
Age, Sex and Previous Comorbidities as Risk Factors Not Associated with SARS-CoV-2 Infection for Long COVID-19: A Systematic Review and Meta-Analysis
 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy and Selection Criteria
2.2. Screening Process, Study Selection, and Data Extraction
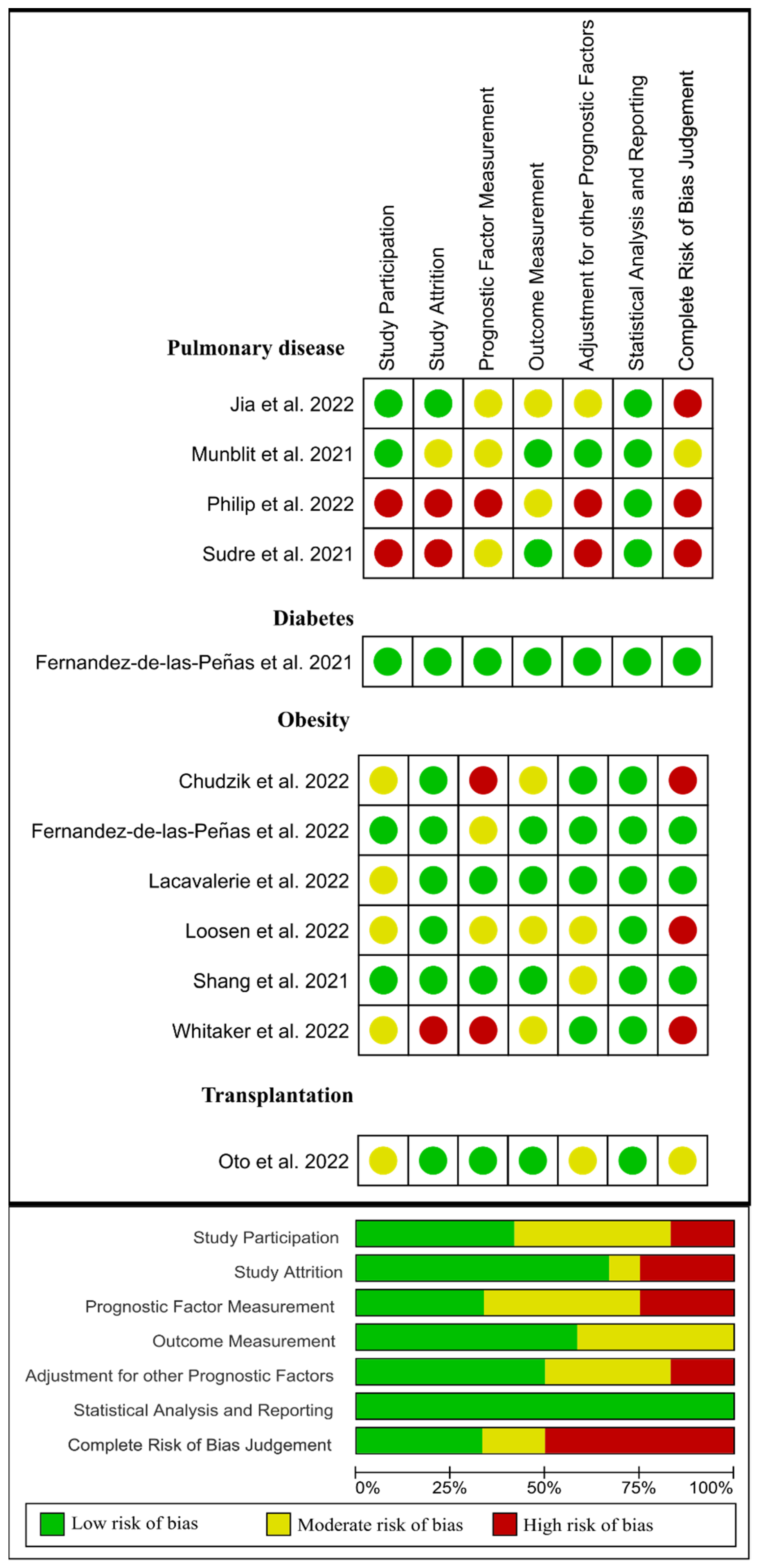
2.3. Risk of Bias
2.4. Data Synthesis
3. Results
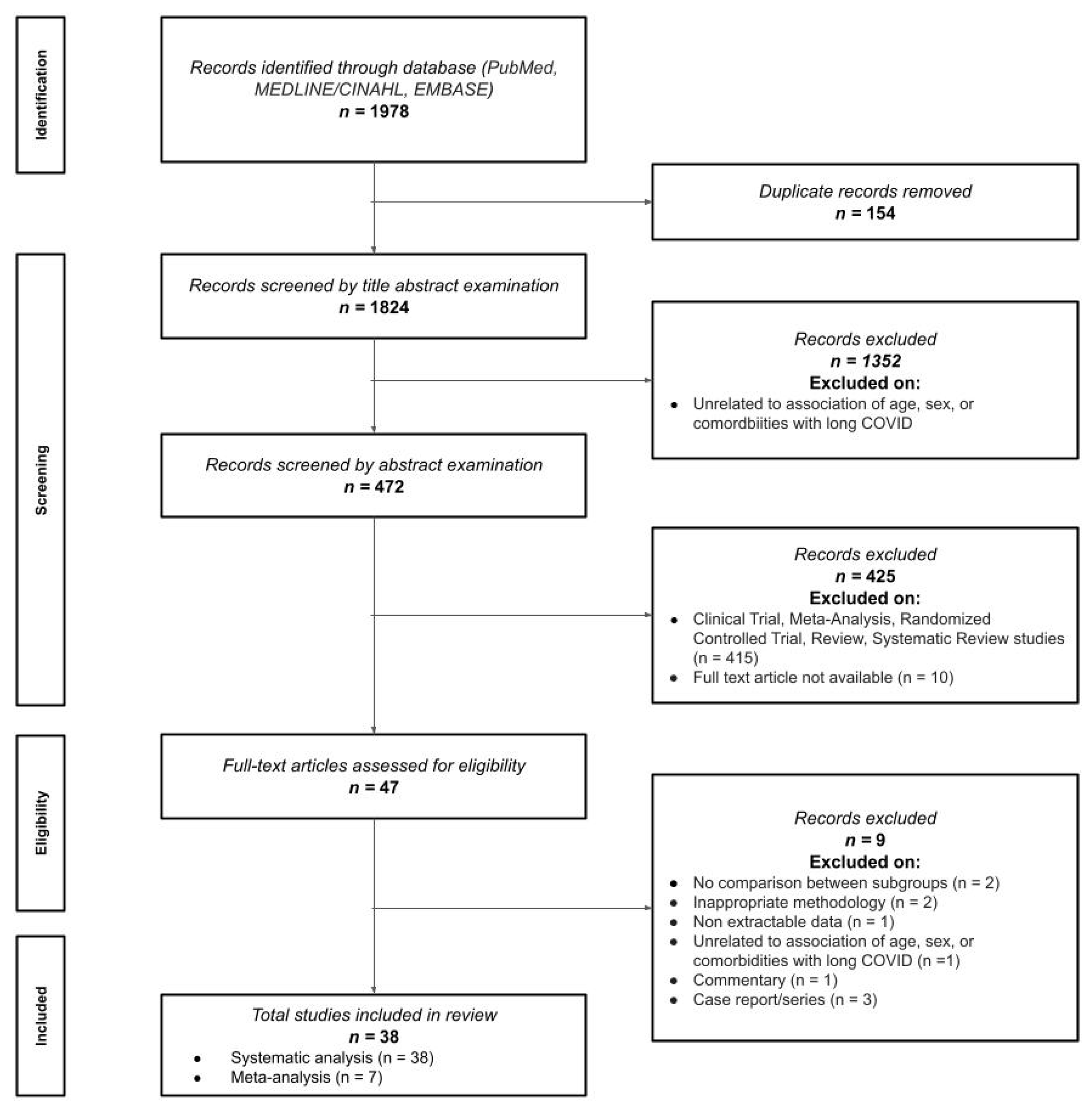
3.1. Study Selection
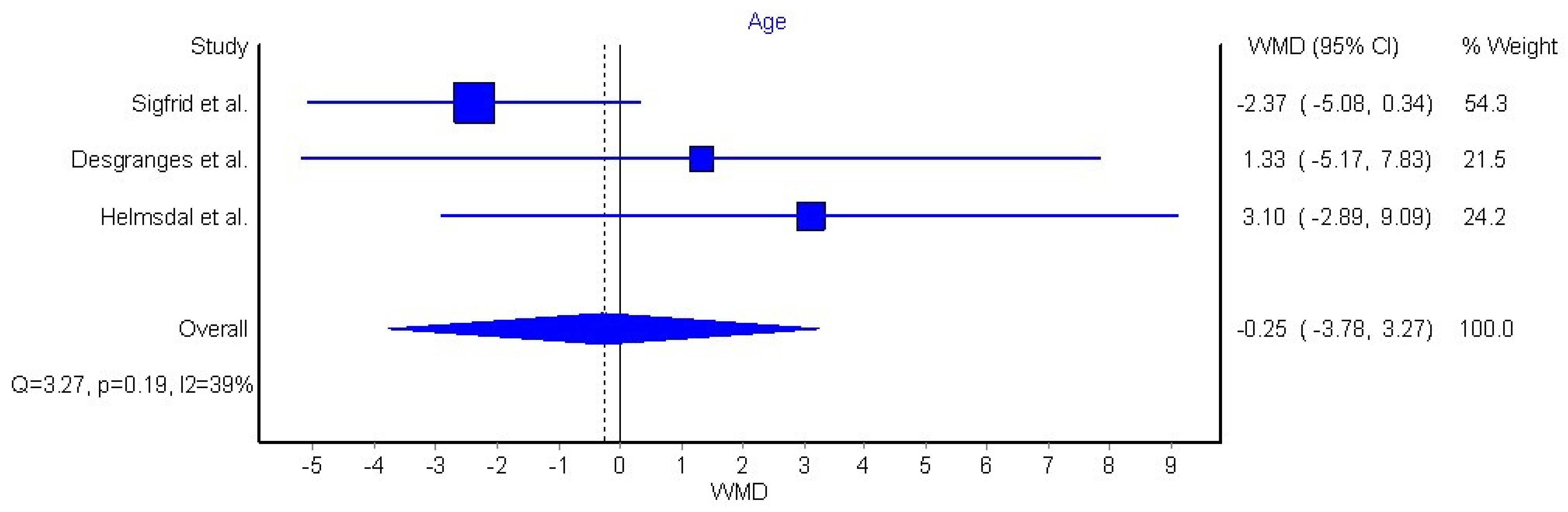
3.2. Age and Post-COVID-19 Condition
3.3. Sex and Post-COVID-19 Condition
3.4. Medical Comorbidities and Post-COVID-19 Condition
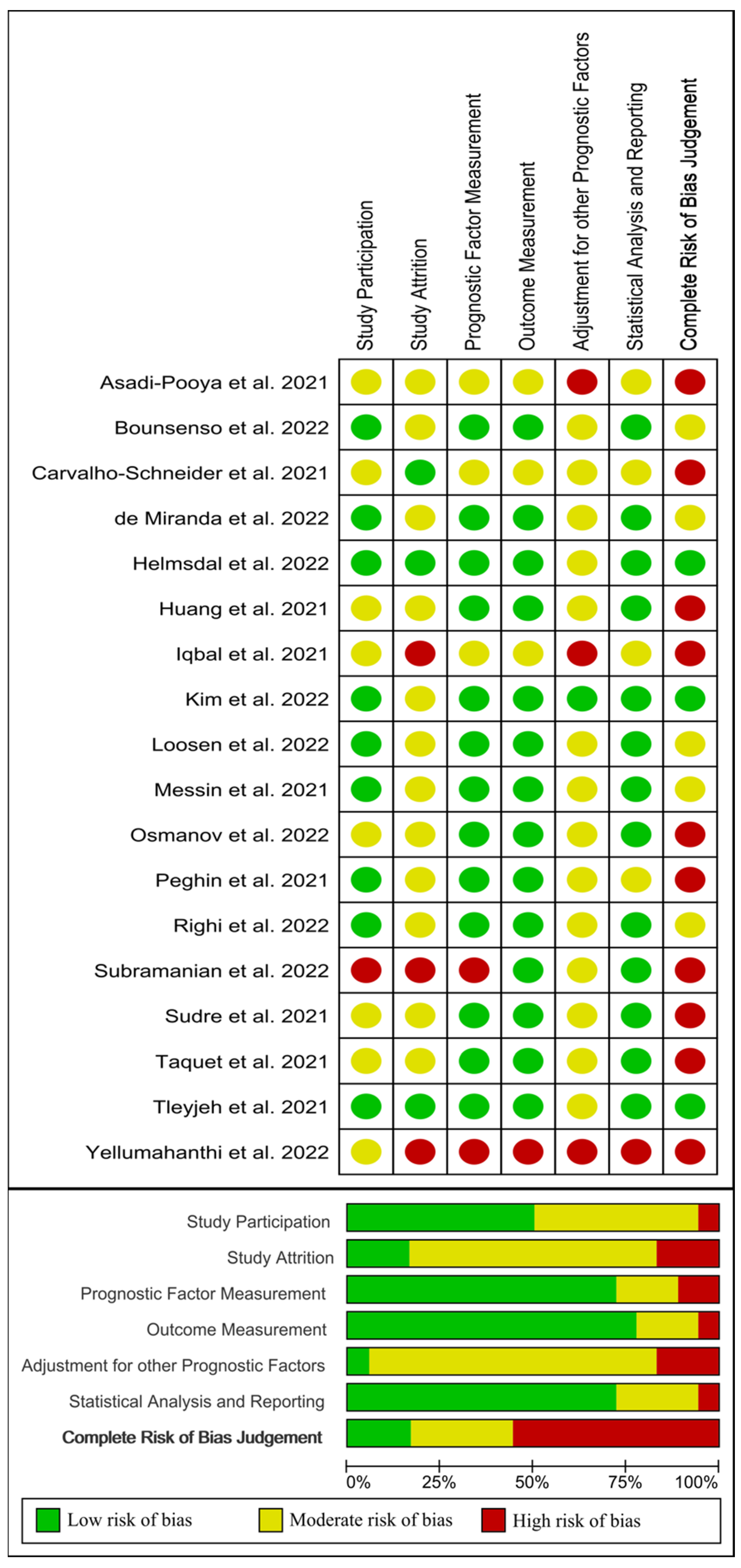
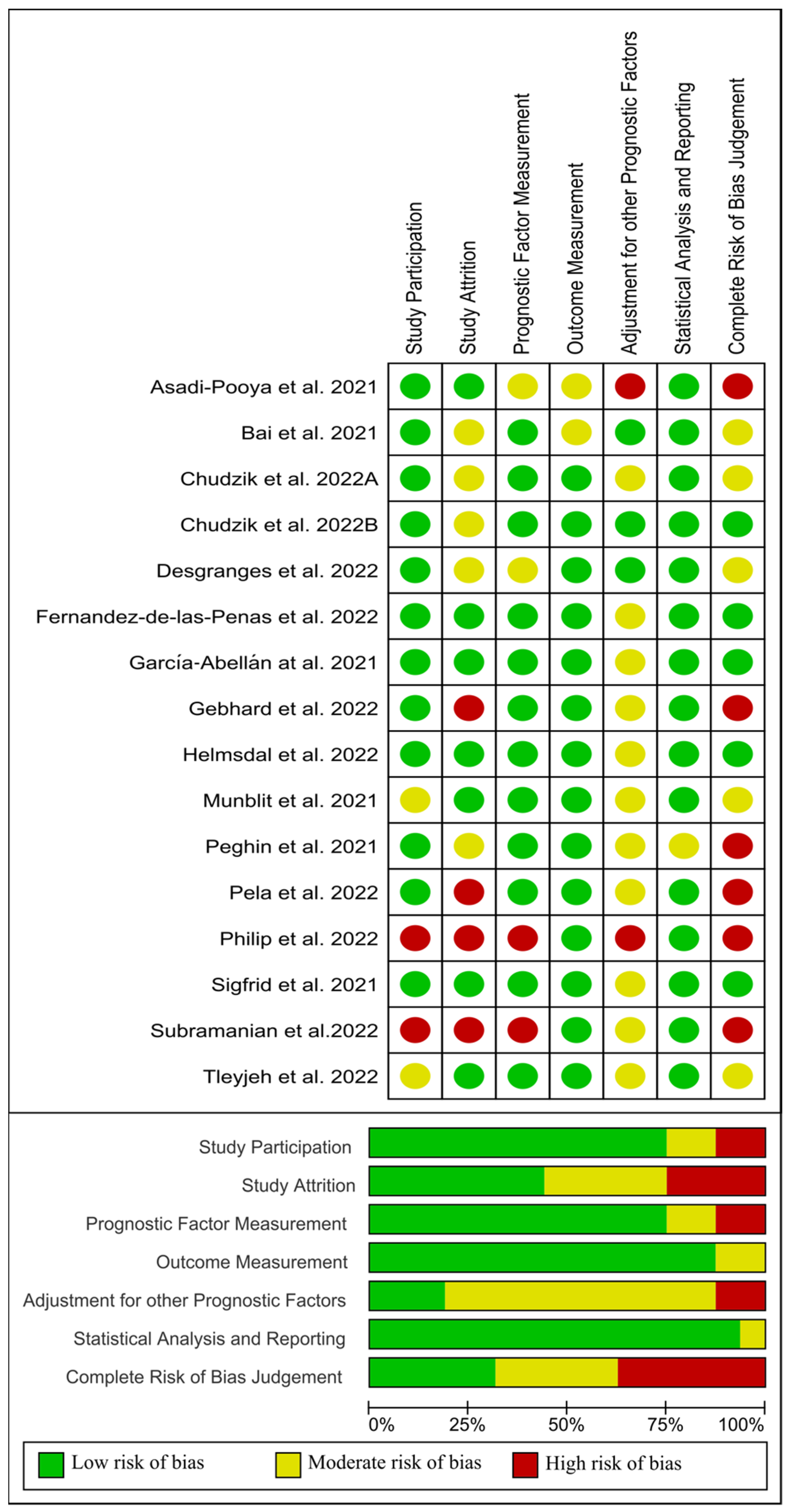
3.5. Risk of Bias
4. Discussion
4.1. Old Age and Long COVID-19
4.2. Female Sex and Long COVID-19
4.3. Medical Comorbidities and Long COVID-19
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Fernández-de-Las-Peñas, C. Long COVID: Current Definition. Infection 2022, 50, 285–286. [Google Scholar] [CrossRef] [PubMed]
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V. A Clinical Case Definition of Post-COVID-19 Condition by a Delphi Consensus. Lancet Infect. Dis. 2022, 22, e102–e107. [Google Scholar] [CrossRef] [PubMed]
- Han, Q.; Zheng, B.; Daines, L.; Sheikh, A. Long-Term Sequelae of COVID-19: A Systematic Review and Meta-Analysis of One-Year Follow-Up Studies on Post-COVID Symptoms. Pathogens 2022, 11, 269. [Google Scholar] [CrossRef]
- Fernández-de-Las-Peñas, C.; Palacios-Ceña, D.; Gómez-Mayordomo, V.; Florencio, L.L.; Cuadrado, M.L.; Plaza-Manzano, G.; Navarro-Santana, M. Prevalence of Post-COVID-19 Symptoms in Hospitalized and Non-Hospitalized COVID-19 Survivors: A Systematic Review and Meta-Analysis. Eur. J. Intern. Med. 2021, 92, 55–70. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Haupert, S.R.; Zimmermann, L.; Shi, X.; Fritsche, L.G.; Mukherjee, B. Global Prevalence of Post COVID-19 Condition or Long COVID: A Meta-Analysis and Systematic Review. J. Infect. Dis. 2022, 226, 1593–1607. [Google Scholar] [CrossRef] [PubMed]
- Yong, S.J. Long COVID or Post-COVID-19 Syndrome: Putative Pathophysiology, Risk Factors, and Treatments. Infect. Dis. 2021, 53, 737–754. [Google Scholar] [CrossRef] [PubMed]
- Crook, H.; Raza, S.; Nowell, J.; Young, M.; Edison, P. Long Covid-Mechanisms, Risk Factors, and Management. BMJ 2021, 374, n1648. [Google Scholar] [CrossRef]
- Akbarialiabad, H.; Taghrir, M.H.; Abdollahi, A.; Ghahramani, N.; Kumar, M.; Paydar, S.; Razani, B.; Mwangi, J.; Asadi-Pooya, A.A.; Malekmakan, L.; et al. Long COVID, a Comprehensive Systematic Scoping Review. Infection 2021, 49, 1163–1186. [Google Scholar] [CrossRef]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-Acute COVID-19 Syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef]
- Iqbal, F.M.; Lam, K.; Sounderajah, V.; Clarke, J.M.; Ashrafian, H.; Darzi, A. Characteristics and Predictors of Acute and Chronic Post-COVID Syndrome: A Systematic Review and Meta-Analysis. eClinicalMedicine 2021, 36, 100899. [Google Scholar] [CrossRef]
- Maglietta, G.; Diodati, F.; Puntoni, M.; Lazzarelli, S.; Marcomini, B.; Patrizi, L.; Caminiti, C. Prognostic Factors for Post-COVID-19 Syndrome: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 1541. [Google Scholar] [CrossRef] [PubMed]
- Thompson, E.J.; Williams, D.M.; Walker, A.J.; Mitchell, R.E.; Niedzwiedz, C.L.; Yang, T.C.; Huggins, C.F.; Kwong, A.S.F.; Silverwood, R.J.; Di Gessa, G.; et al. Long COVID Burden and Risk Factors in 10 UK Longitudinal Studies and Electronic Health Records. Nat. Commun. 2022, 13, 3528. [Google Scholar] [CrossRef] [PubMed]
- Overview|COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19|Guidance|NICE. Available online: https://www.nice.org.uk/guidance/ng188 (accessed on 17 October 2022).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Riley, R.D.; Moons, K.G.M.; Snell, K.I.E.; Ensor, J.; Hooft, L.; Altman, D.G.; Hayden, J.; Collins, G.S.; Debray, T.P.A. A Guide to Systematic Review and Meta-Analysis of Prognostic Factor Studies. BMJ 2019, 364, k4597. [Google Scholar] [CrossRef] [Green Version]
- Hayden, J.A.; van der Windt, D.A.; Cartwright, J.L.; Côté, P.; Bombardier, C. Assessing Bias in Studies of Prognostic Factors. Ann. Intern. Med. 2013, 158, 280–286. [Google Scholar] [CrossRef]
- Grooten, W.J.A.; Tseli, E.; Äng, B.O.; Boersma, K.; Stålnacke, B.-M.; Gerdle, B.; Enthoven, P. Elaborating on the Assessment of the Risk of Bias in Prognostic Studies in Pain Rehabilitation Using QUIPS-Aspects of Interrater Agreement. Diagn. Progn. Res. 2019, 3, 5. [Google Scholar] [CrossRef] [Green Version]
- Tosato, M.; Carfì, A.; Martis, I.; Pais, C.; Ciciarello, F.; Rota, E.; Tritto, M.; Salerno, A.; Zazzara, M.B.; Martone, A.M.; et al. Prevalence and Predictors of Persistence of COVID-19 Symptoms in Older Adults: A Single-Center Study. J. Am. Med. Dir. Assoc. 2021, 22, 1840–1844. [Google Scholar] [CrossRef]
- Vanichkachorn, G.; Newcomb, R.; Cowl, C.T.; Murad, M.H.; Breeher, L.; Miller, S.; Trenary, M.; Neveau, D.; Higgins, S. Post-COVID-19 Syndrome (Long Haul Syndrome): Description of a Multidisciplinary Clinic at Mayo Clinic and Characteristics of the Initial Patient Cohort. Mayo Clin. Proc. 2021, 96, 1782–1791. [Google Scholar] [CrossRef]
- Sadat Larijani, M.; Ashrafian, F.; Bagheri Amiri, F.; Banifazl, M.; Bavand, A.; Karami, A.; Asgari Shokooh, F.; Ramezani, A. Characterization of Long COVID-19 Manifestations and Its Associated Factors: A Prospective Cohort Study from Iran. Microb. Pathog. 2022, 169, 105618. [Google Scholar] [CrossRef]
- Xie, Y.; Bowe, B.; Al-Aly, Z. Burdens of Post-Acute Sequelae of COVID-19 by Severity of Acute Infection, Demographics and Health Status. Nat. Commun. 2021, 12, 6571. [Google Scholar] [CrossRef]
- Ocsovszky, Z.; Otohal, J.; Berényi, B.; Juhász, V.; Skoda, R.; Bokor, L.; Dohy, Z.; Szabó, L.; Nagy, G.; Becker, D.; et al. The Associations of Long-COVID Symptoms, Clinical Characteristics and Affective Psychological Constructs in a Non-Hospitalized Cohort. Physiol. Int. 2022, 109, 230–245. [Google Scholar] [CrossRef] [PubMed]
- Elhadedy, M.A.; Marie, Y.; Halawa, A. COVID-19 in Renal Transplant Recipients: Case Series and a Brief Review of Current Evidence. NEF 2021, 145, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Qui, L.; Zhang, J.; Huang, Y.; Cheng, G.; Chen, Z.; Ming, C.; Lu, X.; Gong, N. Long-Term Clinical and Immunological Impact of Severe COVID-19 on a Living Kidney Transplant Recipient—A Case Report. Front. Immunol. 2021, 12, 3687. [Google Scholar] [CrossRef]
- Bhoori, S.; Rossi, R.E.; Citterio, D.; Mazzaferro, V. COVID-19 in Long-Term Liver Transplant Patients: Preliminary Experience from an Italian Transplant Centre in Lombardy. Lancet Gastroenterol. Hepatol 2020, 5, 532–533. [Google Scholar] [CrossRef] [PubMed]
- Buonsenso, D.; Munblit, D.; Pazukhina, E.; Ricchiuto, A.; Sinatti, D.; Zona, M.; De Matteis, A.; D’Ilario, F.; Gentili, C.; Lanni, R.; et al. Post-COVID Condition in Adults and Children Living in the Same Household in Italy: A Prospective Cohort Study Using the ISARIC Global Follow-Up Protocol. Front. Pediatr. 2022, 10, 447. [Google Scholar] [CrossRef] [PubMed]
- Yellumahanthi, D.K.; Barnett, B.; Barnett, S.; Yellumahanthi, S. COVID-19 Infection: Its Lingering Symptoms in Adults. Cureus 2022, 14, e24736. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-Month Consequences of COVID-19 in Patients Discharged from Hospital: A Cohort Study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef] [PubMed]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, J.C.; Klaser, K.; Antonelli, M.; Canas, L.S.; et al. Attributes and Predictors of Long COVID. Nat. Med. 2021, 27, 626–631. [Google Scholar] [CrossRef]
- Asadi-Pooya, A.A.; Nemati, H.; Shahisavandi, M.; Akbari, A.; Emami, A.; Lotfi, M.; Rostamihosseinkhani, M.; Barzegar, Z.; Kabiri, M.; Zeraatpisheh, Z.; et al. Long COVID in Children and Adolescents. World J. Pediatr. 2021, 17, 495–499. [Google Scholar] [CrossRef]
- Taquet, M.; Dercon, Q.; Luciano, S.; Geddes, J.R.; Husain, M.; Harrison, P.J. Incidence, Co-Occurrence, and Evolution of Long-COVID Features: A 6-Month Retrospective Cohort Study of 273,618 Survivors of COVID-19. PLoS Med. 2021, 18, e1003773. [Google Scholar] [CrossRef]
- Peghin, M.; Palese, A.; Venturini, M.; De Martino, M.; Gerussi, V.; Graziano, E.; Bontempo, G.; Marrella, F.; Tommasini, A.; Fabris, M.; et al. Post-COVID-19 Symptoms 6 Months after Acute Infection among Hospitalized and Non-Hospitalized Patients. Clin. Microbiol. Infect. 2021, 27, 1507–1513. [Google Scholar] [CrossRef] [PubMed]
- Carvalho-Schneider, C.; Laurent, E.; Lemaignen, A.; Beaufils, E.; Bourbao-Tournois, C.; Laribi, S.; Flament, T.; Ferreira-Maldent, N.; Bruyère, F.; Stefic, K.; et al. Follow-up of Adults with Noncritical COVID-19 Two Months after Symptom Onset. Clin. Microbiol. Infect. 2021, 27, 258–263. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, A.; Iqbal, K.; Arshad Ali, S.; Azim, D.; Farid, E.; Baig, M.D.; Bin Arif, T.; Raza, M. The COVID-19 Sequelae: A Cross-Sectional Evaluation of Post-Recovery Symptoms and the Need for Rehabilitation of COVID-19 Survivors. Cureus 2021, 13, e13080. [Google Scholar] [CrossRef]
- Tleyjeh, I.M.; Saddik, B.; AlSwaidan, N.; AlAnazi, A.; Ramakrishnan, R.K.; Alhazmi, D.; Aloufi, A.; AlSumait, F.; Berbari, E.; Halwani, R. Prevalence and Predictors of Post-Acute COVID-19 Syndrome (PACS) after Hospital Discharge: A Cohort Study with 4 Months Median Follow-Up. PLoS ONE 2021, 16, e0260568. [Google Scholar] [CrossRef]
- Osmanov, I.M.; Spiridonova, E.; Bobkova, P.; Gamirova, A.; Shikhaleva, A.; Andreeva, M.; Blyuss, O.; El-Taravi, Y.; DunnGalvin, A.; Comberiati, P.; et al. Risk Factors for Post-COVID-19 Condition in Previously Hospitalised Children Using the ISARIC Global Follow-up Protocol: A Prospective Cohort Study. Eur. Respir. J. 2022, 59, 2101341. [Google Scholar] [CrossRef]
- Righi, E.; Mirandola, M.; Mazzaferri, F.; Dossi, G.; Razzaboni, E.; Zaffagnini, A.; Ivaldi, F.; Visentin, A.; Lambertenghi, L.; Arena, C.; et al. Determinants of Persistence of Symptoms and Impact on Physical and Mental Wellbeing in Long COVID: A Prospective Cohort Study. J. Infect. 2022, 84, 566–572. [Google Scholar] [CrossRef] [PubMed]
- de Miranda, D.A.P.; Gomes, S.V.C.; Filgueiras, P.S.; Corsini, C.A.; Almeida, N.B.F.; Silva, R.A.; Medeiros, M.I.V.A.R.C.; Vilela, R.V.R.; Fernandes, G.R.; Grenfell, R.F.Q. Long COVID-19 Syndrome: A 14-Months Longitudinal Study during the Two First Epidemic Peaks in Southeast Brazil. Trans. R. Soc. Trop. Med. Hyg. 2022, 116, 1007–1014. [Google Scholar] [CrossRef] [PubMed]
- Loosen, S.H.; Jensen, B.-E.O.; Tanislav, C.; Luedde, T.; Roderburg, C.; Kostev, K. Obesity and Lipid Metabolism Disorders Determine the Risk for Development of Long COVID Syndrome: A Cross-Sectional Study from 50,402 COVID-19 Patients. Infection 2022, 50, 1165–1170. [Google Scholar] [CrossRef]
- Messin, L.; Puyraveau, M.; Benabdallah, Y.; Lepiller, Q.; Gendrin, V.; Zayet, S.; Klopfenstein, T.; Toko, L.; Pierron, A.; Royer, P.-Y. COVEVOL: Natural Evolution at 6 Months of COVID-19. Viruses 2021, 13, 2151. [Google Scholar] [CrossRef]
- Kim, Y.; Kim, S.-W.; Chang, H.-H.; Kwon, K.T.; Hwang, S.; Bae, S. One Year Follow-Up of COVID-19 Related Symptoms and Patient Quality of Life: A Prospective Cohort Study. Yonsei Med. J. 2022, 63, 499–510. [Google Scholar] [CrossRef]
- Subramanian, A.; Nirantharakumar, K.; Hughes, S.; Myles, P.; Williams, T.; Gokhale, K.M.; Taverner, T.; Chandan, J.S.; Brown, K.; Simms-Williams, N.; et al. Symptoms and Risk Factors for Long COVID in Non-Hospitalized Adults. Nat. Med. 2022, 28, 1706–1714. [Google Scholar] [CrossRef] [PubMed]
- Helmsdal, G.; Hanusson, K.D.; Kristiansen, M.F.; Foldbo, B.M.; Danielsen, M.E.; Steig, B.Á.; Gaini, S.; Strøm, M.; Weihe, P.; Petersen, M.S. Long COVID in the Long Run—23-Month Follow-up Study of Persistent Symptoms. Open Forum. Infect. Dis. 2022, 9, ofac270. [Google Scholar] [CrossRef] [PubMed]
- Philip, K.E.J.; Buttery, S.; Williams, P.; Vijayakumar, B.; Tonkin, J.; Cumella, A.; Renwick, L.; Ogden, L.; Quint, J.K.; Johnston, S.L.; et al. Impact of COVID-19 on People with Asthma: A Mixed Methods Analysis from a UK Wide Survey. BMJ Open Respir. Res. 2022, 9, e001056. [Google Scholar] [CrossRef]
- Sigfrid, L.; Drake, T.M.; Pauley, E.; Jesudason, E.C.; Olliaro, P.; Lim, W.S.; Gillesen, A.; Berry, C.; Lowe, D.J.; McPeake, J.; et al. Long Covid in Adults Discharged from UK Hospitals after Covid-19: A Prospective, Multicentre Cohort Study Using the ISARIC WHO Clinical Characterisation Protocol. Lancet Reg. Health Eur. 2021, 8, 100186. [Google Scholar] [CrossRef]
- Desgranges, F.; Tadini, E.; Munting, A.; Regina, J.; Filippidis, P.; Viala, B.; Karachalias, E.; Suttels, V.; Haefliger, D.; Kampouri, E.; et al. Post-COVID-19 Syndrome in Outpatients: A Cohort Study. J. Gen. Intern. Med. 2022, 37, 1943–1952. [Google Scholar] [CrossRef] [PubMed]
- Pelà, G.; Goldoni, M.; Solinas, E.; Cavalli, C.; Tagliaferri, S.; Ranzieri, S.; Frizzelli, A.; Marchi, L.; Mori, P.A.; Majori, M.; et al. Sex-Related Differences in Long-COVID-19 Syndrome. J. Women’s Health 2022, 31, 620–630. [Google Scholar] [CrossRef] [PubMed]
- Gebhard, C.E.; Sütsch, C.; Bengs, S.; Todorov, A.; Deforth, M.; Buehler, K.P.; Meisel, A.; Schuepbach, R.A.; Zinkernagel, A.S.; Brugger, S.D.; et al. Understanding the Impact of Sociocultural Gender on Post-Acute Sequelae of COVID-19: A Bayesian Approach. medRxiv 2021. [Google Scholar] [CrossRef]
- Tleyjeh, I.M.; Saddik, B.; Ramakrishnan, R.K.; AlSwaidan, N.; AlAnazi, A.; Alhazmi, D.; Aloufi, A.; AlSumait, F.; Berbari, E.F.; Halwani, R. Long Term Predictors of Breathlessness, Exercise Intolerance, Chronic Fatigue and Well-Being in Hospitalized Patients with COVID-19: A Cohort Study with 4 Months Median Follow-Up. J. Infect. Public Health 2022, 15, 21–28. [Google Scholar] [CrossRef]
- García-Abellán, J.; Padilla, S.; Fernández-González, M.; García, J.A.; Agulló, V.; Andreo, M.; Ruiz, S.; Galiana, A.; Gutiérrez, F.; Masiá, M. Antibody Response to SARS-CoV-2 Is Associated with Long-Term Clinical Outcome in Patients with COVID-19: A Longitudinal Study. J. Clin. Immunol. 2021, 41, 1490–1501. [Google Scholar] [CrossRef]
- Asadi-Pooya, A.A.; Akbari, A.; Emami, A.; Lotfi, M.; Rostamihosseinkhani, M.; Nemati, H.; Barzegar, Z.; Kabiri, M.; Zeraatpisheh, Z.; Farjoud-Kouhanjani, M.; et al. Risk Factors Associated with Long COVID Syndrome: A Retrospective Study. Iran J. Med. Sci. 2021, 46, 428–436. [Google Scholar] [CrossRef]
- Munblit, D.; Bobkova, P.; Spiridonova, E.; Shikhaleva, A.; Gamirova, A.; Blyuss, O.; Nekliudov, N.; Bugaeva, P.; Andreeva, M.; DunnGalvin, A.; et al. Incidence and Risk Factors for Persistent Symptoms in Adults Previously Hospitalized for COVID-19. Clin. Exp. Allergy 2021, 51, 1107–1120. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-las-Peñas, C.; Martín-Guerrero, J.D.; Pellicer-Valero, Ó.J.; Navarro-Pardo, E.; Gómez-Mayordomo, V.; Cuadrado, M.L.; Arias-Navalón, J.A.; Cigarán-Méndez, M.; Hernández-Barrera, V.; Arendt-Nielsen, L. Female Sex Is a Risk Factor Associated with Long-Term Post-COVID Related-Symptoms but Not with COVID-19 Symptoms: The LONG-COVID-EXP-CM Multicenter Study. JCM 2022, 11, 413. [Google Scholar] [CrossRef] [PubMed]
- Bai, F.; Tomasoni, D.; Falcinella, C.; Barbanotti, D.; Castoldi, R.; Mulè, G.; Augello, M.; Mondatore, D.; Allegrini, M.; Cona, A.; et al. Female Gender Is Associated with Long COVID Syndrome: A Prospective Cohort Study. Clin. Microbiol. Infect. 2022, 28, e9–e611. [Google Scholar] [CrossRef] [PubMed]
- Chudzik, M.; Lewek, J.; Kapusta, J.; Banach, M.; Jankowski, P.; Bielecka-Dabrowa, A. Predictors of Long COVID in Patients without Comorbidities: Data from the Polish Long-COVID Cardiovascular (PoLoCOV-CVD) Study. JCM 2022, 11, 4980. [Google Scholar] [CrossRef]
- Chudzik, M.; Babicki, M.; Kapusta, J.; Kałuzińska-Kołat, Ż.; Kołat, D.; Jankowski, P.; Mastalerz-Migas, A. Long-COVID Clinical Features and Risk Factors: A Retrospective Analysis of Patients from the STOP-COVID Registry of the PoLoCOV Study. Viruses 2022, 14, 1755. [Google Scholar] [CrossRef]
- Fernández-de-las-Peñas, C.; Guijarro, C.; Torres-Macho, J.; Velasco-Arribas, M.; Plaza-Canteli, S.; Hernández-Barrera, V.; Arias-Navalón, J.A. Diabetes and the Risk of Long-Term Post-COVID Symptoms. Diabetes 2021, 70, 2917–2921. [Google Scholar] [CrossRef]
- Shang, L.; Wang, L.; Zhou, F.; Li, J.; Liu, Y.; Yang, S. Long-term Effects of Obesity on COVID-19 Patients Discharged from Hospital. Immun. Inflamm. Dis. 2021, 9, 1678–1685. [Google Scholar] [CrossRef]
- Fernández-de-las-Peñas, C.; Torres-Macho, J.; Elvira-Martínez, C.M.; Molina-Trigueros, L.J.; Sebastián-Viana, T.; Hernández-Barrera, V. Obesity Is Associated with a Greater Number of Long-term Post-COVID Symptoms and Poor Sleep Quality: A Multicentre Case-control Study. Int. J. Clin. Pract. 2021, 75, e14917. [Google Scholar] [CrossRef]
- Jia, X.; Cao, S.; Lee, A.S.; Manohar, M.; Sindher, S.B.; Ahuja, N.; Artandi, M.; Blish, C.A.; Blomkalns, A.L.; Chang, I.; et al. Anti-Nucleocapsid Antibody Levels and Pulmonary Comorbid Conditions Are Linked to Post–COVID-19 Syndrome. JCI Insight 2022, 7, e156713. [Google Scholar] [CrossRef]
- Lacavalerie, M.R.; Pierre-Francois, S.; Agossou, M.; Inamo, J.; Cabie, A.; Barnay, J.L.; Neviere, R. Obese Patients with Long COVID-19 Display Abnormal Hyperventilatory Response and Impaired Gas Exchange at Peak Exercise. Future Cardiol. 2022, 18, 577–584. [Google Scholar] [CrossRef]
- Oto, O.A.; Ozturk, S.; Arici, M.; Velioğlu, A.; Dursun, B.; Guller, N.; Şahin, İ.; Eser, Z.E.; Paydaş, S.; Trabulus, S.; et al. Middle-Term Outcomes in Renal Transplant Recipients with COVID-19: A National, Multicenter, Controlled Study. Clin. Kidney J. 2022, 15, 999–1006. [Google Scholar] [CrossRef] [PubMed]
- Whitaker, M.; Elliott, J.; Chadeau-Hyam, M.; Riley, S.; Darzi, A.; Cooke, G.; Ward, H.; Elliott, P. Persistent COVID-19 Symptoms in a Community Study of 606,434 People in England. Nat. Commun. 2022, 13, 1957. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Ashcroft, T.; Chung, A.; Dighero, I.; Dozier, M.; Horne, M.; McSwiggan, E.; Shamsuddin, A.; Nair, H. Risk Factors for Poor Outcomes in Hospitalised COVID-19 Patients: A Systematic Review and Meta-Analysis. J. Glob. Health 2021, 11, 10001. [Google Scholar] [CrossRef] [PubMed]
- Sahu, A.K.; Mathew, R.; Aggarwal, P.; Nayer, J.; Bhoi, S.; Satapathy, S.; Ekka, M. Clinical Determinants of Severe COVID-19 Disease—A Systematic Review and Meta-Analysis. J. Glob. Infect. Dis. 2021, 13, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Mauvais-Jarvis, F.; Bairey Merz, N.; Barnes, P.J.; Brinton, R.D.; Carrero, J.-J.; DeMeo, D.L.; De Vries, G.J.; Epperson, C.N.; Govindan, R.; Klein, S.L.; et al. Sex and Gender: Modifiers of Health, Disease, and Medicine. Lancet 2020, 396, 565–582. [Google Scholar] [CrossRef] [PubMed]
- Abumweis, S.; Alrefai, W.; Alzoughool, F. Association of Obesity with COVID-19 Diseases Severity and Mortality: A Meta-Analysis of Studies. Obes. Med. 2022, 33, 100431. [Google Scholar] [CrossRef]
- Chen, Z.; Peng, Y.; Wu, X.; Pang, B.; Yang, F.; Zheng, W.; Liu, C.; Zhang, J. Comorbidities and Complications of COVID-19 Associated with Disease Severity, Progression, and Mortality in China with Centralized Isolation and Hospitalization: A Systematic Review and Meta-Analysis. Front. Public Health 2022, 10, 923485. [Google Scholar] [CrossRef]
- Liu, D.; Yuan, X.; Gao, F.; Zhao, B.; Ding, L.; Huan, M.; Liu, C.; Jiang, L. High Number and Specific Comorbidities Could Impact the Immune Response in COVID-19 Patients. Front. Immunol. 2022, 13, 899930. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PubMed Search Formula |
| #1 “post-acute COVID-19 syndrome” [MeSH Terms] OR “long COVID-19” [All Fields] OR “long COVID-19 symptoms” [All Fields] OR “long hauler” [All Fields] OR “post-COVID-19” [All Fields] OR “post-acute COVID-19 symptoms” [All Fields] OR “COVID-19 sequelae” [All Fields] #2 “age” [All Fields] #3 “sex” [MeSH Terms] OR “sex” [All Fields] #4 “comorbidity” [MeSH Terms] OR (“transplants” [MeSH Terms] OR “transplantation” [MeSH Terms] OR transplant [All Fields]) OR (“obesity” [MeSH Terms] OR obesity [All Fields]) OR (“diabetes mellitus” [MeSH Terms] OR “diabetes insipidus” [MeSH Terms] OR diabetes [All Fields]) OR (“hypertension” [MeSH Terms] OR hypertension [All Fields]) OR (“lung diseases” [MeSH Terms] OR pulmonary disease [All Fields]) OR (“asthma” [MeSH Terms] OR asthma [All Fields]) OR (“pulmonary disease, chronic obstructive” [MeSH Terms] OR COPD [All Fields]) #5 #1 AND #2 #6 #1 AND #3 #7 #1 AND #4 |
| MEDLINE/CINAHL (via EBSCO) Search Formula |
| #1 “post-acute COVID-19 syndrome” OR “long COVID-19” OR “long COVID-19 symptoms” OR “long hauler” OR “post-COVID-19” OR “post-acute COVID-19 symptoms” OR “COVID-19 sequelae” #2 “age” #3 “sex” #4 “comorbidity” OR “transplants” OR “transplantation” OR “obesity” OR “diabetes mellitus” OR “diabetes” OR “hypertension” OR “pulmonary disease” OR “asthma” OR “chronic obstructive pulmonary disease” #5 #1 AND #2 #6 #1 AND #3 #7 #1 AND #4 |
| WOS (EMBASE)/Web of Science Search Formula |
| (“post-acute COVID-19 syndrome” OR “long COVID-19” OR “long COVID-19 symptoms” OR “long hauler” OR “post-COVID-19” OR “post-acute COVID-19 symptoms” OR “COVID-19 sequelae” AND ((“age”) OR (“sex”) OR (“comorbidity” OR “transplants” OR “transplantation” OR “obesity” OR “diabetes mellitus” OR “diabetes” OR “hypertension” OR “pulmonary disease” OR “asthma” OR “chronic obstructive pulmonary disease”)) |
| Author | Country Study Period | Study Design Sample Size | Age | Symptoms Assessment | Post-COVID-19 Symptoms | Main Findings |
|---|---|---|---|---|---|---|
| Buonsenso et al., 2022 | Italy 1 April 2020–31 April 2021 | Prospective cohort n = 507 | Adults, 44 y | ISARIC Global COVID-19 protocol EQ-5D-5L | Headache, Malaise, Fatigue | Probability of being fully recovered: 1–3 months Adults 0.83 (0.38), p = 0.001 6–9 months Adults 0.83 (0.38), p = 0.016 |
| Yellumahanthi et al., 2022 | USA 13 March 2020–12 March 2021 | Prospective cohort n = 53 | 18–64 y (n = 38) ≥65 y (n = 15) | Self-reported questionnaire three months after | Fatigue, Brain fog Shortness of breath, Joint pain, Loss taste/smell, Anxiety/Depression, Hair loss, Sleep disturbances, Cough | 18–64 y Symptoms present n = 20 Symptoms absent n = 18 >65 y Symptoms present n = 7 Symptoms absent n = 8 p = 0.696 |
| Huang et al., 2021 | China 16 June 2020–13 September 2020 | Cohort study n = 1733 | mean 57 y | EQ-5D-5L | Fatigue, Sleep difficulties, Anxiety/Depression | Per 10-year increase im age—Risk of Fatigue OR 1.17, 95% CI 1.07–1.27 * |
| Sudre et al., 2021 | UK, USA, Sweden March 2020–December 2020 | Prospective cohort n = 8364 | Positive for SARS-CoV-2 42 y (IQR 32–53) Negative for SARS-CoV-2 42 y (IQR 32–53) | COVID-19 Symptoms Study app | Abdominal pain, Chest pain, Sore throat, Shortness of breath, Fatigue, Hoarse voice, Diarrhea, skipped meals, Cough, Muscle pain, Loss of smell, Headache | OR (95% CI)—18–30 y 30–40 y—OR from 2.11 to 4.12 * 40–50 y—OR from 2.24 to 4.35 * 50–60 y—OR from 6.65 to 11.49 * 60–70 y—OR from 6.53 to 14.0 * ≥70 y—OR from 5.46 to 18.56 * |
| Asadi-Pooya et al., 2021 # | Iran February 2020 –February 2021 | Cross-Sectional n = 58 | Mean age 12.3 y (SD 3.3) | Telephone interview | Fatigue, Shortness of breath, Exercise intolerance, Walking intolerance, Cough, Sputum, Sleep difficulty, Muscle/Joint pain, Headache, Chest pain, Palpitation, Loss of smell, Sore throat, Dizziness | OR 1.314 (95% CI 1.043–1.656), p = 0.002 * |
| Taquet et al., 2021 | USA January 2020–December 2020 | Retrospective cohort n = 388,067 | COVID-19 (unmatched) Mean age 46.3 y (SD 9.8) COVID-19 (matched) Mean age 39.4 y (SD 18.4) Influenza (matched) Mean age 38.3 y (SD 19.7) | Electronic health records | Breathlessness, Fatigue/malaise, Chest pain, Throat pain, Headache, Abdominal pain, Myalgia, Cognitive symptoms, Anxiety/depression | 6-month incidence of long COVID-19 symptoms % (95% CI) 10–21 y—55.06 (54.34–55.77) 45–64 y—58.92 (58.24–59.59) ≥65 y—61.05 (60.29–61.81) |
| Peghin et al., 2021 | Italy March 2020–November 2020 | Cohort n = 599 | Mean age 53 y (SD 15.8) | Questionnaire via telephone interview | Dyspnea, Cough, Fatigue, Chest pain, Anosmia/Dysgeusia, Headache, Sleep disorders, Neurological Disorders, Brain Fog, Anxiety/Depression, Skin lesion, Gastrointestinal Dis., Hair loss, Ocular involvement | 41–60 vs.18–40 y OR 1.0 (95% CI 0.6–11.6), p = 0.9 >60 vs. 18–40 y OR 1.03 (95% CI 0.6–1.7), p = 0.9 >60 vs. 41–60 y OR 1.04 (95% CI 0.67–1.6), p = 0.8 |
| Carvalho-Schneider et al., 2021 | France March 2020–August 2020 | Cohort n = 150 | Mean age 49 y (IQR 34–64) | Telephone interviews | Dyspnea Chest pain Palpitations Anosmia/Ageusia Headache Cutaneous signs Arthralgia/Myalgia Digestive disorders Fever Sick leave | One or more long COVID-19 symptom n (%) D30 (n = 150) * <30 y—7 (6.8) 30–39 y—21 (20.4) 40–49 y—24 (23.3) 50–59 y—28 (27.2) 60–69 y—11 (10.7) p = 0.06 D60 (n = 130) * <30 y—4 (4.7) 30–39 y—19 (22.1) 40–49 y—23 (26.7) 50–59 y—21 (24.4) 60–69 y—10 (11.6) p = 0.026 |
| Iqbal et al., 2021 | Pakistan September 2020–December 2020 | Cross Sectional n = 158 | Mean age 40.1 y (SD 12.42) | Questionnaire | Fatigue, Sleep quality, Anxiety/Depression Dyspnea, Joint pain, Loss of smell/taste, Cough, Loss Hair, Headache, Chest pain, Brain fog, Blurred vision, Tinnitus | Relation of age with post-COVID-19 Dyspnea (p = 0.007) * Cough (p < 0.001) * Joint pain (p < 0.001) * Chest pain (p < 0.001) * |
| Tleyjeh et al., 2021 | Saudi Arabia May 2020–January 2021 | Prospective Cohort n = 222 | Mean age 52.5 y (IQR 38.52–66.42) | Structured interview via phone call | Insomnia, Fever, Fatigue, Joint pain, Muscle pain, Memory loss, Headaches, Loss of taste, Abdominal pain, Nausea/Vomiting, Diarrhea, Loss of smell, Sore throat, Runny nose, Chest pain, Cough, Shortness of breath | Hazard model of new or persistent symptoms at follow-up (n = 222) Adjusted HR (95% CI) 0.99 (0.98–1.01), p = 0.38 |
| Osmanov et al., 2022 # | Russia April 2020–February 2021 | Prospective Cohort n = 518 | Mean age 10.4 y (IQR 3–15.2) | Telephone Interview— 1.0 ISARIC COVID-19 Health and Wellbeing Follow-Up Survey for Children | Respiratory symptoms, Neurological symptoms, Sleep problems, Gastrointestinal Dermatological Cardiovascular Fatigue Musculoskeletal | Presence of any persistent symptom at time of follow-up (n = 127) 2–5 y—OR 0.93 (95% CI 0.38–2.22) 6–11 y—OR 2.57 (95% CI 1.29–5.36) * 12–18 y—OR 2.52 (95% CI 1.34–5.01) * |
| Righi et al., 2022 | Italy February 2020 –February 2021 | Prospective Cohort n = 465 | Mean age 56 y (IQR 45–66) | Questionnaire | Cough, Diarrhea, Fatigue, Myalgia, Anosmia, Dysgeusia, Breathlessness | Persistence of symptoms at 9-month follow-up >50 y—OR 2.5 (95% CI 1.28–4.88), p = 0.007 * Persistence of fatigue at 9-month follow-up >50 y—HR 0.98 (95% CI 0.97–0.99) |
| de Miranda et al., 2022 | Brazil March 2020–November 2021 | Longitudinal study n = 646 | Mean age 50.3 y (SD 15.8) | In person or virtual interview | Sore throat, Runny nose, Sputum, Skin lesion, Tachycardia, Vertigo, Chest pain, Joint pain, Diarrhea, Anxiety, Insomnia, Myalgia, Headache, Loss of smell/taste, Dyspnea, Fatigue | Mild COVID-19: 59.3% of 329 patients developed symptoms—<60 y: n = 162 (83.1%) Severe COVID-19: 33.1% of 260 patients developed symptoms ≤60 y old: n = 48 (55.8%) >60 y old: n = 38 (44.2%) |
| Loosen et al., 2022 | Germany 1 March 2020–31 March 2021 | Cross-sectional n = 50,402 | Mean age 48.8 y (SD 19.3) | Medical record data from the Disease Analyzer database | Fatigue, Abnormalities of breathing, Disturbances of smell/taste, Disturbances in attention | ≤30 years/COVID-19 patients: n = 10,443 Patients developing long COVID-19: n = 213 31–45 years/COVID-19 patients: n = 12,963 Patients developing long COVID-19: n = 379 46–60 years/COVID-19 patients: n = 14,424 Patients developing long COVID-19: n = 664 >60 years/COVID-19 patients: n = 12,572 Patients developing long COVID-19: n = 452 |
| Messin et al., 2021 | France March 2020–October 2020 | Retrospective observational n = 74 With persistent symptoms: n = 53 Without persistent symptoms: n = 21 | Mean age: 54.7 y (SD 16.9) | Telephone interview | Asthenia, Dyspnea, Anxiety, Anosmia, Ageusia, Nasal obstruction, Rhinorrhea, Sneezing, Odynophagia, Dysphonia, Chest pain, Palpitations, Headache, Dizziness, Drowsiness, Neuropathic pain, Depressive syndrome, Memory impairment, Attention deficit, Hair loss Diarrhea, Cough, Pain, Erectile dysfunction | 18–30 years—number (%) Symptoms: 5 (9.4)/No symptoms: 4 (19.1) 31–40 years—number (%) Symptoms: 8 (15.1)/No symptoms: 7 (33.3) 41–50 years—number (%) Symptoms: 8 (15.1)/No symptoms: 6 (28.6) 51–60 years—number (%) Symptoms: 9 (17)/No symptoms 0 61–70 years—number (%) Symptoms: 14 (26.4)/No symptoms: 0 >71 years—number (%) Symptoms: 9 (17)/No symptoms: 4 (19.1) |
| Kim et al., 2022 | Korea 31 August 2020–2 March 2021 | Prospective cohort n = 170 With persistent symptoms: n = 129 Without persistent symptoms: n = 41 | Median age: 51 y (IQR 37–61) | Individualized questionnaire | Fever, Myalgia, Cough, Arthralgia, Fatigue, Sore throat, Rhinorrhea, Chest pain, Dyspnea, Palpitation, Arrhythmia, Headache, Cognitive dysfunction, Dizziness, Insomnia, Depression/Anxiety, Vomiting, Diarrhea Anosmia, Ageusia, Tinnitus, Alopecia, Skin rash, Paresthesia | 20–29 years—number (%) Symptoms: 19 (14.7)/No symptoms: 10 (24.4) 30–39 years—number (%) Symptoms: 18 (14)/No symptoms: 6 (14.6) 40–49 years—number (%) Symptoms: 17 (13.2)/No symptoms: 9 (22) 50–59 years—number (%) Symptoms: 35 (27.1)/No symptoms: 9 (22) 60–70 years—number (%) Symptoms: 40 (31)/No symptoms: 7 (17.1) |
| Subramanian et al., 2022 | United Kingdom 31 January 2020–15 April 2021 | Retrospective matched cohort study Non-hospitalized COVID-19 survivors n = 486,149 Matched patients with no evidence of COVID-19 n = 1,944,580 | Patients infected with SARS-CoV-2 Mean age 44.1 y (SD 17.0) Comparator cohort Mean age 43.8 y (SD 16.9) | Interviews and questionnaires | A total of 62 symptoms were significantly associated with SARS-CoV-2 infection after 12 weeks: Anosmia, Hair loss, Sneezing, Ejaculation difficulty, Reduced libido, Shortness of breath at rest, Fatigue, Chest pain, Hoarse voice, Fever | 18–29 years (n = 95,969) With symptoms: n (%) 6932 (7.2) 30–39 years (n = 78,302) With symptoms: n (%) 5805 (7.4) 40–49 years (n = 75,349) With symptoms: n (%) 5784 (7.7) 50–59 years (n = 73,262) With symptoms: n (%) 5485 (7.5) 60–69 years (n = 35,932) With symptoms: n (%) 2790 (7.8) ≥70 years (n = 25,323) With symptoms: n (%) 3073 (12.1) |
| Helmsdal et al., 2022 | Faroe Islands March 2020–January 2022 | Cohort n = 180 | Mean age 40 y (SD 19.4) | Standardized questionnaire via telephone interview | Fatigue, loss taste, loss smell, Headache, Skin rashes, Arthralgia, Dyspnea, Myalgia, Rhinorrhea, Chest tightness, Cough, Diarrhea, Nausea, Anorexia, Chills, Fever, Sore throat | Prevalence (%) of long COVID-19 (n = 170) at 23-months Mean (SD) Age at symptom onset * Symptoms (n = 65) age: 45.1 (18.5) No symptoms (n = 105) age: 36.9 (19.3) p = 0.03 Persistent symptoms vs. No symptoms—n (%) 0–17 y—4 (6.2) vs. 17 (16.2) 18–34 y—16 (24.6) vs. 34 (32.4) 35–49 y—17 (26.2) vs. 22 (21.0) 50–67 y—18 (27.7) vs. 25 (23.8) >67 y—10 (15.4) vs. 7 (6.7) p = 0.1 |
| Author | Country Study Period | Study Design Sample Size | Age | Symptoms Assessment | Post-COVID-19 Symptoms | Main Findings |
|---|---|---|---|---|---|---|
| Bai et al., 2021 | Italy 15 April 2020–15 December 2020 | Prospective Cohort n = 377 Female 137 | Median age 57 y (IQR 49–68) | Interview and physical examination Impact of Event Scale-Revised (IES-R) | Anosmia, Dysgeusia, Gastrointestinal symptoms, Fever, Joint pain, Myalgia, Dyspnea at rest, Exertional dyspnea, Fatigue, Brain fog, PTSD, Depression, Anxiety | Female Sex Risk Long COVID-19 OR 2.78 (95% CI 1.68–4.62) * Long COVID-19 AOR3.32 (95% CI 1.78–6.17) * |
| Pela et al., 2022 | Italy Follow-up: May 2020–March 2021 | Cohort n = 223 Female 89 | Mean age 59 y (SD 13) | Retrospective Medical records Prospective Long COVID-19-19 reevaluation | Dyspnea, Cough, Fatigue, Chest pain, Palpitations, Myalgia, Sleep disturbance | Female Sex Risk Dyspnea OR 2.35 (95% CI 1.12–4.94) * Fatigue OR6.72 (95% CI 2.34–19.26) * Chest pain OR 2.04 (95% CI 1.00–4.15) * Palpitation OR 2.30 (95% CI 1.14–4.65) * |
| Sigfrid et al., 2021 | UK NR | Prospective Cohort n = 327 Female 135 | Media age 60 y (IQR 51.7–67.7) | Washington group short scale MRC Dyspnea Scale EQ5D-5L | Fatigue, Breathlessness, Sleep problems, Headache, Limb weakness, Muscle pain, Joint pain, Dizziness, Palpitations, Ocular problems, Stomach pain, Diarrhea, Cough, Chest pain, Loss of smell, Fever, Loss of taste, Nausea, Vomiting, Skin rashes | Female Sex < 50 years Risk Long COVID-19 (AOR 5.09, 95% CI 1.64–15.74) * Fatigue (AOR 2.06, 95% CI 0.81–3.31) Breathlessness (AOR 7.15, 95% CI 2.24–22.83) * |
| Fernandez-de-las-Peñas et al., 2022 | Spain 10 March 2020–31 May 2020 | Cross-sectional n = 1969 Female 915 | Mean age 61 y (SD 16) | Telephone interview | Fatigue, Dyspnea at rest, Dyspnea at exertion, Pain, Memory loss, Brain fog, Concentration loss, Hair loss, Palpitations, Skin rashes, Diarrhea, Voice problems, Gastrointestinal problems, Ageusia, Anosmia, Ocular Problems, Throat pain, Anxiety/Depression, Sleep quality | Female Sex Risk Symptoms (AOR 2.54, 95% CI 1.67–3.86) * Fatigue (AOR 1.51, 95% CI 1.04–2.20) * Dyspnea rest (AOR 1.42, 95% CI 1.08–1.88) * Dyspnea exertion (AOR 1.4, 95% CI 1.10–1.79) * Pain (AOR 1.34, 95% CI 1.05–1.72) * Hair loss (AOR 4.52, 95% CI 2.78–7.36) * Ocular problems (AOR 1.98, 95% CI 1.18–3.31) * Depression (AOR 1.60, 95% CI 1.00–2.57) * Sleep quality (AOR 1.63, 95% CI 1.09–2.43) * |
| Gebhard et al., 2022 | Switzerland February 2020–December 2020 | Prospective cohort n = 2927 Female 1346 | NR | Self-reported questionnaires | Dyspnea, Reduced exercise performance, Changes in smell and taste | Females reported at least one persistent symptom than males (43.5% vs. 32.0%, p < 0.001) The higher prevalence of PASC in females was observed in both outpatients (40.5% in females vs. 25.4% in males, p < 0.001) and hospitalized patients (63.1% in females vs. 55.2% in males, p < 0.001) |
| Tleyjeh et al., 2022 | Saudi Arabia May 2020–July 2020 | Cohort n = 222 Female 51 | Range > 18 y | Medical research council (MRC) dyspnea scale Metabolic equivalent of task (MET) score Chronic fatigability syndrome questionnaire | Breathlessness, Exercise intolerance, Chronic fatigue, Poor mental well-being | Female Sex Risk Exertional Dyspnea OR4.36 (95% CI 2.25–8.46) * Lower MET exercise tolerance score OR0.19 (95% CI 0.09–0.42) * Chronic Fatigability Syndrome OR3.97 (95% CI 1.85–8.49) * |
| Desgranges et al., 2022 | Switzerland 26 February–27 April 2020 | Prospective cohort n = 418 Female 261 | Median age 41 y (IQR 31–54) | Structured and standardized phone survey | Fatigue, Smell or taste disorder, Dyspnea, Headache, Memory impairment, Hair loss, Sleep disorders | Female Sex Risk Symptoms AOR 1.67 (95% CI 1.09–2.56) * Dyspnea AOR1.71 (95% CI 0.93–3.16) Smell/taste disorder AOR 1.9 (95% CI 1.09–3.22) * Fatigue AOR1.61 (95% CI 1.00–2.59) * |
| García-Abellán at al., 2021 | Spain 10 March–30 June 2020 | Prospective longitudinal study n = 146 Female 58 | Median age 65 y (IQR 55–75) | Self-rated COVID-19 symptom questionnaire (CSQ) | Fatigue, Myalgia, Sweating, Headache, Cough, Difficulty breathing, Congestion, Sore throat, Anosmia, Diarrhea, Vomiting, Abdominal pain | Female Sex Risk Highest COVID-19 symptom questionnaire (CSQ) scores OR 2.41 (95% CI 1.20–4.82) * |
| Asadi-Pooya et al., 2021 | Iran 19 February 2020–20 November 2020 | Retrospective observational study n = 4681 Female 2203 | Mean age 52 y (SD 15) | Telephone interview | Weakness, Muscle pain, Fatigue, Sleep difficulty, Palpitations, Cough, Brain fog, Walking intolerance | Female Sex Risk Long COVID-19 Symptoms OR1.26 (95% CI1.12–1.43) * |
| Munblit et al., 2021 | Russia 8 April 2020–10 July 2020 | Longitudinal cohort study n = 2649 Female 1353 | Median age 56 y (IQR 46–66) | Study case report form (CRF) British Medical Research Council (MRC) dyspnoea scale EQ-5D-5L WHODAS 2.0 | Fatigue, Breathlessness, Forgetfulness, Muscle weakness, Ocular problems, Hair loss, Sleeping problem | Female Sex Risk Symptoms OR1.83 (95% CI 1.55–2.17) * Fatigue OR1.67 (95% CI 1.39–2.02) * Neurological OR2.03 (95% CI 1.60–2.58) * Mood OR1.83 (95% CI 1.41–2.40) * Dermatological OR3.26 (95% CI 2.36–4.57) * Gastrointestinal OR2.50 (95% CI 1.64–3.89) * Sensory OR1.73 (95% CI 2.06–2.89) * Respiratory OR1.31 (95% CI 1.06–1.62) * |
| Chudzik et al., 2022 | Poland 1 September 2020–30 September 2021 | Retrospective cohort n = 2218 Female 1410 | Mean age 54 y (SD 13.5) | Health questionnaire | Fatigue, Headache, Cough Brain fog, Dyspnoea, Hair loss, Olfactory dysfunction, Osteoarticular pain | Female Sex Risk Symptoms OR 1.44 (95% CI 1.20–1.72) * Brain fog OR1.15 (95% CI0.88–1.51) Fatigue OR1.06 (95% CI0.89–1.28) |
| Peghin et al., 2021 | Italy March 2020–November 2020 | Cohort n = 599 Female 320 | Mean age 53 y (SD 15.8) | Questionnaire via telephone interview | Dyspnea, Cough, Fatigue, Myalgia, Chest Pain, Anosmia/Dysgeusia, Headache, Arthralgia, Neurological Disorders Anxiety/Depression, Sleep Disorders, Brain Fog, Skin Lesions, Gastrointestinal Disorders, Hair Loss, Nose Cold, Sneezing, Odynophagia, Ocular Problems | Female Sex Risk Long COVID-19 Symptoms OR 1.55 (95% CI 1.05–2.27) * |
| Philip et al., 2022 | UK October 2020 | Retrospective cohort n = 4500 | Range age 50–59 y | Asthma UK and British Lung Foundation survey | Fatigue, Breathlessness, Pain (chest or whole body) | No association between female sex and long COVID-19 symptoms |
| Helmsdal et al., 2022 | Faroe Islands March 2020–January 2022 | Cohort n= 180 Female 93 | Mean age 40 y (SD 19.4) | Standardized questionnaire via telephone interview | Fatigue, affected taste, affected smell, Headache, Arthralgia, Dyspnea, Myalgia, Skin rashes, Rhinorrhea, Chest tightness, Cough, Nausea, Diarrhea, Fever, Sore throat | No association between female sex and long COVID-19 symptoms |
| Subramanian et al., 2022 | United Kingdom 31 January 2020–15 April 2021 | Retrospective matched cohort study Non-hospitalized COVID-19 survivors n = 486,149 Matched patients with no evidence of COVID-19 n = 1,944,580 | Patients infected with SARS-CoV-2 Mean age 44.1 y (SD 17.0) Comparator cohort Mean age 43.8 y (SD 16.9) | Interviews and questionnaires | Anosmia, Hair loss, Sneezing, Ejaculation difficulty, Reduced libido, Shortness of breath at rest, Fatigue, Chest pain, Hoarse voice, Fever | Female Sex Risk Long COVID-19 Symptoms HR 1.86 (95% CI 1.81–1.90) * aHR 1.52 (95% CI 1.48–1.56) * |
| Author | Country Study Period | Study Design Sample Size | Age | Symptoms Assessment | Post-COVID-19 Symptoms | Main Findings |
|---|---|---|---|---|---|---|
| Diabetes | ||||||
| Fernandez-de-las-Peñas et al., 2021 | Spain 1 March–31 May 2020 | Case-control n = 435 Patients n = 145 Control n = 290 | Patients Mean age 70.2 y (SD 13.2) Controls) Mean age 70.4 y (SD 13.4) | Hospital medical records Telephonic interview | Fatigue, Dyspnea on exertion and at rest, Pain, Memory loss, Skin rashes, Gastrointestinal dis., Brain fog, Concentration loss, Ageusia, Ocular disorder, Anosmia, Tachycardia, Cough, Headache, Sleep, Depression/Anxiety | Number of post-COVID-19 symptoms (IRR 1.06, 95% CI 0.92–1.24) Fatigue (OR 1.45, 95% CI 0.93–2.25) Dyspnea (OR 0.97, 95% CI 0.64–1.47) Pain (OR 0.951, 95% CI 0.76–1.18) Anxiety (OR 1.30, 95% CI 0.77–2.20) Depression (OR 1.31, 95% CI 0.79–2.17) Poor sleep (OR 1.34, 95% CI 0.89–2.03) |
| Obesity | ||||||
| Lacavalerie et al., 2022 | France October 2020–June 2021 | Retrospective observational n = 80 Patients n = 33 Controls n = 18 n = 29 | Patients Mean age 60 y (SD 11) Controls Mean age 50 y (SD 13) | Clinical evaluation with spirometry, cardiopulmonary and exercise testing | Fatigue, Dyspnea, Chest pain, Pulmonary function test, Cardiopulmonary exercise testing | Non-obese vs. obese, p value Pulmonary function test Predicted FEV1 (%) 87 ± 13/75 ± 13 p = 0.002 * Predicted FVC (%) 82 ± 16/74 ± 14 p = 0.04 * TLC (%) 79 ± 9/69 ± 12 p = 0.003 * RV (%) 71 ± 25/86 ± 24 p = 0.04 * KCO (%)100 ± 11/108 ± 12 p = 0.03 * Cardiopulmonary exercise testing Peak VE/VO2 35 ± 5/39 ± 7 p = 0.011 * Ventilatory reserve (%) 40 ± 14/25 ± 21 p = 0.011 * VE VCO2 slope 34 ± 6/31 ± 4 p = 0.045 * Peak SpO2 (%) 98 ± 2/96 ± 3 p = 0.036 * |
| Fernandez-de-las-Peñas et al., 2022 | Spain 1 March 2020–31 March 2021 | Case-control n = 264 Patients n = 88 Control n = 176 | Patients Mean age 52 y (SD 14.5) Controls Mean age 52.2 y (SD 14.2) | Hospital medical records Telephonic interview | Fatigue, Dyspnea, Memory loss, Skin rashes, Brain Fog, Gastrointestinal disorders, Concentration loss, Ageusia, Ocular disorders, Tachycardia, Pain, Anosmia, Headache, Sleep, Depression/Anxiety | Number of post-COVID-19 symptoms (IRR 1.51, 95% CI 1.24–1.84) * Sleep quality (OR 2.27, 95% CI 1.34–3.86) * Fatigue (OR 1.39; 95% CI 0.79–2.43) Dyspnea (OR 1.41; 95% CI 0.79–2.53) Anxiety (OR 1.75, 95% CI 0.82–3.72) Depression (OR 0.83, 95% CI 0.40–1.73) |
| Loosen et al., 2022 | Germany 1 March 2020–31 March 2021 | Retrospective Observational n = 50,402 | Mean age 48.8 y (SD 19.3) | Medical record | Fatigue, Abnormalities of breathing, Loss of smell and taste, disturbances in attention | Obesity (OR 1.25 95% CI 1.08–1.44) * Hypertension (OR 1.31, 95% CI 1.15–1.48) * |
| Shang et al., 2021 | Wuhan, China 20 February–20 March 2020 | Cohort Study n = 118 Patients n = 53 Controls n = 65 | Patients Mean age 51 y (IQR 41–58) Controls Mean age 57 y (IQR 48–62) | Interview, Physical exam, Blood sample, Lung function test, CT scan | Shortness of breath, Fatigue, Sleep problems, Joint pain, Smell disorder, Diarrhea, Constipation | No differences in the prevalence of long COVID-19 Symptoms existed between obese and non-obese patients. |
| Whitaker et al., 2022 | UK 15–28 September 2020 27 October–10 November 2020 25 January–8 February 2021 12–25 May 2021 | Cohort n = 606,434 | Age >18 | Online/telephone survey | Tiredness, Tight chest, Sore throat, Sore eyes, Sneezing, Shortness of breath, Fatigue, Runny nose, Skin lesions, Cough, Pain symptoms, Nausea, Vomiting, Loss of taste or smell, Hoarse voice, Headache, Dizziness, Difficulty sleeping, Diarrhoea, Chest pain, Abdominal pain | Persistence of one or more symptoms for 12 weeks or more Obesity (OR1.39, 95% CI 1.32–1.48) * |
| Chudzik et al., 2022 | Poland 1 September 2020–30 September 2021 | Retrospective observational n = 2218 | Mean age = 53.8 ± 13.5 years | Health questionnaire | Cough, Dyspnea, Fatigue, Hair loss, Olfactory disturbances, Headache, Pain, Brain fog | Presence of overall persistent symptoms Obesity (OR1.16, 95% CI 0.96–1.41) Fatigue (OR 1.49, 95% CI 1.24–1.80) * |
| Pulmonary Disease | ||||||
| Sudre et al., 2021 | UK 25 March–30 June 2020 | Prospective cohort n = 8364 COVID-19 n = 4182 No COVID-19 n = 4182 | Mean age 46 y | COVID-19 Symptom Study app1 | Abdominal pain, Chest pain, Sore throat, Fatigue, Shortness of breath, Hoarse voice, Delirium, Diarrhea, Fever, Cough, Muscle pain, Anosmia, Headache | Presence of long COVID-19 symptoms Asthma (OR 2.14, 95% CI 1.55–2.96) * |
| Munblit et al., 2021 | Russia 8 April–10 July 2020 | Prospective cohort n = 2649 | Median age 56 y | ISARIC Long-term Follow-up Study questionnaire | Fatigue, Shortness of breath, Forgetfulness | Asthma and chronic pulmonary disease were not associated with persistent symptoms overall, but asthma was associated with neurological (OR1.95, 95% CI 1.25–2.98) * and chronic pulmonary disease was associated with fatigue (OR 1.68, 95% CI 1.21–2.32) * |
| Philip et al., 2022 | UK October 2020 | Retrospective cohort n = 4500 COVID-19 n = 471 No COVID-19 n = 3036 COVID-19 n = 972 | Range age 50–59 y | Asthma UK and British Lung Foundation survey | Fatigue, Breathlessness, Pain (chest or whole body) | For many people with asthma, COVID-19 is associated with prolonged symptoms and worsening asthma control |
| Jia et al., 2022 | USA March 2020–February 2021 | Prospective cohort n = 637 Patients n = 617 Controls n = 20 | Patients Mean age 51 y Controls Mean age 54 y | Survey | Cough, Shortness of breath, Fever, Nausea, Vomiting | Comorbid lung disease, asthma and lower levels of initial IgG response to SARS-CoV-2 nucleocapsid antigen were associated with longer symptom duration (mean days: 55 versus 44 days; p = 0.04) * |
| Transplant | ||||||
| Oto et al., 2022 | Turkey 15 March 2021–11 June 2021 | Retrospective cohort n = 944 Patients n = 523 Control n = 421 | Mean age 46 y | Survey | Respiratory symptoms | Persistence of respiratory symptoms without increased risk of acute rejection, BK and CMV infection, thromboembolic event or urinary tract infection |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Notarte, K.I.; de Oliveira, M.H.S.; Peligro, P.J.; Velasco, J.V.; Macaranas, I.; Ver, A.T.; Pangilinan, F.C.; Pastrana, A.; Goldrich, N.; Kavteladze, D.; et al. Age, Sex and Previous Comorbidities as Risk Factors Not Associated with SARS-CoV-2 Infection for Long COVID-19: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 7314. https://doi.org/10.3390/jcm11247314
Notarte KI, de Oliveira MHS, Peligro PJ, Velasco JV, Macaranas I, Ver AT, Pangilinan FC, Pastrana A, Goldrich N, Kavteladze D, et al. Age, Sex and Previous Comorbidities as Risk Factors Not Associated with SARS-CoV-2 Infection for Long COVID-19: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(24):7314. https://doi.org/10.3390/jcm11247314
Chicago/Turabian StyleNotarte, Kin Israel, Maria Helena Santos de Oliveira, Princess Juneire Peligro, Jacqueline Veronica Velasco, Imee Macaranas, Abbygail Therese Ver, Flos Carmeli Pangilinan, Adriel Pastrana, Nathaniel Goldrich, David Kavteladze, and et al. 2022. "Age, Sex and Previous Comorbidities as Risk Factors Not Associated with SARS-CoV-2 Infection for Long COVID-19: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 11, no. 24: 7314. https://doi.org/10.3390/jcm11247314
APA StyleNotarte, K. I., de Oliveira, M. H. S., Peligro, P. J., Velasco, J. V., Macaranas, I., Ver, A. T., Pangilinan, F. C., Pastrana, A., Goldrich, N., Kavteladze, D., Gellaco, M. M. L., Liu, J., Lippi, G., Henry, B. M., & Fernández-de-las-Peñas, C. (2022). Age, Sex and Previous Comorbidities as Risk Factors Not Associated with SARS-CoV-2 Infection for Long COVID-19: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 11(24), 7314. https://doi.org/10.3390/jcm11247314