
Surgical Navigation in Mandibular Reconstruction: Accuracy Evaluation of an Innovative Protocol

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Selection
2.2. Virtual Planning
2.3. 3D Model Printing and Plate Shaping
2.4. Pre-Surgical Navigation: 3D Model Registration
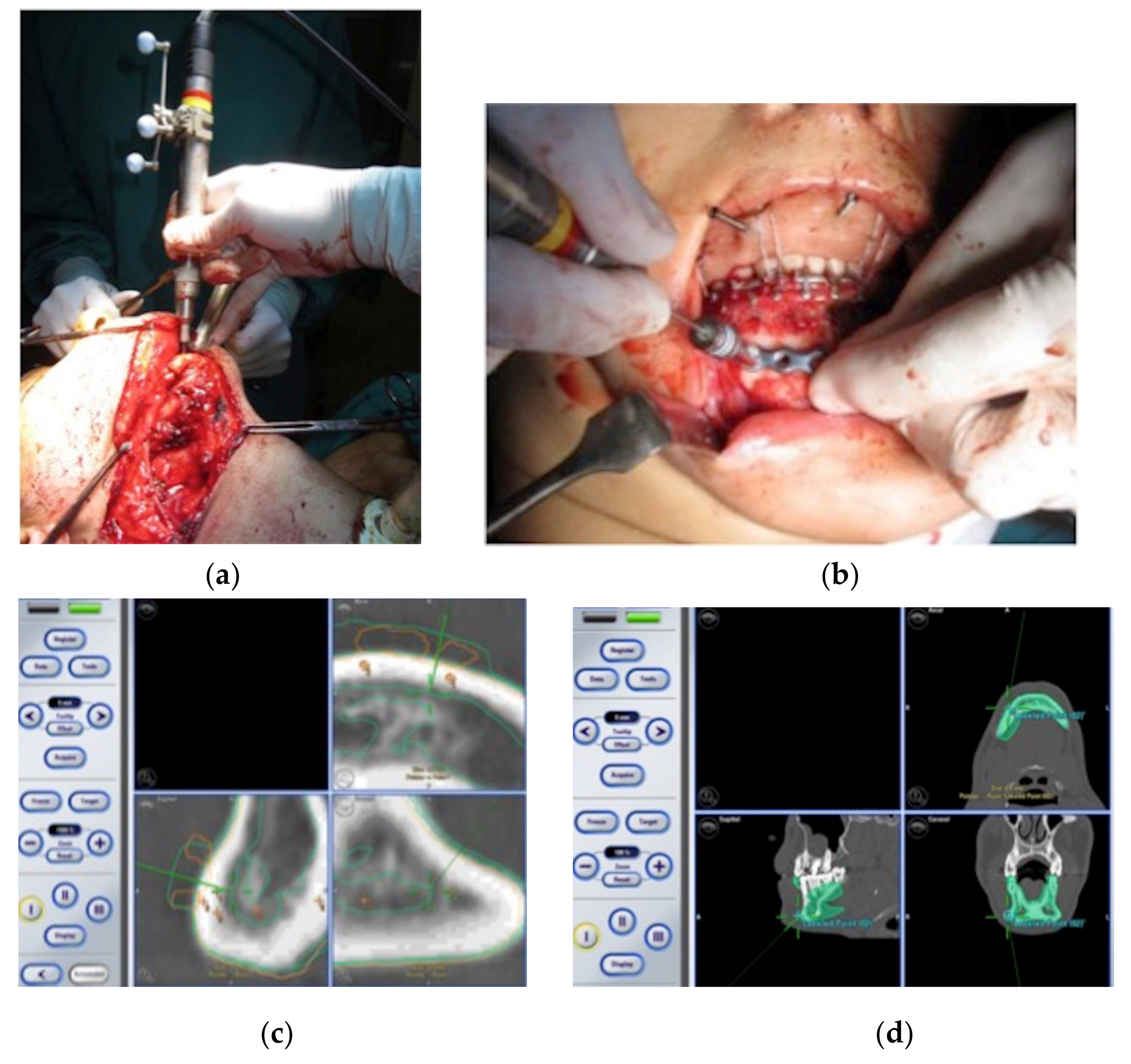
2.5. Intra-Operative Surgical Navigation
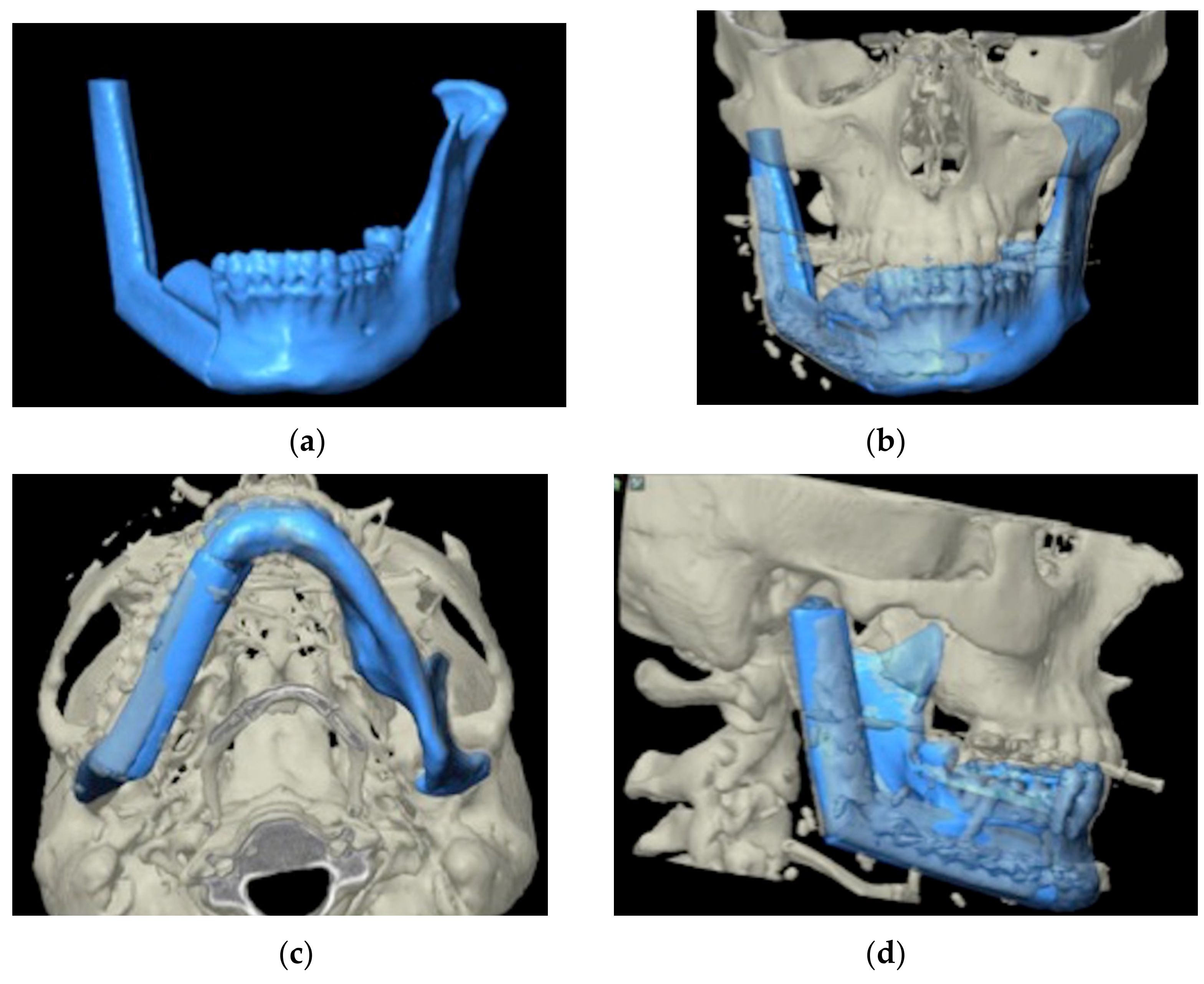
2.6. Post-Operative Evaluation
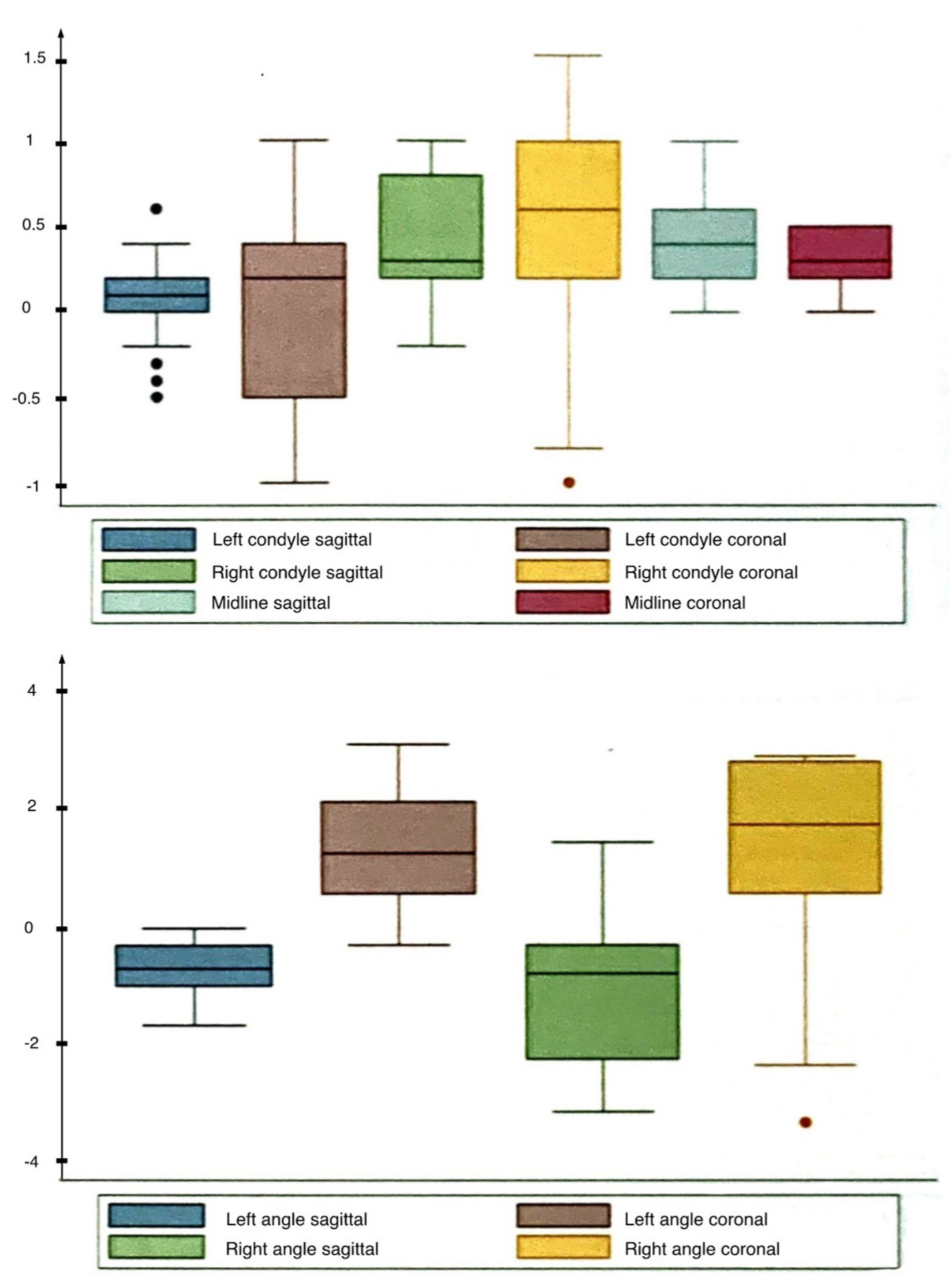
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bak, M.; Jacobson, A.S.; Buchbinder, D.; Urken, M.L. Contemporary reconstruction of the mandible. Oral Oncol. 2010, 46, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, J.J.; Zagalo, C.M.; Oliveira, M.L.; Correia, A.M.; Reis, A.R. Mandible reconstruction: History, state of the art and persistent problems. Prosthet. Orthot. Int. 2015, 39, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Schliephake, H.; Hausamen, J.E. An overview of the principles of reconstructive surgery. In Maxillofacial Surgery, 2nd ed.; Ward Booth, P., Schendel, S.A., Hausamen, J.E., Eds.; Churchill Livingtone: St. Louis, MI, USA, 2007; pp. 535–548. [Google Scholar]
- Wilik, R.M. Bony reconstruction of the jaws. In Peterson’s Principles of Oral an Maxillofacial Surgery, 2nd ed.; Miloro, M., Ed.; BC Decker: Hamilton, ON, Canada, 2004; pp. 783–801. [Google Scholar]
- Goh, B.T.; Lee, S.; Tideman, H.; Stoelinga, P.J. Mandibular reconstruction in adults: A review. Int. J. Oral Maxillofac. Surg. 2008, 37, 597–605. [Google Scholar] [CrossRef] [PubMed]
- Hidalgo, D.A. Fibula free flap: A new method of mandible reconstruction. Plast. Reconstr. Surg. 1989, 84, 71–79. [Google Scholar] [CrossRef]
- Hidalgo, D.A.; Pusic, A.L. Free-flap mandibular reconstruction: A 10-year follow-up study. Plast. Reconstr. Surg. 2002, 110, 438–449, discussion 450–451. [Google Scholar] [CrossRef]
- Yim, K.K.; Wei, F.C. Fibula osteoseptocutaneous flap for mandible reconstruction. Microsurgery 1994, 15, 245–249. [Google Scholar] [CrossRef]
- Brown, J.S.; Lowe, D.; Kanatas, A.; Schache, A. Mandibular reconstruction with vascularised bone flaps: A systematic review over 25 years. Br. J. Oral Maxillofac. Surg. 2017, 55, 113–126. [Google Scholar] [CrossRef]
- Lodders, J.N.; Leusink, F.K.J.; Ridwan-Pramana, A.; Winters, H.A.H.; Karagozoglu, K.H.; Dekker, H.; Forouzanfar, T.; Schulten, E.A.J.M. Long-term outcomes of implant-based dental rehabilitation in head and neck cancer patients after reconstruction with the free vascularized fibula flap. J. Craniomaxillofac. Surg. 2021, 49, 845–854. [Google Scholar] [CrossRef]
- Sozzi, D.; Novelli, G.; Silva, R.; Connelly, S.T.; Tartaglia, G.M. Implant rehabilitation in fibula-free flap reconstruction: A retrospective study of cases at 1–18 years following surgery. J. Craniomaxillofac. Surg. 2017, 45, 1655–1661. [Google Scholar] [CrossRef]
- Zavattero, E.; Ramieri, G.; Agrò, G.; Fasolis, M.; Garzino-Demo, P.; Borbon, C. Implant Dental Rehabilitation of Fibula-Free Flap Reconstructed Jaws. J. Craniofac. Surg. 2021, 32, e134–e136. [Google Scholar] [CrossRef]
- Kumar, V.V.; Jacob, P.C.; Ebenezer, S.; Kuriakose, M.A.; Kekatpure, V.; Baliarsing, A.S.; Al-Nawas, B.; Wagner, W. Implant supported dental rehabilitation following segmental mandibular reconstruction—Quality of life outcomes of a prospective randomized trial. J. Craniomaxillofac. Surg. 2016, 44, 800–810. [Google Scholar] [CrossRef]
- Zhang, L.; Liu, Z.; Li, B.; Yu, H.; Shen, S.G.; Wang, X. Evaluation of computer-assisted mandibular reconstruction with vascularized fibular flap compared to conventional surgery. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 121, 139–148. [Google Scholar] [CrossRef]
- Wilde, F.; Hanken, H.; Probst, F.; Schramm, A.; Heiland, M.; Cornelius, C.P. Multicenter study on the use of patient-specific CAD/CAM reconstruction plates for mandibular reconstruction. Int. J. Comput. Assist. Radiol. Surg. 2015, 10, 2035–2051. [Google Scholar] [CrossRef]
- Mascha, F.; Winter, K.; Pietzka, S.; Heufelder, M.; Schramm, A.; Wilde, F. Accuracy of computer-assisted mandibular reconstructions using patient-specific implants in combination with CAD/CAM fabricated transfer keys. J. Craniomaxillofac. Surg. 2017, 45, 1884–1897. [Google Scholar] [CrossRef]
- Succo, G.; Berrone, M.; Battiston, B.; Tos, P.; Goia, F.; Appendino, P.; Crosetti, E. Step-by-step surgical technique for mandibular reconstruction with fibular free flap: Application of digital technology in virtual surgical planning. Eur. Arch. Otorhinolaryngol. 2015, 272, 1491–1501. [Google Scholar] [CrossRef]
- Wu, J.; Sun, J.; Shen, S.G.; Xu, B.; Li, J.; Zhang, S. Computer-assisted navigation: Its role in intraoperatively accurate mandibular reconstruction. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 122, 134–142. [Google Scholar] [CrossRef]
- Abbate, V.; Orabona, G.D.A.; Solari, D.; Bonavolontà, P.; Iaconetta, G.; Califano, L. Mandibular Surgical Navigation: An Innovative Guiding Method. J. Craniofac. Surg. 2017, 28, 2122–2126. [Google Scholar] [CrossRef]
- Hohlweg-Majert, B.; Schön, R.; Schmelzeisen, R.; Gellrich, N.C.; Schramm, A. Navigational maxillofacial surgery using virtual models. World J. Surg. 2005, 29, 1530–1538. [Google Scholar] [CrossRef]
- Yu, H.; Shen, S.G.; Wang, X.; Zhang, L.; Zhang, S. The indication and application of computer-assisted navigation in oral and maxillofacial surgery-Shanghai’s experience based on 104 cases. J. Craniomaxillofac. Surg. 2013, 41, 770–774. [Google Scholar] [CrossRef]
- Roser, S.M.; Ramachandra, S.; Blair, H.; Grist, W.; Carlson, G.W.; Christensen, A.M.; Weimer, K.A.; Steed, M.B. The accuracy of virtual surgical planning in free fibula mandibular reconstruction: Comparison of planned and final results. J. Oral Maxillofac. Surg. 2010, 68, 2824–2832. [Google Scholar] [CrossRef]
- Wang, L.Y.; Du, H.M.; Zhang, G.; Tang, W.; Liu, L.; Jing, W.; Long, J. The application of digital surgical diagnosis and treatment technology: A promising strategy for surgical reconstruction of craniomaxillofacial defect and deformity. Med. Hypotheses 2011, 77, 1004–1005. [Google Scholar] [CrossRef]
- Sink, J.; Hamlar, D.; Kademani, D.; Khariwala, S.S. Computer-aided stereolithography for presurgical planning in fibula free tissue reconstruction of the mandible. J. Reconstr. Microsurg. 2012, 28, 395–403. [Google Scholar] [CrossRef]
- He, Y.; Zhu, H.G.; Zhang, Z.Y.; He, J.; Sader, R. Three-dimensional model simulation and reconstruction of composite total maxillectomy defects with fibula osteomyocutaneous flap flow-through from radial forearm flap. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 108, e6–e12. [Google Scholar] [CrossRef]
- Lyons, A.J.; James, R.; Collyer, J. Free vascularised iliac crest graft: An audit of 26 consecutive cases. Br. J. Oral Maxillofac. Surg. 2005, 43, 210–214. [Google Scholar] [CrossRef]
- Muñoz Guerra, M.F.; Gías, L.N.; Rodríguez Campo, F.J.; Díaz González, F.J. Vascularized free fibular flap for mandibular reconstruction: A report of 26 cases. J. Oral Maxillofac. Surg. 2001, 59, 140–144. [Google Scholar] [CrossRef]
- Hendra, F.N.; Van Cann, E.M.; Helder, M.N.; Ruslin, M.; de Visscher, J.G.; Forouzanfar, T.; de Vet, H.C.W. Global incidence and profile of ameloblastoma: A systematic review and meta-analysis. Oral Dis. 2020, 26, 12–21. [Google Scholar] [CrossRef]
- Moratin, J.; Horn, D.; Metzger, K.; Ristow, O.; Flechtenmacher, C.; Engel, M.; Hoffmann, J.; Freier, K.; Freudlsperger, C. Squamous cell carcinoma of the mandible—Patterns of metastasis and disease recurrence in dependence of localization and therapy. J. Craniomaxillofac. Surg. 2020, 48, 1158–1163. [Google Scholar] [CrossRef]
- Wilde, F.; Cornelius, C.P.; Schramm, A. Computer-Assisted Mandibular Reconstruction using a Patient-Specific Reconstruction Plate Fabricated with Computer-Aided Design and Manufacturing Techniques. Craniomaxillofac. Trauma Reconstr. 2014, 7, 158–166. [Google Scholar] [CrossRef]
- Wilde, F.; Winter, K.; Kletsch, K.; Lorenz, K.; Schramm, A. Mandible reconstruction using patient-specific pre-bent reconstruction plates: Comparison of standard and transfer key methods. Int. J. Comput. Assist. Radiol. Surg. 2015, 10, 129–140. [Google Scholar] [CrossRef]
- Zhang, W.B.; Yu, Y.; Wang, Y.; Mao, C.; Liu, X.J.; Guo, C.B.; Yu, G.Y.; Peng, X. Improving the accuracy of mandibular reconstruction with vascularized iliac crest flap: Role of computer-assisted techniques. J. Craniomaxillofac. Surg. 2016, 44, 1819–1827. [Google Scholar] [CrossRef] [PubMed]
- Hassfeld, S.; Mühling, J.; Zöller, J. Intraoperative navigation in oral and maxillofacial surgery. Int. J. Oral Maxillofac. Surg. 1995, 24 Pt 2, 111–119, (In English and German). [Google Scholar] [CrossRef]
- Hassfeld, S.; Mühling, J. Computer assisted oral and maxillofacial surgery--a review and an assessment of technology. Int. J. Oral Maxillofac. Surg. 2001, 30, 2–13. [Google Scholar] [CrossRef] [PubMed]
- Austin, R.E.; Antonyshyn, O.M. Current applications of 3-d intraoperative navigation in craniomaxillofacial surgery: A retrospective clinical review. Ann. Plast. Surg. 2012, 69, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Bell, R.B. Computer planning and intraoperative navigation in cranio-maxillofacial surgery. Oral Maxillofac. Surg. Clin. N. Am. 2010, 22, 135–156. [Google Scholar] [CrossRef]
- Yu, H.; Shen, G.; Wang, X.; Zhang, S. Navigation-guided reduction and orbital floor reconstruction in the treatment of zygomatic-orbital-maxillary complex fractures. J. Oral Maxillofac. Surg. 2010, 68, 28–34. [Google Scholar] [CrossRef]
- Novelli, G.; Tonellini, G.; Mazzoleni, F.; Sozzi, D.; Bozzetti, A. Surgical navigation recording systems in orbitozygomatic traumatology. J. Craniofac. Surg. 2012, 23, 890–892. [Google Scholar] [CrossRef]
- Novelli, G.; Tonellini, G.; Mazzoleni, F.; Bozzetti, A.; Sozzi, D. Virtual surgery simulation in orbital wall reconstruction: Integration of surgical navigation and stereolithographic models. J. Craniomaxillofac. Surg. 2014, 42, 2025–2034. [Google Scholar] [CrossRef]
- Novelli, G.; Gramegna, M.; Tonellini, G.; Valente, G.; Boni, P.; Bozzetti, A.; Sozzi, D. Orbital Osteoblastoma: Technical Innovations in Resection and Reconstruction Using Virtual Surgery Simulation. Craniomaxillofac. Trauma Reconstr. 2016, 9, 271–276. [Google Scholar] [CrossRef]
- Bell, R.B.; Weimer, K.A.; Dierks, E.J.; Buehler, M.; Lubek, J.E. Computer planning and intraoperative navigation for palatomaxillary and mandibular reconstruction with fibular free flaps. J. Oral Maxillofac. Surg. 2011, 69, 724–732. [Google Scholar] [CrossRef]
- Shan, X.F.; Chen, H.M.; Liang, J.; Huang, J.W.; Zhang, L.; Cai, Z.G.; Guo, C. Surgical navigation-assisted mandibular reconstruction with fibula flaps. Int. J. Oral Maxillofac. Surg. 2016, 45, 448–453. [Google Scholar] [CrossRef]
- Heiland, M.; Habermann, C.R.; Schmelzle, R. Indications and limitations of intraoperative navigation in maxillofacial surgery. J. Oral Maxillofac. Surg. 2004, 62, 1059–1063. [Google Scholar] [CrossRef]
- Casap, N.; Wexler, A.; Eliashar, R. Computerized navigation for surgery of the lower jaw: Comparison of 2 navigation systems. J. Oral Maxillofac. Surg. 2008, 66, 1467–1475. [Google Scholar] [CrossRef]
- Widmann, G.; Keiler, M.; Zangerl, A.; Stoffner, R.; Longato, S.; Bale, R.; Puelacher, W. Computer-assisted surgery in the edentulous jaw based on 3 fixed intraoral reference points. J. Oral Maxillofac. Surg. 2010, 68, 1140–1147. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MARKERPOINTS | MEAN ± SD (Range) | MEDIAN (95%CI) |
|---|---|---|
| Left condyle sagittal (mm) | 0.07 ± 0.28 (−0.5; 0.6) | 0.1 (0.0:0.2) |
| Left condyle coronal (mm) | 0.06 ± 0.58 (−1.0; 1.0) | 0.2 (−0.5; 0.4) |
| Right condyle sagittal (mm) | 0.4 ± 0.38 (−0.2; 1.0) | 0.3 ± (0.2; 0.7) |
| Right condyle coronal (mm) | 0.43 ± 0.68 (−1.0; 1.5) | 0.6 (0.2; 1.0) |
| Midline sagittal (mm) | 0.45 ± 0.30 (0.0; 1.0) | 0.4 (0.2; 0.6) |
| Midline coronal (mm) | 0.29 ± 0.17 (0.0; 0.5) | 0.3 (0.2; 0.5) |
| Left angle sagittal (mm) | −0.7 ± 0.48 (−1.7; 0.0) | −0.7 (−1.0; −0.3) |
| Left angle coronal (mm) | 1.46 ± 1.02 (−0.3; 3.2) | 1.3 (0.6; 2.1) |
| Right angle sagittal (mm) | −1.07 ± 1.42 (−3.2; 1.5) | −0.8 (−2.2; −0.3) |
| Right angle coronal (mm) | 1.36 ± 1.73 (−3.4; 3.0) | 1.8 (0.7; 2.8) |
| MARKERPOINTS | LEFT (n = 7) Mean ± SD (Range) Median (95% CI) | RIGHT (n = 14) Mean ± SD (Range) Median (95% CI) | p Value Student’s t-Test * Wilcoxon Sum Rank Test |
|---|---|---|---|
| Left condyle sagittal (mm) | 0.23 ± 0.21 0.2 (−0.1; 0.4) | −0.01 ± 0.29 0.0 (−0.3; 0.2) | 0.030 |
| Left condyle coronal (mm) | 0.01 ± 0.51 0.2 (−0.3; 0.4) | 0.08 ± 0.63 0.2 (−0.5; 0.7) | 0.409 |
| Right condyle sagittal (mm) | 0.63 ± 0.28 0.6 (0.3; 0.9) | 0.28 ± 0.38 0.3 (−0.1; 0.5) | 0.022 |
| Right condyle coronal (mm) | 0.53 ± 0.68 0.8 (0.2; 1.0) | 0.39 ± 0.70 0.5 (−0.3; 1.0) | 0.332 |
| Midline sagittal (mm) | 0.43 ± 0.41 0.3 (0.1; 1.0) | 0.46 ± 0.25 0.4 (0.2; 0.6) | 0.404 |
| Midline coronal (mm) | 0.30 ± 0.18 0.3 (0.2; 0.5) | 0.29 ± 0.17 0.3 (0.1; 0.5) | 0.432 |
| Left angle sagittal (mm) | −1.21 ± 0.31 −1.2 (−1.5; −0.9) | −0.44 ± 0.31 −0.3 (−0.7; −0.2) | <0.0001 |
| Left angle coronal (mm) | 2.29 ± 1.19 2.6 (2.2; 3.0) | 1.04 ± 0.62 1.1 (0.5; 1.5) | 0.002 |
| Right angle sagittal (mm) | −0.44 ± 0.35 −0.5 (−0.8; −0.3) | −1.39 ± 1.65 −1.8 (−2.9; −0.1) | 0.078 |
| Right angle coronal (mm) | 0.77 ± 0.62 0.6 (0.4; 1.2) | 1.65 ± 2.04 2.4 (1.5; 2.9) | 0.023 * |
| MARKERPOINTS | LEFT (n = 7) Mean ± SD | p Value Student’s t-Test |
|---|---|---|
| Left condyle sagittal (mm) | 0.23 ± 0.21 | 0.026 |
| Left condyle coronal (mm) | 0.01 ± 0.51 | 0.943 |
| Right condyle sagittal (mm) | 0.63 ± 0.28 | 0.001 |
| Right condyle coronal (mm) | 0.53 ± 0.68 | 0.086 |
| Midline sagittal (mm) | 0.43 ± 0.41 | 0.033 |
| Midline coronal (mm) | 0.30 ± 0.18 | 0.005 |
| Left angle sagittal (mm) | −1.21 ± 0.31 | <0.0001 |
| Left angle coronal (mm) | 2.29 ± 1.19 | 0.002 |
| Right angle sagittal (mm) | −0.44 ± 0.35 | 0.016 |
| Right angle coronal (mm) | 0.77 ± 0.62 | 0.016 |
| MARKERPOINTS | RIGHT (n = 14) Mean ± SD | p Value Student’s t-Test |
|---|---|---|
| Left condyle sagittal (mm) | −0.01 ± 0.29 | 0.854 |
| Left condyle coronal (mm) | 0.08 ± 0.63 | 0.648 |
| Right condyle sagittal (mm) | 0.28 ± 0.38 | 0.016 |
| Right condyle coronal (mm) | 0.39 ± 0.70 | 0.061 |
| Midline sagittal (mm) | 0.46 ± 0.25 | <0.0001 |
| Midline coronal (mm) | 0.29 ± 0.17 | <0.0001 |
| Left angle sagittal (mm) | −0.44 ± 0.31 | <0.0001 |
| Left angle coronal (mm) | 1.04 ± 0.62 | <0.0001 |
| Right angle sagittal (mm) | −1.39 ± 1.65 | 0.008 |
| Right angle coronal (mm) | 1.65 ± 2.04 | 0.010 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sozzi, D.; Filippi, A.; Canzi, G.; De Ponti, E.; Bozzetti, A.; Novelli, G. Surgical Navigation in Mandibular Reconstruction: Accuracy Evaluation of an Innovative Protocol. J. Clin. Med. 2022, 11, 2060. https://doi.org/10.3390/jcm11072060
Sozzi D, Filippi A, Canzi G, De Ponti E, Bozzetti A, Novelli G. Surgical Navigation in Mandibular Reconstruction: Accuracy Evaluation of an Innovative Protocol. Journal of Clinical Medicine. 2022; 11(7):2060. https://doi.org/10.3390/jcm11072060
Chicago/Turabian StyleSozzi, Davide, Andrea Filippi, Gabriele Canzi, Elena De Ponti, Alberto Bozzetti, and Giorgio Novelli. 2022. "Surgical Navigation in Mandibular Reconstruction: Accuracy Evaluation of an Innovative Protocol" Journal of Clinical Medicine 11, no. 7: 2060. https://doi.org/10.3390/jcm11072060
APA StyleSozzi, D., Filippi, A., Canzi, G., De Ponti, E., Bozzetti, A., & Novelli, G. (2022). Surgical Navigation in Mandibular Reconstruction: Accuracy Evaluation of an Innovative Protocol. Journal of Clinical Medicine, 11(7), 2060. https://doi.org/10.3390/jcm11072060