
COVID-19 Patients Presenting with Post-Intubation Upper Airway Complications: A Parallel Epidemic?

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Kowalski, L.P.; Sanabria, A.; Ridge, J.A.; Ng, W.T.; Bree, R.; Rinaldo, A.; Takes, R.P.; Mäkitie, A.A.; Carvalho, A.L.; Bradford, C.R.; et al. COVID-19 pandemic: Effects and evidence-based recommendations for otolaryngology and head and neck surgery practice. Head Neck 2020, 42, 1259–1267. [Google Scholar] [CrossRef] [Green Version]
- Sommer, D.D.; Engels, P.T.; Weitzel, E.; Khalili, S.; Corsten, M.; Tewfik, M.A.; Fung, K.; Cote, D.; Gupta, M.; Sne, N.; et al. Recommendations from the CSO-HNS taskforce on performance of tracheotomy during the COVID-19 pandemic. J. Otolaryngol. Head Neck Surg. 2020, 49, 23. [Google Scholar] [CrossRef] [PubMed]
- Pearson, F.; Andrews, M. Detection and Management of Tracheal Stenosis Following Cuffed Tube Tracheostomy. Ann. Thorac. Surg. 1971, 12, 359–374. [Google Scholar] [CrossRef]
- Stauffer, J.L.; Olson, D.E.; Petty, T.L. Complications and consequences of endotracheal intubation and tracheostomy. A prospective study of 150 critically ill adult patients. Am. J. Med. 1981, 70, 65–76. [Google Scholar] [CrossRef]
- Kastanos, N.; Estopá Miró, R.; Marín Perez, A.; Xaubet Mir, A.; Agustí-Vidal, A. Laryngotracheal injury due to endotracheal intubation: Incidence, evolution and predisposing factors. A prospective long term study. Crit. Care Med. 1983, 11, 362–367. [Google Scholar] [CrossRef]
- Grillo, H.C.; Donahue, D.M.; Mathisen, D.J.; Wain, J.C.; Wright, C.D. Postintubation tracheal stenosis. Treatment and results. J. Thorac. Cardiovasc. Surg. 1995, 109, 486–493. [Google Scholar] [CrossRef] [Green Version]
- Brichet, A.; Verkindre, C.; Dupont, J.; Carlier, M.; Darras, J.; Wurtz, A.; Ramon, P.; Marquette, C.H. Multidisciplinary approach to management of postintubation tracheal stenoses. Eur. Respir. J. 1999, 13, 888–893. [Google Scholar] [CrossRef]
- Siempos, I.I.; Ntaidou, T.K.; Filippidis, F.T.; Choi, A.M.K. Effect of early versus late or no tracheostomy on mortality and pneumonia of critically ill patients receiving mechanical ventilation: A systematic review and meta-analysis. Lancet Respir. Med. 2015, 3, 150–158. [Google Scholar] [CrossRef]
- Liu, J.; Zhang, X.; Gong, W.; Li, S.; Wang, F.; Fu, S.; Zhang, M.; Hang, Y. Correlations between controlled endotracheal tube cuff pressure and postprocedural complications: A multicenter study. Anesth. Analg. 2010, 111, 1133–1137. [Google Scholar] [CrossRef]
- Fiz, I.; Monnier, P.; Koelmel, J.C.; Di Dio, D.; Fiz, F.; Missale, F.; Piazza, C.; Peretti, G.; Sittel, C. Multicentric study applying the european laryngological society classification of benign laryngotracheal stenosis in adults treated by tracheal or cricotracheal resection and anastomosis. Laryngoscope 2020, 130, 1640–1645. [Google Scholar] [CrossRef]
- Nikolovski, N.; Kopacheva-Barsova, G.; Pejkovska, A. Laryngotracheal Stenosis: A Retrospective Analysis of Their Aetiology, Diagnose and Treatment. Open Access Maced. J. Med. Sci. 2019, 7, 1649–1656. [Google Scholar] [CrossRef] [Green Version]
- Piazza, C.; Filauro, M.; Dikkers, F.G.; Nouraei, S.A.; Sandu, K.; Sittel, C.; Amin, M.R.; Campos, G.; Eckel, H.E.; Peretti, G. Long term intubation and high rate of tracheostomy in COVID-19 patients might determine an unprecedented increase of airway stenoses: A call to action from the European Laryngological Society. Eur. Arch. Oto-Rhino-Laryngol. 2021, 278, 1–7. [Google Scholar] [CrossRef] [PubMed]
- To, K.K.; Tsang, O.T.; Leung, W.S.; Tam, A.R.; Wu, T.C.; Lung, D.C.; Yip, C.C.; Cai, J.P.; Chan, J.M.; Chik, T.S.; et al. Temporal profiles of viral load in posterior oropharyngeal saliva samples and serum antibody responses during infection by SARS-CoV-2: An observational cohort study. Lancet Infect. Dis. 2020, 20, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Galluccio, G.; Lucantoni, G.; Battistoni, P.; Paone, G.; Batzella, S.; Lucifora, V.; Iacono, R.D. Interventional endoscopy in the management of benign tracheal stenoses: Definitive treatment at long-term follow-up. Eur. J. Cardio-Thorac. Surg. 2009, 35, 429–434. [Google Scholar] [CrossRef]
- Rosell, A.; Stratakos, G. Therapeutic bronchoscopy for central airway diseases. Eur. Respir. Rev. 2020, 29, 190178. [Google Scholar] [CrossRef]
- Emam, W.; Mostafa, Y.; Madkour, A.; Wagih, K.; Ezzelregal, H.; Anagnostopoulos, N.; Stratakos, G. Bronchoscopic management as an alternative treatment in non-operable benign tracheal stenosis. Int. J. Clin. Pract. 2021, 75, e14058. [Google Scholar] [CrossRef] [PubMed]
- Nouraei, S.A.R.; Ma, E.; Patel, A.; Howard, D.; Sandhu, G. Estimating the population incidence of adult post-intubation laryngotracheal stenosis. Clin. Otolaryngol. 2007, 32, 411–412. [Google Scholar] [CrossRef]
- Shinn, J.R.; Kimura, K.S.; Campbell, B.R.; Lowery, A.S.; Wootten, C.T.; Garrett, C.G.; Francis, D.O.; Hillel, A.T.; Du, L.; Casey, J.D.; et al. Incidence and outcomes of acute laryngeal injury after prolonged mechanical ventilation. Crit. Care Med. 2019, 47, 1699–1706. [Google Scholar] [CrossRef]
- Touman, A.; Stratakos, G. Long-Term Complications of Tracheal Intubation. In Tracheal Intubation [Internet]; Erbay, R.H., Ed.; IntechOpen: London, UK, 2018; Available online: https://www.intechopen.com/chapters/59759 (accessed on 26 February 2022).
- Dorris, E.R.; Russell, J.; Murphy, M. Post-intubation subglottic stenosis: Aetiology at the cellular and molecular level. Eur. Respir. Rev. 2021, 30, 200218. [Google Scholar] [CrossRef] [PubMed]
- Kossyvaki, V.; Anagnostopoulos, N.; Kaltsakas, G.; Emmanouil, P.; Alsaid, A.; Touman, A.; Tzavara, C.; Koulouris, N.; Stratakos, G. The Value of Dyspnea and Spirometry in Detecting Relapse of Benign Tracheal Stenosis. Respiration 2022, 101, 174–183. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy region, Italy. JAMA 2020, 16, 1574–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients with 2019 Novel Coronavirus—Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Naunheim, M.R.; Zhou, A.S.; Puka, E.; Franco, R.A., Jr.; Carroll, T.L.; Teng, S.E.; Mallur, P.S.; Song, P.C. Laryngeal complications of COVID-19. Laryngoscope Investig. Otolaryngol. 2020, 30, 1117–1124. [Google Scholar] [CrossRef] [PubMed]
- Moran, J.V.; A Godil, S.; Goldner, B.; Godil, K.; Aslam, J. Post-Extubation Stridor Complicating COVID-19-Associated Acute Respiratory Distress Syndrome: A Case Series. Cureus 2020, 12, e10492. [Google Scholar] [CrossRef] [PubMed]
- Rouhani, M.J.; Clunie, G.; Thong, G.; Lovell, L.; Roe, J.; Ashcroft, M.; Holroyd, A.; Sandhu, G.; Al Yaghchi, C. A Prospective Study of Voice, Swallow, and Airway Outcomes Following Tracheostomy for COVID-19. Laryngoscope 2021, 131, E1918–E1925. [Google Scholar] [CrossRef] [PubMed]
- Miwa, M.; Nakajima, M.; Kaszynski, R.H.; Hamada, S.; Nakano, T.; Shirokawa, M.; Goto, H.; Yamaguchi, Y. Two Cases of Post-intubation Laryngotracheal Stenosis Occurring after Severe COVID-19. Intern. Med. 2021, 60, 473–477. [Google Scholar] [CrossRef]
- Scholfield, D.W.; Warner, E.; Ahmed, J.; Ghufoor, K. Subglottic and tracheal stenosis associated with coronavirus disease 2019. J. Laryngol. Otol. 2021, 135, 656–658. [Google Scholar] [CrossRef] [PubMed]
- Mattioli, F.; Marchioni, A.; Andreani, A.; Cappiello, G.; Fermi, M.; Presutti, L. Post-intubation tracheal stenosis in COVID-19 patients. Eur. Arch. Oto-Rhino-Laryngol. 2021, 283, 847–848. [Google Scholar] [CrossRef] [PubMed]
- Alturk, A.; Bara, A.; Darwish, B. Post intubation tracheal stenosis after severe COVID-19 infection: A report of two cases. Ann. Med. Surg. 2021, 67, 102468. [Google Scholar] [CrossRef]
- Sandu, K. Laryngotracheal Complications in Intubated COVID-19 Patients. Clin. Med. Insights: Case Rep. 2021, 14, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Fiacchini, G.; Tricò, D.; Ribechini, A.; Forfori, F.; Brogi, E.; Lucchi, M.; Berrettini, S.; Bertini, P.; Guarracino, F.; Bruschini, L. Evaluation of the Incidence and Potential Mechanisms of Tracheal Complications in Patients With COVID-19. JAMA Otolaryngol. Head Neck Surg. 2021, 147, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Bradley, B.T.; Maioli, H.; Johnston, R.; Chaudhry, I.; Fink, S.L.; Xu, H.; Najafian, B.; Deutsch, G.; Lacy, J.M.; Williams, T.; et al. Histopathology and ultrastructural findings of fatal COVID-19 infections in Washington State: A case series. Lancet 2020, 396, 320–332. [Google Scholar] [CrossRef]
- Angel, L.; Kon, Z.N.; Chang, S.H.; Rafeq, S.; Shekar, S.P.; Mitzman, B.; Amoroso, N.; Goldenberg, R.; Sureau, K.; Smith, D.E.; et al. Novel Percutaneous Tracheostomy for Critically Ill Patients with COVID-19. Ann. Thorac. Surg. 2020, 110, 1006–1011. [Google Scholar] [CrossRef] [PubMed]
- Marudi, A.; Branchetti, G.; Bertellini, E. Permissive Apnea in COVID-19 Tracheostomy: Alternative Health Worker Safe Procedure in Intensive Care Unit. Ann. Thorac. Surg. 2021, 111, 729–738. [Google Scholar] [CrossRef]
- Ershadi, R.; Rafieian, S.; Sarbazzadeh, J.; Vahedi, M. Tracheal stenosis following mild-to-moderate COVID-19 infection without history of tracheal intubation: A case report. Gen. Thorac. Cardiovasc. Surg. 2021, 23, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Freitag, L.; Ernst, A.; Unger, M.; Kovitz, K.; Marquette, C.H. A proposed classification system of central airway stenosis. Eur. Respir. J. 2007, 30, 7–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roncati, L.; Bergonzini, G.; Lusenti, B.; Nasillo, V.; Paolini, A.; Zanelli, G.; Corrado, S. High density of IgG4 secreting plasma cells in the fibrotic tissue from a surgically resected tracheal ring impaired by complex subglottic stenosis pots tracheostomy as immune expression of a Th2 response due to severe COVID-19. Ann. Hematol. 2021, 100, 2659–2660. [Google Scholar] [CrossRef] [PubMed]
- Fiorelli, S.; Menna, C.; Massullo, D.; Rendina, E.A. Managing benign tracheal stenosis during COVID-19 outbreak. Gen. Thorac. Cardiovasc. Surg. 2021, 69, 412–413. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | N (%) or Mean ± St Dev |
|---|---|
| Age (years, mean ± st dev) | 58 ± 9.5 |
| Gender (M/F) | 15/8 |
| Comorbidities | |
| BMI (mean ± st dev) | 29.4 ± 7 |
| Obesity (BMI > 30) (%) | 8/23 (34.7%) |
| Smoking History | 5/23 (21.7%) |
| Cardiovascular (Hypertension, Coronary dis) | 5/23 (21.7%) |
| Diabetes mellitus | 4/23 (17.4%) |
| Sleep Apnea Hypopnea s. | 3/23 (13%) |
| Other (COPD, Asthma, GERD etc) | None |
| COVID related | |
| Days of ICU hospitalization [mean ± st dev, (min–max), median] | 31.85 ± 22.7, (6–98), 25.5 |
| Days of orotracheal intubation before tracheostomy was performed. [mean ± st dev, (min–max), median] | 17.35 ± 7.4, (6–34), 15 |
| Tracheostomy, TC/surgical | 11/23 (47.8%), 9/2 |
| ICU pathogens (Pseudomonas sp., Klebsiella pn., Staph. Aureus, Acinetobacter sp.) isolated from aspirates. | 18/23 (78.3%) |
| Clinical/Radiological | N (%) or Mean ± St Dev |
|---|---|
| Dyspnea mMRC score | 3.04 ± 0.97 |
| Inspiratory stridor | 20/23 (86.7%) |
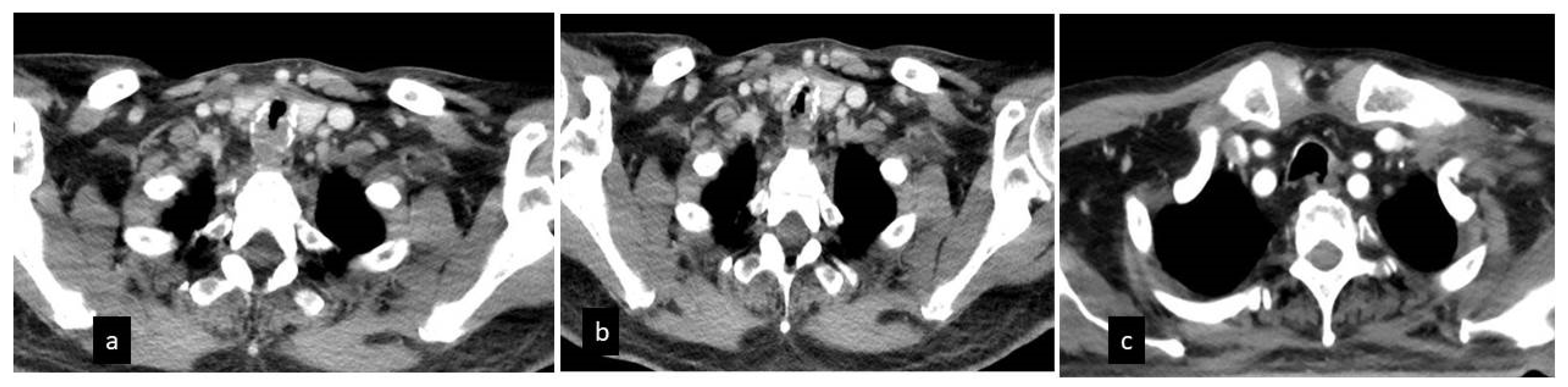
| Evidence tracheal cartilage fracture in the CT | 19/23 (82.6%) |
| Evidence of residual bilateral ground glass opacities | 13/23 (56.5%) |
| Bronchoscopy findings | |
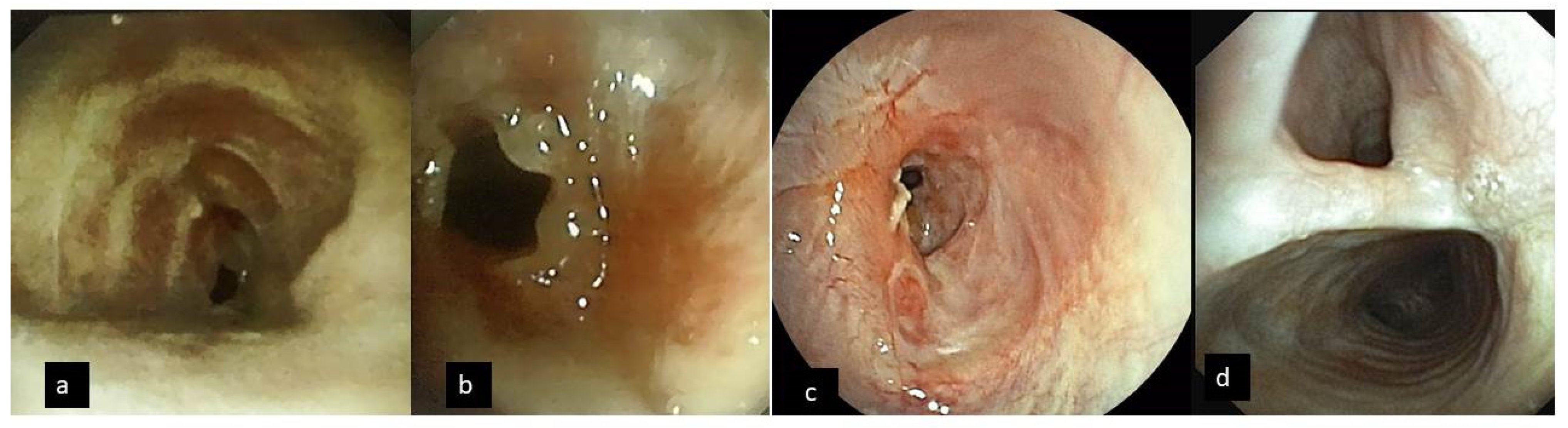
| Tracheal stenosis % | 84.45% ± 8.3% |
| Length of stenosis (cm) | 2.85 ± 0.9 |
| Subglottic/mid trachea | 12/11 |
| Complex or mixed/simple web | 21/2 |
| Distortion of the airway due to anterior wall cartilage fracture | 19/23 (82.6%) |
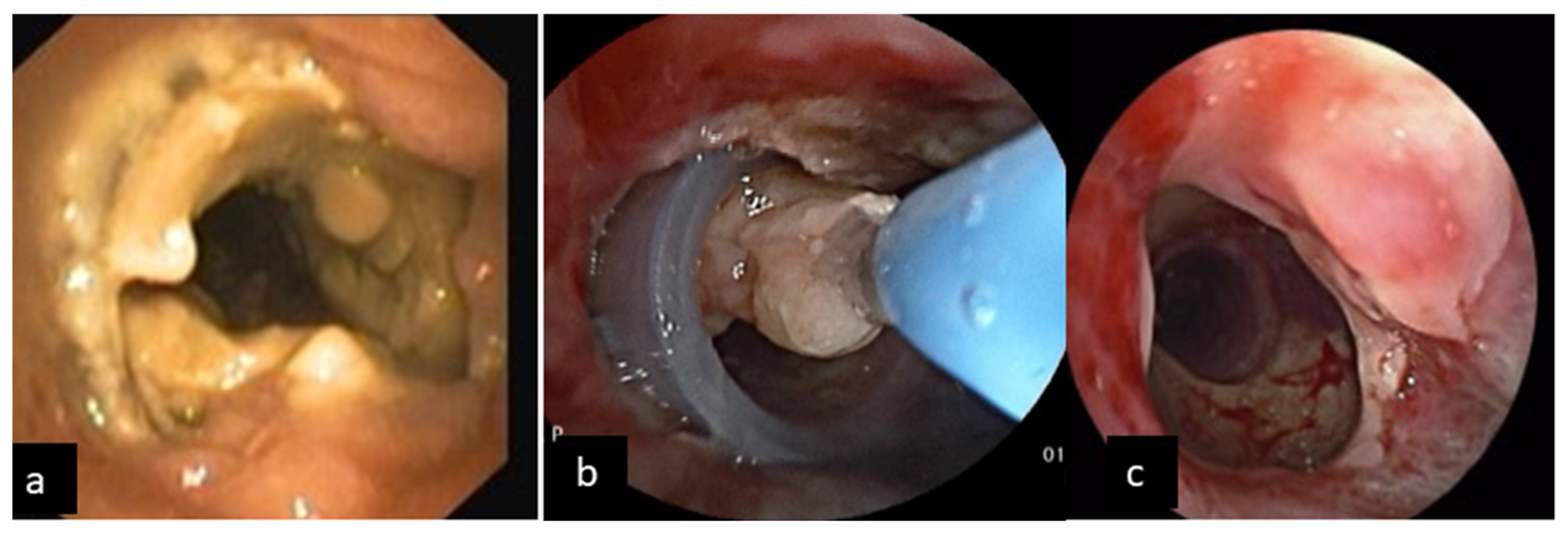
| Excessive Dynamic Airway Collapse | 5/23 (21.7%) |
| Tracheo-esophageal fistula | 2/23 (8.7%) |
| Foreign body aspiration | 1/23 (4.3%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stratakos, G.; Anagnostopoulos, N.; Alsaggaf, R.; Koukaki, E.; Bakiri, K.; Emmanouil, P.; Zisis, C.; Vachlas, K.; Vourlakou, C.; Koutsoukou, A. COVID-19 Patients Presenting with Post-Intubation Upper Airway Complications: A Parallel Epidemic? J. Clin. Med. 2022, 11, 1719. https://doi.org/10.3390/jcm11061719
Stratakos G, Anagnostopoulos N, Alsaggaf R, Koukaki E, Bakiri K, Emmanouil P, Zisis C, Vachlas K, Vourlakou C, Koutsoukou A. COVID-19 Patients Presenting with Post-Intubation Upper Airway Complications: A Parallel Epidemic? Journal of Clinical Medicine. 2022; 11(6):1719. https://doi.org/10.3390/jcm11061719
Chicago/Turabian StyleStratakos, Grigoris, Nektarios Anagnostopoulos, Rajaa Alsaggaf, Evangelia Koukaki, Katerina Bakiri, Philip Emmanouil, Charalampos Zisis, Konstantinos Vachlas, Christina Vourlakou, and Antonia Koutsoukou. 2022. "COVID-19 Patients Presenting with Post-Intubation Upper Airway Complications: A Parallel Epidemic?" Journal of Clinical Medicine 11, no. 6: 1719. https://doi.org/10.3390/jcm11061719
APA StyleStratakos, G., Anagnostopoulos, N., Alsaggaf, R., Koukaki, E., Bakiri, K., Emmanouil, P., Zisis, C., Vachlas, K., Vourlakou, C., & Koutsoukou, A. (2022). COVID-19 Patients Presenting with Post-Intubation Upper Airway Complications: A Parallel Epidemic? Journal of Clinical Medicine, 11(6), 1719. https://doi.org/10.3390/jcm11061719