
The Effect of the Frequently Used Cinacalcet for pHPT during the COVID-19 Pandemic on Perioperative Decrease in Parathyroid Hormone


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Data Acquisition
2.2. Statistical Analysis
3. Result
3.1. Baseline Patient Characteristics
3.2. Impact of Cincalcet on the Perioperative Biochemical Changes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ASA | American Society of Anesthesiologists |
| COVID-19 | coronavirus disease 2019 |
| IQR | interquartile range |
| IOPTH | intraoperative parathyroid hormone |
| PTH | parathyroid hormone |
| pHPT | primary hyperparathyroidism |
References
- Bilezikian, J.P.; Cusano, N.E.; Khan, A.A.; Liu, J.M.; Marcocci, C.; Bandeira, F. Primary hyperparathyroidism. Nat. Rev. Dis. Primers 2016, 2, 16033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shawky, M.S.; Sakr, M.F.; Nabawi, A.S.; Abdel-Aziz, T.E.; De Jong, M.C.; Garcia, V.R.; Rozalén García, V.; Lam, F.; Soromani, F.; Smart, J.; et al. Influence of common clinical variables on intraoperative parathyroid hormone monitoring during surgery for primary hyperparathyroidism. J. Endocrinol. Investig. 2020, 43, 1205–1212. [Google Scholar] [CrossRef] [PubMed]
- Melton, L.J., 3rd. The epidemiology of primary hyperparathyroidism in North America. J. Bone Miner Res. 2002, 17 (Suppl. 2), N12-7. [Google Scholar] [PubMed]
- Abood, A.; Vestergaard, P. Increasing incidence of primary hyperparathyroidism in Denmark. Dan Med. J. 2013, 60, A4567. [Google Scholar]
- Griebeler, M.L.; Kearns, A.E.; Ryu, E.; Hathcock, M.A.; Melton, L.J., 3rd; Wermers, R.A. Secular trends in the incidence of primary hyperparathyroidism over five decades (1965–2010). Bone 2015, 73, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Nilsson, I.L. Primary hyperparathyroidism: Should surgery be performed on all patients? Current evidence and residual uncertainties. J. Intern. Med. 2019, 285, 149–164. [Google Scholar] [CrossRef] [Green Version]
- Weber, T.; Dotzenrath, C.; Dralle, H.; Niederle, P.; Riss, K.; Holzer, J.; Kußmann, J.; Trupka, A.; Negele, T.; Kaderli, R.; et al. Management of primary and renal hyperparathyroidism: Guidelines from the German Association of Endocrine Surgeons (CAEK). Langenbecks Arch. Surg. 2021, 406, 571–585. [Google Scholar] [CrossRef]
- Callender, G.G.; Udelsman, R. Surgery for primary hyperparathyroidism. Cancer 2014, 120, 3602–3616. [Google Scholar] [CrossRef]
- Udelsman, R.; Akerstrom, G.; Biagini, C.; Duh, Q.Y.; Miccoli, P.; Niederle, B.; Tonelli, F. The surgical management of asymptomatic primary hyperparathyroidism: Proceedings of the Fourth International Workshop. J. Clin. Endocrinol. Metab. 2014, 99, 3595–3606. [Google Scholar] [CrossRef] [Green Version]
- Wilhelm, S.M.; Wang, T.S.; Ruan, D.T.; Lee, J.A.; Asa, S.L.; Duh, Q.Y.; Doherty, G.M.; Herrera, M.F.; Pasieka, J.L.; Perrier, N.D.; et al. The American Association of Endocrine Surgeons Guidelines for Definitive Management of Primary Hyperparathyroidism. JAMA Surg. 2016, 151, 959–968. [Google Scholar] [CrossRef]
- Irvin, G.L.; Solorzano, C.C.; Carneiro, D.A. Quick intraoperative parathyroid hormone assay: Surgical adjunct to allow limited parathyroidectomy, improve success rate, and predict outcome. World J. Surg. 2004, 28, 1287–1292. [Google Scholar] [CrossRef]
- Bell, D.; Hale, J.; Go, C.; Challis, B.G.; Das, T.; Fish, B.; Casey, R.T. A single-centre retrospective analysis of cinacalcet therapy in primary hyperparathyroidism. Endocr. Connect. 2021, 10, 1435–1444. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Gittoes, N.J.; Criseno, S.; Appelman-Dijkstra, N.M.; Bollerslev, J.; Canalis, E.; Rejnmark, L.; Hassan-Smith, Z. ENDOCRINOLOGY IN THE TIME OF COVID-19: Management of calcium metabolic disorders and osteoporosis. Eur. J. Endocrinol. 2020, 183, G57–G65. [Google Scholar] [CrossRef]
- Dandurand, K.; Ali, D.S.; Khan, A.A. Primary Hyperparathyroidism: A Narrative Review of Diagnosis and Medical Management. J. Clin. Med. 2021, 10, 1604. [Google Scholar] [CrossRef]
- Khan, A.; Bilezikian, J.; Bone, H.; Gurevich, A.; Lakatos, P.; Misiorowski, W.; Rozhinskaya, L.; Trotman, M.-L.; Tóth, M. Cinacalcet normalizes serum calcium in a double-blind randomized, placebo-controlled study in patients with primary hyperparathyroidism with contraindications to surgery. Eur. J. Endocrinol. 2015, 172, 527–535. [Google Scholar] [CrossRef] [Green Version]
- Ng, C.H.; Chin, Y.H.; Tan, M.H.Q.; Ng, J.X.; Yang, S.P.; Kiew, J.J.; Khoo, C.M. Cinacalcet and primary hyperparathyroidism: Systematic review and meta regression. Endocr. Connect. 2020, 9, 724–735. [Google Scholar] [CrossRef]
- Norman, J.; Lopez, J.; Politz, D. Cinacalcet (Sensipar) provides no measurable clinical benefits for patients with primary hyperparathyroidism and may accelerate bone loss with prolonged use. Ann. Surg. Oncol. 2012, 19, 1466–1471. [Google Scholar] [CrossRef]
- Schwarz, P.; Body, J.J.; Cap, J.; Hofbauer, L.C.; Farouk, M.; Gessl, A.; Kuhn, J.M.; Marcocci, C.; Mattin, C.; Muñoz Torres, M. The PRIMARA study: A prospective, descriptive, observational study to review cinacalcet use in patients with primary hyperparathyroidism in clinical practice. Eur. J. Endocrinol. 2014, 171, 727–735. [Google Scholar] [CrossRef]
- Irvin, G.L., 3rd; Carneiro, D.M.; Solorzano, C.C. Progress in the operative management of sporadic primary hyperparathyroidism over 34 years. Ann. Surg. 2004, 239, 704–708, discussion 8–11. [Google Scholar] [CrossRef]
- Sokoll, L.J.; Drew, H.; Udelsman, R. Intraoperative parathyroid hormone analysis: A study of 200 consecutive cases. Clin. Chem. 2000, 46, 1662–1668. [Google Scholar] [CrossRef] [Green Version]
- Patel, K.N.; Caso, R. Intraoperative Parathyroid Hormone Monitoring: Optimal Utilization. Surg. Oncol. Clin. N. Am. 2016, 25, 91–101. [Google Scholar] [CrossRef]
- Miller, B.S.; England, B.G.; Nehs, M.; Burney, R.E.; Doherty, G.M.; Gauger, P.G. Interpretation of intraoperative parathyroid hormone monitoring in patients with baseline parathyroid hormone levels of <100 pg/mL. Surgery 2006, 140, 883–889, discussion 9–90. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| All Patients | Cinacalcet (CG) | Non-Cinacalcet (non-CG) | |
|---|---|---|---|
| Number of Patients (n) | 72 | 22 | 50 |
| Age † | 63.5 (53–76) | 60 (52–70) | 66 (55–77) |
| Sex * | |||
| Male | 21 (29%) | 11 (52%) | 10 (48%) |
| Female | 51 (71%) | 11 (22%) | 40 (78%) |
| ASA * | |||
| I | 10 (14%) | 3 (14%) | 7 (14%) |
| II | 38 (53%) | 12 (55%) | 26 (52%) |
| III | 23 (32%) | 6 (8%) | 17 (34%) |
| IV | 1 (1%) | 1 (4%) | 0 |
| Symptomatic pHPT * | 39 (54%) | 12 (55%) | 27 (54%) |
| Asymptomatic pHPT * | 33 (46%) | 10 (45%) | 23 (46%) |
| Chron. renal failure * | 3 (4%) | 1 (5%) | 2 (4%) |
| Serum creatinine preoperative (45–84 µmol/L) † | 71.5 (59.7–82.2) | 74.5 (62.2–89.2) | 71 (59.0–80.7) |
| Serum urea preoperative (2,8–8,1 mmol/L) † | 4.6 (3.8–5.5) | 4.5 (3.8–5.6) | 4.6 (3.8–5.5) |
| Surgical procedure * | |||
| NSD adenom extirpation | 72 (100%) | 22 (100%) | 50 (100%) |
| Thyreoidectomy | 23 (32%) | 6 (27%) | 17 (34%) |
| Hemithyreoidectomy | 17 (24%) | 5 (23%) | 12 (24%) |
| Duration of surgery (min) † | 90 (59.5–115.0) | 90 (62.5–100.7) | 90 (56.2–115.0) |
| Hospital stay (days) † | 6 (5.0–6.0) | 6 (5.2–6.0) | 6 (5.0–6.7) |
| Laboratory Parameter (Normal Values) | CG | non-CG | p Value |
|---|---|---|---|
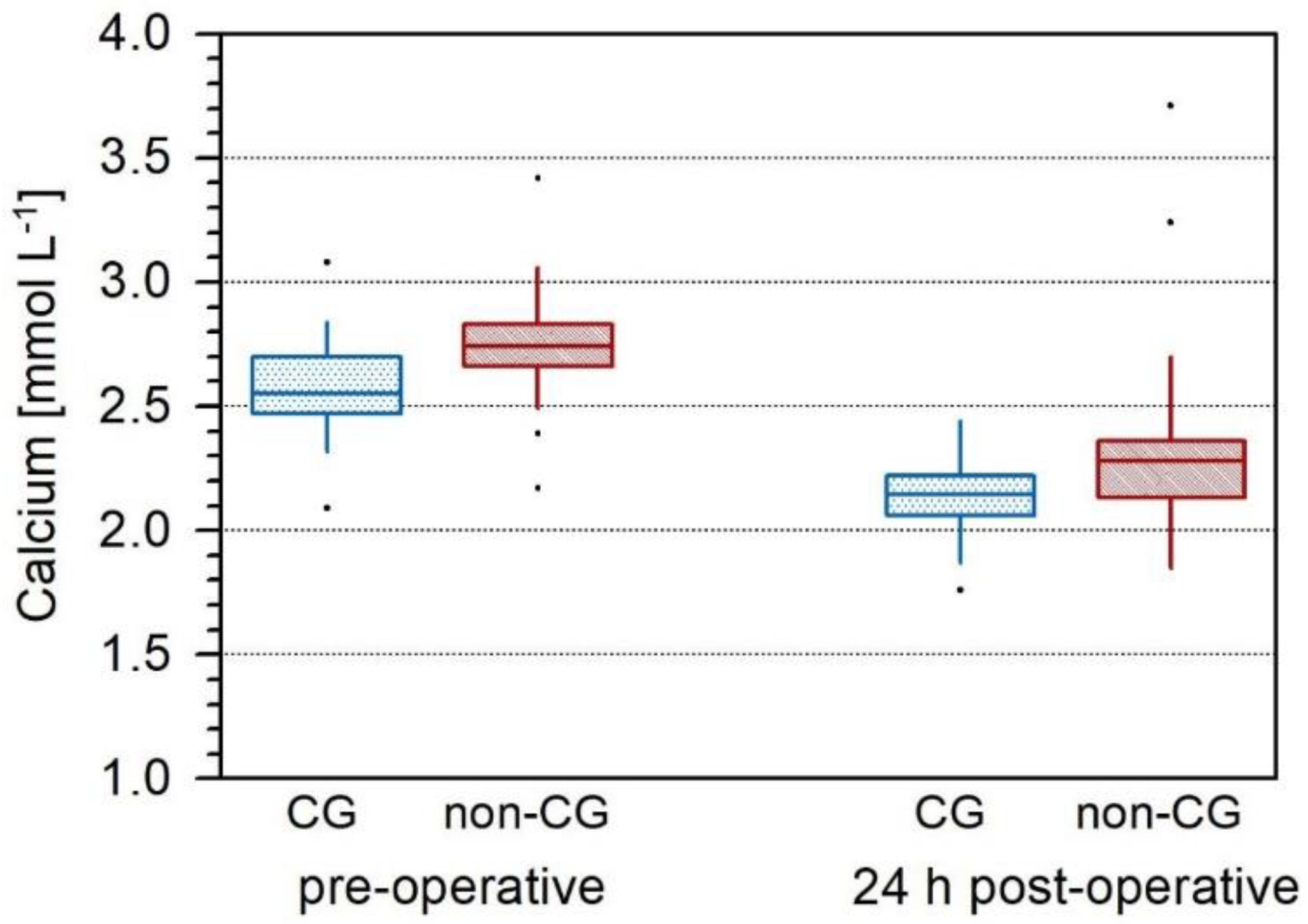
| Calcium preoperative (2.2–2.55 mmol/L) (8.8–10.23 mg/dL) | 2.55 (2.48–2.7) mmol/L 10.23 (9.95–10.82) mg/dL | 2.74 (2.66–2.83) mmol/L 10.99 (10.67–11.35) mg/dL | <0.001 * |
| Calcium 24 h postoperative (2.2–2.55 mmol/L) (8.8–10.23 mg/dL) | 2.14 (2.06–2.21) 8.58 (8.26–8.86) mg/dL | 2.28 (2.13–2.35) mmol/L 9.14 (8.54–9.42) mg/dL | 0.008 * |
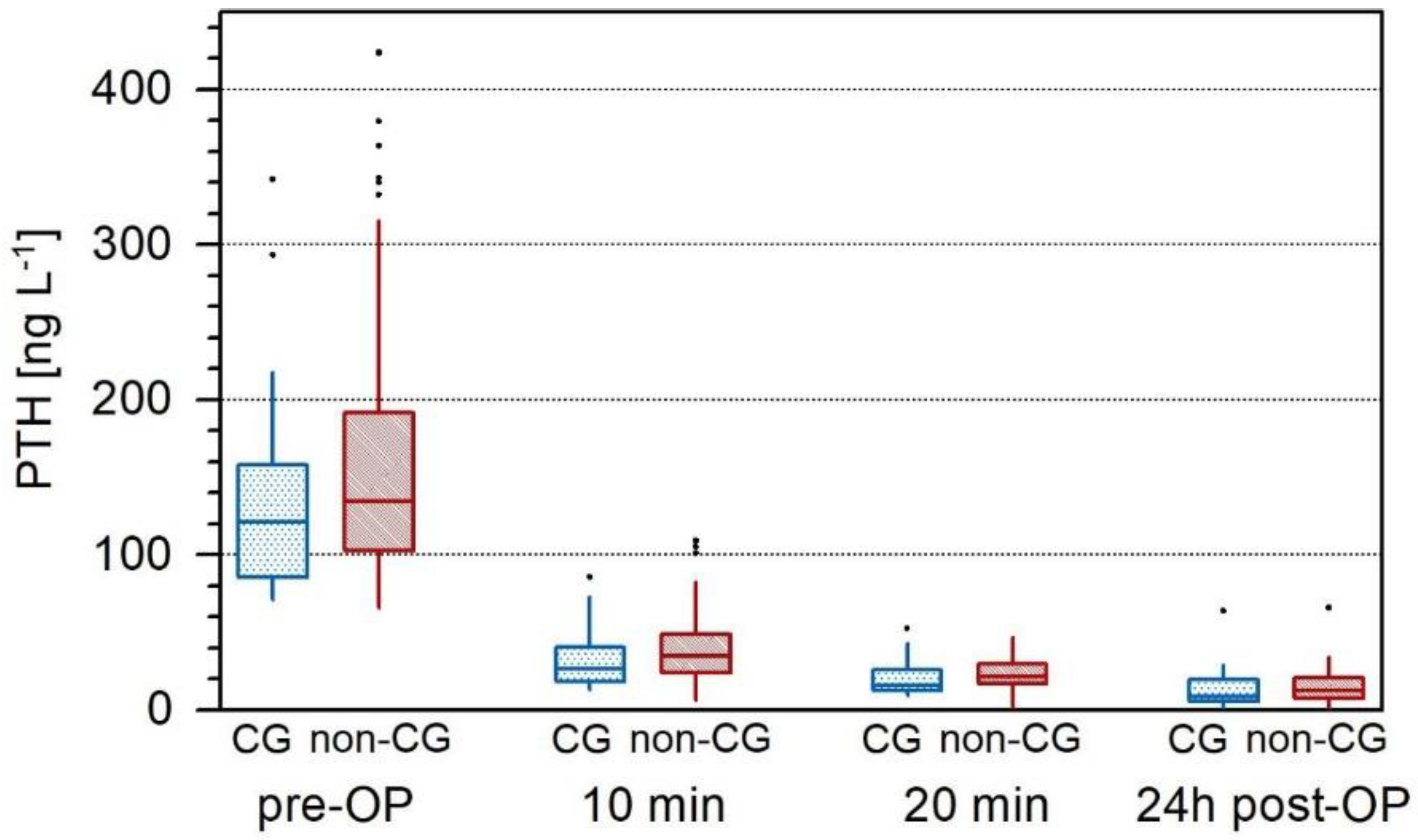
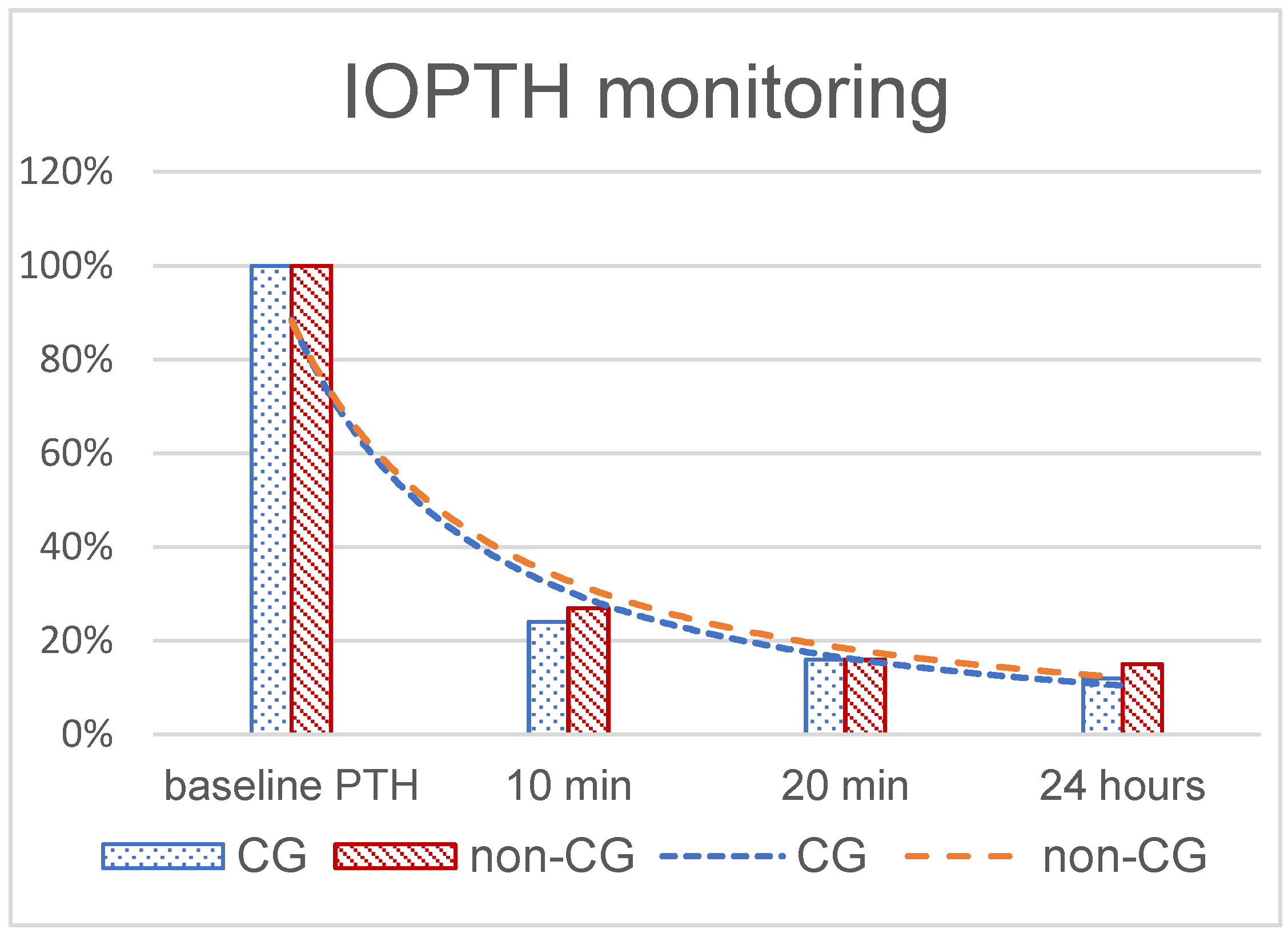
| PTH preoperative (14.5–87.1 ng/L) | 121.3(91.6–157.0) | 134.7 (103.7–188.8) | 0.282 † |
| PTH decrease of ≥50% | |||
| PTH 10 min avarage value (min–max) | 26.7 (18.6–40.0) 44.25 (12.9–85.6) | 34.7 (23.8–48.5) 57.65 (6.3–109) | 0.227 † |
| PTH 20 min | 15.9 (12.6–25.1) | 21.4 (17.1–28.8) | 0.790 † |
| PTH 24 h | 8.55 (5.55–18.3) | 12.2 (7.15–20.37) | 0.546 † |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Radulova-Mauersberger, O.; Keßler, J.; Keßler, U.; Stange, K.; Korn, S.; Weitz, J.; Bork, U. The Effect of the Frequently Used Cinacalcet for pHPT during the COVID-19 Pandemic on Perioperative Decrease in Parathyroid Hormone. J. Clin. Med. 2022, 11, 2015. https://doi.org/10.3390/jcm11072015
Radulova-Mauersberger O, Keßler J, Keßler U, Stange K, Korn S, Weitz J, Bork U. The Effect of the Frequently Used Cinacalcet for pHPT during the COVID-19 Pandemic on Perioperative Decrease in Parathyroid Hormone. Journal of Clinical Medicine. 2022; 11(7):2015. https://doi.org/10.3390/jcm11072015
Chicago/Turabian StyleRadulova-Mauersberger, Olga, Julia Keßler, Ulrich Keßler, Katrin Stange, Sandra Korn, Jürgen Weitz, and Ulrich Bork. 2022. "The Effect of the Frequently Used Cinacalcet for pHPT during the COVID-19 Pandemic on Perioperative Decrease in Parathyroid Hormone" Journal of Clinical Medicine 11, no. 7: 2015. https://doi.org/10.3390/jcm11072015
APA StyleRadulova-Mauersberger, O., Keßler, J., Keßler, U., Stange, K., Korn, S., Weitz, J., & Bork, U. (2022). The Effect of the Frequently Used Cinacalcet for pHPT during the COVID-19 Pandemic on Perioperative Decrease in Parathyroid Hormone. Journal of Clinical Medicine, 11(7), 2015. https://doi.org/10.3390/jcm11072015