Med. 2015, 3, 310–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tietjens, J.R.; Claman, D.; Kezirian, E.J.; De Marco, T.; Mirzayan, A.; Sadroonri, B.; Goldberg, A.N.; Long, C.; Gerstenfeld, E.P.; Yeghiazarians, Y. Obstructive Sleep Apnea in Cardiovascular Disease: A Review of the Literature and Proposed Multidisciplinary Clinical Management Strategy. J. Am. Heart Assoc. 2019, 8, e010440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeghiazarians, Y.; Jneid, H.; Tietjens, J.R.; Redline, S.; Brown, D.L.; El-Sherif, N.; Mehra, R.; Bozkurt, B.; Ndumele, C.E.; Somers, V.K. Obstructive Sleep Apnea and Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation 2021, 144, e56–e67. [Google Scholar] [CrossRef] [PubMed]
- Reutrakul, S.; Mokhlesi, B. Obstructive Sleep Apnea and Diabetes: A State of the Art Review. Chest 2017, 152, 1070–1086. [Google Scholar] [CrossRef]
- Mok, Y.; Tan, C.W.; Wong, H.S.; How, C.H.; Tan, K.L.A.; Hsu, P.P. Obstructive sleep apnoea and Type 2 diabetes mellitus: Are they connected? Singap. Med. J. 2017, 58, 179–183. [Google Scholar] [CrossRef] [Green Version]
- Ditmer, M.; Gabryelska, A.; Turkiewicz, S.; Białasiewicz, P.; Małecka-Wojciesko, E.; Sochal, M. Sleep Problems in Chronic Inflammatory Diseases: Prevalence, Treatment, and New Perspectives: A Narrative Review. J. Clin. Med. 2021, 11, 67. [Google Scholar] [CrossRef]
- Gabryelska, A.; Sochal, M.; Wasik, B.; Białasiewicz, P. Patients With Obstructive Sleep Apnea Are Over Four Times More Likely to Suffer From Psoriasis Than the General Population. J. Clin. Sleep Med. 2018, 14, 153. [Google Scholar] [CrossRef]
- Kuna, K.; Szewczyk, K.; Gabryelska, A.; Białasiewicz, P.; Ditmer, M.; Strzelecki, D.; Sochal, M. Potential Role of Sleep Deficiency in Inducing Immune Dysfunction. Biomedicines 2022, 10, 2159. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.-H.; Lin, H.-C. Obstructive sleep apnea and the risk of autoimmune diseases: A longitudinal population-based study. Sleep Med. 2012, 13, 583–588. [Google Scholar] [CrossRef]
- Parish, J.M. Genetic and immunologic aspects of sleep and sleep disorders. Chest 2013, 143, 1489–1499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verbraecken, J. More than sleepiness: Prevalence and relevance of nonclassical symptoms of obstructive sleep apnea. Curr. Opin. Pulm. Med. 2022, 28, 552–558. [Google Scholar] [CrossRef] [PubMed]
- Gabryelska, A.; Sochal, M.; Wasik, B.; Szczepanowski, P.; Białasiewicz, P. Factors Affecting Long-Term Compliance of CPAP Treatment—A Single Centre Experience. J. Clin. Med. 2021, 11, 139. [Google Scholar] [CrossRef]
- Luyster, F.S.; Buysse, D.J.; Strollo, P.J.J. Comorbid insomnia and obstructive sleep apnea: Challenges for clinical practice and research. J. Clin. sleep Med. 2010, 6, 196–204. [Google Scholar] [CrossRef] [Green Version]
- Cistulli, P.A.; Armitstead, J.; Pepin, J.-L.; Woehrle, H.; Nunez, C.M.; Benjafield, A.; Malhotra, A. Short-term CPAP adherence in obstructive sleep apnea: A big data analysis using real world data. Sleep Med. 2019, 59, 114–116. [Google Scholar] [CrossRef]
- Lechat, B.; Appleton, S.; Melaku, Y.A.; Hansen, K.; McEvoy, R.D.; Adams, R.; Catcheside, P.; Lack, L.; Eckert, D.J.; Sweetman, A. Comorbid insomnia and sleep apnoea is associated with all-cause mortality. Eur. Respir. J. 2022, 60, 2101958. [Google Scholar] [CrossRef]
- Jehan, S.; Auguste, E.; Pandi-Perumal, S.R.; Kalinowski, J.; Myers, A.K.; Zizi, F.; Rajanna, M.G.; Jean-Louis, G.; McFarlane, S.I. Depression, Obstructive Sleep Apnea and Psychosocial Health. Sleep Med. Disord. Int. J. 2017, 1, 00012. [Google Scholar]
- Reddy, A.; Mansuri, Z.; Vadukapuram, R.; Trivedi, C. Increased Suicidality and Worse Outcomes in MDD Patients With OSA: A Nationwide Inpatient Analysis of 11 Years From 2006 to 2017. J. Acad. Consult. Psychiatry 2022, 63, 46–52. [Google Scholar] [CrossRef]
- Sochal, M.; Ditmer, M.; Gabryelska, A.; Białasiewicz, P. The Role of Brain-Derived Neurotrophic Factor in Immune-Related Diseases: A Narrative Review. J. Clin. Med. 2022, 11, 6023. [Google Scholar] [CrossRef] [PubMed]
- Shi, X.-J.; Du, Y.; Lei-Chen; Li, X.-S.; Yao, C.-Q.; Cheng, Y. Effects of brain-derived neurotrophic factor (BDNF) on the Schizophrenia model of animals. J. Psychiatr. Res. 2022, 156, 538–546. [Google Scholar] [CrossRef] [PubMed]
- Meshkat, S.; Alnefeesi, Y.; Jawad, M.Y.; Di Vincenzo, J.D.; Rodrigues, N.B.; Ceban, F.; Lui, L.M.; McIntyre, R.S.; Rosenblat, J.D. Brain-Derived Neurotrophic Factor (BDNF) as a biomarker of treatment response in patients with Treatment Resistant Depression (TRD): A systematic review & meta-analysis. Psychiatry Res. 2022, 317, 114857. [Google Scholar] [CrossRef] [PubMed]
- Miuli, A.; Mancusi, G.; Pettorruso, M.; Di Carlo, F.; Clemente, K.; Di Meo, I.; D’Andrea, A.; Pernaci, G.; Di Crosta, T.; d’Andrea, G.; et al. Impact of sleep disorders and disease duration on neurotrophins levels in cocaine use disorder. Neurosci. Lett. 2022, 786, 136805. [Google Scholar] [CrossRef]
- Nordvall, G.; Forsell, P.; Sandin, J. Neurotrophin-targeted therapeutics: A gateway to cognition and more? Drug Discov. Today 2022, 27, 103318. [Google Scholar] [CrossRef]
- Xie, H.; Yung, W. Chronic intermittent hypoxia-induced deficits in synaptic plasticity and neurocognitive functions: A role for brain-derived neurotrophic factor. Acta Pharmacol. Sin. 2012, 33, 5–10. [Google Scholar] [CrossRef] [Green Version]
- Watson, A.J.; Henson, K.; Dorsey, S.G.; Frank, M.G. The truncated TrkB receptor influences mammalian sleep. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2015, 308, R199–R207. [Google Scholar] [CrossRef] [Green Version]
- Castrén, E.; Monteggia, L.M. Brain-Derived Neurotrophic Factor Signaling in Depression and Antidepressant Action. Biol. Psychiatry 2021, 90, 128–136. [Google Scholar] [CrossRef]
- Sochal, M.; Małecka-Panas, E.; Gabryelska, A.; Fichna, J.; Talar-Wojnarowska, R.; Szmyd, B.; Białasiewicz, P. Brain-derived neurotrophic factor is elevated in the blood serum of Crohn’s disease patients, but is not influenced by anti-TNF-α treatment—A pilot study. Neurogastroenterol. Motil. Off. J. Eur. Gastrointest. Motil. Soc. 2021, 33, e13978. [Google Scholar] [CrossRef]
- Panaree, B.; Chantana, M.; Wasana, S.; Chairat, N. Effects of obstructive sleep apnea on serum brain-derived neurotrophic factor protein, cortisol, and lipid levels. Sleep Breath. 2011, 15, 649–656. [Google Scholar] [CrossRef]
- Campos-Rodriguez, F.; Asensio-Cruz, M.I.; Cordero-Guevara, J.; Jurado-Gamez, B.; Carmona-Bernal, C.; Gonzalez-Martinez, M.; Troncoso, M.F.; Sanchez-Lopez, V.; Arellano-Orden, E.; Garcia-Sanchez, M.I.; et al. Effect of continuous positive airway pressure on inflammatory, antioxidant, and depression biomarkers in women with obstructive sleep apnea: A randomized controlled trial. Sleep 2019, 42, zsz145. [Google Scholar] [CrossRef] [PubMed]
- Kaminska, M.; O’Sullivan, M.; Mery, V.P.; Lafontaine, A.L.; Robinson, A.; Gros, P.; Martin, J.G.; Benedetti, A.; Kimoff, R.J. Inflammatory markers and BDNF in obstructive sleep apnea (OSA) in Parkinson’s disease (PD). Sleep Med. 2022, 90, 258–261. [Google Scholar] [CrossRef] [PubMed]
- Flores, K.R.; Viccaro, F.; Aquilini, M.; Scarpino, S.; Ronchetti, F.; Mancini, R.; Di Napoli, A.; Scozzi, D.; Ricci, A. Protective role of brain derived neurotrophic factor (BDNF) in obstructive sleep apnea syndrome (OSAS) patients. PLoS ONE 2020, 15, e0227834. [Google Scholar] [CrossRef] [Green Version]
- Kapur, V.K.; Auckley, D.H.; Chowdhuri, S.; Kuhlmann, D.C.; Mehra, R.; Ramar, K.; Harrod, C.G. Clinical practice guideline for diagnostic testing for adult obstructive sleep apnea: An American academy of sleep medicine clinical practice guideline. J. Clin. Sleep Med. 2017, 13, 479–504. [Google Scholar] [CrossRef] [PubMed]
- Smyka, M.; Kosińska-Kaczyńska, K.; Sochacki-Wójcicka, N.; Zgliczyńska, M.; Wielgoś, M. Sleep quality according to the Pittsburgh Sleep Quality Index in over 7000 pregnant women in Poland. Sleep Biol. Rhythm. 2021, 19, 353–360. [Google Scholar] [CrossRef]
- Backhaus, J.; Junghanns, K.; Broocks, A.; Riemann, D.; Hohagen, F. Test-retest reliability and validity of the Pittsburgh Sleep Quality Index in primary insomnia. J. Psychosom. Res. 2002, 53, 737–740. [Google Scholar] [CrossRef] [PubMed]
- Chabowski, M.; Łuczak, J.; Dudek, K.; Jankowska-Polańska, B. Sleep disorders and adherence to inhalation therapy in patients with chronic obstructive pulmonary disease. Adv. Exp. Med. Biol. 2019, 1160, 43–52. [Google Scholar] [CrossRef]
- Mollayeva, T.; Thurairajah, P.; Burton, K.; Mollayeva, S.; Shapiro, C.M.; Colantonio, A. The Pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: A systematic review and meta-analysis. Sleep Med. Rev. 2016, 25, 52–73. [Google Scholar] [CrossRef]
- Staniszewska, A.; Mąka, A.; Religioni, U.; Olejniczak, D. Sleep disturbances among patients with epilepsy. Neuropsychiatr. Dis. Treat. 2017, 13, 1797–1803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smarr, K.L.; Keefer, A.L. Measures of depression and depressive symptoms: Beck Depression Inventory-II (BDI-II), Center for Epidemiologic Studies Depression Scale (CES-D), Geriatric Depression Scale (GDS), Hospital Anxiety and Depression Scale (HADS), and Patient Health Questionn. Arthritis Care Res. 2011, 63 (Suppl. S1), S454–S466. [Google Scholar] [CrossRef]
- Mirghafourvand, M.; Charandabi, S.M.A.; lak, T.B.; Aliasghari, F. Predictors of Depression in Iranian Women with Polycystic Ovarian Syndrome. Community Ment. Health J. 2018, 54, 1274–1283. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Steer, R.A.; Brown, G. Beck depression inventory–II. Psychol. Assess. 1996. Available online: http://www.nctsn.org/content/beck-depression-inventory-second-edition-bdi-ii (accessed on 12 September 2022).
- Dabson, K.S.; MOHAMMAD, K.P. Psychometric characteristics of Beck depression inventory–II in patients with major depressive disorder. Brain Behav. 2007, 11, e2344. [Google Scholar] [CrossRef]
- Wiglusz, M.S.; Landowski, J.; Michalak, L.; Cubała, W.J. Validation of the Polish version of the Beck Depression Inventory in patients with epilepsy. Epilepsy Behav. 2017, 77, 58–61. [Google Scholar] [CrossRef] [PubMed]
- Kokoszka, A.; Cichoń, E.; Obrębski, M.; Kiejna, A.; Rajba, B. Cut-off points for Polish-language versions of depression screening tools among patients with Type 2 diabetes. Prim. Care Diabetes 2020, 14, 663–671. [Google Scholar] [CrossRef]
- Soldatos, C.R.; Dikeos, D.G.; Paparrigopoulos, T.J. Athens Insomnia Scale: Validation of an instrument based on ICD-10 criteria. J. Psychosom. Res. 2000, 48, 555–560. [Google Scholar] [CrossRef]
- Fornal-Pawłowska, M.; Wołyńczyk-Gmaj, D.; Szelenberger, W. Validation of the Polish version of the Athens Insomnia Scale. Psychiatr. Pol. 2011, 45, 211–221. [Google Scholar]
- Fang, Y.-Y.; Luo, M.; Yue, S.; Han, Y.; Zhang, H.-J.; Zhou, Y.-H.; Liu, K.; Liu, H.-G. 7,8-Dihydroxyflavone protects retinal ganglion cells against chronic intermittent hypoxia-induced oxidative stress damage via activation of the BDNF/TrkB signaling pathway. Sleep Breath. 2022, 26, 287–295. [Google Scholar] [CrossRef]
- An, J.R.; Zhao, Y.S.; Luo, L.F.; Guan, P.; Tan, M.; Ji, E.S. Huperzine A, reduces brain iron overload and alleviates cognitive deficit in mice exposed to chronic intermittent hypoxia. Life Sci. 2020, 250, 117573. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Zhao, J.; Qu, Y.; Sun, Q.; Li, T.-T.; Yan, M.-L.; Duan, M.-J.; Li, K.-X.; Wang, Y.-R.; Huang, S.-Y.; et al. Metoprolol prevents neuronal dendrite remodeling in a canine model of chronic obstructive sleep apnea. Acta Pharmacol. Sin. 2020, 41, 620–628. [Google Scholar] [CrossRef]
- Wu, X.; Lu, H.; Hu, L.; Gong, W.; Wang, J.; Fu, C.; Liu, Z.; Li, S. Chronic intermittent hypoxia affects endogenous serotonergic inputs and expression of synaptic proteins in rat hypoglossal nucleus. Am. J. Transl. Res. 2017, 9, 546–557. [Google Scholar] [PubMed]
- Zhang, J.; Guo, X.; Shi, Y.; Ma, J.; Wang, G. Intermittent hypoxia with or without hypercapnia is associated with tumorigenesis by decreasing the expression of brain derived neurotrophic factor and miR-34a in rats. Chin. Med. J. 2014, 127, 43–47. [Google Scholar] [PubMed]
- Xie, H.; Leung, K.-L.; Chen, L.; Chan, Y.-S.; Ng, P.-C.; Fok, T.-F.; Wing, Y.-K.; Ke, Y.; Li, A.M.; Yung, W.-H. Brain-derived neurotrophic factor rescues and prevents chronic intermittent hypoxia-induced impairment of hippocampal long-term synaptic plasticity. Neurobiol. Dis. 2010, 40, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.Q.; Yi, S.; Chen, B.B.; Cui, P.P.; Wang, Y.; Li, Y.Z. mTOR/NF-κB signaling pathway protects hippocampal neurons from injury induced by intermittent hypoxia in rats. Int. J. Neurosci. 2021, 131, 994–1003. [Google Scholar] [CrossRef] [PubMed]
- Turkiewicz, S.; Ditmer, M.; Sochal, M.; Białasiewicz, P.; Strzelecki, D.; Gabryelska, A. Obstructive Sleep Apnea as an Acceleration Trigger of Cellular Senescence Processes through Telomere Shortening. Int. J. Mol. Sci. 2021, 22, 12536. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.; Machaalani, R.; Waters, K.A. Brain-derived neurotrophic factor (BDNF) and TrkB in the piglet brainstem after post-natal nicotine and intermittent hypercapnic hypoxia. Brain Res. 2008, 1232, 195–205. [Google Scholar] [CrossRef]
- Makhout, S.; Vermeiren, E.; Van De Maele, K.; Bruyndonckx, L.; De Winter, B.Y.; Van Hoorenbeeck, K.; Verhulst, S.L.; Van Eyck, A. The Role of Brain-Derived Neurotrophic Factor in Obstructive Sleep Apnea and Endothelial Function in a Pediatric Population With Obesity. Front. Med. 2022, 8, 835515. [Google Scholar] [CrossRef]
- Campos-Rodriguez, F.; Cordero-Guevara, J.; Asensio-Cruz, M.I.; Sanchez-Armengol, A.; Sanchez-Lopez, V.; Arellano-Orden, E.; Gozal, D.; Martinez-Garcia, M.A. Interleukin 6 as a marker of depression in women with sleep apnea. J. Sleep Res. 2021, 30, e13035. [Google Scholar] [CrossRef]
- Gabryelska, A.; Sochal, M. Evaluation of HIF-1 Involvement in the BDNF and ProBDNF Signaling Pathways among Obstructive Sleep Apnea Patients. Int. J. Mol. Sci. 2022, 23, 14876. [Google Scholar] [CrossRef]
- Shah, F.; Forsgren, S.; Holmlund, T.; Levring Jäghagen, E.; Berggren, D.; Franklin, K.A.; Stål, P. Neurotrophic factor BDNF is upregulated in soft palate muscles of snorers and sleep apnea patients. Laryngoscope Investig. Otolaryngol. 2019, 4, 174–180. [Google Scholar] [CrossRef] [Green Version]
- Svanborg, E. Upper airway nerve lesions in obstructive sleep apnea. Am. J. Respir. Crit. Care Med. 2001, 164, 187–189. [Google Scholar] [CrossRef] [PubMed]
- Shah, F.; Holmlund, T.; Jäghagen, E.L.; Berggren, D.; Franklin, K.; Forsgren, S.; Stål, P. Axon and Schwann Cell Degeneration in Nerves of Upper Airway Relates to Pharyngeal Dysfunction in Snorers and Patients With Sleep Apnea. Chest 2018, 154, 1091–1098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arslan, B.; Şemsi, R.; İriz, A.; Dinçel, A.S. The evaluation of serum brain-derived neurotrophic factor and neurofilament light chain levels in patients with obstructive sleep apnea syndrome. Laryngoscope Investig. Otolaryngol. 2021, 6, 1466–1473. [Google Scholar] [CrossRef] [PubMed]
- Targa, A.; Dakterzada, F.; Benítez, I.; López, R.; Pujol, M.; Dalmases, M.; Arias, A.; Sánchez-de-la-Torre, M.; Zetterberg, H.; Blennow, K.; et al. Decrease in sleep depth is associated with higher cerebrospinal fluid neurofilament light levels in patients with Alzheimer’s disease. Sleep 2021, 44, zsaa147. [Google Scholar] [CrossRef] [PubMed]
- Gabryelska, A.; Szmyd, B.; Panek, M.; Szemraj, J.; Kuna, P.; Białasiewicz, P. Serum hypoxia-inducible factor-1α protein level as a diagnostic marker of obstructive sleep apnea. Pol. Arch. Intern. Med. 2020, 130, 158–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabryelska, A.; Szmyd, B.; Szemraj, J.; Stawski, R.; Sochal, M.; Białasiewicz, P. Patients with obstructive sleep apnea present with chronic upregulation of serum HIF-1α protein. J. Clin. sleep Med. 2020, 16, 1761–1768. [Google Scholar] [CrossRef]
- Gabryelska, A.; Stawski, R.; Sochal, M. Influence of one-night CPAP therapy on the changes of HIF-1α protein in OSA patients—A pilot study. J. Sleep Res. 2020, 29, e12995. [Google Scholar] [CrossRef]
- Lu, D.; Li, N.; Yao, X.; Zhou, L. Potential inflammatory markers in obstructive sleep apnea-hypopnea syndrome. Bosn. J. basic Med. Sci. 2017, 17, 47–53. [Google Scholar] [CrossRef] [Green Version]
- Qaid, E.Y.A.; Zulkipli, N.N.; Zakaria, R.; Ahmad, A.H.; Othman, Z.; Muthuraju, S.; Sasongko, T.H. The role of mTOR signalling pathway in hypoxia-induced cognitive impairment. Int. J. Neurosci. 2021, 131, 482–488. [Google Scholar] [CrossRef]
- More, C.E.; Papp, C.; Harsanyi, S.; Gesztelyi, R.; Mikaczo, A.; Tajti, G.; Kardos, L.; Seres, I.; Lorincz, H.; Csapo, K.; et al. Altered irisin/BDNF axis parallels excessive daytime sleepiness in obstructive sleep apnea patients. Respir. Res. 2019, 20, 67. [Google Scholar] [CrossRef] [Green Version]
- Fan, T.-T.; Chen, W.-H.; Shi, L.; Lin, X.; Tabarak, S.; Chen, S.-J.; Que, J.-Y.; Bao, Y.-P.; Tang, X.-D.; Shi, J.; et al. Objective sleep duration is associated with cognitive deficits in primary insomnia: BDNF may play a role. Sleep 2019, 42, zsy192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mikoteit, T.; Brand, S.; Eckert, A.; Holsboer-Trachsler, E.; Beck, J. Brain-derived neurotrophic factor is a biomarker for subjective insomnia but not objectively assessable poor sleep continuity. J. Psychiatr. Res. 2019, 110, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Giese, M.; Unternährer, E.; Hüttig, H.; Beck, J.; Brand, S.; Calabrese, P.; Holsboer-Trachsler, E.; Eckert, A. BDNF: An indicator of insomnia? Mol. Psychiatry 2014, 19, 151–152. [Google Scholar] [CrossRef] [PubMed]
- Backhaus, J.; Junghanns, K.; Hohagen, F. Sleep disturbances are correlated with decreased morning awakening salivary cortisol. Psychoneuroendocrinology 2004, 29, 1184–1191. [Google Scholar] [CrossRef]
- Riemann, D.; Klein, T.; Rodenbeck, A.; Feige, B.; Horny, A.; Hummel, R.; Weske, G.; Al-Shajlawi, A.; Voderholzer, U. Nocturnal cortisol and melatonin secretion in primary insomnia. Psychiatry Res. 2002, 113, 17–27. [Google Scholar] [CrossRef]
- Claro, A.E.; Palanza, C.; Mazza, M.; Rizzi, A.; Tartaglione, L.; Marano, G.; Muti-Schuenemann, G.; Rigoni, M.; Muti, P.; Pontecorvi, A.; et al. Why do we not reverse the path? Stress can cause depression, reduction of brain-derived neurotrophic factor and increased inflammation. World J. Psychiatry 2022, 12, 1264–1267. [Google Scholar] [CrossRef]
- Gabryelska, A.; Turkiewicz, S.; Karuga, F.F.; Sochal, M.; Strzelecki, D.; Białasiewicz, P. Disruption of Circadian Rhythm Genes in Obstructive Sleep Apnea Patients—Possible Mechanisms Involved and Clinical Implication. Int. J. Mol. Sci. 2022, 23, 709. [Google Scholar] [CrossRef]
- Gabryelska, A.; Sochal, M.; Turkiewicz, S.; Białasiewicz, P. Relationship between HIF-1 and Circadian Clock Proteins in Obstructive Sleep Apnea Patients—Preliminary Study. J. Clin. Med. 2020, 9, 1599. [Google Scholar] [CrossRef]
- Cain, S.W.; Chang, A.-M.; Vlasac, I.; Tare, A.; Anderson, C.; Czeisler, C.A.; Saxena, R. Circadian Rhythms in Plasma Brain-derived Neurotrophic Factor Differ in Men and Women. J. Biol. Rhythm. 2017, 32, 75–82. [Google Scholar] [CrossRef]
- Wall, A.M.; Corcoran, A.E.; O’Halloran, K.D.; O’Connor, J.J. Effects of prolyl-hydroxylase inhibition and chronic intermittent hypoxia on synaptic transmission and plasticity in the rat CA1 and dentate gyrus. Neurobiol. Dis. 2014, 62, 8–17. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Control Group (n = 30) | OSA Group (n = 30) | p-Value | ||
|---|---|---|---|---|
| Demographic data | Sex [M (%)/F(%)] | 17 (56.7%)/13(43.3%) | 27 (90%)/3(10%) | 0.007 |
| Age [years] | 46.5 (36.8–58.5) | 59.5 (48.8–67.0) | <0.001 | |
| BMI [kg/m2] | 27.6 (24.3–30.7) | 36.0 (31.2–39.4) | <0.001 | |
| Polysomnography | TST (h) | 6.0 ± 0.9 | 5.9 ± 1.1 | 0.994 |
| REM (h) | 1.2 ± 0.5 | 1.2 ± 0.6 | 0.408 | |
| NREM (h) | 4.8 ± 0.7 | 4.7 ± 0.9 | 0.525 | |
| Sleep Efficiency (%) | 85.2 (76.4–91.1) | 83.8 (70.3–87.8) | 0.412 | |
| Sleep onset latency (min) | 19.5 (8.1–31.8) | 15.8 (7.4–29.4) | 0.647 | |
| Sleep Maintenance Efficiency (%) | 93.5 (82.6–97.4) | 89.1 (77.2–92.2) | 0.205 | |
| REM latency (min) | 102.5 (80.1–144.0) | 97.3 (56.4–164.3) | 0.595 | |
| Arousal index (events/h) | 9.4 (6.0–14.2) | 24.8 (18.3–34.5) | <0.001 | |
| AHI (events/h) | 2.5 (1.3–4.2) | 49.0 (37.5–71.3) | <0.001 | |
| AHI in REM sleep (events/h) | 4.0 ± 5.2 | 48.4 ± 25.9 | <0.001 | |
| AHI in NREM sleep (events/h) | 1.6 (1.1–3.7) | 47.6 (36.9–69.0) | <0.001 | |
| Total nuber of desaturations | 10.5 (6.3–18.5) | 248.0 (203.0–383.5) | <0.001 | |
| Desaturation Index | 2.5 ± 1.8 | 56.6 ± 26.3 | <0.001 | |
| Mean SpO2 of desaturations during sleep | 91.0 (90.0–92.4) | 86.0 (81.9–88.5) | <0.001 | |
| Questionnaires | AIS | 10.0 (7.0–14.0) | 11.0 (7.5–13.5) | 0.902 |
| PSQI | 10.0 (7.0–11.0) | 11.0 (7.0–13.0) | 0.378 | |
| Subjective sleep quality (component 1 PSQI) | 2.0 (1.0–2.0) | 2.0 (1.0–2.0) | 0.482 | |
| Sleep latency (component 2 PSQI) | 1.0 (1.0–2.0) | 1.0 (1.0–2.0) | 0.821 | |
| Sleep duration (component 3 PSQI) | 1.0 (0.0–2.0) | 2.0 (1.0–2.5) | 0.200 | |
| Sleep efficiency (component 4 PSQI) | 1.0 (0.0–2.0) | 1.0 (0.0–3.0) | 0.594 | |
| Sleep disturbance (component 5 PSQI) | 1.0 (1.0–2.0) | 2.0 (1.0–2.0) | 0.029 | |
| Use of sleep medication (component 6 PSQI) [yes (%)/no (%)] | 24(80%)/6(20%) | 22(73.3%)/8(27.7%) | 0.542 | |
| Daytime dysfunction (component 7 PSQI) | 2.0 (1.0–3.0) | 1.0 (1.0–2.5) | 0.452 | |
| Reported time spent lying in bed in PSQI (min) | 420.0 (390.0–540.0) | 450.0 (360.0–525.0) | 0.521 | |
| Subjective Sleep Efficiency in PSQI (%) | 79.9 ± 15.3 | 76.6 ± 15.4 | 0.403 | |
| BDI | 14.0 (7.0–20.0) | 11.0 (8.0–16.5) | 0.885 | |
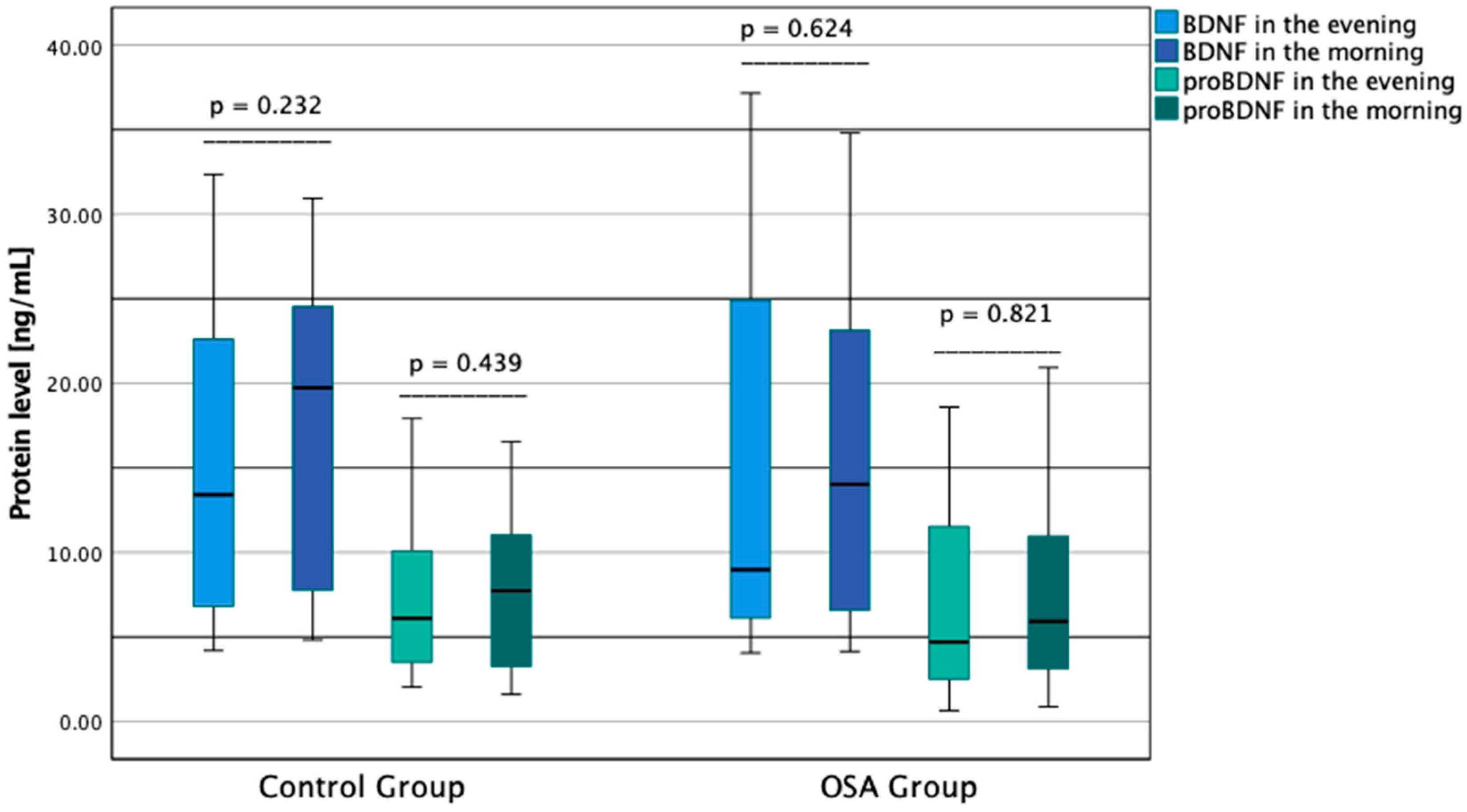
| Protein Concentration | BDNF evening [ng/mL] | 13.4 (6.8–22.8) | 9.0 (6.1–25.2) | 0.442 |
| BDNF morning [ng/mL] | 19.7 (7.7–24.7) | 9.2 (6.6–23.4) | 0.626 | |
| proBDNF evening [ng/mL] | 6.1 (3.5–10.1) | 4.7 (2.5–11.8) | 0.559 | |
| proBDNF morning [ng/mL] | 7.7 (3.2–11.2) | 5.9 (3.0–11.1) | 0.496 | |
| OSA Group (n = 30) | OSA Group (n = 30) | OSA Group (n = 30) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| AIS (−) Group (≤5; n = 6) | AIS (+) Group (>5; n = 24) | p-Value | PSQI (−) Group (≤5; n = 5) | PSQI (+) Group (>5; n = 25) | p-Value | BDI (−) Group (≤19; n = 25) | BDI (+) Group (>19; n = 5) | p-Value | ||
| Demographic data | Sex [M (%)/F(%)] | 6 (100%)/0 (0.0%) | 21 (87.5%)/3(12.5%) | 0.361 | 5 (100%)/0(0.0%) | 22 (88.0%)/3 (12.0%) | 0.414 | 24 92.0%)/1(8.0%) | 2(40.0%)/3(60.0%) | 0.064 |
| Age [years] | 57.7 ± 10.1 | 57.5± 10.2 | 0.979 | 56.4 ± 10.7 | 57.8 ± 10.1 | 0.780 | 56.7 ±10.0 | 61.8 ± 9.8 | 0.307 | |
| BMI [kg/m2] | 35.5 ± 4.5 | 35.6 ± 5.7 | 0.968 | 36.1 ± 4.8 | 35.5 ± 5.6 | 0.835 | 35.2 ± 5.6 | 37.5 ± 3.8 | 0.399 | |
| Polysomnography | TST (h) | 6.1 ± 0.9 | 5.8 ± 1.2 | 0.575 | 6.4 ± 0.8 | 5.8 ± 1.2 | 0.284 | 5.9 ± 1.1 | 5.7 ± 1.1 | 0.701 |
| REM (h) | 1.2 ± 0.7 | 1.2 ± 0.6 | 0.763 | 1.4 ± 0.7 | 1.1 ± 0.6 | 0.399 | 2.8 ± 1.6 | 1.5 ± 1.0 | 0.205 | |
| NREM (h) | 4.9 ± 0.6 | 4.7 ±0.9 | 0.613 | 5.0 ± 0.6 | 4.7 ± 0.9 | 0.439 | 4.8 ± 0.9 | 4.2 ± 0.7 | 0.170 | |
| Sleep Efficiency (%) | 80.3 ± 15.3 | 79.2 ± 14.2 | 0.894 | 87.2 ± 8.1 | 11.8 ± 11.7 | 0.305 | 80.0 ± 15.1 | 77.9 ± 11.3 | 0.808 | |
| Sleep onset latency (min) | 13.0 (5.5–27.4) | 16.8 (8.1–30.1) | 0.679 | 11.1 ± 5.9 | 23.9 ± 24.5 | 0.029 | 15.5 (7.3–25.3) | 30.5 (9.8–78.5) | 0.033 | |
| Sleep Maintenance Efficiency (%) | 88.7 (74.1–94.9) | 89.1 (76.7–92.2) | 0.808 | 91.1 ± 5.1 | 23.9 ± 24.7 | 0.115 | 89.1 (77.2–93.7) | 88.0 (73.1–92.4) | 0.992 | |
| REM latency (min) | 86.8 ± 33.0 | 120.2 ± 70.22 | 0.107 | 81.5 ± 33.8 | 68.7 ± 119.9 | 0.085 | 117.0 ± 69.1 | 96.0 ± 44.1 | 0.521 | |
| arousal index (events/h) | 25.9 (23.0–28.2) | 23.6 (16.6–36.5) | 0.710 | 24.7 ± 1.9 | 29.2 ± 18.2 | 0.235 | 29.2 ± 17.3 | 24.6 ± 13.9 | 0.573 | |
| AHI | 48.3 (37.1–64.0) | 49.7 (37.7–73.2) | 0.609 | 46.3 (36.6–63.3) | 51.5 (38.1–72.2) | 0.519 | 53.0 ± 19.6 | 67.0 ± 34.9 | 0.213 | |
| AHI in REM sleep (events/h) | 42.7 (30.8–65.8) | 47.4 (27.2–65.4) | 0.636 | 39.5 (22.5–56.2) | 50.9 (27.2–65.9) | 0.407 | 45.2 ± 22.9 | 64.3 ± 36.5 | 0.134 | |
| AHI in NREM sleep (events/h) | 46.2 (33.0–64.2) | 47.6 (37.9–70.6) | 0.557 | 37.3 (32.7–67.4) | 47.6 (38.0–69.8) | 0.471 | 52.0 ± 20.5 | 67.8 ± 35.8 | 0.177 | |
| Total number of desaturations | 320.0 (249.5–498.5) | 211.0 (188.5–383.5) | 0.707 | 347.0 (235.0–377.0) | 229.5 (194.8–381.3) | 0.605 | 235.0 (188.5–363.0) | 318.0 (215.8–727.0) | 0.254 | |
| Desaturation Index | 53.3 ± 15.5 | 57.5 ± 28.5 | 0.730 | 51.7 ± 16.8 | 57.6 ± 27.9 | 0.653 | 54.8 ± 25.1 | 65.9 ± 33.1 | 0.398 | |
| Mean SpO2 of desaturations during sleep | 85.4 (84.4–86.9) | 86.7 (81.2–88.8) | 0.376 | 85.1 (83.9–87.8) | 86.4 (81.3–88.7) | 0.422 | 86.0 (82.5–88.2) | 85.4 (81.6–93.5) | 0.700 | |
| Questionaires | AIS | N/A | N/A | N/A | 2.5 (0.5–3.8) | 12.0 (8.0–14.0) | <0.001 | 10.0 (6.3–13.0) | 14.0 (10.5–15.0) | 0.046 |
| PSQI | 5.0 (2.5–8.5) | 11.0 (7.5–13.0) | 0.001 | N/A | N/A | N/A | 10.5 (6.3–12.0) | 13.0 (10.0–14.5) | 0.090 | |
| Sleep latency (component 2 PSQI) | 0.0 (0.0–0.5) | 2.0 (1.0–2.0) | <0.001 | N/A | N/A | N/A | 2.0 (1.0–2.0) | 2.0 (1.0–2.5) | 0.356 | |
| Sleep duration (component 3 PSQI) | 1.0 (0.5–1.0) | 2.0 (1.0–2.0) | 0.014 | N/A | N/A | N/A | 1.0 (1.0–2.0) | 2.0 (0.5–2.5) | 0.690 | |
| Sleep efficiency (component 4 PSQI) | 0.0 (0.0–0.5) | 2.0 (1.0–3.0) | <0.001 | N/A | N/A | N/A | 2.0 (1.0–2.8) | 2.0 (1.0–2.5) | 0.792 | |
| Sleep disturbance (component 5 PSQI) | 0.0 (0.0–1.0) | 1.5 (0.0–3.0) | 0.044 | N/A | N/A | N/A | 1.0 (0.0–2.8) | 2.0 (0.5–3.0) | 0.385 | |
| Use of sleep medication (component 6 PSQI) [yes (%)/no (%)] | 6(100%)/0(0%) | 18(75%)/6(25%) | 0.171 | N/A | N/A | N/A | 20(83.3%)/4(16.7%) | 4(66.7%)/2(33.3%) | 0.361 | |
| Daytime dysfunction (component 7 PSQI) | 0.0 (0.0–2.5) | 0.0 (0.0–0.8) | 0.327 | N/A | N/A | N/A | 0.0 (0.0–0.0) | 1.0 (0.0–2.0) | 0.327 | |
| Sleep latency (component 2 PSQI) | 1.0 (0.5–3.0) | 1.0 (1.0–2.0) | 0.973 | N/A | N/A | N/A | 1.0 (1.0–2.0) | 2.0 (1.5–3.0) | 0.127 | |
| Reported time spent lying in bed in PSQI (min) | 534.0 ± 57.7 | 425.4 ± 99.2 | 0.027 | N/A | N/A | N/A | 77.4 ± 15.3 | 72.6 ± 17.1 | 0.726 | |
| Subjective Sleep Efficiency in PSQI (%) | 90.2 ± 13.8 | 73.7 ± 14.4 | 0.027 | N/A | N/A | N/A | 441.0 ± 105.2 | 459.0 ± 89.8 | 0.541 | |
| BDI | 7.0 (2.0–10.5) | 14.0 (8.5–19.5) | 0.013 | 9.0 (5.0–9.0) | 13.5 (8.0–18.3) | 0.033 | N/A | N/A | N/A | |
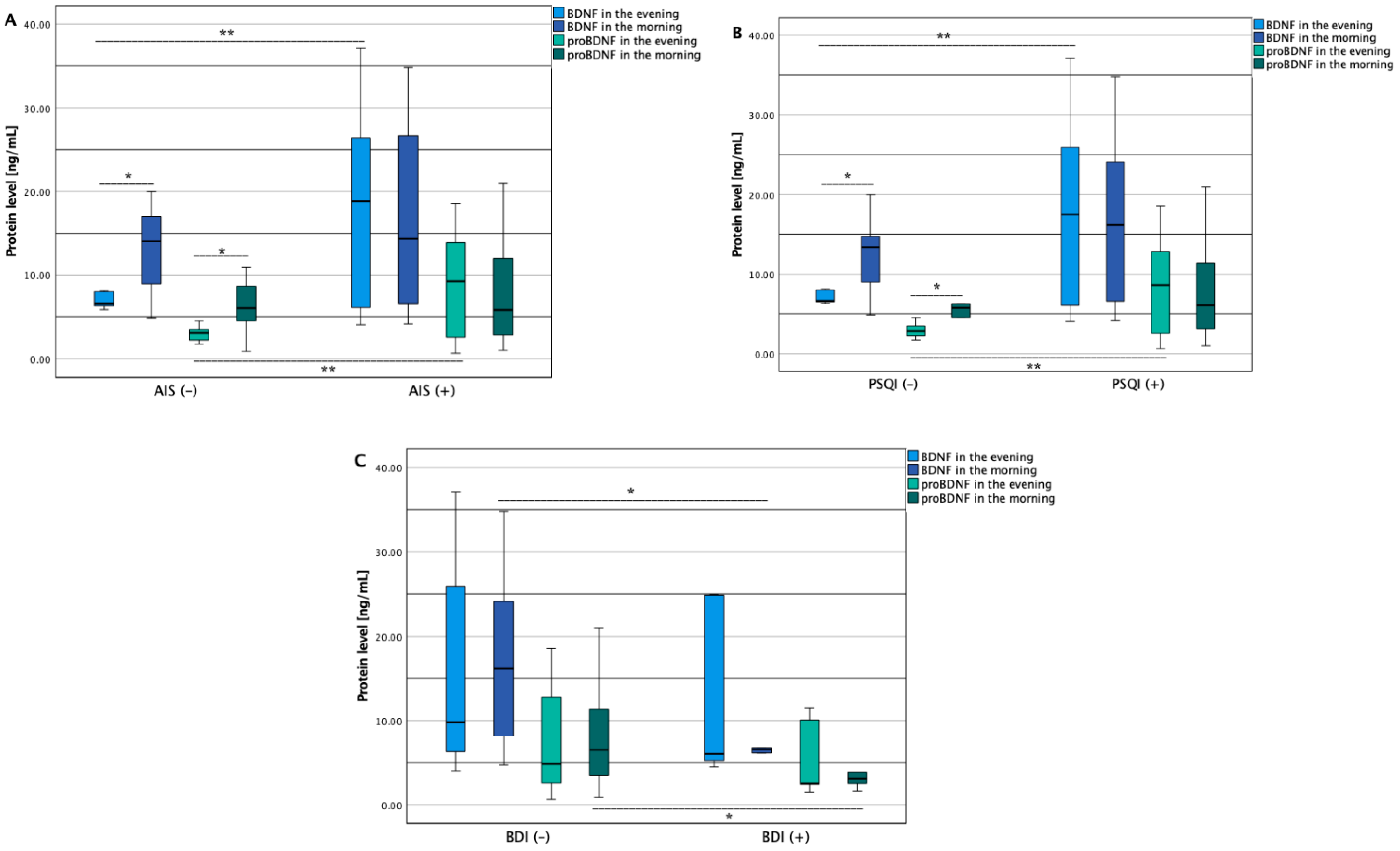
| Protein Concentration | BDNF evening [ng/mL] | 6.6 (6.2–8.1) | 18.8 (6.1–26.7) | <0.001 * | 6.6 (6.4–8.1) | 17.5 (6.0–26.4) | <0.001 * | 9.8 (6.3–26.4) | 6.1 (4.9–24.9) | 0.303 |
| BDNF morning [ng/mL] | 14.0 (8.0–17.8) | 14.4 (6.6–28.0) | 0.277 | 13.4 (6.9–17.3) | 16.2 (6.6–26.7) | 0.222 | 16.2 (8.0–26.7) | 6.6 (5.2–14.3) | 0.047 ** | |
| proBDNF evening [ng/mL] | 3.1 (2.1–3.8) | 9.7 (2.5–28.0) | <0.001 * | 2.9 (2.0–4.0) | 8.6 (2.5–13.9) | <0.001 * | 4.9 (2.6–13.9) | 2.6 (2.0–10.8) | 0.388 | |
| proBDNF morning [ng/mL] | 6.0 (3.6–9.2) | 5.8 (2.7–12.3) | 0.630 | 5.8 (2.7–8.6) | 6.1 (2.9–12.0) | 0.504 | 7.8 ± 5.1 | 3.5 ± 1.7 | 0.003 ** | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gabryelska, A.; Turkiewicz, S.; Ditmer, M.; Karuga, F.F.; Strzelecki, D.; Białasiewicz, P.; Sochal, M. BDNF and proBDNF Serum Protein Levels in Obstructive Sleep Apnea Patients and Their Involvement in Insomnia and Depression Symptoms. J. Clin. Med. 2022, 11, 7135. https://doi.org/10.3390/jcm11237135
Gabryelska A, Turkiewicz S, Ditmer M, Karuga FF, Strzelecki D, Białasiewicz P, Sochal M. BDNF and proBDNF Serum Protein Levels in Obstructive Sleep Apnea Patients and Their Involvement in Insomnia and Depression Symptoms. Journal of Clinical Medicine. 2022; 11(23):7135. https://doi.org/10.3390/jcm11237135
Chicago/Turabian StyleGabryelska, Agata, Szymon Turkiewicz, Marta Ditmer, Filip Franciszek Karuga, Dominik Strzelecki, Piotr Białasiewicz, and Marcin Sochal. 2022. "BDNF and proBDNF Serum Protein Levels in Obstructive Sleep Apnea Patients and Their Involvement in Insomnia and Depression Symptoms" Journal of Clinical Medicine 11, no. 23: 7135. https://doi.org/10.3390/jcm11237135
APA StyleGabryelska, A., Turkiewicz, S., Ditmer, M., Karuga, F. F., Strzelecki, D., Białasiewicz, P., & Sochal, M. (2022). BDNF and proBDNF Serum Protein Levels in Obstructive Sleep Apnea Patients and Their Involvement in Insomnia and Depression Symptoms. Journal of Clinical Medicine, 11(23), 7135. https://doi.org/10.3390/jcm11237135