
Effect of Transcutaneous Vagus Nerve Stimulation in Erosive Hand Osteoarthritis: Results from a Pilot Trial

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
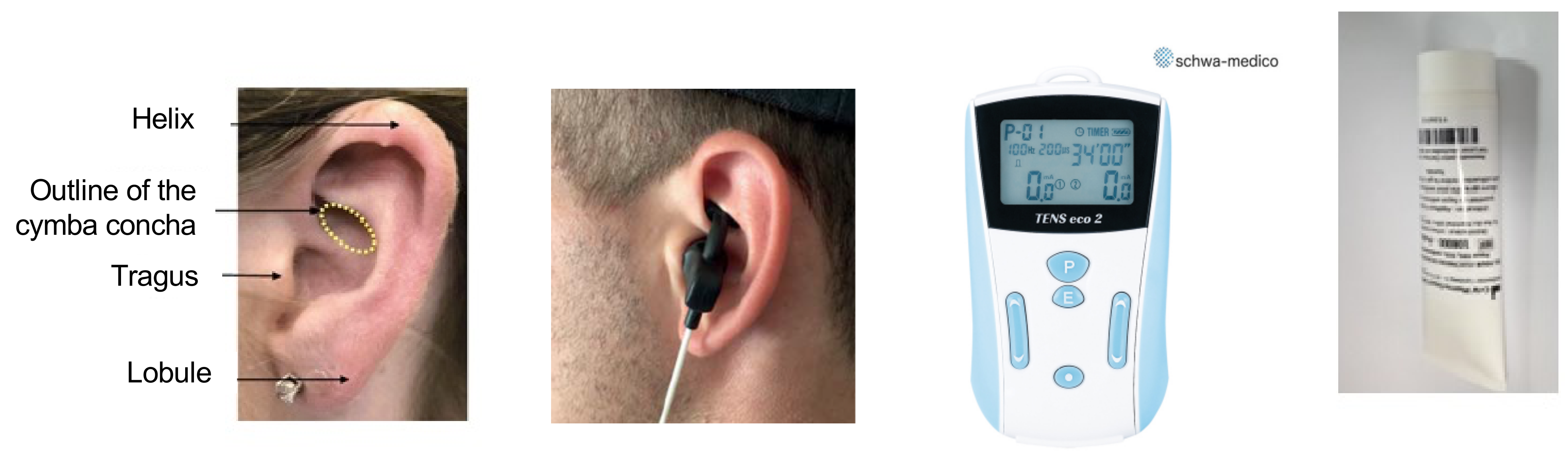
2.2. Procedures
2.3. Outcomes
2.4. Statistical Analysis
3. Results
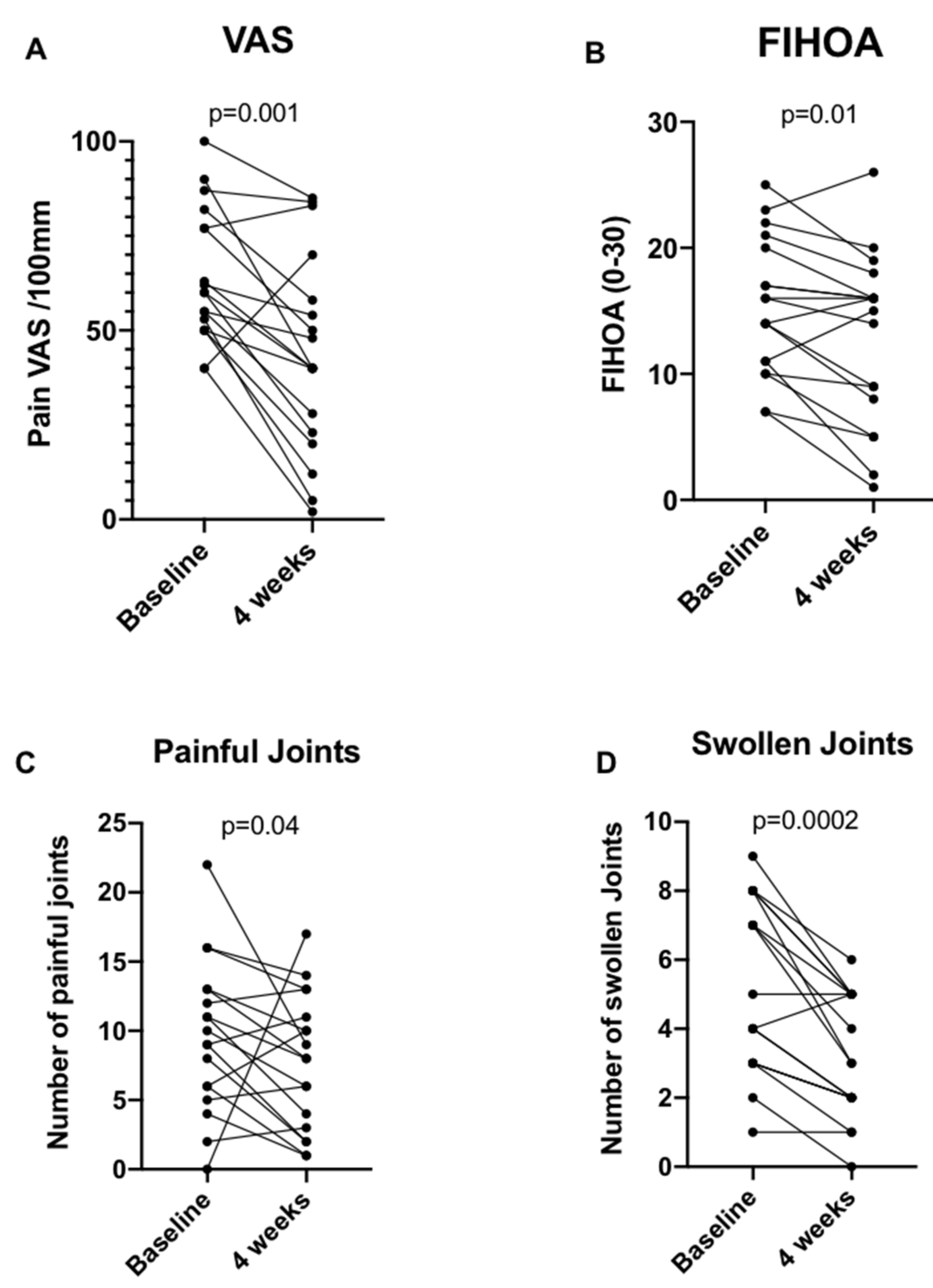
3.1. Efficacy
3.2. Safety
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hodkinson, B.; Maheu, E.; Michon, M.; Carrat, F.; Berenbaum, F. Assessment and Determinants of Aesthetic Discomfort in Hand Osteoarthritis. Ann. Rheum. Dis. 2012, 71, 45–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haugen, I.K.; Englund, M.; Aliabadi, P.; Niu, J.; Clancy, M.; Kvien, T.K.; Felson, D.T. Prevalence, Incidence and Progression of Hand Osteoarthritis in the General Population: The Framingham Osteoarthritis Study. Ann. Rheum. Dis. 2011, 70, 1581–1586. [Google Scholar] [CrossRef]
- Bijsterbosch, J.; Watt, I.; Meulenbelt, I.; Rosendaal, F.R.; Huizinga, T.W.J.; Kloppenburg, M. Clinical Burden of Erosive Hand Osteoarthritis and Its Relationship to Nodes. Ann. Rheum. Dis. 2010, 69, 1784–1788. [Google Scholar] [CrossRef] [Green Version]
- Kloppenburg, M.; Kroon, F.P.; Blanco, F.J.; Doherty, M.; Dziedzic, K.S.; Greibrokk, E.; Haugen, I.K.; Herrero-Beaumont, G.; Jonsson, H.; Kjeken, I.; et al. 2018 Update of the EULAR Recommendations for the Management of Hand Osteoarthritis. Ann. Rheum. Dis. 2019, 78, 16–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richette, P.; Latourte, A.; Sellam, J.; Wendling, D.; Piperno, M.; Goupille, P.; Pers, Y.-M.; Eymard, F.; Ottaviani, S.; Ornetti, P.; et al. Efficacy of Tocilizumab in Patients with Hand Osteoarthritis: Double Blind, Randomised, Placebo-Controlled, Multicentre Trial. Ann. Rheum. Dis. 2020, 80, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Kroon, F.P.B.; Kortekaas, M.C.; Boonen, A.; Böhringer, S.; Reijnierse, M.; Rosendaal, F.R.; Riyazi, N.; Starmans, M.; Turkstra, F.; van Zeben, J.; et al. Results of a 6-Week Treatment with 10 Mg Prednisolone in Patients with Hand Osteoarthritis (HOPE): A Double-Blind, Randomised, Placebo-Controlled Trial. Lancet 2019, 394, 1993–2001. [Google Scholar] [CrossRef]
- Notarnicola, A.; Iannone, F.; Maccagnano, G.; Lacarpia, N.; Bizzoca, D.; Moretti, B. Chondrocytes Treated with Different Shock Wave Devices. Muscles Ligaments Tendons J. 2017, 7, 152–156. [Google Scholar] [CrossRef]
- Rosas-Ballina, M.; Tracey, K.J. Cholinergic Control of Inflammation. J. Intern. Med. 2009, 265, 663–679. [Google Scholar] [CrossRef]
- Randich, A.; Gebhart, G.F. Vagal Afferent Modulation of Nociception. Brain Res. Brain Res. Rev. 1992, 17, 77–99. [Google Scholar] [CrossRef]
- Bassi, G.S.; Dias, D.P.M.; Franchin, M.; Talbot, J.; Reis, D.G.; Menezes, G.B.; Castania, J.A.; Garcia-Cairasco, N.; Resstel, L.B.M.; Salgado, H.C.; et al. Modulation of Experimental Arthritis by Vagal Sensory and Central Brain Stimulation. Brain Behav. Immun. 2017, 64, 330–343. [Google Scholar] [CrossRef]
- Ben-Menachem, E. Vagus-Nerve Stimulation for the Treatment of Epilepsy. Lancet Neurol. 2002, 1, 477–482. [Google Scholar] [CrossRef]
- O’Reardon, J.P.; Cristancho, P.; Peshek, A.D. Vagus Nerve Stimulation (VNS) and Treatment of Depression: To the Brainstem and Beyond. Psychiatry 2006, 3, 54–63. [Google Scholar] [PubMed]
- Koopman, F.A.; Chavan, S.S.; Miljko, S.; Grazio, S.; Sokolovic, S.; Schuurman, P.R.; Mehta, A.D.; Levine, Y.A.; Faltys, M.; Zitnik, R.; et al. Vagus Nerve Stimulation Inhibits Cytokine Production and Attenuates Disease Severity in Rheumatoid Arthritis. Proc. Natl. Acad. Sci. USA 2016, 113, 8284–8289. [Google Scholar] [CrossRef] [Green Version]
- Bonaz, B.; Sinniger, V.; Hoffmann, D.; Clarençon, D.; Mathieu, N.; Dantzer, C.; Vercueil, L.; Picq, C.; Trocmé, C.; Faure, P.; et al. Chronic Vagus Nerve Stimulation in Crohn’s Disease: A 6-Month Follow-up Pilot Study. Neurogastroenterol. Motil. 2016, 28, 948–953. [Google Scholar] [CrossRef] [PubMed]
- Lange, G.; Janal, M.N.; Maniker, A.; Fitzgibbons, J.; Fobler, M.; Cook, D.; Natelson, B.H. Safety and Efficacy of Vagus Nerve Stimulation in Fibromyalgia: A Phase I/II Proof of Concept Trial. Pain Med. 2011, 12, 1406–1413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mertens, A.; Raedt, R.; Gadeyne, S.; Carrette, E.; Boon, P.; Vonck, K. Recent Advances in Devices for Vagus Nerve Stimulation. Expert Rev. Med. Devices 2018, 15, 527–539. [Google Scholar] [CrossRef] [PubMed]
- Peuker, E.T.; Filler, T.J. The Nerve Supply of the Human Auricle. Clin. Anat. 2002, 15, 35–37. [Google Scholar] [CrossRef] [PubMed]
- Hanna, P.; Dacey, M.J.; Brennan, J.; Moss, A.; Robbins, S.; Achanta, S.; Biscola, N.P.; Swid, M.A.; Rajendran, P.S.; Mori, S.; et al. Innervation and Neuronal Control of the Mammalian Sinoatrial Node a Comprehensive Atlas. Circ. Res. 2021, 128, 1279–1296. [Google Scholar] [CrossRef]
- Yakunina, N.; Kim, S.S.; Nam, E.-C. Optimization of Transcutaneous Vagus Nerve Stimulation Using Functional MRI. Neuromodulation 2017, 20, 290–300. [Google Scholar] [CrossRef]
- Wang, Z.; Fang, J.; Liu, J.; Rong, P.; Jorgenson, K.; Park, J.; Lang, C.; Hong, Y.; Zhu, B.; Kong, J. Frequency-Dependent Functional Connectivity of the Nucleus Accumbens during Continuous Transcutaneous Vagus Nerve Stimulation in Major Depressive Disorder. J. Psychiatr. Res. 2018, 102, 123–131. [Google Scholar] [CrossRef]
- Frangos, E.; Ellrich, J.; Komisaruk, B.R. Non-Invasive Access to the Vagus Nerve Central Projections via Electrical Stimulation of the External Ear: FMRI Evidence in Humans. Brain Stimul. 2015, 8, 624–636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sclocco, R.; Garcia, R.G.; Kettner, N.W.; Isenburg, K.; Fisher, H.P.; Hubbard, C.S.; Ay, I.; Polimeni, J.R.; Goldstein, J.; Makris, N.; et al. The Influence of Respiration on Brainstem and Cardiovagal Response to Auricular Vagus Nerve Stimulation: A Multimodal Ultrahigh-Field (7T) FMRI Study. Brain Stimul. 2019, 12, 911–921. [Google Scholar] [CrossRef] [PubMed]
- Courties, A.; Sellam, J.; Berenbaum, F. Role of the Autonomic Nervous System in Osteoarthritis. Best Pract. Res. Clin. Rheumatol. 2017, 31, 661–675. [Google Scholar] [CrossRef]
- Altman, R.; Alarcón, G.; Appelrouth, D.; Bloch, D.; Borenstein, D.; Brandt, K.; Brown, C.; Cooke, T.D.; Daniel, W.; Gray, R. The American College of Rheumatology Criteria for the Classification and Reporting of Osteoarthritis of the Hand. Arthritis Rheum. 1990, 33, 1601–1610. [Google Scholar] [CrossRef]
- Verbruggen, G.; Veys, E.M. Numerical Scoring Systems for the Anatomic Evolution of Osteoarthritis of the Finger Joints. Arthritis Rheum. 1996, 39, 308–320. [Google Scholar] [CrossRef]
- Farmer, A.D.; Strzelczyk, A.; Finisguerra, A.; Gourine, A.V.; Gharabaghi, A.; Hasan, A.; Burger, A.M.; Jaramillo, A.M.; Mertens, A.; Majid, A.; et al. International Consensus Based Review and Recommendations for Minimum Reporting Standards in Research on Transcutaneous Vagus Nerve Stimulation (Version 2020). Front. Hum. Neurosci. 2020, 14, 568051. [Google Scholar] [CrossRef] [PubMed]
- Kloppenburg, M.; Maheu, E.; Kraus, V.B.; Cicuttini, F.; Doherty, M.; Dreiser, R.-L.; Henrotin, Y.; Jiang, G.-L.; Mandl, L.; Martel-Pelletier, J.; et al. OARSI Clinical Trials Recommendations: Design and Conduct of Clinical Trials for Hand Osteoarthritis. Osteoarthr. Cartil. 2015, 23, 772–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dreiser, R.L.; Maheu, E.; Guillou, G.B.; Caspard, H.; Grouin, J.M. Validation of an Algofunctional Index for Osteoarthritis of the Hand. Rev. Rhum. Engl. Ed. Fr. 1995, 62, 43S–53S. [Google Scholar]
- Dreiser, R.L.; Maheu, E.; Guillou, G.B. Sensitivity to Change of the Functional Index for Hand Osteoarthritis. Osteoarthr. Cartil. 2000, 8 (Suppl. A), S25–S28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tubach, F.; Ravaud, P.; Martin-Mola, E.; Awada, H.; Bellamy, N.; Bombardier, C.; Felson, D.T.; Hajjaj-Hassouni, N.; Hochberg, M.; Logeart, I.; et al. Minimum Clinically Important Improvement and Patient Acceptable Symptom State in Pain and Function in Rheumatoid Arthritis, Ankylosing Spondylitis, Chronic Back Pain, Hand Osteoarthritis, and Hip and Knee Osteoarthritis: Results from a Prospective Multinational Study. Arthritis Care Res. 2012, 64, 1699–1707. [Google Scholar] [CrossRef]
- Addorisio, M.E.; Imperato, G.H.; de Vos, A.F.; Forti, S.; Goldstein, R.S.; Pavlov, V.A.; van der Poll, T.; Yang, H.; Diamond, B.; Tracey, K.J.; et al. Investigational Treatment of Rheumatoid Arthritis with a Vibrotactile Device Applied to the External Ear. Bioelectron. Med. 2019, 5, 4. [Google Scholar] [CrossRef] [PubMed]
- Tarn, J.; Legg, S.; Mitchell, S.; Simon, B.; Ng, W.-F. The Effects of Noninvasive Vagus Nerve Stimulation on Fatigue and Immune Responses in Patients with Primary Sjögren’s Syndrome. Neuromodulation 2019, 22, 580–585. [Google Scholar] [CrossRef] [PubMed]
- Aranow, C.; Atish-Fregoso, Y.; Lesser, M.; Mackay, M.; Anderson, E.; Chavan, S.; Zanos, T.P.; Datta-Chaudhuri, T.; Bouton, C.; Tracey, K.J.; et al. Transcutaneous Auricular Vagus Nerve Stimulation Reduces Pain and Fatigue in Patients with Systemic Lupus Erythematosus: A Randomised, Double-Blind, Sham-Controlled Pilot Trial. Ann. Rheum. Dis. 2021, 80, 203–208. [Google Scholar] [CrossRef]
- Marsal, S.; Corominas, H.; De Agustin De Oro, J.; Perez Garcia, C.; Lopez Lasanta, M.; Borrell, H.; Reina, D.; Sanmarti, R. Non-Invasive Vagus Nerve Stimulation Improves Signs and Symptoms of Rheumatoid Arthritis: Results of a Pilot Study [Abstract]. Arthritis Rheumatol. 2020, 72 (Suppl. S10), 3997–3999. [Google Scholar]
- Genovese, M.C.; Gaylis, N.B.; Sikes, D.; Kivitz, A.; Horowitz, D.L.; Peterfy, C.; Glass, E.V.; Levine, Y.A.; Chernoff, D. Safety and Efficacy of Neurostimulation with a Miniaturised Vagus Nerve Stimulation Device in Patients with Multidrug-Refractory Rheumatoid Arthritis: A Two-Stage Multicentre, Randomised Pilot Study. Lancet Rheumatol. 2020, 2, e527–e538. [Google Scholar] [CrossRef]
- Drewes, A.M.; Brock, C.; Rasmussen, S.E.; Møller, H.J.; Brock, B.; Deleuran, B.W.; Farmer, A.D.; Pfeiffer-Jensen, M. Short-Term Transcutaneous Non-Invasive Vagus Nerve Stimulation May Reduce Disease Activity and pro-Inflammatory Cytokines in Rheumatoid Arthritis: Results of a Pilot Study. Scand. J. Rheumatol. 2021, 50, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Frangos, E.; Komisaruk, B.R. Access to Vagal Projections via Cutaneous Electrical Stimulation of the Neck: FMRI Evidence in Healthy Humans. Brain Stimul. 2017, 10, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Kraus, T.; Kiess, O.; Hösl, K.; Terekhin, P.; Kornhuber, J.; Forster, C. CNS BOLD FMRI Effects of Sham-Controlled Transcutaneous Electrical Nerve Stimulation in the Left Outer Auditory Canal—A Pilot Study. Brain Stimul. 2013, 6, 798–804. [Google Scholar] [CrossRef] [PubMed]
- Butt, M.F.; Albusoda, A.; Farmer, A.D.; Aziz, Q. The Anatomical Basis for Transcutaneous Auricular Vagus Nerve Stimulation. J. Anat. 2020, 236, 588–611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaptchuk, T.J.; Goldman, P.; Stone, D.A.; Stason, W.B. Do Medical Devices Have Enhanced Placebo Effects? J. Clin. Epidemiol. 2000, 53, 786–792. [Google Scholar] [CrossRef]
- Henrotin, Y.; Sanchez, C.; Bay-Jensen, A.C.; Mobasheri, A. Osteoarthritis Biomarkers Derived from Cartilage Extracellular Matrix: Current Status and Future Perspectives. Ann. Phys. Rehabil. Med. 2016, 59, 145–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishijima, M.; Kaneko, H.; Kaneko, K. The Evolving Role of Biomarkers for Osteoarthritis. Ther. Adv. Musculoskelet. Dis. 2014, 6, 144–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Baseline Characteristics n = 18 | |
|---|---|
| Age, years | 69 [66.7; 73.2] |
| Sex Men Women | 3 (17%) 15 (83%) |
| Body mass index, kg/m2 | 22.7 [20.7; 26.3] |
| Systolic blood pressure, mmHg | 129 [116; 139] |
| Diastolic blood pressure, mmHg | 77 [72.7; 79.2] |
| Cardiac frequency, beats per minute | 75 [67.2; 85.5] |
| Hand Pain VAS, /100 mm | 60 [50; 78.2] |
| Number of painful joints, /30 | 9.5 [5.7; 13] |
| Number of swollen joints, /30 | 4.5 [3; 8] |
| FIHOA, /30 | 15 [10.7; 20.2] |
| Severity | Adverse Event | Number of Patients | Related to Device (Yes/No/Uncertain) | Recovery at 4 Weeks |
|---|---|---|---|---|
| Minor | Local tingling or pain | 6 | Yes | Yes for 4/6 patients |
| Bilateral conjunctivitis | 1 | No | Yes | |
| Scotoma right eye | 1 | No | No | |
| Floating body left eye | 1 | No | Yes | |
| Auricular device desadaptation of the cymba concha | 1 | Yes | No | |
| Mild | Insomnia | 1 | Uncertain | No |
| Hand pain when trying to replace the earpiece | 1 | Yes | Yes | |
| Post-stimulation fatigue | 1 | Yes | Yes |
| Baseline n = 18 | 4 Weeks n = 18 | Median Change Value [IQR] (V1 − V0) | p-Value | |
|---|---|---|---|---|
| Systolic blood pressure, mmHg | 129 [116; 139] | 134 [124; 146.8] | −6 [−17; 5.25] | 0.08 |
| Diastolic blood pressure, mmHg | 77 [72.7; 79.2] | 81 [70; 88.25] | −0.5[−10; 3] | 0.09 |
| Cardiac frequency, Beats per minute | 75 [67.2; 85.5] | 79.5 [69; 87.2] | 0.5 [−13; 12.2] | 0.82 |
| Hand Pain VAS, /100 mm | 60 [50; 78.2] | 40 [22.2; 61] | −23.5 [−37.2; 7.7] | 0.001 |
| Number of painful joints, /30 | 9.5 [5.7; 13] | 8 [2.7; 11.5] | −3 [−5.2; 1] | 0.04 |
| Number of swollen joints, /30 | 4.5 [3; 8] | 3 [2; 5] | −2 [−3; −1] | 0.0002 |
| FIHOA, /30 | 15 [10.7; 20.2] | 15.5 [7.2; 16.5] | −2 [−5.2; −0.75] | 0.01 |
| Paracetamol consumption (g/week) | 0.32 [0.0; 5.5] | 0.0 [0.0; 2] | 0.0 [−1.25; 0] | 0.19 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Courties, A.; Deprouw, C.; Maheu, E.; Gibert, E.; Gottenberg, J.-E.; Champey, J.; Banneville, B.; Chesnel, C.; Amarenco, G.; Rousseau, A.; et al. Effect of Transcutaneous Vagus Nerve Stimulation in Erosive Hand Osteoarthritis: Results from a Pilot Trial. J. Clin. Med. 2022, 11, 1087. https://doi.org/10.3390/jcm11041087
Courties A, Deprouw C, Maheu E, Gibert E, Gottenberg J-E, Champey J, Banneville B, Chesnel C, Amarenco G, Rousseau A, et al. Effect of Transcutaneous Vagus Nerve Stimulation in Erosive Hand Osteoarthritis: Results from a Pilot Trial. Journal of Clinical Medicine. 2022; 11(4):1087. https://doi.org/10.3390/jcm11041087
Chicago/Turabian StyleCourties, Alice, Camille Deprouw, Emmanuel Maheu, Eric Gibert, Jacques-Eric Gottenberg, Julien Champey, Béatrice Banneville, Camille Chesnel, Gérard Amarenco, Alexandra Rousseau, and et al. 2022. "Effect of Transcutaneous Vagus Nerve Stimulation in Erosive Hand Osteoarthritis: Results from a Pilot Trial" Journal of Clinical Medicine 11, no. 4: 1087. https://doi.org/10.3390/jcm11041087
APA StyleCourties, A., Deprouw, C., Maheu, E., Gibert, E., Gottenberg, J. -E., Champey, J., Banneville, B., Chesnel, C., Amarenco, G., Rousseau, A., Berenbaum, F., & Sellam, J. (2022). Effect of Transcutaneous Vagus Nerve Stimulation in Erosive Hand Osteoarthritis: Results from a Pilot Trial. Journal of Clinical Medicine, 11(4), 1087. https://doi.org/10.3390/jcm11041087