
Microwave Therapy for Cellulite: An Effective Non-Invasive Treatment

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients’ Population
2.2. Study Protocol
2.3. Objective and Patient’s Assessments
2.3.1. Cellulite Severity Scale (CSS) and Nürnberger–Müller Classification Scale
2.3.2. Photographic Evaluation
2.3.3. Buttocks’ and Posterior Thighs’ Circumference Measurements
2.3.4. Five-Point Likert Scale Questionnaire
2.3.5. Side Effects
2.4. Statistical Analysis
2.5. Post-Treatment Protocol
3. Results
3.1. Cellulite Severity Scale (CSS) and Nürnberger–Müller Classification Scale
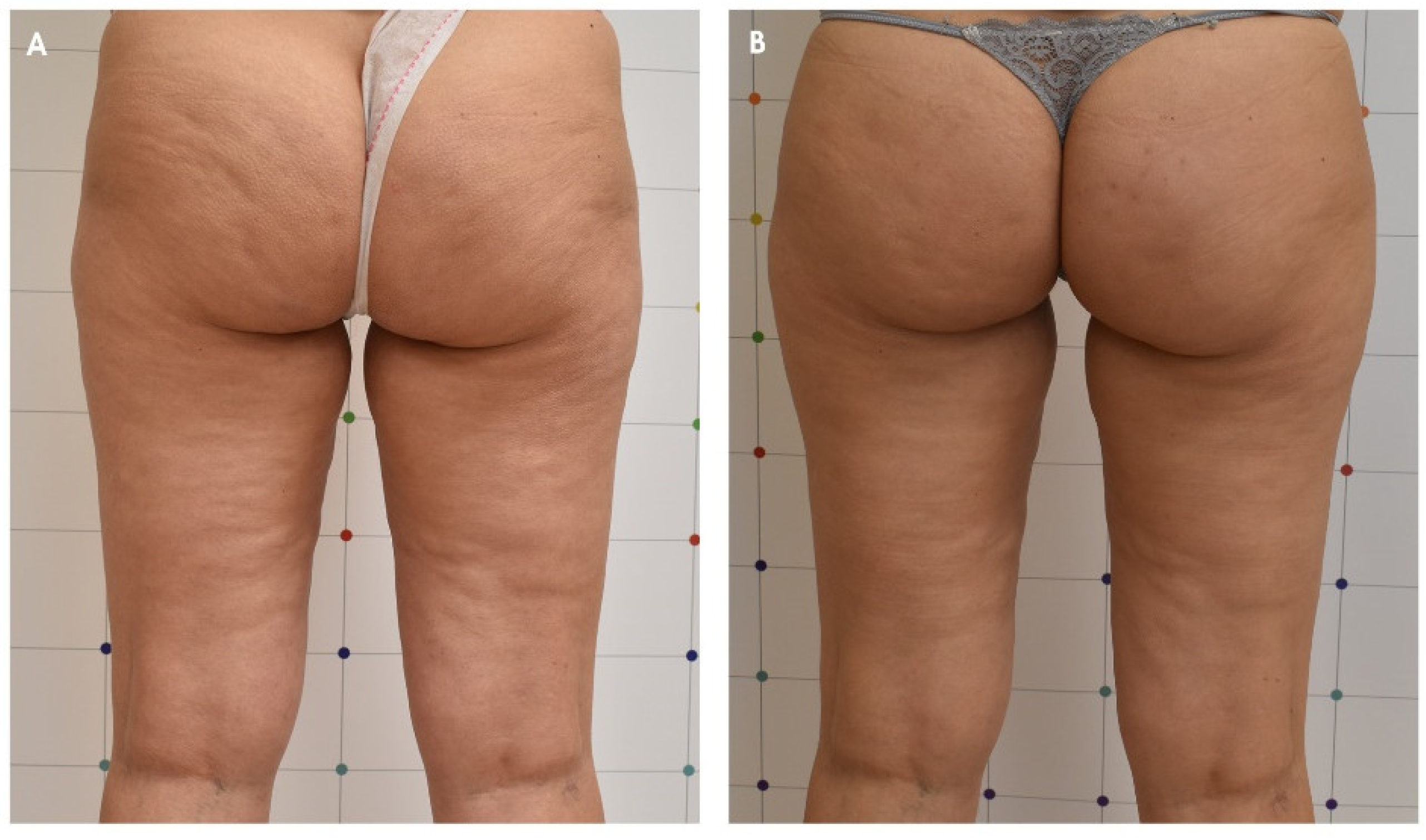
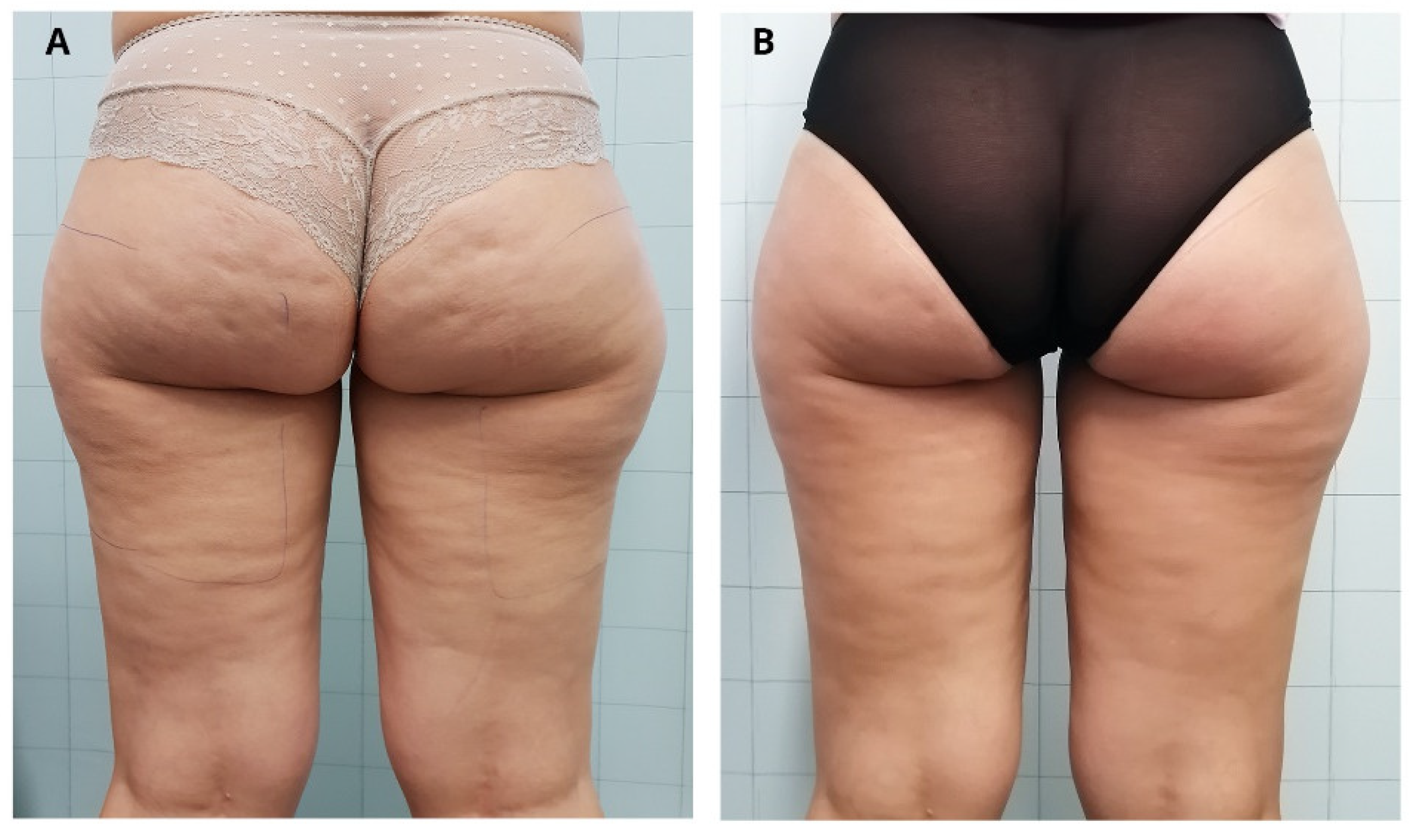
3.2. Photographic Evaluation
3.3. Patient Satisfaction Index with Five-Point Likert Scale Questionnaire
3.4. Buttocks and Posterior Thighs Circumference Measurements
3.5. Side Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rossi, A.; Vergnanini, A. Cellulite: A review. J. Eur. Acad. Dermatol. Venereol. 2000, 14, 251–262. [Google Scholar] [CrossRef]
- Draelos, Z.; Marenus, K. Cellulite. Etiology and purported treatment. Dermatol. Surg. 1997, 23, 1177–1781. [Google Scholar] [CrossRef] [PubMed]
- Segers, A.; Abulafia, J.; Kriner, J.; Cortondo, O. Celulitis. Estudo histopatológico e histoquímico de 100 casos. Med. Cut. ILA 1984, 12, 167–172. [Google Scholar]
- Scherwitz, C.; Braun-Flaco, O. So-called cellulite. J. Dermatol. Surg. Oncol. 1978, 4, 230–234. [Google Scholar] [CrossRef]
- Hexsel, D.M.; Abreu, M.; Rodrigues, T.C.; Soirefmann, M.; do Prado, D.; Gamboa, M.M.L. Side-By-Side Comparison of Areas with and without Cellulite Depressions Using Magnetic Resonance Imaging. Dermatol. Surg. 2009, 35, 1471–1477. [Google Scholar] [CrossRef]
- Sadick, N. Treatment for cellulite. Int. J. Womens Dermatol. 2019, 5, 68–72. [Google Scholar] [CrossRef]
- Hexsel, D.; Camozzato, F.O.; Silva, A.F.; Siega, C. Acoustic wave therapy for cellulite, body shaping and fat reduction. Clin. Trial J. Cosmet. Laser Ther. 2017, 19, 165–173. [Google Scholar] [CrossRef]
- Uebel, C.O.; Piccinini, P.S.; Martinelli, A.; Aguiar, D.F.; Ramos, R.F. Cellulite: A surgical treatment approach. Aesthetic Surg. J. 2018, 38, 1099–1114. [Google Scholar] [CrossRef]
- Rawlings, A.V. Cellulite and its treatment. Int. J. Cosmet. Sci. 2006, 28, 175–190. [Google Scholar] [CrossRef]
- Writers, A.M. Cellulite: No clear evidence that any type of treatment is effective. Drugs Ther. Perspect. 2015, 31, 437–440. [Google Scholar] [CrossRef]
- Modena, D.O.; da Silva, N.C.; Delinocente, T.C.P.; de Araújo, T.B.; de Carvalho, T.M.; Grecco, C.; Moreira, R.G.; Campos, G.; de Souza, J.R.; Guidi, R.M. Effectiveness of the Electromagnetic Shock Wave Therapy in the Treatment of Cellulite. Dermatol. Res. Pract. 2019, 2019, 8246815. [Google Scholar] [CrossRef]
- Foster, K.R.; Ziskin, M.C.; Balzano, Q. Thermal Response of Human Skin to Microwave Energy: A Critical Review. Health Phys. 2016, 111, 528–541. [Google Scholar] [CrossRef] [PubMed]
- Toker, S.; Boone-Kukoyi, Z.; Thompson, N.; Ajifa, H.; Clement, T.; Ozturk, B.; Aslan, K. Microwave Heating of Synthetic Skin Samples for Potential Treatment of Gout Using the Metal-Assisted and Microwave-Accelerated Decrystallization Technique. ACS Omega 2016, 1, 744–754. [Google Scholar] [CrossRef]
- Zerbinati, N.; D’Este, E.; Farina, A.; Cornaglia, A.I.; Jafferany, M.; Golubovic, M.; Binic, I.; Sigova, J.; Van Thuong, N.; Tirant, M.; et al. Remodeling of collagen constituting interlobular septa of subcutaneous adipose tissue following microwaves application. Dermatol. Ther. 2020, 33, e13362. [Google Scholar] [CrossRef]
- Bonan, P.; Marini, L.; Lotti, T. Microwaves in body sculpting: A prospective study. Dermatol. Ther. 2018, 32, e12782. [Google Scholar] [CrossRef] [PubMed]
- Di Pietro, A.; Ferri, S.; Bonan, P.; Verdelli, A.; Stevan, S.; Tartaglia, C.; Perosino, E. Effectiveness of microwaves in the treatment of cellulite: A preliminary study. J. Plastic Pathol. Dermatol. 2019, 15, 3. [Google Scholar]
- Bonan, P.; Verdelli, A. Combined microwaves and fractional microablative CO2 laser treatment for postpartum abdominal laxity. J. Cosmet. Dermatol. 2021, 20, 124–131. [Google Scholar] [CrossRef]
- Hexsel, D.; Dal’Forno, T.; Hexsel, C. A validated photonumeric cellulite severity scale. J. European Acad. Dermatol. Venereol. 2009, 23, 523–528. [Google Scholar] [CrossRef]
- Nürnberger, F.; Müller, G. So-Called Cellulite: An Invented Disease. J. Dermatol. Surg. Oncol. 1978, 4, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Belenky, I.; Margulis, A.; Elman, M.; Bar-Yosef, U.; Paun, S.D. Exploring Channeling Optimized Radiofrequency Energy: A Review of Radiofrequency History and Applications in Esthetic Fields. Adv. Ther. 2012, 29, 249–266. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, R.M.V.; Arend Barichello, P.; Lima Medeiros, M. Effect of Capacitive Radiofrequency on the Fibrosis of Patients with Cellulite. Dermatol. Res. Pract. 2013, 2013, 715829. [Google Scholar]
- Beasley, K.L.; Weiss, R.A. Radiofrequency in cosmetic dermatology. Dermatol. Clin. 2014, 32, 79–90. [Google Scholar] [CrossRef]
- Pahlavani, N.; Nattagh-Eshtivani, E.; Amanollahi, A.; Ranjbar, G.; Aghdaei, H.A.; Navashenaq, J.G.; Shabaninezhad, Z.; Sharahi, N.R.; Maleki, M.; Malekahmadi, M.; et al. Effects of microwave technology on the subcutaneous abdominal fat and anthropometric indices of overweight adults: A clinical trial. J. Cosmet. Dermatol. 2021. [Google Scholar] [CrossRef]
- Kennedy, J.; Verne, S.; Griffith, R.; Falto-Aizpurua, L.; Nouri, K. Non-invasive subcutaneous fat reduction: A review. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 1679–1688. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N° of patients | 26 |
| Mean age (years; mean ± SD) | 38.0 ± 13.1 |
| BMI (Kg/m2; mean ± SD) | 22.6 ± 2.3 |
| Smoking habits n (%) | 0 (0) |
| Contraceptive methods n (%) | 13 (50) |
| Pregnancy history n (%) | 16 (60) |
| CSS n (%) Mild Moderate Severe | 2 (7.7) 15 (57.7) 9 (34.6) |
| Cellulite Severity Scale | Classification |
|---|---|
| 1–5 | Mild |
| 6–10 | Moderate |
| 11–15 | Severe |
| CSS n (%) | Pre-Treatment (n = 26) | Post-Treatment (n = 26) |
|---|---|---|
| Mild | 2 (7.7) | 19 (73.1) |
| Moderate | 15 (57.7) | 7 (26.9) |
| Severe | 9 (34.6) | 0 (0) |
| CSS Key Morphologic Aspects of Cellulite | Pre-Treatment Posterior Thigh/Buttocks (n = 26) | Post-Treatment (3MFU) Posterior Thigh/ Buttocks (n = 26) | p Value |
|---|---|---|---|
| Average number of depressions | 2.2 ± 0.7 | 0.9 ± 0.3 | p ˂ 0.01 |
| Average depth of depressions | 2.1 ± 0.9 | 0.8 ± 0.5 | p ˂ 0.01 |
| Average morphological appearance of skin surface alterations | 2.1 ± 0.8 | 0.8 ± 0.4 | p ˂ 0.01 |
| Average grade of laxity, flaccidity or sagging skin | 2.1 ± 0.7 | 1.0 ± 0.6 | p ˂ 0.01 |
| Nürnberger–Müller classification | 2.2 ± 0.6 | 1.0 ± 0.6 | p ˂ 0.01 |
| CSS mean total score | 10.7 ± 3.1 | 4.5 ± 1.8 | p ˂ 0.01 |
| Cellulite Grades | Pre-Treatment (n = 26) | Post-Treatment (n = 26) |
|---|---|---|
| Grade 0, n (%) | 0 (0) | 6 (23.1) |
| Grade 1, n (%) | 2 (7.7) | 15 (57.7) |
| Grade 2, n (%) | 16 (61.5) | 5 (19.2) |
| Grade 3, n (%) | 8 (30.8) | 0 (0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bennardo, L.; Fusco, I.; Cuciti, C.; Sicilia, C.; Salsi, B.; Cannarozzo, G.; Hoffmann, K.; Nisticò, S.P. Microwave Therapy for Cellulite: An Effective Non-Invasive Treatment. J. Clin. Med. 2022, 11, 515. https://doi.org/10.3390/jcm11030515
Bennardo L, Fusco I, Cuciti C, Sicilia C, Salsi B, Cannarozzo G, Hoffmann K, Nisticò SP. Microwave Therapy for Cellulite: An Effective Non-Invasive Treatment. Journal of Clinical Medicine. 2022; 11(3):515. https://doi.org/10.3390/jcm11030515
Chicago/Turabian StyleBennardo, Luigi, Irene Fusco, Cristina Cuciti, Claudia Sicilia, Benedetta Salsi, Giovanni Cannarozzo, Klaus Hoffmann, and Steven Paul Nisticò. 2022. "Microwave Therapy for Cellulite: An Effective Non-Invasive Treatment" Journal of Clinical Medicine 11, no. 3: 515. https://doi.org/10.3390/jcm11030515
APA StyleBennardo, L., Fusco, I., Cuciti, C., Sicilia, C., Salsi, B., Cannarozzo, G., Hoffmann, K., & Nisticò, S. P. (2022). Microwave Therapy for Cellulite: An Effective Non-Invasive Treatment. Journal of Clinical Medicine, 11(3), 515. https://doi.org/10.3390/jcm11030515