
Chest X-ray Does Not Predict the Risk of Endotracheal Intubation and Escalation of Treatment in COVID-19 Patients Requiring Noninvasive Respiratory Support

 , , , , , , ,
, , , , , , ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Measurements
2.2. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guan, W.; Ni, Z.; Hu, Y.; Liang, W.; Ou, C.; He, J.; Liu, L.; Shan, H.; Lei, C.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239. [Google Scholar] [CrossRef] [PubMed]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; The Northwell COVID-19 Research Consortium; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; et al. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized with COVID-19 in the New York City Area. JAMA 2020, 323, 2052. [Google Scholar] [CrossRef] [PubMed]
- Vahidy, F.S.; Drews, A.L.; Masud, F.N.; Schwartz, R.L.; Askary, B.B.; Boom, M.L.; Phillips, R.A. Characteristics and Outcomes of COVID-19 Patients during Initial Peak and Resurgence in the Houston Metropolitan Area. JAMA 2020, 324, 998. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline Characteristics and Outcomes of 1591 Patients Infected with SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaschetto, R.; Barone-Adesi, F.; Racca, F.; Pissaia, C.; Maestrone, C.; Colombo, D.; Olivieri, C.; De Vita, N.; Santangelo, E.; Scotti, L.; et al. Outcomes of COVID-19 Patients Treated with Continuous Positive Airway Pressure Outside the Intensive Care Unit. ERJ Open Res. 2021, 7, 00541-02020. [Google Scholar] [CrossRef] [PubMed]
- Boscolo, A.; Pasin, L.; Sella, N.; Pretto, C.; Tocco, M.; Tamburini, E.; Rosi, P.; Polati, E.; Donadello, K.; Gottin, L.; et al. Outcomes of COVID-19 Patients Intubated after Failure of Non-Invasive Ventilation: A Multicenter Observational Study. Sci. Rep. 2021, 11, 17730. [Google Scholar] [CrossRef] [PubMed]
- Brochard, L.; Slutsky, A.; Pesenti, A. Mechanical Ventilation to Minimize Progression of Lung Injury in Acute Respiratory Failure. Am. J. Respir. Crit. Care Med. 2017, 195, 438–442. [Google Scholar] [CrossRef] [PubMed]
- Reeves, R.A.; Pomeranz, C.; Gomella, A.A.; Gulati, A.; Metra, B.; Hage, A.N.; Lange, S.; Parekh, M.; Donuru, A.; Lakhani, P.; et al. Performance of a Severity Score on Admission Chest Radiography in Predicting Clinical Outcomes in Hospitalized Patients with Coronavirus Disease (COVID-19). Am. J. Roentgenol. 2021, 217, 623–632. [Google Scholar] [CrossRef] [PubMed]
- Sargent, W.; Ali, S.; Kukran, S.; Harvie, M.; Soin, S. The Prognostic Value of Chest X-Ray in Patients with COVID-19 on Admission and When Starting CPAP. Clin. Med. 2021, 21, e14–e19. [Google Scholar] [CrossRef]
- Giraudo, C.; Cavaliere, A.; Fichera, G.; Weber, M.; Motta, R.; Pelloso, M.; Tosato, F.; Lupi, A.; Calabrese, F.; Carretta, G.; et al. Validation of a Composed COVID-19 Chest Radiography Score: The Care Project. ERJ Open Res. 2020, 6, 00359-02020. [Google Scholar] [CrossRef] [PubMed]
- Balbi, M.; Conti, C.; Imeri, G.; Caroli, A.; Surace, A.; Corsi, A.; Mercanzin, E.; Arrigoni, A.; Villa, G.; Di Marco, F.; et al. Post-Discharge Chest CT Findings and Pulmonary Function Tests in Severe COVID-19 Patients. Eur. J. Radiol. 2021, 138, 109676. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.; Chen, C.; Hu, Y.; Lv, W.; Ai, T.; Xia, L. Chest CT Imaging Features and Severity Scores as Biomarkers for Prognostic Prediction in Patients with COVID-19. Ann. Transl. Med. 2020, 8, 1449. [Google Scholar] [CrossRef] [PubMed]
- Francone, M.; Iafrate, F.; Masci, G.M.; Coco, S.; Cilia, F.; Manganaro, L.; Panebianco, V.; Andreoli, C.; Colaiacomo, M.C.; Zingaropoli, M.A.; et al. Chest CT Score in COVID-19 Patients: Correlation with Disease Severity and Short-Term Prognosis. Eur. Radiol. 2020, 30, 6808–6817. [Google Scholar] [CrossRef] [PubMed]
- Pasin, L.; Sella, N.; Correale, C.; Boscolo, A.; Rosi, P.; Saia, M.; Mantoan, D.; Navalesi, P. Regional COVID-19 Network for Coordination of SARS-CoV-2 Outbreak in Veneto, Italy. J. Cardiothorac. Vasc. Anesth. 2020, 34, 2341–2345. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Johnston, R.; Jones, K.; Manley, D. Confounding and Collinearity in Regression Analysis: A Cautionary Tale and an Alternative Procedure, Illustrated by Studies of British Voting Behaviour. Qual. Quant. 2018, 52, 1957–1976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cammarota, G.; Vaschetto, R.; Azzolina, D.; De Vita, N.; Olivieri, C.; Ronco, C.; Longhini, F.; Bruni, A.; Colombo, D.; Pissaia, C.; et al. Early Extubation with Immediate Non-Invasive Ventilation versus Standard Weaning in Intubated Patients for Coronavirus Disease 2019: A Retrospective Multicenter Study. Sci. Rep. 2021, 11, 13418. [Google Scholar] [CrossRef] [PubMed]
- Scala, R.; Pisani, L. Noninvasive Ventilation in Acute Respiratory Failure: Which Recipe for Success? Eur. Respir. Rev. 2018, 27, 180029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akoumianaki, E.; Ischaki, E.; Karagiannis, K.; Sigala, I.; Zakyn-thinos, S. The Role of Noninvasive Respiratory Management in Patients with Severe COVID-19 Pneumonia. JPM 2021, 11, 884. [Google Scholar] [CrossRef] [PubMed]
- Knight, S.R.; Ho, A.; Pius, R.; Buchan, I.; Carson, G.; Drake, T.M.; Dunning, J.; Fairfield, C.J.; Gamble, C.; Green, C.A.; et al. Risk Stratification of Patients Admitted to Hospital with Covid-19 Using the ISARIC WHO Clinical Characterisation Protocol: Development and Validation of the 4C Mortality Score. BMJ 2020, 370, m3339. [Google Scholar] [CrossRef] [PubMed]
- Liang, W.; Liang, H.; Ou, L.; Chen, B.; Chen, A.; Li, C.; Li, Y.; Guan, W.; Sang, L.; Lu, J.; et al. Development and Validation of a Clinical Risk Score to Predict the Occurrence of Critical Illness in Hospitalized Patients with COVID-19. JAMA Int. Med. 2020, 180, 1081. [Google Scholar] [CrossRef] [PubMed]
- King, J.T.; Yoon, J.S.; Rentsch, C.T.; Tate, J.P.; Park, L.S.; Kidwai-Khan, F.; Skanderson, M.; Hauser, R.G.; Jacobson, D.A.; Erdos, J.; et al. Development and Validation of a 30-Day Mortality Index Based on Pre-Existing Medical Administrative Data from 13,323 COVID-19 Patients: The Veterans Health Administration COVID-19 (VACO) Index. PLoS ONE 2020, 15, e0241825. [Google Scholar] [CrossRef] [PubMed]
- Ji, D.; Zhang, D.; Xu, J.; Chen, Z.; Yang, T.; Zhao, P.; Chen, G.; Cheng, G.; Wang, Y.; Bi, J.; et al. Prediction for Progression Risk in Patients with COVID-19 Pneumonia: The CALL Score. Clin. Infect. Dis. 2020, 71, 1393–1399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ji, L.; Cao, C.; Gao, Y.; Zhang, W.; Xie, Y.; Duan, Y.; Kong, S.; You, M.; Ma, R.; Jiang, L.; et al. Prognostic Value of Bedside Lung Ultrasound Score in Patients with COVID-19. Crit. Care 2020, 24, 700. [Google Scholar] [CrossRef] [PubMed]
- Bonadia, N.; Carnicelli, A.; Piano, A.; Buonsenso, D.; Gilardi, E.; Kadhim, C.; Torelli, E.; Petrucci, M.; Di Maurizio, L.; Biasucci, D.G.; et al. Lung Ultrasound Findings Are Associated with Mortality and Need for Intensive Care Admission in COVID-19 Patients Evaluated in the Emergency Department. Ultrasound Med. Biol. 2020, 46, 2927–2937. [Google Scholar] [CrossRef] [PubMed]
- Lichter, Y.; Topilsky, Y.; Taieb, P.; Banai, A.; Hochstadt, A.; Merdler, I.; Gal Oz, A.; Vine, J.; Goren, O.; Cohen, B.; et al. Lung Ultrasound Predicts Clinical Course and Outcomes in COVID-19 Patients. Intensive Care Med. 2020, 46, 1873–1883. [Google Scholar] [CrossRef] [PubMed]
- Persona, P.; Valeri, I.; Zarantonello, F.; Forin, E.; Sella, N.; Andreatta, G.; Correale, C.; Serra, E.; Boscolo, A.; Volpicelli, G.; et al. Patients in Intensive Care Unit for COVID-19 Pneumonia: The Lung Ultrasound Patterns at Admission and Discharge. An Observational Pilot Study. Ultrasound J. 2021, 13, 10. [Google Scholar] [CrossRef] [PubMed]
- Bellani, G.; Grasselli, G.; Cecconi, M.; Antolini, L.; Borelli, M.; De Giacomi, F.; Bosio, G.; Latronico, N.; Filippini, M.; Gemma, M.; et al. Noninvasive Ventilatory Support of Patients with COVID-19 Outside the Intensive Care Units (WARd-COVID). Ann. ATS 2021, 18, 1020–1026. [Google Scholar] [CrossRef] [PubMed]
- Xiao, N.; Cooper, J.G.; Godbe, J.M.; Bechel, M.A.; Scott, M.B.; Nguyen, E.; McCarthy, D.M.; Abboud, S.; Allen, B.D.; Parekh, N.D. Chest Radiograph at Admission Predicts Early Intubation among Inpatient COVID-19 Patients. Eur. Radiol. 2021, 31, 2825–2832. [Google Scholar] [CrossRef] [PubMed]
- Fusco, R.; Grassi, R.; Granata, V.; Setola, S.V.; Grassi, F.; Cozzi, D.; Pecori, B.; Izzo, F.; Petrillo, A. Artificial Intelligence and COVID-19 Using Chest CT Scan and Chest X-Ray Images: Machine Learning and Deep Learning Approaches for Diagnosis and Treatment. JPM 2021, 11, 993. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; Greco, M.; Zanella, A.; Albano, G.; Antonelli, M.; Bellani, G.; Bonanomi, E.; Cabrini, L.; Carlesso, E.; Castelli, G.; et al. Risk Factors Associated with Mortality Among Patients with COVID-19 in Intensive Care Units in Lombardy, Italy. JAMA Int. Med. 2020, 180, 1345. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Use of Chest Imaging in COVID-19: A Rapid Advice Guide, 11 June 2020; World Health Organization: Geneva, Switzerland, 2020; Available online: https://apps.who.int/iris/handle/10665/332336 (accessed on 22 November 2021).
- Fortarezza, F.; Boscolo, A.; Pezzuto, F.; Lunardi, F.; Jesús Acosta, M.; Giraudo, C.; Del Vecchio, C.; Sella, N.; Tiberio, I.; Godi, I.; et al. Proven COVID-19-Associated Pulmonary Aspergillosis in Patients with Severe Respiratory Failure. Mycoses 2021, 64, 1223–1229. [Google Scholar] [CrossRef] [PubMed]
- Calabrese, F.; Pezzuto, F.; Fortarezza, F.; Boscolo, A.; Lunardi, F.; Giraudo, C.; Cattelan, A.; Del Vecchio, C.; Lorenzoni, G.; Vedovelli, L.; et al. Machine Learning-based Analysis of Alveolar and Vascular Injury in SARS-CoV-2 Acute Respiratory Failure. J. Pathol. 2021, 254, 173–184. [Google Scholar] [CrossRef] [PubMed]
- Cocconcelli, E.; Biondini, D.; Giraudo, C.; Lococo, S.; Bernardinello, N.; Fichera, G.; Barbiero, G.; Castelli, G.; Cavinato, S.; Ferrari, A.; et al. Clinical Features and Chest Imaging as Predictors of Intensity of Care in Patients with COVID-19. J Clin. Med. 2020, 9, 2990. [Google Scholar] [CrossRef] [PubMed]
- Brakohiapa, E.K.K.; Sarkodie, B.; Botwe, B.O.; Dzefi-Tettey, K.; Anim, D.A.; Edzie, E.K.; Goleku, P.N.; Jimah, B.B.; Amankwa, A.T. Comparing radiological presentations of first and second strains of COVID-19 infections in a low-resource country. Heliyon 2021, 7, e07818. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
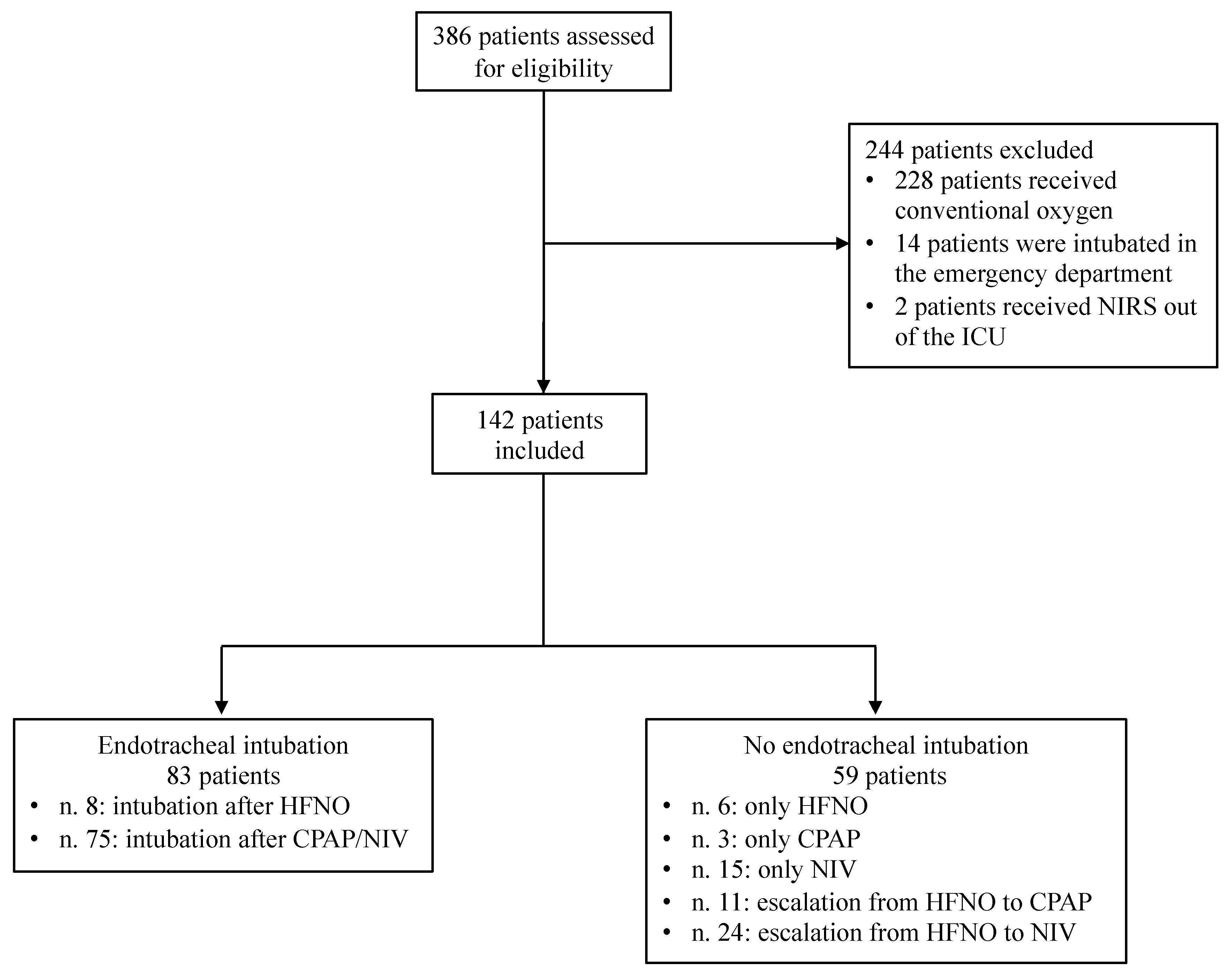
| Variable | All Patients (n = 142) | No Intubation (n = 59) | Intubation (n = 83) | p-Value |
|---|---|---|---|---|
| Age (years) | 69 (58–75) | 70 (60–79) | 69 (58–73) | 0.09 |
| Weight (kg) | 78 (69–97) | 76 (68–96) | 79 (72–102) | 0.43 |
| Body mass index (kg/m2) | 26 (22–31) | 25 (22–32) | 27 (24–30) | 0.66 |
| Female gender (n [%]) | 44 (31) | 19 (32) | 25 (30) | 0.86 |
| Hypertension (n [%]) | 81 (57) | 35 (59) | 46 (55) | 0.86 |
| Obesity (n [%]) | 45 (32) | 14 (24) | 31 (37) | 0.10 |
| Diabetes (n [%]) | 38 (27) | 19 (32) | 19 (23) | 0.26 |
| Days since symptom onset | 6 (4–9) | 6 (3–8) | 7 (4–10) | 0.04 |
| SOFA score | 3 (2–4) | 2 (2–3) | 3 (2–4) | <0.01 |
| Charlson comorbidity index | 3 (2–5) | 3 (2–5) | 3 (2–4) | 0.10 |
| C-reactive protein (mg/L) | 97 (58–160) | 90 (41–123) | 113 (62–180) | 0.04 |
| Procalcitonin (μg/L) | 0.18 (0.06–0.48) | 0.13 (0.06–0.48) | 0.19 (0.07–0.47) | 0.56 |
| D-dimer (μg/L) | 323 (171–670) | 294 (150–523) | 335 (200–801) | 0.20 |
| Leukocyte count (× 109 cells/L) | 7.58 (4.84–10.57) | 6.84 (3.32–9.60) | 7.81 (5.98–11.26) | 0.03 |
| Lymphocyte count (× 109 cells/L) | 0.80 (0.55–1.11) | 0.78 (0.48–1.22) | 0.80 (0.59–1.10) | 0.75 |
| IL-6 (pg/mL) | 55 (31–148) | 51 (26–99) | 67 (39–165) | 0.03 |
| PaO2/FiO2 (mmHg) | 118 (90–160) | 148 (105–177) | 104 (78–134) | <0.01 |
| PaCO2 (mmHg) | 35 (31–38) | 35 (30–38) | 35 (31–38) | 0.75 |
| Variable | All Patients (n = 142) | No Intubation (n = 59) | Intubation (n = 83) | p-Value |
|---|---|---|---|---|
| Pronation (n [%]) | 85 (60) | 14 (24) | 71 (86) | <0.01 |
| Duration of invasive mechanical ventilation (days) | n.a. | n.a. | 8 (6–13) | n.a. |
| Hospital length of stay (days) | 22 (14–32) | 16 (12–22) | 29 (21–41) | <0.01 |
| Hospital mortality (n [%]) | 20 (14) | 1 (2) | 19 (23) | <0.01 |
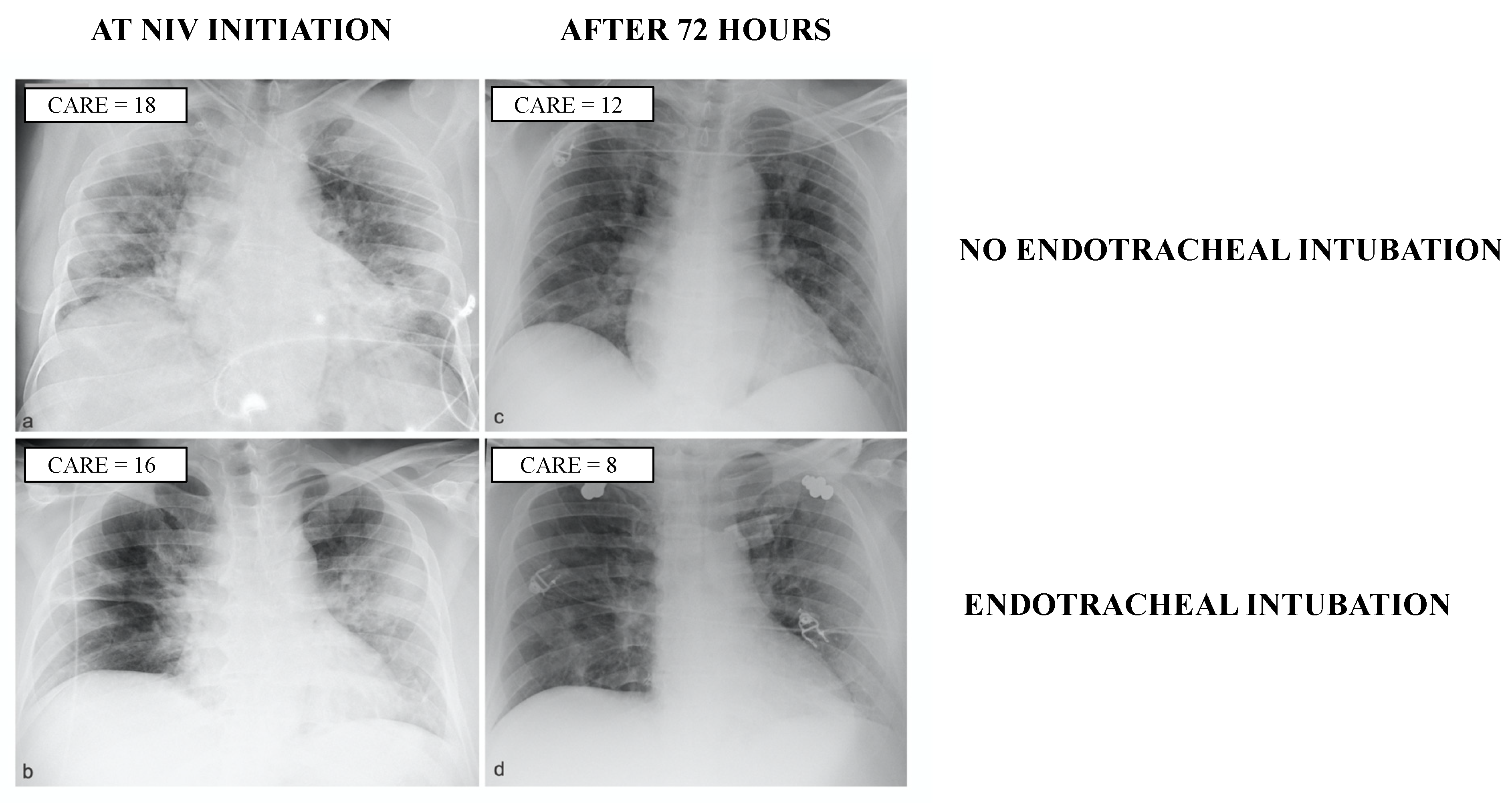
| CARE Score | All Patients (n = 142) | No Intubation (n = 59) | Intubation (n = 83) | p-Value |
|---|---|---|---|---|
| First CARE score | 9 (6–14) | 10 (6–13) | 9 (5–15) | 0.98 |
| Second CARE score | 8 (4–14) * | 10 (5–17) | 8 (3–12) * | 0.04 |
| Delta CARE score | −1 (−5–3) | −1 (−4–6) | −2 (−6–2) | 0.01 |
| Variable | Univariable | Multivariable | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| First CARE score | 1.01 (0.96–1.06) | 0.69 | ||
| Age | 0.97 (0.94–1.00) | 0.07 | ||
| Female gender | 0.91 (0.44–1.86) | 0.79 | ||
| Days since symptom onset | 1.09 (1.00–1.20) | 0.06 | ||
| SOFA score | 1.55 (1.15–2.10) | <0.01 | 1.40 (0.99–1.99) | 0.06 |
| Charlson comorbidity index | 0.86 (0.75–1.00) | 0.04 | 0.79 (0.65–0.95) | 0.01 |
| C-reactive protein | 1.01 (1.00–1.01) | 0.04 | 1.01 (1.00–1.01) | 0.03 |
| Procalcitonin | 1.06 (0.92–1.22) | 0.40 | ||
| D-dimer | 1.00 (1.00–1.00) | 0.66 | ||
| Leukocyte count | 1.06 (0.99–1.14) | 0.88 | ||
| Lymphocyte count | 0.81 (0.60–1.09) | 0.17 | ||
| IL-6 | 1.00 (1.00–1.01) | 0.11 | ||
| PaO2/FiO2 | 0.99 (0.98–1.00) | <0.01 | 0.99 (0.98–1.00) | 0.01 |
| PaCO2 | 1.03 (0.98–1.09) | 0.22 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pettenuzzo, T.; Giraudo, C.; Fichera, G.; Della Paolera, M.; Tocco, M.; Weber, M.; Gorgi, D.; Carlucci, S.; Lionello, F.; Lococo, S.; et al. Chest X-ray Does Not Predict the Risk of Endotracheal Intubation and Escalation of Treatment in COVID-19 Patients Requiring Noninvasive Respiratory Support. J. Clin. Med. 2022, 11, 1636. https://doi.org/10.3390/jcm11061636
Pettenuzzo T, Giraudo C, Fichera G, Della Paolera M, Tocco M, Weber M, Gorgi D, Carlucci S, Lionello F, Lococo S, et al. Chest X-ray Does Not Predict the Risk of Endotracheal Intubation and Escalation of Treatment in COVID-19 Patients Requiring Noninvasive Respiratory Support. Journal of Clinical Medicine. 2022; 11(6):1636. https://doi.org/10.3390/jcm11061636
Chicago/Turabian StylePettenuzzo, Tommaso, Chiara Giraudo, Giulia Fichera, Michele Della Paolera, Martina Tocco, Michael Weber, Davide Gorgi, Silvia Carlucci, Federico Lionello, Sara Lococo, and et al. 2022. "Chest X-ray Does Not Predict the Risk of Endotracheal Intubation and Escalation of Treatment in COVID-19 Patients Requiring Noninvasive Respiratory Support" Journal of Clinical Medicine 11, no. 6: 1636. https://doi.org/10.3390/jcm11061636
APA StylePettenuzzo, T., Giraudo, C., Fichera, G., Della Paolera, M., Tocco, M., Weber, M., Gorgi, D., Carlucci, S., Lionello, F., Lococo, S., Boscolo, A., De Cassai, A., Pasin, L., Rossato, M., Vianello, A., Vettor, R., Sella, N., & Navalesi, P. (2022). Chest X-ray Does Not Predict the Risk of Endotracheal Intubation and Escalation of Treatment in COVID-19 Patients Requiring Noninvasive Respiratory Support. Journal of Clinical Medicine, 11(6), 1636. https://doi.org/10.3390/jcm11061636