

Statins Use in Patients with Cardiovascular Diseases and COVID-19 Outcomes: An Italian Population-Based Cohort Study

 , ,
, ,  , ,
, ,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Source
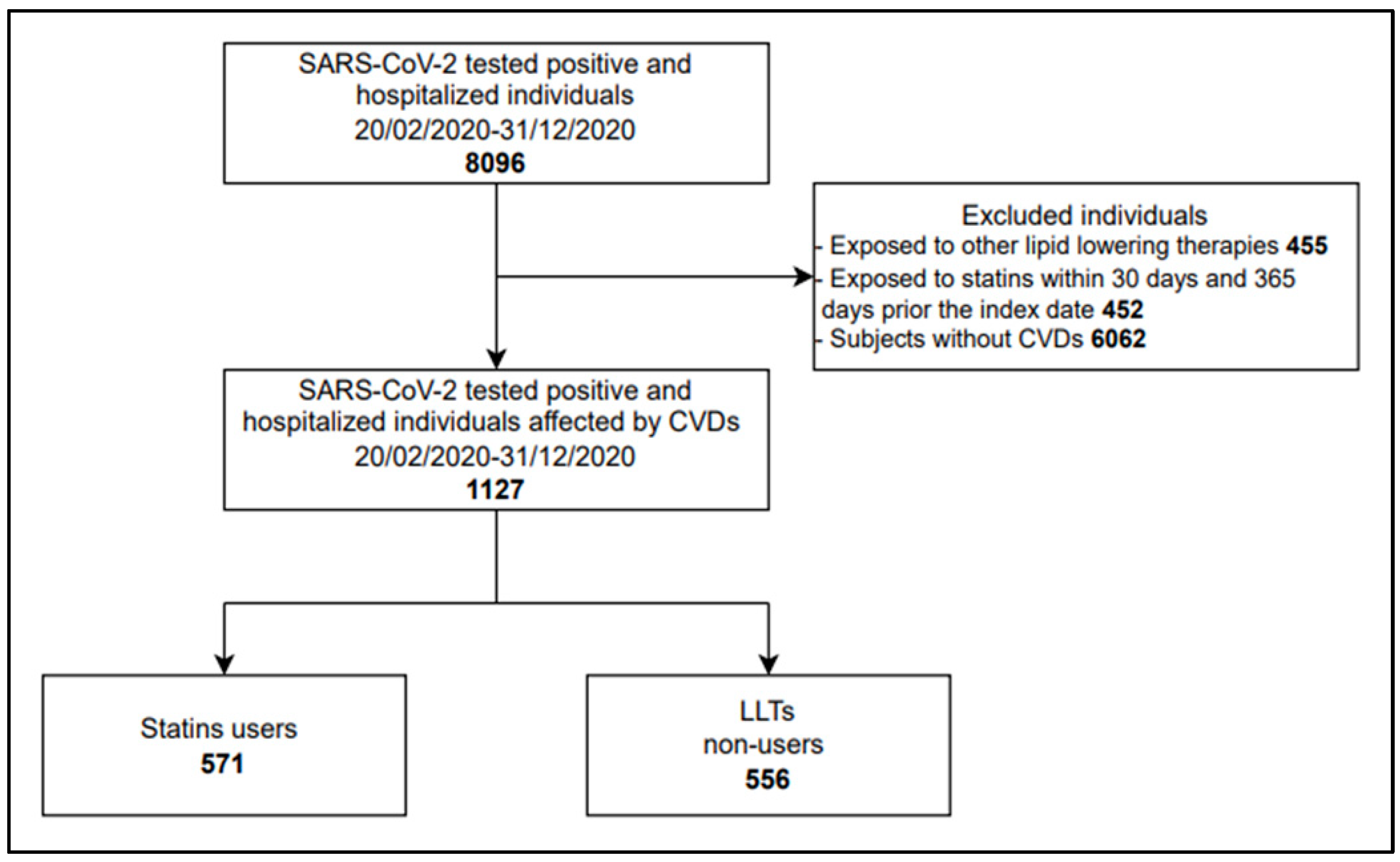
2.2. Study Population
2.3. Study Groups
2.4. Outcome
2.5. Patients’ Characteristics
2.6. Statistical Analysis
3. Results
3.1. Descriptive Statistics
3.2. Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). Timeline: WHO’s COVID-19 Response. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/interactive-timeline#! (accessed on 13 December 2022).
- Chow, R.; Simone, C.B., 2nd; Lock, M. Hydroxychloroquine for the treatment of COVID-19: The importance of scrutiny of positive trials. Ann. Palliat. Med. 2020, 9, 3716–3720. [Google Scholar] [CrossRef]
- Wu, K.S.; Lin, P.C.; Chen, Y.S.; Pan, T.C.; Tang, P.L. The use of statins was associated with reduced COVID-19 mortality: A systematic review and meta-analysis. Ann. Med. 2021, 53, 874–884. [Google Scholar] [CrossRef] [PubMed]
- Schiavone, M.; Gobbi, C.; Biondi-Zoccai, G.; D’Ascenzo, F.; Palazzuoli, A.; Gasperetti, A.; Mitacchione, G.; Viecca, M.; Galli, M.; Fedele, F.; et al. Acute Coronary Syndromes and Covid-19: Exploring the Uncertainties. J. Clin. Med. 2020, 9, 1683. [Google Scholar] [CrossRef] [PubMed]
- Lamers, M.M.; Haagmans, B.L. SARS-CoV-2 pathogenesis. Nat. Rev. Microbiol. 2022, 20, 270–284. [Google Scholar] [CrossRef] [PubMed]
- Subir, R.; Jagat, J.M.; Kalyan, K.G. Pros and cons for use of statins in people with coronavirus disease-19 (COVID-19). Diabetes Metab. Syndr. 2020, 14, 1225–1229. [Google Scholar] [CrossRef]
- Fajgenbaum, D.C.; Rader, D.J. Teaching Old Drugs New Tricks: Statins for COVID-19? Cell Metab. 2020, 32, 145–147. [Google Scholar] [CrossRef]
- Schönbeck, U.; Libby, P. Inflammation, immunity, and HMG-CoA reductase inhibitors: Statins as antiinflammatory agents? Circulation 2004, 109, II18–II26. [Google Scholar] [CrossRef] [Green Version]
- Minz, M.M.; Bansal, M.; Kasliwal, R.R. Statins and SARS-CoV-2 disease: Current concepts and possible benefits. Diabetes Metab. Syndr. 2020, 14, 2063–2067. [Google Scholar] [CrossRef]
- Ganjali, S.; Bianconi, V.; Penson, P.E.; Pirro, M.; Banach, M.; Watts, G.F.; Sahebkar, A. Commentary: Statins, COVID-19, and coronary artery disease: Killing two birds with one stone. Metabolism 2020, 113, 154375. [Google Scholar] [CrossRef]
- Castiglione, V.; Chiriacò, M.; Emdin, M.; Taddei, S.; Vergaro, G. Statin therapy in COVID-19 infection. Eur. Heart J. Cardiovasc. Pharmacother. 2020, 6, 258–259. [Google Scholar] [CrossRef]
- Vahedian-Azimi, A.; Mohammadi, S.M.; Banach, M.; Beni, F.H.; Guest, P.C.; Al-Rasadi, K.; Jamialahmadi, T.; Sahebkar, A. Improved COVID-19 Outcomes following Statin Therapy: An Updated Systematic Review and Meta-analysis. BioMed Res. Int. 2021, 2021, 1901772. [Google Scholar] [CrossRef] [PubMed]
- Hariyanto, T.I.; Kurniawan, A. Statin and outcomes of coronavirus disease 2019 (COVID-19): A systematic review, meta-analysis, and meta-regression. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 1662–1670. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Arocutipa, C.; Melgar-Talavera, B.; Alvarado-Yarasca, Á.; Saravia-Bartra, M.M.; Cazorla, P.; Belzusarri, I.; Hernandez, A.V. Statins reduce mortality in patients with COVID-19: An updated meta-analysis of 147 824 patients. Int. J. Infect. Dis. 2021, 110, 374–381. [Google Scholar] [CrossRef]
- Kow, C.S.; Hasan, S.S. The Association Between the Use of Statins and Clinical Outcomes in Patients with COVID-19: A Systematic Review and Meta-analysis. Am. J. Cardiovasc. Drugs 2022, 22, 167–181. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Pal, R.; Banerjee, M.; Yadav, U.; Bhattacharjee, S. Statin use and clinical outcomes in patients with COVID-19: An updated systematic review and meta-analysis. Postgrad. Med. J. 2022, 98, 354–359. [Google Scholar] [CrossRef]
- Permana, H.; Huang, I.; Purwiga, A.; Kusumawardhani, N.Y.; Sihite, T.A.; Martanto, E.; Wisaksana, R.; Soetedjo, N.N.M. In-hospital use of statins is associated with a reduced risk of mortality in coronavirus-2019 (COVID-19): Systematic review and meta-analysis. Pharmacol. Rep. 2021, 73, 769–780. [Google Scholar] [CrossRef]
- Bikdeli, B.; Talasaz, A.H.; Rashidi, F.; Sharif-Kashani, B.; Farrokhpour, M.; Bakhshandeh, H.; Sezavar, H.; Dabbagh, A.; Beigmohammadi, M.T.; Payandemehr, P.; et al. Intermediate versus standard-dose prophylactic anticoagulation and statin therapy versus placebo in critically-ill patients with COVID-19: Rationale and design of the INSPIRATION/INSPIRATION-S studies. Thromb. Res. 2020, 196, 382–394. [Google Scholar] [CrossRef]
- Hariyanto, T.I.; Kurniawan, A. Statin therapy did not improve the in-hospital outcome of coronavirus disease 2019 (COVID-19) infection. Diabetes Metab. Syndr. 2020, 14, 1613–1615. [Google Scholar] [CrossRef]
- Mitacchione, G.; Schiavone, M.; Curnis, A.; Arca, M.; Antinori, S.; Gasperetti, A.; Mascioli, G.; Severino, P.; Sabato, F.; Caracciolo, M.M.; et al. Impact of prior statin use on clinical outcomes in COVID-19 patients: Data from tertiary referral hospitals during COVID-19 pandemic in Italy. J. Clin. Lipidol. 2021, 15, 68–78. [Google Scholar] [CrossRef]
- Ayeh, S.K.; Abbey, E.J.; Khalifa, B.A.A.; Nudotor, R.D.; Osei, A.D.; Chidambaram, V.; Osuji, N.; Khan, S.; Salia, E.L.; Oduwole, M.O.; et al. Statins use and COVID-19 outcomes in hospitalized patients. PLoS ONE 2021, 16, e0256899. [Google Scholar] [CrossRef] [PubMed]
- El-Solh, A.A.; Lawson, Y.; El-Solh, D.A. All-cause mortality in COVID-19 patients receiving statin therapy: Analysis of veterans affairs database cohort study. Intern. Emerg. Med. 2022, 17, 685–694. [Google Scholar] [CrossRef] [PubMed]
- Bansal, M. Cardiovascular disease and COVID-19. Diabetes Metab. Syndr. 2020, 14, 247–250. [Google Scholar] [CrossRef] [PubMed]
- Nishiga, M.; Wang, D.W.; Han, Y.; Lewis, D.B.; Wu, J.C. COVID-19 and cardiovascular disease: From basic mechanisms to clinical perspectives. Nat. Rev. Cardiol. 2020, 17, 543–558. [Google Scholar] [CrossRef]
- Harrison, S.L.; Buckley, B.J.R.; Rivera-Caravaca, J.M.; Zhang, J.; Lip, G.Y.H. Cardiovascular risk factors, cardiovascular disease, and COVID-19: An umbrella review of systematic reviews. Eur. Heart J. Qual. Care Clin. Outcomes 2021, 7, 330–339. [Google Scholar] [CrossRef]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, e596–e646, Erratum in Circulation 2019, 140, e649–e650; Erratum in Circulation 2020, 141, e60; Erratum in Circulation 2020, 141, e774. [Google Scholar] [CrossRef]
- Andrade, S.E.; Kahler, K.H.; Frech, F.; Chan, K.A. Methods for evaluation of medication adherence and persistence using automated databases. Pharmacoepidemiol. Drug. Saf. 2006, 15, 565–574; discussion 575–577. [Google Scholar] [CrossRef]
- Ikari, Y.; Matsue, Y.; Torii, S.; Hasegawa, M.; Aihara, K.; Kuroda, S.; Sano, T.; Kitai, T.; Yonetsu, T.; Kohsaka, S.; et al. Association Between Statin Use Prior to Admission and Lower Coronavirus Disease 2019 (COVID-19) Severity in Patients with Cardiovascular Disease or Risk Factors. Circ. J. 2021, 85, 939–943. [Google Scholar] [CrossRef]
- Saad, M.; Kennedy, K.F.; Louis, D.W.; Imran, H.; Sherrod, C.F., 4th; Aspry, K.; Mentias, A.; Poppas, A.; Abbott, J.D.; Aronow, H.D. Preadmission Statin Treatment and Outcome in Patients Hospitalized with COVID-19. Am. J. Cardiol. 2022, 177, 28–33. [Google Scholar] [CrossRef]
- Daniels, L.B.; Ren, J.; Kumar, K.; Bui, Q.M.; Zhang, J.; Zhang, X.; Sawan, M.A.; Eisen, H.; Longhurst, C.A.; Messer, K. Relation of prior statin and anti-hypertensive use to severity of disease among patients hospitalized with COVID-19: Findings from the American Heart Association’s COVID-19 Cardiovascular Disease Registry. PLoS ONE 2021, 16, e0254635. [Google Scholar] [CrossRef]
- Terlecki, M.; Wojciechowska, W.; Klocek, M.; Olszanecka, A.; Stolarz-Skrzypek, K.; Grodzicki, T.; Małecki, M.; Katra, B.; Garlicki, A.; Bociąga-Jasik, M.; et al. Association between cardiovascular disease, cardiovascular drug therapy, and in-hospital outcomes in patients with COVID-19: Data from a large single-center registry in Poland. Kardiol. Pol. 2021, 79, 773–780. [Google Scholar] [CrossRef] [PubMed]
- Scheen, A.J. Statins and clinical outcomes with COVID-19: Meta-analyses of observational studies. Diabetes Metab. 2021, 47, 101220. [Google Scholar] [CrossRef] [PubMed]
- Reiner, Ž.; Hatamipour, M.; Banach, M.; Pirro, M.; Al-Rasadi, K.; Jamialahmadi, T.; Radenkovic, D.; Montecucco, F.; Sahebkar, A. Statins and the COVID-19 main protease: In silico evidence on direct interaction. Arch. Med. Sci. 2020, 16, 490–496. [Google Scholar] [CrossRef]
- Totura, A.L.; Whitmore, A.; Agnihothram, S.; Schäfer, A.; Katze, M.G.; Heise, M.T.; Baric, R.S. Toll-like Receptor 3 Signaling via TRIF Contributes to a Protective Innate Immune Response to Severe Acute Respiratory Syndrome Coronavirus Infection. mBio 2015, 6, e00638-15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dashti-Khavidaki, S.; Khalili, H. Considerations for Statin Therapy in Patients with COVID-19. Pharmacotherapy 2020, 40, 484–486. [Google Scholar] [CrossRef] [Green Version]
- Maragaritis, M.; Channon, K.M.; Antoniades, C. Statins as regulators of redox in the vascular endothelium: Beyond lipid lowering. Antioxid. Redox Signal. 2014, 20, 1198–1215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in Covid-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef]
- Volpato, S.; Palmieri, E.; Fellin, R.; Zuliani, G. Acute phase markers are associated with reduced plasma lipid levels in a population of hospitalized elderly patients. Gerontology 2000, 46, 22–27. [Google Scholar] [CrossRef]
- Deniz, O.; Gumus, S.; Yaman, H.; Ciftci, F.; Ors, F.; Cakir, E.; Tozkoparan, E.; Bilgic, H.; Ekiz, K. Serum total cholesterol, HDL-C and LDL-C concentrations significantly correlate with the radiological extent of disease and the degree of smear positivity in patients with pulmonary tuberculosis. Clin. Biochem. 2007, 40, 162–166. [Google Scholar] [CrossRef]
- Deniz, O.; Tozkoparan, E.; Yaman, H.; Cakir, E.; Gumus, S.; Ozcan, O.; Bozlar, U.; Bilgi, C.; Bilgic, H.; Ekiz, K. Serum HDL-C levels, log (TG/HDL-C) values and serum total cholesterol/HDL-C ratios significantly correlate with radiological extent of disease in patients with community-acquired pneumonia. Clin. Biochem. 2006, 39, 287–292. [Google Scholar] [CrossRef]
- Zeiser, R. Immune modulatory effects of statins. Immunology 2018, 154, 69–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kočar, E.; Režen, T.; Rozman, D. Cholesterol, lipoproteins, and COVID-19: Basic concepts and clinical applications. Biochim. Biophys. Acta Mol. Cell Biol. Lipids 2021, 1866, 158849. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Torres, I.; Guarner-Lans, V.; Soria-Castro, E.; Manzano-Pech, L.; Palacios-Chavarría, A.; Valdez-Vázquez, R.R.; Domínguez-Cherit, J.G.; Herrera-Bello, H.; Castillejos-Suastegui, H.; Moreno-Castañeda, L.; et al. Alteration in the Lipid Profile and the Desaturases Activity in Patients with Severe Pneumonia by SARS-CoV-2. Front. Physiol. 2021, 12, 667024. [Google Scholar] [CrossRef] [PubMed]
- Shen, L.; Qiu, L.; Wang, L.; Huang, H.; Liu, D.; Xiao, Y.; Liu, Y.; Jin, J.; Liu, X.; Wang, D.W.; et al. Statin Use and In-hospital Mortality in Patients with COVID-19 and Coronary Heart Disease. Sci. Rep. 2021, 11, 23874. [Google Scholar] [CrossRef] [PubMed]
- Nowak, M.M.; Niemczyk, M.; Florczyk, M.; Kurzyna, M.; Pączek, L. Effect of Statins on All-Cause Mortality in Adults: A Systematic Review and Meta-Analysis of Propensity Score-Matched Studies. J. Clin. Med. 2022, 11, 5643. [Google Scholar] [CrossRef] [PubMed]
- Antonazzo, I.C.; Fornari, C.; Rozza, D.; Conti, S.; Pasquale, R.D.; Cortesi, P.; Kaleci, S.; Ferrara, P.; Zucchi, A.; Maifredi, G.; et al. Azithromycin use and outcomes in COVID-19 patients: An observational real-world study. Int. J. Infect. Dis. 2022, 124, 27–34. [Google Scholar] [CrossRef]
- Shrank, W.H.; Patrick, A.R.; Brookhart, M.A. Healthy user and related biases in observational studies of preventive interventions: A primer for physicians. J. Gen. Intern. Med. 2011, 26, 546–550. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Statins User (N = 571) | Non-LLT User (N = 556) | Total (N = 1127) |
|---|---|---|---|
| N | 571 | 556 | 1127 |
| Female | 176 (30.8%) | 239 (43.0%) * | 415 (36.8%) |
| Age mean ± SD | 76.8 (8.5) | 76.3 (12.3) | 76.6 (10.5) |
| Age groups | |||
| 0–44 | 0 (0.0%) | 7 (1.3%) * | 7 (0.6%) |
| 45–64 | 59 (10.3%) | 89 (16%) * | 148 (13.1%) |
| ≥65 | 512 (89.7%) | 460 (82.7%) * | 972 (86.2%) |
| Previous statins exposure, N (%) | |||
| Atorvastatin | 345 (60.4%) | --- | --- |
| Simvastatin | 114 (20.0%) | --- | --- |
| Rosuvastatin | 93 (16.3%) | --- | --- |
| Pravastatin | 12 (2.1%) | --- | --- |
| Fluvastatin | 6 (1.1%) | --- | --- |
| Lovastatin | 1 (0.2%) | --- | --- |
| Statins adherence groups, N (%) | |||
| ≥80% | 406 (71.1%) | --- | --- |
| 50–79% | 105 (18.4%) | --- | --- |
| <50% | 60 (10.5%) | --- | --- |
| Comorbidity, N (%) | |||
| Alzheimer/Dementia | 12 (2.1%) | 41 (7.4%) * | 53 (4.7%) |
| Respiratory disease | 71 (12.4%) | 83 (14.9%) | 154 (13.7%) |
| Other cardiac diseases | 268 (46.9%) | 269 (48.4%) | 537 (47.6%) |
| Hypertension | 470 (82.3%) | 398 (71.6%) * | 868 (77%) |
| Dyslipidemia | 477 (83.5%) | 63 (11.3%) * | 540 (47.9%) |
| Diabetes | 228 (39.9%) | 146 (26.3%) * | 374 (33.2%) |
| Chronic liver disease | 66 (11.6%) | 85 (15.3%) | 151 (13.4%) |
| Rheumatic disease | 19 (3.3%) | 9 (1.6%) | 28 (2.5%) |
| Cancer | 66 (11.6%) | 80 (14.4%) | 146 (13.0%) |
| HIV | 1 (0.2%) | 1 (0.2%) | 2 (0.2%) |
| Concomitant therapies within 3 months, N (%) | |||
| Anticoagulants | 190 (33.3%) | 12 (2.2%) * | 202 (17.9%) |
| Corticosteroids for systemic use | 63 (11.0%) | 65 (11.7%) | 128 (11.4%) |
| Nonsteroidal anti-inflammatory drugs | 40 (7.0%) | 37 (6.7%) | 77 (6.8%) |
| Chloroquine, hydroxychloroquine | 13 (2.3%) | 12 (2.2%) | 25 (2.2%) |
| Immunosuppressant drugs | 4 (0.7%) | 9 (1.6%) | 13 (1.2%) |
| N. different ATC (5 level), median (q1–q3) | 5 (4–7) | 3 (1–5) * | 4 (2–6) |
| Outcome | Number of Events | Unadjusted Relative Risk * | Adjusted Relative Risk *,§ |
|---|---|---|---|
| ICU access | |||
| Non-LLT user | 30 (5.4%) | Reference | Reference |
| Statins user | 31 (5.4%) | 1.01 (0.60, 1.69) | 0.54 (0.22, 1.32) |
| Mechanical ventilation | |||
| Non-LLT user | 21 (3.8%) | Reference | Reference |
| Statins user | 29 (5.1%) | 1.36 (0.77, 2.42) | 1.00 (0.38, 2.67) |
| Mortality at 14 days | |||
| Non-LLT user | 32 (5.8%) | Reference | Reference |
| Statins user | 19 (3.3%) | 0.57 (0.32, 1.01) | 0.42 (0.16, 1.10) |
| Mortality at 30 days | |||
| Non-LLT user | 51 (9.2%) | Reference | Reference |
| Statins user | 31 (9.2%) | 0.58 (0.37, 0.91) | 0.39 (0.18, 0.85) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antonazzo, I.C.; Fornari, C.; Rozza, D.; Conti, S.; Di Pasquale, R.; Cortesi, P.A.; Kaleci, S.; Ferrara, P.; Zucchi, A.; Maifredi, G.; et al. Statins Use in Patients with Cardiovascular Diseases and COVID-19 Outcomes: An Italian Population-Based Cohort Study. J. Clin. Med. 2022, 11, 7492. https://doi.org/10.3390/jcm11247492
Antonazzo IC, Fornari C, Rozza D, Conti S, Di Pasquale R, Cortesi PA, Kaleci S, Ferrara P, Zucchi A, Maifredi G, et al. Statins Use in Patients with Cardiovascular Diseases and COVID-19 Outcomes: An Italian Population-Based Cohort Study. Journal of Clinical Medicine. 2022; 11(24):7492. https://doi.org/10.3390/jcm11247492
Chicago/Turabian StyleAntonazzo, Ippazio Cosimo, Carla Fornari, Davide Rozza, Sara Conti, Raffaella Di Pasquale, Paolo Angelo Cortesi, Shaniko Kaleci, Pietro Ferrara, Alberto Zucchi, Giovanni Maifredi, and et al. 2022. "Statins Use in Patients with Cardiovascular Diseases and COVID-19 Outcomes: An Italian Population-Based Cohort Study" Journal of Clinical Medicine 11, no. 24: 7492. https://doi.org/10.3390/jcm11247492
APA StyleAntonazzo, I. C., Fornari, C., Rozza, D., Conti, S., Di Pasquale, R., Cortesi, P. A., Kaleci, S., Ferrara, P., Zucchi, A., Maifredi, G., Silenzi, A., Cesana, G., Mantovani, L. G., & Mazzaglia, G. (2022). Statins Use in Patients with Cardiovascular Diseases and COVID-19 Outcomes: An Italian Population-Based Cohort Study. Journal of Clinical Medicine, 11(24), 7492. https://doi.org/10.3390/jcm11247492