
Histological Comparison of Buccal and Lingual Mucosa Grafts for Urethroplasty: Do They Share Tissue Structures and Vascular Supply?

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Protocol and Patient Selection
2.2. Surgical Technique
2.2.1. Buccal Mucosa Graft Harvesting
2.2.2. Lingual Mucosa Graft Harvesting
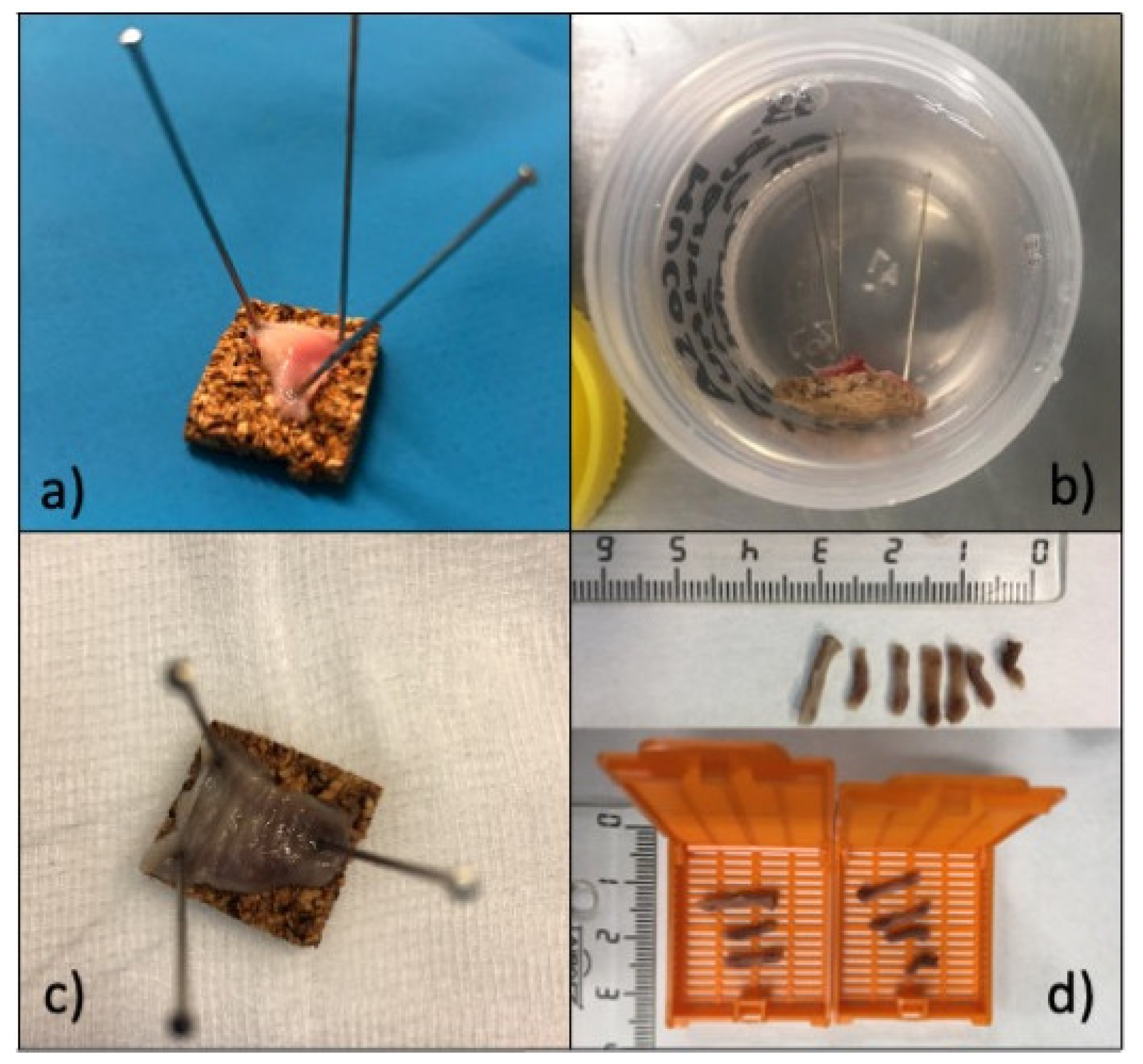
2.2.3. Graft Preparation, Sample Procurement, and Histological Analysis
2.3. Clinical Information
Clinical Information, Data Storage and Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lumen, N.; Campos-Juanatey, F.; Greenwell, T.; Martins, F.E.; Osman, N.I.; Riechardt, S.; Waterloos, M.; Barratt, R.; Chan, G.; Esperto, F.; et al. European Association of Urology Guidelines on Urethral Stricture Disease (Part 1): Management of Male Urethral Stricture Disease. Eur. Urol. 2021, 80, 190–200. [Google Scholar] [CrossRef] [PubMed]
- Wessells, H.; Angermeier, K.W.; Elliott, S.; Gonzalez, C.M.; Kodama, R.; Peterson, A.C.; Reston, J.; Rourke, K.; Stoffel, J.; Vanni, A.J.; et al. Male Urethral Stricture: American Urological Association Guideline. J. Urol. 2017, 197, 182–190. [Google Scholar] [CrossRef] [PubMed]
- Burger, R.A.; Muller, S.C.; el-Damanhoury, H.; Tschakaloff, A.; Riedmiller, H.; Hohenfellner, R. The buccal mucosal graft for urethral reconstruction: A preliminary report. J. Urol. 1992, 147, 662–664. [Google Scholar] [CrossRef]
- Wang, A.; Chua, M.; Talla, V.; Fernandez, N.; Ming, J.; Sarino, E.M.; DeLong, J.; Virasoro, R.; Tonkin, J.; McCammon, K. Lingual versus buccal mucosal graft for augmentation urethroplasty: A meta-analysis of surgical outcomes and patient-reported donor site morbidity. Int. Urol. Nephrol. 2021, 53, 907–918. [Google Scholar] [CrossRef]
- Kamp, S.; Knoll, T.; Osman, M.; Hacker, A.; Michel, M.S.; Alken, P. Donor-site morbidity in buccal mucosa urethroplasty: Lower lip or inner cheek? BJU Int. 2005, 96, 619–623. [Google Scholar] [CrossRef]
- Song, L.J.; Xu, Y.M.; Lazzeri, M.; Barbagli, G. Lingual mucosal grafts for anterior urethroplasty: A review. BJU Int. 2009, 104, 1052–1056. [Google Scholar] [CrossRef]
- Filipas, D.; Fisch, M.; Fichtner, J.; Fitzpatrick, J.; Berg, K.; Störkel, S.; Hohenfellner, R.; Thüroff, J.W. The histology and immunohistochemistry of free buccal mucosa and full-skin grafts after exposure to urine. BJU Int. 1999, 84, 108–111. [Google Scholar] [CrossRef]
- El-Sherbiny, M.T.; Abol-Enein, H.; Dawaba, M.S.; Ghoneim, M.A. Treatment of urethral defects: Skin, buccal or bladder mucosa, tube or patch? An experimental study in dogs. J. Urol. 2002, 167, 2225–2228. [Google Scholar] [CrossRef]
- Cavalcanti, A.G.; Restrepo, C.F.; Simões, M.; Costa, W.S.; Sampaio, F.J.B.; de Souza, D.B. What Is the Best Way to Prepare A Buccal Mucosa Graft for Urethroplasty? A Histology-Based Preliminary Report. Urol. Int. 2018, 100, 397–401. [Google Scholar] [CrossRef]
- Humby, G.; Higgins, T.T. A one-stage operation for hypospadias. Br. J. Surg. 1941, 29, 84–92. [Google Scholar] [CrossRef]
- Dessanti, A.; Rigamonti, W.; Merulla, V.; Falchetti, D.; Caccia, G. Autologous buccal mucosa graft for hypospadias repair: An initial report. J. Urol. 1992, 147, 1081–1083. [Google Scholar] [CrossRef]
- Barbagli, G.; Fossati, N.; Sansalone, S.; Larcher, A.; Romano, G.; Dell’Acqua, V.; Guazzoni, G.F.; Lazzeri, M. Prediction of early and late complications after oral mucosal graft harvesting: Multivariable analysis from a cohort of 553 consecutive patients. J. Urol. 2014, 191, 688–693. [Google Scholar] [CrossRef] [PubMed]
- O’Riordan, A.; Narahari, R.; Kumar, V.; Pickard, R. Outcome of dorsal buccal graft urethroplasty for recurrent bulbar urethral strictures. BJU Int. 2008, 102, 1148–1151. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, J.; Kaviani, A.; Hosseini, M.; Mazloomfard, M.M.; Razi, A. Dorsal versus ventral oral mucosal graft urethroplasty. Urol. J. 2011, 8, 48–53. [Google Scholar] [PubMed]
- Spilotros, M.; Sihra, N.; Malde, S.; Pakzad, M.H.; Hamid, R.; Ockrim, J.L.; Greenwell, T.J. Buccal mucosal graft urethroplasty in men-risk factors for recurrence and complications: A third referral centre experience in anterior urethroplasty using buccal mucosal graft. Transl. Androl. Urol. 2017, 6, 510–516. [Google Scholar] [CrossRef] [Green Version]
- Esperto, F.; Verla, W.; Ploumidis, A.; Barratt, R.; La Rocca, R.; Lumen, N.; Yuan, Y.; Campos-Juanatey, F.; Greenwell, T.; Martins, F.; et al. What is the role of single-stage oral mucosa graft urethroplasty in the surgical management of lichen sclerosus-related stricture disease in men? A systematic review. World J. Urol. 2021, 40, 393–408. [Google Scholar] [CrossRef]
- Kulkarni, S.; Barbagli, G.; Sansalone, S.; Lazzeri, M. One-sided anterior urethroplasty: A new dorsal onlay graft technique. BJU Int. 2009, 104, 1150–1155. [Google Scholar] [CrossRef]
- Simonato, A.; Gregori, A.; Lissiani, A.; Galli, S.; Ottaviani, F.; Rossi, R.; Zappone, A.; Carmignani, G. The tongue as an alternative donor site for graft urethroplasty: A pilot study. J. Urol. 2006, 175, 589–592. [Google Scholar] [CrossRef]
- Abrate, A.; Gregori, A.; Simonato, A. Lingual mucosal graft urethroplasty 12 years later: Systematic review and meta-analysis. Asian J. Urol. 2019, 6, 230–241. [Google Scholar] [CrossRef]
- Guerrerosantos, J.; Dicksheet, S.; Ruiz-Razura, A. Free tongue composite graft for correction of a vermilion defect. Plast. Reconstr. Surg. 1985, 76, 451–454. [Google Scholar] [CrossRef]
- Simonato, A.; Gregori, A.; Ambruosi, C.; Venzano, F.; Varca, V.; Romagnoli, A.; Carmignani, G. Lingual mucosal graft urethroplasty for anterior urethral reconstruction. Eur. Urol. 2008, 54, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Barbagli, G.; De Angelis, M.; Romano, G.; Ciabatti, P.G.; Lazzeri, M. The use of lingual mucosal graft in adult anterior urethroplasty: Surgical steps and short-term outcome. Eur. Urol. 2008, 54, 671–676. [Google Scholar] [CrossRef] [PubMed]
- Das, S.K.; Kumar, A.; Sharma, G.K.; Pandey, A.K.; Bansal, H.; Trivedi, S.; Dwivedi, U.S.; Bhattacharya, V.; Singh, P.B. Lingual mucosal graft urethroplasty for anterior urethral strictures. Urology 2009, 73, 105–108. [Google Scholar] [CrossRef]
- Sharma, G.K.; Pandey, A.; Bansal, H.; Swain, S.; Das, S.K.; Trivedi, S.; Dwivedi, U.S.; Singh, P.B. Dorsal onlay lingual mucosal graft urethroplasty for urethral strictures in women. BJU Int. 2010, 105, 1309–1312. [Google Scholar] [CrossRef]
- Xu, Y.-M.; Li, C.; Xie, H.; Sa, Y.-L.; Fu, Q.; Wu, D.-L.; Zhang, J.; Feng, C.; Jin, C.-R.; Song, L.-J.; et al. Intermediate-Term Outcomes and Complications of Long Segment Urethroplasty with Lingual Mucosa Grafts. J. Urol. 2017, 198, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Campos-Juanatey, F.; Bugeja, S.; Dragova, M.; Frost, A.V.; Ivaz, S.L.; Andrich, D.E.; Mundy, A.R. Single-stage tubular urethral reconstruction using oral grafts is an alternative to classical staged approach for selected penile urethral strictures. Asian J. Androl. 2020, 22, 134–139. [Google Scholar] [PubMed]
- Sharma, A.K.; Chandrashekar, R.; Keshavamurthy, R.; Nelvigi, G.G.; Kamath, A.J.; Sharma, S.; Venkatesh, G. Lingual versus buccal mucosa graft urethroplasty for anterior urethral stricture: A prospective comparative analysis. Int. J. Urol. 2013, 20, 1199–1203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, A.; Das, S.K.; Trivedi, S.; Dwivedi, U.S.; Singh, P.B. Substitution urethroplasty for anterior urethral strictures: Buccal versus lingual mucosal graft. Urol. Int. 2010, 84, 78–83. [Google Scholar] [CrossRef]
- Maarouf, A.M.; Elsayed, E.R.; Ragab, A.; Salem, E.; Sakr, A.M.N.; Omran, M.; Abdelmonem, I.I.; Khalil, S.A.S.; Abdalsamad, K.; Abouhashem, S.; et al. Buccal versus lingual mucosal graft urethroplasty for complex hypospadias repair. J. Pediatr. Urol. 2013, 9, 754–758. [Google Scholar] [CrossRef]
- Lumen, N.; Vierstraete-Verlinde, S.; Oosterlinck, W.; Hoebeke, P.; Palminteri, E.; Goes, C.; Maes, H.; Spinoit, A. Buccal Versus Lingual Mucosa Graft in Anterior Urethroplasty: A Prospective Comparison of Surgical Outcome and Donor Site Morbidity. J. Urol. 2016, 195, 112–117. [Google Scholar] [CrossRef]
- Pal, D.K.; Gupta, D.K.; Ghosh, B.; Bera, M.K. A comparative study of lingual mucosal graft urethroplasty with buccal mucosal graft urethroplasty in urethral stricture disease: An institutional experience. Urol. Ann. 2016, 8, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Wang, T.; Cao, S.; Song, L.; Hu, X.; Zhang, J.; Xu, Y.; Fu, Q. Multi-Factorial Analysis of Recurrence and Complications of Lingual Mucosa Graft Urethroplasty for Anterior Urethral Stricture: Experience from a Chinese Referral Center. Urology 2021, 152, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Markiewicz, M.R.; Margarone, J.E.; Barbagli, G.; Scannapieco, F.A. Oral Mucosa Harvest: An Overview of Anatomic and Biologic Considerations. EAU-EBU Update Ser. 2007, 5, 179–187. [Google Scholar] [CrossRef]
- Duckett, J.W.; Coplen, D.; Ewalt, D.; Baskin, L.S. Buccal mucosal urethral replacement. J. Urol. 1995, 153, 1660–1663. [Google Scholar] [CrossRef]
- Levy, M.E.; Elliott, S.P. Graft Use in Bulbar Urethroplasty. Urol. Clin. N. Am. 2017, 44, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Mokhless, I.A.; Kader, M.A.; Fahmy, N.; Youssef, M. The multistage use of buccal mucosa grafts for complex hypospadias: Histological changes. J. Urol. 2007, 177, 1496–1499. [Google Scholar] [CrossRef]
- Soave, A.; Steurer, S.; Dahlem, R.; Rink, M.; Reiss, P.; Fisch, M.; Engel, O. Histopathological characteristics of buccal mucosa transplants in humans after engraftment to the urethra: A prospective study. J. Urol. 2014, 192, 1725–1729. [Google Scholar] [CrossRef]
- Souza, G.F.; Calado, A.A.; Delcelo, R.; Ortiz, V.; Macedo, A., Jr. Histopathological evaluation of urethroplasty with dorsal buccal mucosa: An experimental study in rabbits. Int. Braz. J. Urol. 2008, 34, 345–351. [Google Scholar] [CrossRef] [Green Version]
- Song, L.J.; Xu, Y.M.; Hu, X.Y.; Zhang, H.Z. Urethral substitution using autologous lingual mucosal grafts: An experimental study. BJU Int. 2008, 101, 739–743. [Google Scholar] [CrossRef]
- Vandana, K.L.; Savitha, B. Thickness of gingiva in association with age, gender and dental arch location. J. Clin. Periodontol. 2005, 32, 828–830. [Google Scholar] [CrossRef]
- Kurtzman, J.T.; Sukumar, S.; Pan, S.-M.; Mendonca, S.; Lai, Y.; Pagan, C.A.; Brandes, S.B. The Impact of Preoperative Oral Health on Buccal Mucosa Graft Histology. J. Urol. 2021, 206, 655–661. [Google Scholar] [CrossRef] [PubMed]
- Massimo, C.; Simona, N.G.; Barbara, T.; Elisa, C.; Luisa, F.; Alessandro, G.; Donatella, P.; Teruzzi, E.; Falcone, M.; Omidreza, S.; et al. Squamous Cell Carcinoma Developing in a Buccal Mucosa Graft after Urethroplasty: A Report of 2 Cases of Malignant Degeneration. Case Rep. Urol. 2021, 2021, 5569373. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables, Units | Global | BMG | LMG | p |
|---|---|---|---|---|
| Age, years (median, IQR) | 56 (44.1–66.8) | 57.7 (50.7–74.9) | 54.9 (41.5–66.7) | 0.320 |
| Length, cm (median, IQR) | 5.5 (4.5–7) | 5 (4.5–5.5) | 7 (6.5–8) | 0.000 |
| Width, cm (median, IQR) | 1.5 (1.5–2) | 2 (1.5–2) | 1.5 (1.5–1.5) | 0.000 |
| Total thickness, µm (median, IQR) | 1598.9 (1200–2100) | 1692.8 (1382.4–2194.8) | 1347 (1005.7–1650) | 0.1 |
| Epithelium thickness, µm (mean, SD) | 510.2 (223.7) | 576.8 (234.3) | 415.2 (171.5) | 0.009 |
| Submucosal thickness, µm (median, IQR) | 654 (378.6–943.3) | 823.6 (470.4–1026.2) | 438 (267.6–654) | 0.005 |
| Muscular thickness, µm (median, IQR) | 477.6 (286.8–772.5) | 324.5 (205.5–483) | 572.5 (483.2–878) | 0.003 |
| Vascular area, % (median, IQR) | 5 (5–10) | 5 (5–10) | 5 (2–10) | 0.231 |
| Vascular density, nº plexus/mm2 (median, IQR) | 5 (2–7) | 4 (3–7) | 3 (2–6) | 0.297 |
| Adipose tissue, % (median, IQR) | 5 (0–20) | 10 (2–40) | 2 (0–10) | 0.018 |
| Cavalcanti-Group 2- | Present Series-BMG- | |
|---|---|---|
| Graft thickness, µm | Mean 1830 (SD 520) | Median 1692.8 (IQR 1382.4–2194.8) |
| Epithelium, µm (mean) | 530 (SD 160) | 576.8 (SD 234.3) |
| Subepithelial layer, µm | Mean 1220 (SD 580) | Median 823.6 (IQR 470.4–1026.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campos-Juanatey, F.; Azueta Etxebarria, A.; Calleja Hermosa, P.; Marcos Gonzalez, S.; Alonso Mediavilla, E.; Correas Gomez, M.A.; Portillo Martin, J.A.; Gutierrrez Baños, J.L. Histological Comparison of Buccal and Lingual Mucosa Grafts for Urethroplasty: Do They Share Tissue Structures and Vascular Supply? J. Clin. Med. 2022, 11, 2064. https://doi.org/10.3390/jcm11072064
Campos-Juanatey F, Azueta Etxebarria A, Calleja Hermosa P, Marcos Gonzalez S, Alonso Mediavilla E, Correas Gomez MA, Portillo Martin JA, Gutierrrez Baños JL. Histological Comparison of Buccal and Lingual Mucosa Grafts for Urethroplasty: Do They Share Tissue Structures and Vascular Supply? Journal of Clinical Medicine. 2022; 11(7):2064. https://doi.org/10.3390/jcm11072064
Chicago/Turabian StyleCampos-Juanatey, Felix, Ainara Azueta Etxebarria, Paola Calleja Hermosa, Sara Marcos Gonzalez, Eneko Alonso Mediavilla, Miguel Angel Correas Gomez, Jose Antonio Portillo Martin, and Jose Luis Gutierrrez Baños. 2022. "Histological Comparison of Buccal and Lingual Mucosa Grafts for Urethroplasty: Do They Share Tissue Structures and Vascular Supply?" Journal of Clinical Medicine 11, no. 7: 2064. https://doi.org/10.3390/jcm11072064
APA StyleCampos-Juanatey, F., Azueta Etxebarria, A., Calleja Hermosa, P., Marcos Gonzalez, S., Alonso Mediavilla, E., Correas Gomez, M. A., Portillo Martin, J. A., & Gutierrrez Baños, J. L. (2022). Histological Comparison of Buccal and Lingual Mucosa Grafts for Urethroplasty: Do They Share Tissue Structures and Vascular Supply? Journal of Clinical Medicine, 11(7), 2064. https://doi.org/10.3390/jcm11072064