
Randomized Controlled Trial Comparing a Multidisciplinary Intervention by a Geriatrician and a Cardiologist to Usual Care after a Heart Failure Hospitalization in Older Patients: The SENECOR Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Procedures
2.3. Variables
2.4. Geriatrician’s Interventions
2.5. Study Outcome
2.6. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Farré, N.; Vela, E.; Clèries, M.; Bustins, M.; Cainzos-Achirica, M.; Enjuanes, C.; Moliner, P.; Ruiz, S.; Rotellar, J.M.V.; Comín-Colet, J. Real world heart failure epidemiology and outcome: A population-based analysis of 88,195 patients. PLoS ONE 2017, 12, e0172745. [Google Scholar] [CrossRef] [PubMed]
- Fang, J.; Mensah, G.A.; Croft, J.B.; Keenan, N.L. Heart Failure-Related Hospitalization in the U.S., 1979 to 2004. J. Am. Coll. Cardiol. 2008, 52, 428–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avaldi, V.M.; Lenzi, J.; Castaldini, I.; Urbinati, S.; Di Pasquale, G.; Morini, M.; Protonotari, A.; Maggioni, A.P.; Fantini, M.P. Hospital Readmissions of Patients with Heart Failure: The Impact of Hospital and Primary Care Organizational Factors in Northern Italy. PLoS ONE 2015, 10, e0127796. [Google Scholar] [CrossRef]
- Senni, M.; Gavazzi, A.; Oliva, F.; Mortara, A.; Urso, R.; Pozzoli, M.; Metra, M.; Lucci, D.; Gonzini, L.; Cirrincione, V.; et al. In-hospital and 1-year outcomes of acute heart failure patients according to presentation (de novo vs. worsening) and ejection fraction. Results from IN-HF Outcome Registry. Int. J. Cardiol. 2014, 173, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Nichols, G.A.; Reynolds, K.; Kimes, T.M.; Rosales, A.G.; Chan, W.W. Comparison of Risk of Re-hospitalization, All-Cause Mortality, and Medical Care Resource Utilization in Patients With Heart Failure and Preserved Versus Reduced Ejection Fraction. Am. J. Cardiol. 2015, 116, 1088–1092. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, P.A.; Albert, N.M.; Allen, L.A.; Bluemke, D.A.; Butler, J.; Fonarow, G.C.; Ikonomidis, J.S.; Khavjou, O.; Konstam, M.A.; Maddox, T.M.; et al. Forecasting the Impact of Heart Failure in the United States. Circ. Heart Fail. 2013, 6, 606–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hafkamp, F.J.; Tio, R.A.; Otterspoor, L.C.; de Greef, T.; van Steenbergen, G.J.; van de Ven, A.R.T.; Smits, G.; Post, H.; van Veghel, D. Optimal effectiveness of heart failure management—An umbrella review of meta-analyses examining the effectiveness of interventions to reduce (re)hospitalizations in heart failure. Heart Fail. Rev. 2022, 1–66. [Google Scholar] [CrossRef] [PubMed]
- Keller, K.M.; Howlett, S.E. Sex Differences in the Biology and Pathology of the Aging Heart. Can. J. Cardiol. 2016, 32, 1065–1073. [Google Scholar] [CrossRef] [Green Version]
- Yáñez-Bisbe, L.; Garcia-Elias, A.; Tajes, M.; Almendros, I.; Rodríguez-Sinovas, A.; Inserte, J.; Ruiz-Meana, M.; Farré, R.; Farré, N.; Benito, B. Aging Impairs Reverse Remodeling and Recovery of Ventricular Function after Isoproterenol-Induced Cardiomyopathy. Int. J. Mol. Sci. 2021, 23, 174. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Imazio, M.; Cotroneo, A.; Gaschino, G.; Chinaglia, A.; Gareri, P.; Lacava, R.; Voci, T.D.; Trinchero, R. Management of heart failure in elderly people. Int. J. Clin. Pr. 2008, 62, 270–280. [Google Scholar] [CrossRef]
- Rich, M.W.; Chyun, D.A.; Skolnick, A.H.; Alexander, K.P.; Forman, D.E.; Kitzman, D.W.; Maurer, M.S.; McClurken, J.B.; Resnick, B.M.; Shen, W.K.; et al. Knowledge Gaps in Cardiovascular Care of the Older Adult Population. Circulation 2016, 133, 2103–2122. [Google Scholar] [CrossRef]
- Vitale, C.; Jankowska, E.; Hill, L.; Piepoli, M.; Doehner, W.; Anker, S.D.; Lainscak, M.; Jaarsma, T.; Ponikowski, P.; Rosano, G.M.; et al. Heart Failure Association of the European Society of Cardiology position paper on frailty in patients with heart failure. Eur. J. Heart Fail. 2019, 21, 1299–1305. [Google Scholar] [CrossRef]
- Gastelurrutia, P.; Lupón, J.; Altimir, S.; de Antonio, M.; González, B.; Cabanes, R.; Rodríguez, M.; Urrutia, A.; Domingo, M.; Zamora, E.; et al. Fragility is a key determinant of survival in heart failure patients. Int. J. Cardiol. 2014, 175, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Uchmanowicz, I.; Nessler, J.; Gobbens, R.; Gackowski, A.; Kurpas, D.; Straburzynska-Migaj, E.; Kałuzna-Oleksy, M.; Jankowska, E.A. Coexisting Frailty With Heart Failure. Front. Physiol. 2019, 10, 791. [Google Scholar] [CrossRef] [Green Version]
- Roig, T.; Márquez, M.Á.; Hernández, E.; Pineda, I.; Sabartés, O.; Miralles, R.; Inzitari, M. Valoración geriátrica y factores asociados a mortalidad en ancianos con insuficiencia cardíaca ingresados en una unidad de geriatría de agudos. Rev. Española Geriatría Gerontol. 2013, 48, 254–258. [Google Scholar] [CrossRef]
- Carrasco-Sánchez, F.J.; Páez-Rubio, M.I.; García-Moreno, J.M.; Vázquez-García, I.; Araujo-Sanabria, J.; La Llave, E.P.-D. Variables predictoras de mortalidad en pacientes ancianos hospitalizados por insuficiencia cardiaca con fracción de eyección preservada. Med. Clín. 2013, 141, 423–429. [Google Scholar] [CrossRef]
- Formiga, F.; Chivite, D.; Conde, A.; Ruiz-Laiglesia, F.; Franco Álvaro, G.; Bocanegra, C.P.; Manzano, L.; Pérez-Barquero, M.M. Basal functional status predicts three-month mortality after a heart failure hospitalization in elderly patients—The prospective RICA study. Int. J. Cardiol. 2014, 172, 127–131. [Google Scholar] [CrossRef]
- Gastelurrutia, P.; Lupón, J.; Altimir, S.; de Antonio, M.; González, B.; Cabanes, R.; Cano, L.; Urrutia, A.; Domingo, M.; Zamora, E.; et al. Effect of Fragility on Quality of Life in Patients with Heart Failure. Am. J. Cardiol. 2013, 112, 1785–1789. [Google Scholar] [CrossRef] [PubMed]
- Ellis, G.; Whitehead, M.A.; Robinson, D.; O’Neill, D.; Langhorne, P. Comprehensive geriatric assessment for older adults admitted to hospital: Meta-analysis of randomised controlled trials. BMJ 2011, 343, d6553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Auerbach, A.D.; Hamel, M.B.; Davis, R.B.; Connors, A.F.; Regueiro, C.; Desbiens, N.; Goldman, L.; Califf, R.M.; Dawson, N.V.; Wenger, N.; et al. Resource Use and Survival of Patients Hospitalized with Congestive Heart Failure: Differences in Care by Specialty of the Attending Physician. Ann. Intern. Med. 2000, 132, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-García, J.; Salamanca-Bautista, P.; Ferrero-Gregori, A.; Montero-Pérez-Barquero, M.; Puig, T.; Aramburu-Bodas, Ó.; Vázquez, R.; Formiga, F.; Delgado, J.; Arias-Jiménez, J.L.; et al. Prognostic Impact of Physician Specialty on the Prognosis of Outpatients with Heart Failure: Propensity Matched Analysis of the REDINSCOR and RICA Registries. Rev. Española Cardiol. 2017, 70, 347–354. [Google Scholar] [CrossRef]
- Green, A.R.; Leff, B.; Wang, Y.; Spatz, E.S.; Masoudi, F.A.; Peterson, P.N.; Daugherty, S.L.; Matlock, D.D. Geriatric Conditions in Patients Undergoing Defibrillator Implantation for Prevention of Sudden Cardiac Death. Circ. Cardiovasc. Qual. Outcomes 2016, 9, 23–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005, 173, 489–495. [Google Scholar] [CrossRef] [Green Version]
- Abraham, W.T.; Psotka, M.A.; Fiuzat, M.; Filippatos, G.; Lindenfeld, J.; Mehran, R.; Ambardekar, A.V.; Carson, P.E.; Jacob, R.; Januzzi, L.J., Jr.; et al. Standardized definitions for evaluation of heart failure therapies: Scientific expert panel from the Heart Failure Collaboratory and Academic Research Consortium. Eur. J. Heart Fail. 2020, 22, 2175–2186. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.; Brody, E. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Mahoney, F.; Barthel, D. Funtional evaluation: The Barthel Index. MD State Med. J. 1965, 14, 61–65. [Google Scholar]
- Pfeiffer, E. A Short Portable Mental Status Questionnaire for the Assessment of Organic Brain Deficit in Elderly Patients. J. Am. Geriatr. Soc. 1975, 23, 433–441. [Google Scholar] [CrossRef]
- Feng, Y.-S.; Kohlmann, T.; Janssen, M.F.; Buchholz, I. Psychometric properties of the EQ-5D-5L: A systematic review of the literature. Qual. Life Res. 2021, 30, 647–673. [Google Scholar] [CrossRef]
- Spertus, J.A.; Jones, P.G.; Sandhu, A.T.; Arnold, S.V. Interpreting the Kansas City Cardiomyopathy Questionnaire in Clinical Trials and Clinical Care. J. Am. Coll. Cardiol. 2020, 76, 2379–2390. [Google Scholar] [CrossRef]
- Garcia-Caselles, P.; Miralles, R.; Arellano, M.; Torres, R.; Aguilera, A.; Pi-Figueras, M.; Cervera, A. Validation of a modified version of the gijon’s social-familial evaluation scale (sfes): The “Barcelona sfes version”, for patients with cognitive impairment. Arch. Gerontol. Geriatr. 2004, 38, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Martí, D.; Miralles, R.; Llorach, I.; García-Palleiro, P.; Esperanza, A.; Guillem, J.; Cervera, A.M. Trastornos depresivos en una unidad de convalecencia: Experiencia y validación de una versión española de 15 preguntas de la escala de depresión geriátrica de Yesavage. Rev. Esp. Geriatr. Gerontol. 2000, 35, 7–14. [Google Scholar]
- Rubenstein, L.Z.; Harker, J.O.; Salvà, A.; Guigoz, Y.; Vellas, B. Screening for Undernutrition in Geriatric Practice: Developing the Short-Form Mini-Nutritional Assessment (MNA-SF). J. Gerontol. Ser. A 2001, 56, M366–M372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Comin-Colet, J.; Verdú-Rotellar, J.M.; Vela, E.; Clèries, M.; Bustins, M.; Mendoza, L.; Badosa, N.; Cladellas, M.; Ferré, S.; Bruguera, J. Efficacy of an Integrated Hospital-primary Care Program for Heart Failure: A Population-based Analysis of 56,742 Patients. Rev. Española Cardiol. 2014, 67, 283–293. [Google Scholar] [CrossRef] [PubMed]
- Sample Size and Power Calculator. Available online: https://www.imim.cat/ofertadeserveis/software-public/granmo/ (accessed on 7 May 2018).
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Mizuno, M.; Kajimoto, K.; Sato, N.; Yumino, D.; Minami, Y.; Murai, K.; Munakata, R.; Asai, K.; Keida, T.; Sakata, Y.; et al. Clinical profile, management, and mortality in very-elderly patients hospitalized with acute decompensated heart failure: An analysis from the ATTEND registry. Eur. J. Intern. Med. 2016, 27, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Komajda, M.; Hanon, O.; Hochadel, M.; Lopez-Sendon, J.L.; Follath, F.; Ponikowski, P.; Harjola, V.-P.; Drexler, H.; Dickstein, K.; Tavazzi, L.; et al. Contemporary management of octogenarians hospitalized for heart failure in Europe: Euro Heart Failure Survey II. Eur. Heart J. 2008, 30, 478–486. [Google Scholar] [CrossRef] [Green Version]
- Ruiz-Laiglesia, F.-J.; Sanchez-Marteles, M.; Perez-Calvo, J.-I.; Formiga, F.; Bartolome-Satue, J.A.; Armengou-Arxe, A.; Lopez-Quiros, R.; Perez-Silvestre, J.; Serrado-Iglesias, A.; Montero-Perez-Barquero, M. Comorbidity in heart failure. Results of the Spanish RICA Registry. QJM Int. J. Med. 2014, 107, 989–994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saczynski, J.S.; Darling, C.E.; Spencer, F.A.; Lessard, D.; Gore, J.M.; Goldberg, R.J. Clinical Features, Treatment Practices, and Hospital and Long-Term Outcomes of Older Patients Hospitalized with Decompensated Heart Failure: The Worcester Heart Failure Study. J. Am. Geriatr. Soc. 2009, 57, 1587–1594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desai, A.S.; Claggett, B.; Pfeffer, M.A.; Bello, N.; Finn, P.V.; Granger, C.B.; McMurray, J.J.; Pocock, S.; Swedberg, K.; Yusuf, S.; et al. Influence of Hospitalization for Cardiovascular Versus Noncardiovascular Reasons on Subsequent Mortality in Patients with Chronic Heart Failure Across the Spectrum of Ejection Fraction. Circ. Heart Fail. 2014, 7, 895–902. [Google Scholar] [CrossRef] [Green Version]
- Belarte-Tornero, L.; Valdivielso-Moré, S.; Elcano, M.V.; Solé-González, E.; Ruíz-Bustillo, S.; Calvo-Fernández, A.; Subinara, I.; Cabero, P.; Soler, C.; Cubero-Gallego, H.; et al. Prognostic Implications of Chronic Heart Failure and Utility of NT-proBNP Levels in Heart Failure Patients with SARS-CoV-2 Infection. J. Clin. Med. 2021, 10, 323. [Google Scholar] [CrossRef]
- Jepma, P.; Verweij, L.; Buurman, B.M.; Terbraak, M.S.; Daliri, S.; Latour, C.H.M.; ter Riet, G.; Çarkit, F.K.; Dekker, J.; Klunder, J.L.; et al. The nurse-coordinated cardiac care bridge transitional care programme: A randomised clinical trial. Age Ageing 2021, 50, 2105–2115. [Google Scholar] [CrossRef] [PubMed]
- Comín-Colet, J.; Enjuanes, C.; Rotellar, J.M.V.; Linas, A.; Ruiz-Rodriguez, M.D.P.; González-Robledo, G.; Farre, N.; Borja, P.M.; Bustillo, S.R.; Bruguera-Cortada, J. Impact on clinical events and healthcare costs of adding telemedicine to multidisciplinary disease management programmes for heart failure: Results of a randomized controlled trial. J. Telemed. Telecare 2015, 22, 282–295. [Google Scholar] [CrossRef]
- Visco, V.; Ferruzzi, G.J.; Nicastro, F.; Virtuoso, N.; Carrizzo, A.; Galasso, G.; Vecchione, C.; Ciccarelli, M. Artificial Intelligence as a Business Partner in Cardiovascular Precision Medicine: An Emerging Approach for Disease Detection and Treatment Optimization. Curr. Med. Chem. 2021, 28, 6569–6590. [Google Scholar] [CrossRef] [PubMed]
- Orr, N.M.; Forman, D.E.; De Matteis, G.; Gambassi, G. Heart Failure Among Older Adults in Skilled Nursing Facilities: More of a Dilemma Than Many Now Realize. Curr. Geriatr. Rep. 2015, 4, 318–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Usual Care (n = 75) | Intervention (n = 75) | p-Value | |
|---|---|---|---|
| Age (years) | 82.6 ± 4.5 | 81.6 ± 4.9 | 0.22 |
| Female | 38 (50.7) | 37 (49.3) | 0.87 |
| Hypertension | 67 (89.3) | 66 (88) | 0.59 |
| Diabetes mellitus | 32 (42.7) | 32 (42.7) | 0.82 |
| Dyslipidemia | 49 (65.3) | 46 (61.3) | 0.61 |
| Stroke/TIA | 9 (12) | 10 (13.3) | 0.88 |
| Chronic kidney disease | 54 (72) | 52 (69.3) | 0.72 |
| Anemia | 48 (64) | 42 (56) | 0.32 |
| Sleep apnea | 8 (10.7) | 8 (10.7) | 0.98 |
| Peripheral vascular disease | 10 (13.3) | 14 (18.7) | 0.41 |
| Chronic lung disease | 28 (37.3) | 20 (26.7) | 0.16 |
| Cancer | 19 (25.3) | 18 (24) | 0.92 |
| Myocardial infarction | 21 (28) | 15 (20) | 0.25 |
| Coronary intervention | 16 (21.3) | 13 (17.3) | 0.54 |
| TAVI or Mitraclip | 1 (1.4) | 3 (4) | 0.51 |
| Cardiac surgery: | |||
| 2 (2.7) 3 (4) 1 (1.4) | 3 (4) 7 (9.3) 3 (4) | 0.37 |
| Atrial fibrillation or flutter | 47 (62.7) | 57 (76) | 0.08 |
| Moderate to severe valve disease | 25 (33.3) | 24 (32) | 0.86 |
| Device therapy: | |||
| 9 (12) 3 (4) | 14 (18.7) 2 (2.7) | 0.19 |
| Previous history of HF | 42 (56) | 43 (57.3) | 0.87 |
| Duration of HF *: | |||
| 7 (16.3) 3 (7) 6 (14) 22 (51.2) 5 (11.6) | 9 (20.5) 1 (2.3) 3 (6.8) 14 (31.8) 16 (36.4) | 0.06 |
| HF hospitalization the previous year * | 19 (45.2) | 15 (36.6) | 0.42 |
| HF categories: | |||
| 47 (62.7) 11 (14.7) 17 (22.7) | 51 (68) 16 (21.3) 8 (10.7) | 0.72 |
| Echocardiographic parameters | |||
| LVEF (%) | 51.3 ± 14.4 | 53.5 ± 13.9 | 0.34 |
| TAPSE (mm), n = 138 | 17.9 ± 4.0 | 17.2 ± 3.9 | 0.30 |
| Left ventricular mass index (g/m2). n = 145 | 129.9 ± 35.8 | 127.3 ± 33.7 | 0.96 |
| Right ventricle (mm), n = 95 | 28.1 ± 7.0 | 30.4 ± 6.6 | 0.09 |
| Medications at discharge | |||
| ACEI/ARB-2/ARNI | 35 (46.7) | 43 (57.3) | 0.19 |
| MRA | 9 (12) | 12 (16) | 0.48 |
| Betablockers | 55 (73.3) | 53 (70.7) | 0.72 |
| Diuretics | 71 (94.7) | 73 (97.3) | 0.34 |
| Anticoagulation | 48 (64) | 58 (77.3) | 0.07 |
| Antiplatelet therapy | 16 (21.3) | 15 (20) | 0.84 |
| Oral antidiabetic drugs | 24 (32) | 24 (32) | 0.96 |
| Insulin | 14 (18.4) | 14 (18.4) | 1.0 |
| Proton-pump inhibitors | 58 (77.3) | 47 (62.7) | 0.05 |
| Statin | 52 (69.3) | 44 (58.7) | 0.17 |
| Calcium channel antagonists | 23 (31.3) | 21 (28.4) | 0.72 |
| Nitrates | 17 (22.7) | 14 (18.7) | 0.55 |
| Hydralazine | 9 (12) | 12 (16) | 0.48 |
| Amiodarone | 12 (16) | 13 (17.6) | 0.80 |
| Digoxin | 2 (2.7) | 2 (2.7) | 0.69 |
| Vitamin D supplements | 25 (33.3) | 21 (28) | 0.48 |
| Oral iron supplements | 21 (28) | 21 (28) | 1.0 |
| Benzodiazepines | 17 (22.7) | 13 (17.3) | 0.41 |
| Antidepressant drugs | 16 (21.3) | 23 (30.7) | 0.19 |
| Bronchodilators | 28 (37.3) | 22 (29.3) | 0.30 |
| Usual Care (n = 75) | Intervention (n = 75) | p-Value | |
|---|---|---|---|
| Length of hospitalization (days) | 9 (6–12) | 9 (5–13) | 0.71 |
| NT-proBNP at discharge, pg/mL | 2843 (1162–5943) | 2454 (1456–4328) | 0.51 |
| High-sensitivity T troponin (Hs-TnT) at discharge, ng/L | 46.29 (29.55–74.99) | 37.18 (27.81–63.5) | 0.15 |
| eGFR (mL/min) at discharge | 44.2 ± 19.5 | 48.5 ± 20.4 | 0.19 |
| Days from discharge to the first appointment | 6 (5–11) | 7 (6–12) | 0.08 |
| Type of follow-up: | |||
| 36 (48) 20 (26.7) 14 (18.7) | 42 (56) 10 (13.3) 14 (18.7) | 0.16 |
| Frailty (Clinical Frailty Scale) ≥ 4 | 39 (52) | 39 (52) | 1 |
| Clinical Frailty Scale | 4.1 ± 1.4 | 3.9 ± 1.2 | 0.49 |
| Barthel index | 84.0 ± 19.8 | 87.9 ± 13.4 | 0.17 |
| Basic activities of daily living (Barthel index): | |||
| 22 (31.4) 38 (54.3) 10 (14.3) | 20 (27.8) 49 (68.1) 3 (4.2) | 0.073 |
| Instrumental activities of daily living (Lawton index) | 5.2 ± 2.3 | 4.7 ± 1.9 | 0.19 |
| Pfeiffer Short Portable Mental Status Questionnaire (SPMSQ) | 1.33 ± 1.4 | 1.76 ± 1.8 | 0.11 |
| NYHA functional class | 2.3 ± 0.6 | 2.2 ± 0.6 | 0.35 |
| Usual Care (n = 75) | Intervention (n = 75) | Hazard Ratio | p-Value | |
|---|---|---|---|---|
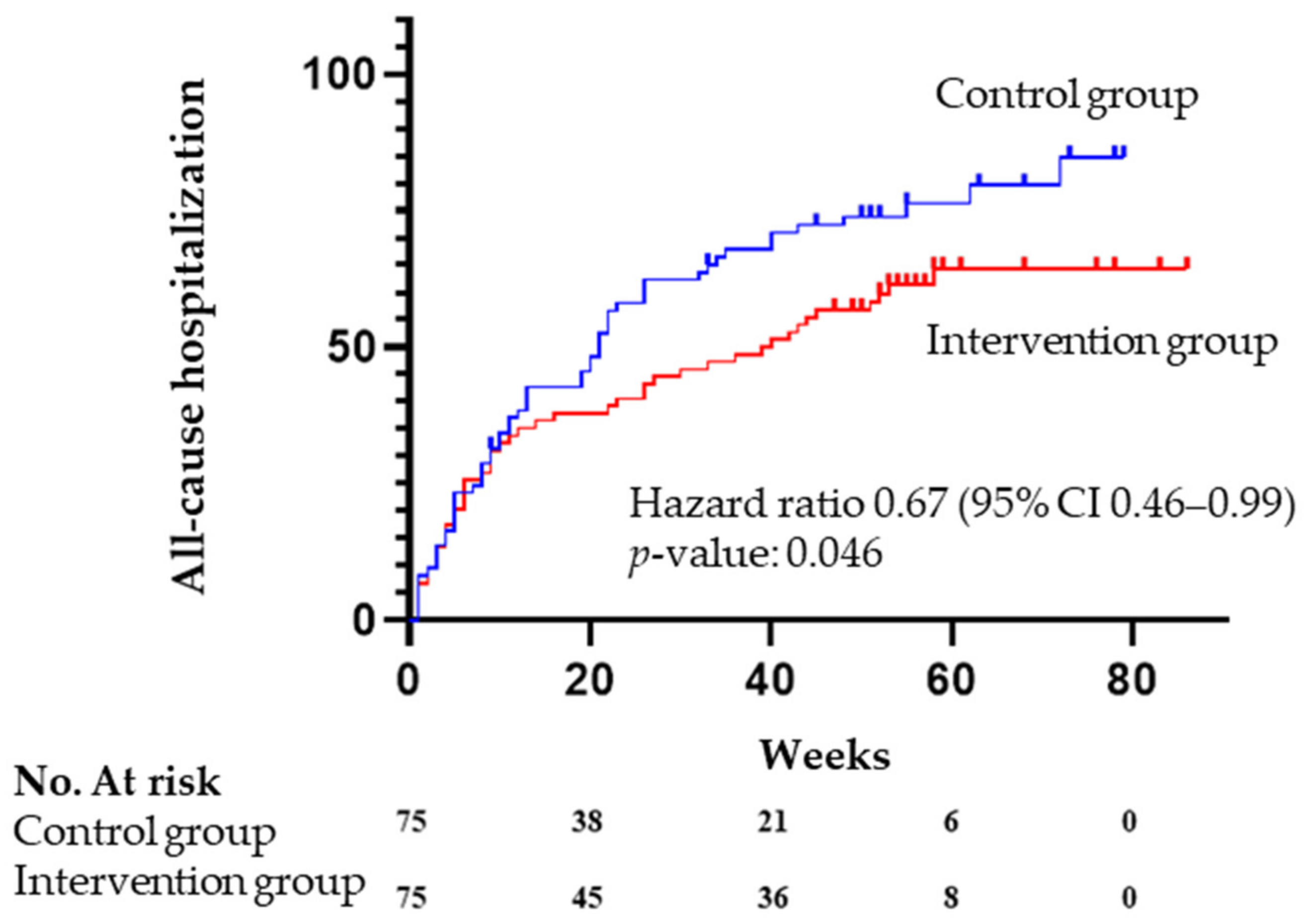
| All-cause hospitalization | 58 (77.3) | 47 (62.7) | 0.67 (0.46–0.99) | 0.046 |
| HF hospitalization | 30 (40) | 26 (34.7) | 0.79 (0.46–1.33) | 0.37 |
| Planned intervention/ hospitalization | 11 (14.7) | 17 (22.7) | 1.48 (0.69–3.20) | 0.315 |
| All cause hospitalization or death | 60 (80.0) | 47 (62.7) | 0.67 (0.45–0.98) | 0.038 |
| All-cause mortality | 20 (26.7) | 17 (22.7) | 0.81 (0.43–1.56) | 0.53 |
| Emergency room visit | 35 (46.7) | 32 (42.72) | 0.80 (0.492–1.296) | 0.36 |
| Intervention | Control | HR | CI 95 | p | |
|---|---|---|---|---|---|
| Overall | 47/75 | 58/75 | 0.67 | 0.46–0.99 | 0.046 |
| Sex | |||||
| Female | 20/37 | 33/38 | 0.44 | 0.25–0.78 | 0.005 |
| Male | 27/38 | 25/37 | 1.02 | 0.59–1.76 | 0.94 |
| Left ventricular ejection fraction | |||||
| Preserved | 25/47 | 40/46 | 0.41 | 0.24–0.67 | <0.001 |
| Reduced | 19/23 | 18/29 | 1.59 | 0.83–3.04 | 0.16 |
| Frailty | |||||
| Yes | 24/39 | 31/39 | 0.70 | 0.41–1.19 | 0.19 |
| No | 23/35 | 26/35 | 0.70 | 0.40–1.24 | 0.22 |
| Previous HF diagnosis | |||||
| Yes | 17/32 | 25/33 | 0.49 | 0.26–0.92 | 0.026 |
| No | 30/43 | 33/42 | 0.81 | 0.49.1.33 | 0.41 |
| HF hospitalization in ≤12 months | |||||
| Yes | 16/19 | 11/15 | 1.12 | 0.51–2.45 | 0.78 |
| No | 17/27 | 17/23 | 0.70 | 0.35–1.37 | 0.30 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herrero-Torrus, M.; Badosa, N.; Roqueta, C.; Ruiz-Bustillo, S.; Solé-González, E.; Belarte-Tornero, L.C.; Valdivielso-Moré, S.; Vázquez, O.; Farré, N. Randomized Controlled Trial Comparing a Multidisciplinary Intervention by a Geriatrician and a Cardiologist to Usual Care after a Heart Failure Hospitalization in Older Patients: The SENECOR Study. J. Clin. Med. 2022, 11, 1932. https://doi.org/10.3390/jcm11071932
Herrero-Torrus M, Badosa N, Roqueta C, Ruiz-Bustillo S, Solé-González E, Belarte-Tornero LC, Valdivielso-Moré S, Vázquez O, Farré N. Randomized Controlled Trial Comparing a Multidisciplinary Intervention by a Geriatrician and a Cardiologist to Usual Care after a Heart Failure Hospitalization in Older Patients: The SENECOR Study. Journal of Clinical Medicine. 2022; 11(7):1932. https://doi.org/10.3390/jcm11071932
Chicago/Turabian StyleHerrero-Torrus, Marta, Neus Badosa, Cristina Roqueta, Sonia Ruiz-Bustillo, Eduard Solé-González, Laia C. Belarte-Tornero, Sandra Valdivielso-Moré, Olga Vázquez, and Núria Farré. 2022. "Randomized Controlled Trial Comparing a Multidisciplinary Intervention by a Geriatrician and a Cardiologist to Usual Care after a Heart Failure Hospitalization in Older Patients: The SENECOR Study" Journal of Clinical Medicine 11, no. 7: 1932. https://doi.org/10.3390/jcm11071932
APA StyleHerrero-Torrus, M., Badosa, N., Roqueta, C., Ruiz-Bustillo, S., Solé-González, E., Belarte-Tornero, L. C., Valdivielso-Moré, S., Vázquez, O., & Farré, N. (2022). Randomized Controlled Trial Comparing a Multidisciplinary Intervention by a Geriatrician and a Cardiologist to Usual Care after a Heart Failure Hospitalization in Older Patients: The SENECOR Study. Journal of Clinical Medicine, 11(7), 1932. https://doi.org/10.3390/jcm11071932