
Wearable Intelligent Machine Learning Rehabilitation Assessment for Stroke Patients Compared with Clinician Assessment
 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Participants and Protocol
2.1.1. Participants
2.1.2. Procedure
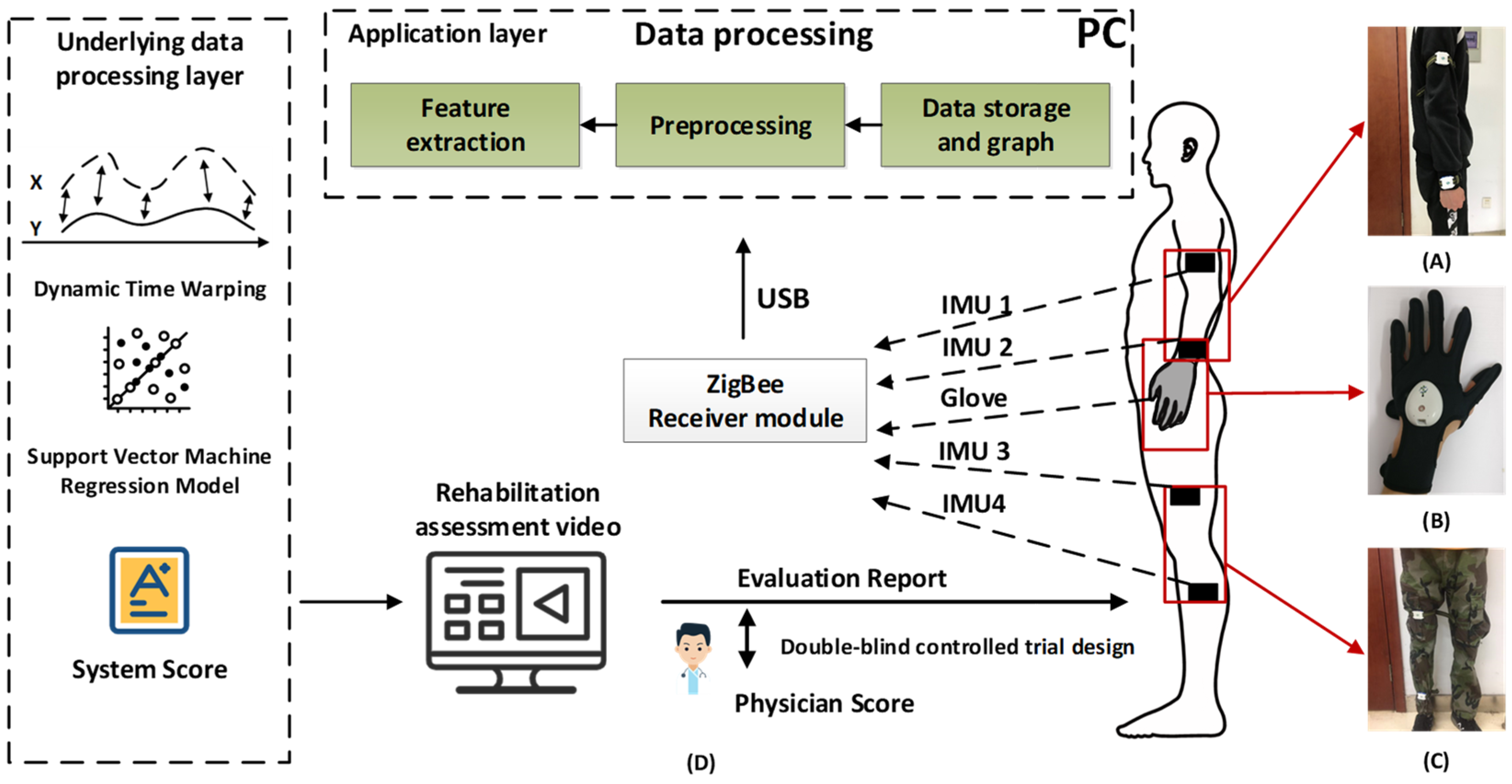
2.2. Intelligent Rehabilitation Assessment System
2.3. Machine Learning Model
2.3.1. Rehabilitation Assessment Movements
2.3.2. Establishment of Machine Learning Rehabilitation Assessment Model
2.4. Rehabilitation Assessment Software
2.5. Data Analysis
3. Result
3.1. Clinical Characteristics of Patients
3.2. Analysis of System Assessment Results
3.3. Analysis of System Deviation and Relative Deviation
3.4. Data Distribution Analysis of System Deviationand Relative Deviation
3.5. Analysis of Time Used for Scoring and Safety Report
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviation
| Abbreviation | Full name |
| SAS | Statistical analysis system |
| CI | Confidence intervals |
| SD | Standard deviation |
| CFDA | China Food and Drug Administration |
| EMG | Electromyography |
| IMU | Inertial measurement unit |
| FMA | Fugl–Meyer assessment |
| DTW | Dynamic time warping |
| SVR | Support vector regression |
| t-test | Student’s t test |
References
- Lin, B.; Zhang, Z.; Mei, Y.; Wang, C.; Xu, H.; Liu, L.; Wang, W. Cumulative risk of stroke recurrence over the last 10 years: A systematic review and meta-analysis. Neurol. Sci. 2021, 42, 61–71. [Google Scholar] [CrossRef] [PubMed]
- Dobkin, B.H. Strategies for stroke rehabilitation. Lancet Neurol. 2004, 3, 528–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rech, K.D.; Salazar, A.P.; Marchese, R.; Schifino, G.; Cimolin, V.; Pagnussat, A.S. Fugl-Meyer Assessment Scores Are Related With Kinematic Measures in People with Chronic Hemiparesis after Stroke. J. Stroke Cereb. Dis. 2020, 29, 104463. [Google Scholar] [CrossRef] [Green Version]
- Hernández, E.D.; Forero, S.M.; Galeano, C.P.; Barbosa, N.E.; Sunnerhagen, K.S.; Murphy, M.A. Intra- and inter-rater reliability of Fugl-Meyer Assessment of Lower Extremity early after stroke. Braz. J. Phys. Ther. 2021, 25, 709–718. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.-Y.; Lin, G.-H.; Huang, Y.-J.; Song, C.-Y.; Lee, Y.-C.; How, M.-J.; Chen, Y.-M.; Hsueh, I.-P.; Chen, M.-H.; Hsieh, C.-L. Improving the utility of the Brunnstrom recovery stages in patients with stroke: Validation and quantification. Medicine 2016, 95, e4508. [Google Scholar] [CrossRef] [PubMed]
- Naghdi, S.; Ansari, N.N.; Mansouri, K.; Hasson, S. A neurophysiological and clinical study of Brunnstrom recovery stages in the upper limb following stroke. Brain Inj. 2010, 24, 1372–1378. [Google Scholar] [CrossRef] [PubMed]
- Gladstone, D.; Danells, C.J.; Black, S. The Fugl-Meyer assessment of motor recovery after stroke: A critical review of its measurement properties. Neurorehabil. Neural Repair. 2002, 16, 232–240. [Google Scholar] [CrossRef]
- Hsueh, I.-P.; Hsu, M.; Sheu, C.-F.; Lee, S.; Hsieh, C.-L.; Lin, J.-H. Psychometric comparisons of 2 versions of the Fugl-Meyer Motor Scale and 2 versions of the Stroke Rehabilitation Assessment of Movement. Neurorehabilit. Neural Repair 2008, 22, 737–744. [Google Scholar] [CrossRef]
- Massé, F.; Gonzenbach, R.R.; Arami, A.; Paraschiv-Ionescu, A.; Luft, A.R.; Aminian, K. Improving activity recognition using a wearable barometric pressure sensor in mobility-impaired stroke patients. J. Neuroeng. Rehabil. 2015, 12, 72. [Google Scholar] [CrossRef] [Green Version]
- Pan, D.; Liu, H.; Qu, D.; Zhang, Z. Human Falling Detection Algorithm Based on Multisensor Data Fusion with SVM. Mob. Inf. Syst. 2020, 2020, 8826088. [Google Scholar] [CrossRef]
- Tognetti, A.; Lorussi, F.; Bartalesi, R.; Quaglini, S.; Tesconi, M.; Zupone, G.; De Rossi, D. Wearable kinesthetic system for capturing and classifying upper limb gesture in post-stroke rehabilitation. J. Neuroeng. Rehabil. 2005, 2, 8. [Google Scholar] [CrossRef] [PubMed]
- Pizzolato, S.; Tagliapietra, L.; Cognolato, M.; Reggiani, M.; Müller, H.; Atzori, M. Comparison of six electromyography acquisition setups on hand movement classification tasks. PLoS ONE 2017, 12, e0186132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panwar, M.; Biswas, D.; Bajaj, H.; Jobges, M.; Turk, R.; Maharatna, K.; Acharyya, A. Rehab-Net: Deep Learning Framework for Arm Movement Classification Using Wearable Sensors for Stroke Rehabilitation. IEEE Trans Biomed. Eng. 2019, 66, 3026–3037. [Google Scholar] [CrossRef]
- Jochumsen, M.; Niazi, I.K.; Navid, M.S.; Anwar, M.N.; Farina, D.; Dremstrup, K. Online multi-class brain-computer interface for detection and classification of lower limb movement intentions and kinetics for stroke rehabilitation. Brain Comput. Interfaces 2015, 2, 202–210. [Google Scholar] [CrossRef]
- Yang, G.; Deng, J.; Pang, G.; Zhang, H.; Li, J.; Deng, B.; Pang, Z.; Xu, J.; Jiang, M.; Liljeberg, P.; et al. An IoT-Enabled Stroke Rehabilitation System Based on Smart Wearable Armband and Machine Learning. IEEE J. Transl. Eng. Health Med. 2018, 6, 2100510. [Google Scholar] [CrossRef]
- Li, Y.; Zhang, X.; Gong, Y.; Cheng, Y.; Gao, X.; Chen, X. Motor Function Evaluation of Hemiplegic Upper-Extremities Using Data Fusion from Wearable Inertial and Surface EMG Sensors. Sensors 2017, 17, 582. [Google Scholar] [CrossRef] [Green Version]
- Salazar, A.J.; Silva, A.S.; Silva, C.; Borges, C.M.; Correia, M.V.; Santos, R.S.; Vilas-Boas, J.P. Low-cost wearable data acquisition for stroke rehabilitation: A proof-of-concept study on accelerometry for functional task assessment. Top. Stroke Rehabil. 2014, 21, 12–22. [Google Scholar] [CrossRef]
- Torriani-Pasin, C.; Demers, M.; Polese, J.C.; Bishop, L.; Wade, E.; Hempel, S.; Winstein, C. mHealth technologies used to capture walking and arm use behavior in adult stroke survivors: A scoping review beyond measurement properties. Disabil. Rehabil. 2021, 23, 6094–6106. [Google Scholar] [CrossRef]
- Leuenberger, K.; Gonzenbach, R.; Wachter, S.; Luft, A.; Gassert, R. A method to qualitatively assess arm use in stroke survivors in the home environment. Med. Biol. Eng. Comput. 2017, 55, 141–150. [Google Scholar] [CrossRef] [Green Version]
- Yu, L.; Xiong, D.; Guo, L.; Wang, J. A remote quantitative Fugl-Meyer assessment framework for stroke patients based on wearable sensor networks. Comput. Methods Programs Biomed. 2016, 128, 100–110. [Google Scholar] [CrossRef]
- González-Ortega, D.; Díaz, F.J.; Martínez-Zarzuela, M.; Antón-Rodríguez, M. A Kinect-based system for cognitive rehabilitation exercises monitoring. Comput. Methods Programs Biomed. 2014, 113, 620–631. [Google Scholar] [CrossRef] [PubMed]
- Aşkın, A.; Atar, E.; Koçyiğit, H.; Tosun, A. Effects of Kinect-based virtual reality game training on upper extremity motor recovery in chronic stroke. Somatosens. Mot. Res. 2018, 35, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Liao, W.-W.; Waller, S.M.; Whitall, J. Kinect-based individualized upper extremity rehabilitation is effective and feasible for individuals with stroke using a transition from clinic to home protocol. Cogent Med. 2018, 5, 1412121. [Google Scholar] [CrossRef]
- Wang, C.; Peng, L.; Hou, Z.-G.; Li, J.; Zhang, T.; Zhao, J. Quantitative Assessment of Upper-Limb Motor Function for Post-Stroke Rehabilitation Based on Motor Synergy Analysis and Multi-Modality Fusion. IEEE Trans. Neural. Syst. Rehabil. Eng. 2020, 28, 943–952. [Google Scholar] [CrossRef]
- Knorr, B.; Hughes, R.; Sherrill, D.; Stein, J.; Akay, M.; Bonato, P. (Eds.) Quantitative measures of functional upper limb movement in persons after stroke. In Proceedings of the 2nd International IEEE EMBS Conference on Neural Engineering, Arlington, VA, USA, 16–19 March; IEEE: Piscataway, NJ, USA, 2005. [Google Scholar]
- Held, J.P.O.; Yu, K.; Pyles, C.; Veerbeek, J.M.; Bork, F.; Heining, S.-M.; Navab, N.; Luft, A.R. Augmented Reality-Based Rehabilitation of Gait Impairments: Case Report. JMIR mHealth uHealth 2020, 8, e17804. [Google Scholar] [CrossRef] [PubMed]
- Lin, G.-H.; Li, C.-Y.; Sheu, C.-F.; Huang, C.-Y.; Lee, S.-C.; Huang, Y.-H.; Hsieh, C.-L. Using Machine Learning to Develop a Short-Form Measure Assessing 5 Functions in Patients With Stroke. Arch. Phys. Med. Rehabil. 2021, 103, 1574–1581. [Google Scholar] [CrossRef]
- Zhu, L.; Najafizadeh, L. Dynamic time warping-based averaging framework for functional near-infrared spectroscopy brain imaging studies. J. Biomed. Opt. 2017, 22, 66011. [Google Scholar] [CrossRef]
- Fu, T.-C. A review on time series data mining. Eng. Appl. Artif. Intell. 2011, 24, 164–181. [Google Scholar] [CrossRef]
- Zhang, M.; Chen, J.; Ling, Z.; Zhang, B.; Yan, Y.; Xiong, D.; Guo, L. Quantitative Evaluation System of Upper Limb Motor Function of Stroke Patients Based on Desktop Rehabilitation Robot. Sensors 2022, 22, 1170. [Google Scholar] [CrossRef]
- Ding, K.; Zhang, B.; Ling, Z.; Chen, J.; Guo, L.; Xiong, D.; Wang, J. Quantitative Evaluation System of Wrist Motor Function for Stroke Patients Based on Force Feedback. Sensors 2022, 22, 3368. [Google Scholar] [CrossRef]
- Lorussi, F.; Carbonaro, N.; De Rossi, D.; Paradiso, R.; Veltink, P.; Tognetti, A. Wearable Textile Platform for Assessing Stroke Patient Treatment in Daily Life Conditions. Front. Bioeng. Biotechnol. 2016, 4, 28. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Mean (SD) | Min–Max | 95% CI |
|---|---|---|---|
| Age | 56.47 ± 9.70 | 33.00–74.00 | 54.71–58.22 |
| Height | 167.80 ± 6.95 | 150.00–180.00 | 166.50–169.00 |
| Weight | 69.68 ± 10.95 | 48.00–114.00 | 67.69–71.66 |
| Pulse | 77.59 ± 7.95 | 60.00–110.00 | 76.16–79.03 |
| Systolic pressure | 128.8 ± 12.71 | 92.00–116.00 | 126.50–131.10 |
| Diastolic pressure | 81.75 ± 9.25 | 57.00–107.00 | 80.08–83.42 |
| Respiratory rate | 18.89 ± 1.68 | 13.00–26.00 | 18.59–19.20 |
| Item | Physician’s FMA Score | Assessment System Score | |
|---|---|---|---|
| Total score | Mean ± SD | 41.48 ± 26.35 | 41.78 ± 25.42 |
| 95% CI | 36.72–46.25 | 37.19–46.38 | |
| Upper-limb score | Mean ± SD | 24.03 ± 19.26 | 24.62 ± 18.35 |
| 95% CI | 20.55–27.51 | 21.27–27.97 | |
| Lower-limb score | Mean ± SD | 17.45 ± 8.79 | 17.17 ± 9.21 |
| 95% CI | 15.86–19.04 | 15.50–18.83 |
| Item | Intercept | Slope | 95% CI of Slope | R2 | p Value |
|---|---|---|---|---|---|
| Total score | 2.43 | 0.95 | 0.92–0.98 | 0.9667 | 0.0001 ** |
| Upper-limb score | 1.98 | 0.94 | 0.90–0.98 | 0.9577 | 0.0001 ** |
| Lower-limb score | 0.22 | 0.97 | 0.90–1.04 | 0.8575 | 0.0001 ** |
| Item | Score Deviation | Relative Deviation (%) | |
|---|---|---|---|
| Total score | Mean ± SD | 0.30 ± 4.83 | 3.49 ± 16.55 |
| 95% CI | −0.57–1.17 | 0.50–6.48 | |
| Upper-limb score | Mean ± SD | 0.58 ± 3.97 | 7.20 ± 26.77 |
| 95% CI | −0.13–1.30 | 2.36–12.04 | |
| Lower-limb score | Mean ± SD | −0.28 ± 3.49 | −0.78 ± 25.77 |
| 95% CI | −0.91–0.35 | −5.44–3.88 |
| Item | Deviation Distribution (%) | Relative Deviation Distribution (%) | |
|---|---|---|---|
| Total score | Outside of Mean ± 1.96 SD | 9 ± 7.50 | 5 ± 4.17 |
| Within Mean ± 1.96 SD | 111 ± 92.50 | 115 ± 95.83 | |
| Upper score | Outside of Mean ± 1.96 SD | 6 ± 5.00 | 5 ± 4.17 |
| Within Mean ± 1.96 SD | 114 ± 95.00 | 115 ± 95.83 | |
| Lower score | Outside of Mean ± 1.96 SD | 5 ± 4.17 | 4 ± 3.33 |
| Within Mean ± 1.96 SD | 115 ± 95.83 | 116 ± 96.67 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, L.; Zhang, B.; Wang, J.; Wu, Q.; Li, X.; Zhou, L.; Xiong, D. Wearable Intelligent Machine Learning Rehabilitation Assessment for Stroke Patients Compared with Clinician Assessment. J. Clin. Med. 2022, 11, 7467. https://doi.org/10.3390/jcm11247467
Guo L, Zhang B, Wang J, Wu Q, Li X, Zhou L, Xiong D. Wearable Intelligent Machine Learning Rehabilitation Assessment for Stroke Patients Compared with Clinician Assessment. Journal of Clinical Medicine. 2022; 11(24):7467. https://doi.org/10.3390/jcm11247467
Chicago/Turabian StyleGuo, Liquan, Bochao Zhang, Jiping Wang, Qunqiang Wu, Xinming Li, Linfu Zhou, and Daxi Xiong. 2022. "Wearable Intelligent Machine Learning Rehabilitation Assessment for Stroke Patients Compared with Clinician Assessment" Journal of Clinical Medicine 11, no. 24: 7467. https://doi.org/10.3390/jcm11247467
APA StyleGuo, L., Zhang, B., Wang, J., Wu, Q., Li, X., Zhou, L., & Xiong, D. (2022). Wearable Intelligent Machine Learning Rehabilitation Assessment for Stroke Patients Compared with Clinician Assessment. Journal of Clinical Medicine, 11(24), 7467. https://doi.org/10.3390/jcm11247467