
A Natural History of Erectile Dysfunction in Elderly Men: A Population-Based, Twelve-Year Prospective Study



Abstract
:1. Purpose
2. Introduction
3. Materials and Methods
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Shabsigh, R.; Perelman, M.A.; Lockhart, D.C.; Lue, T.F.; Broderick, G.A. Health issues of men: Prevalence and correlates of erectile dysfunction. J. Urol. 2005, 174, 662–667. [Google Scholar] [CrossRef]
- Dong, J.Y.; Zhang, Y.H.; Qin, L.Q. Erectile dysfunction and risk of cardiovascular disease: Meta-analysis of prospective cohort studies. J. Am. Coll. Cardiol. 2011, 58, 1378–1385. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.Y.; Huang, W.; Zhang, Y. Relation between hypertension and erectile dysfunction: A meta-analysis of cross-section studies. Int. J. Impot. Res. 2018, 30, 141–146. [Google Scholar] [CrossRef]
- Kouidrat, Y.; Pizzol, D.; Cosco, T.; Thompson, T.; Carnaghi, M.; Bertoldo, A.; Solmi, M.; Stubbs, B.; Veronese, N. High prevalence of erectile dysfunction in diabetes: A systematic review and meta-analysis of 145 studies. Diabet. Med. 2017, 34, 1185–1192. [Google Scholar] [CrossRef]
- Araujo, A.B.; Durante, R.; Feldman, H.A.; Goldstein, I.; McKinlay, J.B. The relationship between depressive symptoms and male erectile dysfunction: Cross-sectional results from the Massachusetts Male Aging Study. Psychosom. Med. 1998, 60, 458–465. [Google Scholar] [CrossRef]
- Corona, G.; Rastrelli, G.; Filippi, S.; Vignozzi, L.; Mannucci, E.; Maggi, M. Erectile dysfunction and central obesity: An Italian perspective. Asian J. Androl. 2014, 16, 581–591. [Google Scholar]
- Wei, M.; Macera, C.A.; Davis, D.R.; Hornung, C.A.; Nankin, H.R.; Blair, S.N. Total cholesterol and high density lipoprotein cholesterol as important predictors of erectile dysfunction. Am. J. Epidemiol. 1994, 140, 930–937. [Google Scholar] [CrossRef]
- Ludwig, W.; Phillips, M. Organic causes of erectile dysfunction in men under. Urol. Int. 2014, 92, 1–6. [Google Scholar] [CrossRef]
- Janiszewski, P.M.; Janssen, I.; Ross, R. Abdominal obesity and physical inactivity are associated with erectile dysfunction independent of body mass index. J. Sex. Med. 2009, 6, 1990–1998. [Google Scholar] [CrossRef]
- Chen, L.; Shi, G.-R.; Huang, D.-D.; Li, Y.; Ma, C.-C.; Shi, M.; Su, B.-X. Male sexual dysfunction: A review of literature on its pathological mechanisms, potential risk factors, and herbal drug intervention. Biomed. Pharmacother. 2019, 112, 108585. [Google Scholar] [CrossRef]
- Schouten, B.W.V.; Bosch, J.L.H.R.; Bernsen, R.M.D. Incidence rates of erectile dysfunction in the Dutch general population. Effects of definition, clinical relevance and duration of follow-up in the Krimpen Study. Int. J. Impot. Res. 2005, 17, 58–62. [Google Scholar] [CrossRef]
- Travison, T.G.; Sand, M.S.; Rosen, R.C.; Shabsigh, R.; Eardley, I.; McKinlay, J.B. The natural progression and regression of erectile dysfunction: Follow-up results from the MMAS and MALES studies. J. Sex. Med. 2011, 8, 1917–1924. [Google Scholar] [CrossRef]
- Travison, T.G.; Shabsigh, R.; Araujo, A.B.; Kupelian, V.; O’Donnell, A.B.; McKinlay, J.B. The natural progression and remission of erectile dysfunction: Results from the Massachusetts male aging study. J. Urol. 2007, 177, 241–246. [Google Scholar] [CrossRef]
- McCulloch, D.K.; Young, R.J.; Prescott, R.J.; Campbell, I.W.; Clarke, B.F. The natural history of impotence in diabetic men. Diabetologia 1984, 26, 437–440. [Google Scholar] [CrossRef] [Green Version]
- Rosen, R.C.; Cappelleri, J.C.; Smith, M.D.; Lipsky, J.; Pen, B.M. Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction. Int. J. Impot. Res. 1999, 11, 319–326. [Google Scholar] [CrossRef] [Green Version]
- Rhoden, E.L.; Telöken, C.; Sogari, P.R.; Vargas Souto, C.A. The use of the simplified International Index of Erectile Function (IIEF-5) as a diagnostic tool to study the prevalence of erectile dysfunction. Int. J. Impot. Res. 2002, 14, 245–250. [Google Scholar] [CrossRef] [Green Version]
- National Institutes of Health (NIH) Consensus Conference. Impotence. NIH Consensus Development Panel on Impotence. JAMA 1993, 270, 83–90. [Google Scholar] [CrossRef]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [Green Version]
- Saramies, J.; Koiranen, M.; Auvinen, J.; Uusitalo, H.; Hussi, E.; Cederberg, H.; Tuomilehto, J. 22-year trends in dysglycemia and body mass index: A population-based cohort study in Savitaipale, Finland. Prim. Care Diabetes 2021, 15, 977–984. [Google Scholar] [CrossRef]
- Chew, K.K.; Stuckey, B.; Bremner, A.; Earle, C.; Jamrozik, K. Male erectile dysfunction: Its prevalence in Western Australia and associated sociodemographic factors. J. Sex. Med. 2008, 5, 60–69. [Google Scholar] [CrossRef]
- Ahn, T.Y.; Park, J.K.; Lee, S.W.; Hong, J.H.; Park, N.C.; Kim, J.J.; Park, K.; Park, H.; Hyun, J.S. Prevalence and risk factors for erectile dysfunction in Korean men: Results of an epidemiological study. J. Sex. Med. 2007, 4, 1269–1276. [Google Scholar] [CrossRef]
- Eardley, I. The incidence, prevalence, and natural history of erectile dysfunction. Sex. Med. Rev. 2013, 1, 3–16. [Google Scholar] [CrossRef]
- Suija, K.; Kerkelä, M.; Rajala, U.; Jokelainen, J.; Laakso, M.; Härkönen, P.; Keinänen-Kiukaanniemi, S.; Timonen, M. The association between erectile dysfunction, depressive symptoms and testosterone levels among middle-aged men. Scand. J. Public Health 2014, 42, 677–682. [Google Scholar] [CrossRef]
- Sánchez-Cruz, J.J.; Cabrera-León, A.; Martín-Morales, A.; Fernández, A.; Burgos, R.; Rejas, J. Male Erectile Dysfunction and Health-Related Quality of Life. Eur. Urol. 2003, 44, 245–253. [Google Scholar] [CrossRef]
- Erens, B.; Mitchell, K.R.; Gibson, L.; Datta, J.; Lewis, R.; Field, N.; Wellings, K. Health status, sexual activity and satisfaction among older people in Britain: A mixed methods study. PLoS ONE 2019, 27, 14. [Google Scholar] [CrossRef]
- Corona, G.; Lee, D.M.; Forti, G.; O’Connor, D.B.; Maggi, M.; O’Neill, T.W. Age-related changes in general and sexual health in middle-aged and older men: Results from the European Male Ageing Study (EMAS). J. Sex. Med. 2010, 7, 1362–1380. [Google Scholar] [CrossRef]
- Koskimäki, J.; Shiri, R.; Tammela, T.; Häkkinen, J.; Hakama, M.; Auvinen, A. Regular Intercourse Protects Against Erectile Dysfunction: Tampere Aging Male Urologic Study. Am. J. Med. 2008, 121, 592–596. [Google Scholar] [CrossRef]
- Sharma, A.; Sharma, R.P. Erectile Dysfunction: The Male Stigma. Int. J. Surg. 2019, 5, 172–178. [Google Scholar] [CrossRef]
- Yafi, F.A.; Huynh, L.M.; Ahlering, T.; Rosen, R. What Is a "Validated Questionnaire"? A Critical Review of Erectile Function Assessment. J. Sex. Med. 2020, 17, 849–860. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Men Who Participated in the Baseline Study, N = 359 | Men Who Participated in the Follow-Up Study, N = 218 | Men Who Participated Both in the Baseline and Follow-Up Studies, N = 189 | Incidence ** N (%) *** p | |||||
|---|---|---|---|---|---|---|---|---|
| All | ED Prevalence | All | ED Prevalence | All | ED Prevalence at Baseline | ED Prevalence at Follow-up | ||
| N | % | N | % | N | N (%) | N (%) | ||
| Age group | * p ≤ 0.001 | * p < 0.001 | * p < 0.001 | * p ≤ 0.001 | ||||
| 50–54 | 57 | 38.6 | 46 | 16 (34.8) | 33 (71.7) | 17 (56.7) 0.581 | ||
| 55–59 | 105 | 41.0 | 60 | 24 (40.0) | 36 (60.0) | 19 (52.8) 0.209 | ||
| 60–64 | 76 | 68.4 | 33 | 75.8 | 42 | 25 (59.5) | 37 (88.1) | 12 (70.6) 0.352 |
| 65–69 | 66 | 84.8 | 72 | 58.3 | 25 | 21 (84.0) | 25 (100) | 4 (100.0) 0.099 |
| 70–74 | 55 | 87.3 | 56 | 85.7 | 16 | 14 (87.5) | 16 (100) | 2 (100.0) 0.250 |
| 75–79 | 31 | 100 | ||||||
| 80–86 | 26 | 100 | ||||||
| Total | 359 | 61.6 | 218 | 78.9 | 189 | 100(52.9) | 147(77.8) | 54 (60.7) |
| Education | * p = 0.01 | * p = 0.03 | * p = 0.005 | * p = 0.028 | ||||
| Higher | 19 | 42.1 | 23 | 56.5 | 19 | 8 (42.1) | 10 (52.6) | 3 (27.3) 0.024 |
| Vocational | 74 | 41.9 | 77 | 77.9 | 69 | 27 (39.1) | 52 (75.4) | 27 (64.3) 0.279 |
| Basic | 92 | 64.1 | 94 | 81.9 | 82 | 53 (64.6) | 67 (81.7) | 18 (62.1) 0.631 |
| Total | 185 | 53.0 | 194 | 77.3 | 170 | 88 (51.8) | 129 (75.9) | 48 (58.5) |
| Social class | * p = 0.81 | * p = 0.38 | * p = 0.78 | * p = 0.42 | ||||
| Upper | 55 | 60.0 | 60 | 75.0 | 49 | 28 (57.1) | 36 (73.5) | 11 (52.4) 0.491 |
| Upper middle | 18 | 50.0 | 20 | 65.0 | 18 | 9 (50.0) | 12(66.7) | 3 (33.3) 0.100 |
| Middle | 18 | 44.4 | 20 | 75.0 | 17 | 7 (41.2) | 12 (70.6) | 6 (60.0) 0.921 |
| Working | 56 | 53.6 | 56 | 80.4 | 52 | 27 (51.9) | 42 (80.8) | 17 (68.0) 0.233 |
| Other | 14 | 57 | 14 | 92.9 | 13 | 8 (61.5) | 12 (92.3) | 4 (80.0) 0.313 |
| Total | 161 | 54.) | 170 | 77.1 | 149 (100) | 79 (53.0) | 114 (76.5) | |
| Marital status | * p = 0.03 | * p = 0.16 | * p = 0.053 | * p = 0.044 | ||||
| Married or cohabiting | 271 | 58.3 | 160 | 75.6 | 150 | 74 (49.3) | 112 (74.7) | 45 (59.2) 0.494 |
| Single, divorced, or widowed | 83 | 71.1 | 42 | 85.7 | 39 | 26 (66.7) | 35 (89.7) | 9 (69.2) 0.494 |
| Total | 354 | 61.3 | 202 | 77.7 | 189 | 100 (52.9) | 147 (77.8) | 54 (60.7) |
| Smoking | * p = 0.069 | * p = 0.90 | * p = 0.040 | * p = 0.33 | ||||
| Never smoked | 142 | 64.1 | 84 | 81 | 84 | 50 (59.5) | 68 (81.0) | 19 (55.9) 0.467 |
| Stopped smoking | 129 | 65.1 | 92 | 78.3 | 64 | 35 (54.7) | 50 (78.1) | 19 (65.5) 0.516 |
| Current smoker | 76 | 50.0 | 19 | 78.9 | 35 | 12 (34.3) | 24 (68.6) | 13 (56.5) 0.636 |
| Total | 347 | 61.4 | 195 | 79.5 | 183 | 97 (53.0) | 142 (77.6) | 54 (60.7) |
| Weekly alcohol consumption (g) | * p = 0.18 | * p = 0.44 | * p = 0.10 | * p = 0.52 | ||||
| No alcohol consumption | 43 | 72.1 | 33 | 84.8 | 23 (14.6) | 16 (69.6) | 19 (82.6) | 3 (42.9) 0.339 |
| <168 g | 210 | 57.1 | 116 | 75.0 | 120 (75.9) | 56 (46.7) | 92 (76.7) | 39 (60.9) 0.635 |
| ≥168 g | 32 | 62.5 | 14 | 71.4 | 15 (9.5) | 9 (60.0) | 10 (66.7) | 4 (66.7) 0.719 |
| Total | 285 | 60.0 | 163 | 76.7 | 158 (100) | 81 (51.3) | 121 (76.6) | 46 (59.7) |
| Body Mass Index | * p = 0.47 | * p = 0.07 | * p = 0.96 | * p = 0.03 | ||||
| <30 kg/m2 | 289 | 60.6 | 185 | 76.8 | 159 | 84 (52.8) | 119 (74.8) | 42 (56.0) 0.037 |
| ≥30 kg/m2 | 69 | 65.2 | 33 | 90.9 | 30 | 16 (53.3) | 28 (93.3) | 12 (85.7) 0.037 |
| Total | 358 | 61.5 | 218 | 78.9 | 189 | 100 (52.9) | 147 (77.8) | 54 (60.7) |
| Interest in sexual life | * p < 0.001 | * p < 0.001 | * p < 0.001 | * p = 0.095 | ||||
| As before | 180 | 43.9 | 92 | 66.3 | 104 | 38 (36.5) | 75 (72.1) | 38 (57.6) 0.311 |
| Reduced | 171 | 78.4 | 108 | 87.0 | 82 | 59 (72.0) | 69 (84.1) | 16 (69.6) 0.311 |
| Not at all | 7 | 100 | 11 | 100 | 3 | 3 (100) | 3 (100) | 0 (0.0) |
| Total | 358 | 61.5 | 211 | 78.7 | 189 | 100 (52.9) | 147 (77.8) | 54 (60.7) |
| BDI-I score | * p = 0.002 | * p = 0.015 | * p = 0.016 | * p = 0.339 | ||||
| <10 | 332 | 59.3 | 198 | 76.8 | 179 | 91 (50.8) | 138 (77.1) | 51 (60.7) 0.975 |
| ≥10 | 27 | 88.9 | 20 | 100 | 10 | 9 (90.0) | 9 (90.0) | 3 (60.0) 0.975 |
| Total | 359 | 61.6 | 218 | 78.9 | 189 | 100 (52.9) | 147 (77.8) | 54 (60.7) |
| Variable | All Men | Men Participated to Both Baseline and Follow-Up | ||||||
|---|---|---|---|---|---|---|---|---|
| Baseline (N = 359) | Follow-Up (N = 172) | Baseline (N = 189) | Follow-Up (N = 189) | |||||
| Category | Unadjusted OR (95% CI) | Adjusted OR (95% CI) | Unadjusted OR (95% CI) | Adjusted OR (95% CI) | Unadjusted OR (95% CI) | Adjusted OR (95% CI) | Unadjusted OR (95% CI) | Adjusted OR (95% CI) |
| Age (years) | ||||||||
| 50–54 | ref | ref | ref | ref | ||||
| 55–59 | 1.1 (0.6,2.1) | 0.9 (0.4,1.9) | 1.3 (0.6,2.8) | 1.0 (0.4,2.5) | ||||
| 60–64 | 3.4 (1.7,7.1) | 2.5 (1.1,5.6) | ref | ref | 2.8 (1.2,6.5) | 2.6 (1.0,7.1) | ref | ref |
| 65–69 | 8.9 (3.8,21.0) | 6.1 (2.4,15.8) | 0.4 (0.2,1.1) | 0.4 (0.1,1.2) | 9.8 (2.9,33.7) | 10 (2.6,40.1) | 0.4 (0.2,1.2) | 0.4 (0.1,1.2) |
| 70 and over | 11.0 (4.2,28.4) | 6.3 (2.2,18.1) | 4.2 (1.4,12.3) | 3.8 (1.2,12.1) | 13.0 (2.6,65.1) | 7.9 (1.4,43.6) | 3.7 (1.2,10.8) | 3.5 (1.1,11.3) |
| Education | ||||||||
| Higher or vocational | ref | ref | ref | ref | ref | ref | ref | ref |
| Basic | 2.5 (1.4,4.5) | 2.7 (1.4,5.4) | 1.7 (0.8,3.3) | 1.5 (0.7,3.6) | 2.8 (1.5,5.2) | 3.0 (1.4,6.3) | 1.9 (0.9,3.9) | 1.7 (0.7,4.0) |
| Marital status | ||||||||
| Married or cohabiting | ref | ref | ref | ref | ref | ref | ref | ref |
| Single, divorced, or widowed | 1.8 (1.0,3.0) | 2.1 (1.1,3.9) | 1.9 (0.8,4.9) | 3.0 (0.9,9.7) | 2.1 (1.0,4.3) | 3.0 (1.2,7.5) | 3.0 (1.0,8.9) | 4.1 (1.1,14.4) |
| Body mass index | ||||||||
| <30 kg/m2 | ref | ref | ref | ref | ref | ref | ref | ref |
| ≥30 kg/m2 | 1.5 (0.8,2.8) | 1.1 (0.5,2.4) | 3.0 (0.9,10.4) | 3.6 (0.7,18.6) | 0.7 (0.3,1.8) | 0.7 (0.2,2.4) | 4.1 (0.9,18.1) | 3.7 (0.7,19.5) |
| Interest in sexual life | ||||||||
| As before | ref | ref | ref | ref | ref | ref | ref | ref |
| Reduced or not at all | 4.9 (3.1,7.8) | 3.3 (1.9,5.7) | 3.8 (1.9,7.7) | 2.8 (1.2,6.8) | 4.7 (2.5,8.7) | 4.0 (1.9,8.4) | 4.1 (1.9,8.6) | 3.3 (1.3,8.1) |
| Beck’s BDI-I score | ||||||||
| <10 | ref | ref | ref | ref | ref | ref | ref | ref |
| ≥10 | 3.7 (1.8,7.7) | 2.4 (1.1,5.6) | 5.4 (1.3,23.5) | 2.5 (0.5,12.8) | 3.9 (1.4,11.1) | 3.4 (1.0,11.3) | 5.1 (1.2,22.4) | 2.3 (0.4,12.3) |
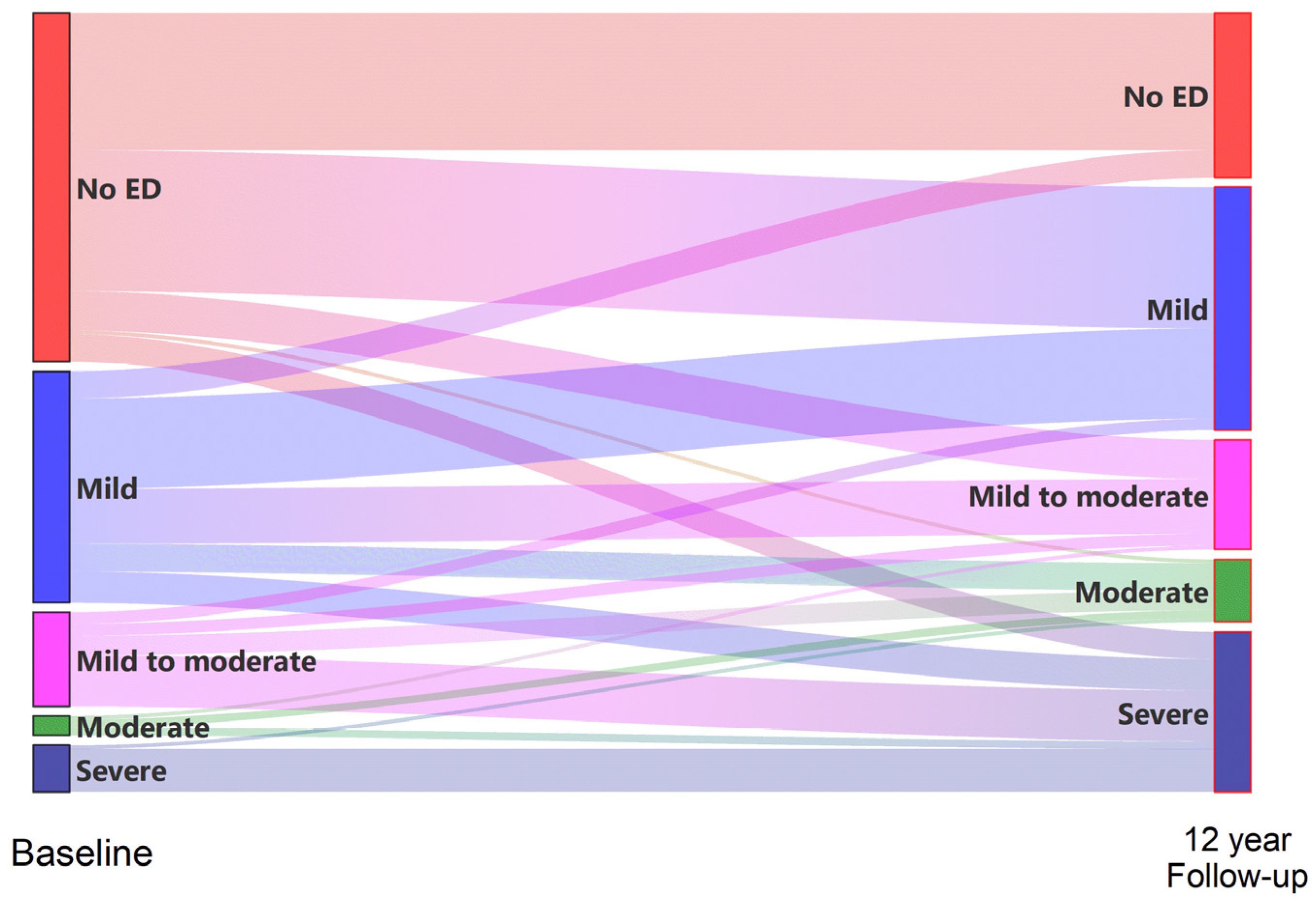
| ED at the Baseline | ||||||
|---|---|---|---|---|---|---|
| No ED | Mild | Mild to Moderate | Moderate | Severe | Total | |
| ED at 12-Year Follow-Up | N (%) | N (%) | N (%) | N (%) | N (%) | N (%) |
| No ED | 35 (39.3) | 7 (11.9) | 42 (22.2) | |||
| Mild | 36 (40.4) | 23 (39.0) | 3 (12.5) | 62 (32.8) | ||
| Mild to moderate | 10 (11.2) | 14 (23.7) | 3 (12.5) | 1 (20.0) | 28 (14.8) | |
| Moderate | 1 (1.1) | 7 (11.9) | 5 (20.8) | 2 (40.0) | 1 (8.3) | 16 (8.5) |
| Severe | 7 (7.9) | 8 (13.6) | 13 (54.2) | 2 (40.0) | 11 (91.7) | 41 (21.7) |
| Total | 89 (100) | 59 (100) | 24 (100) | 5 (100) | 12 (100) | 189 (100) |
| Erectile Function Remained Same or Improved | Erectile Function Decreased | Erectile Dysfunction Persistence | |||||||
|---|---|---|---|---|---|---|---|---|---|
| N | % | OR (95% CI) | N | % | OR (95% CI) | N | % | OR (95% CI) | |
| Baseline age | p ≤ 0.001 | p = 0.009 | p ≤ 0.001 | ||||||
| 50–54 | 46 | 28.3 | ref | 45 | 53.3 | ref | 46 | 34.8 | ref |
| 55–59 | 60 | 41.7 | 1.8 (0.8,4.1) | 59 | 44.1 | 0.7 (0.3,1.5) | 60 | 28.3 | 0.7 (0.3,1.7) |
| 60–64 | 42 | 19 | 0.6 (0.2,1.6) | 37 | 64.9 | 1.6 (0.7,3.9) | 42 | 59.5 | 2.8 (1.2,6.5) |
| 65–69 | 25 | 4 | 0.1 (0.0,0.9) | 22 | 77.3 | 3.0 (0.9,9.5) | 25 | 84 | 9.8 (2.9,33.7) |
| 70–75 | 16 | 0 | n.a. | 14 | 85.7 | 5.2 (1.1,26.2) | 16 | 87.5 | 13.1 (2.6,65.1) |
| Education | p = 0.073 | p = 0.568 | p = 0.002 | ||||||
| Higher or vocational | 88 | 33 | ref | 81 | 55.6 | ref | 88 | 36.4 | ref |
| Basic | 82 | 20.7 | 0.5 (0.3,1.1) | 80 | 60 | 1.2 (0.6,2.2) | 82 | 59.8 | 2.6 (1.4,4.8) |
| Social class | p = 0.280 | p = 0.285 | p = 0.699 | ||||||
| Upper | 49 | 30.6 | ref | 46 | 54.3 | ref | 49 | 51 | ref |
| Upper middle | 18 | 38.9 | 1.4 (0.5,4.4) | 17 | 52.9 | 0.9 (0.3,2.9) | 18 | 50 | 1.0 (0.3,2.8) |
| Middle | 17 | 29.4 | 0.9 (0.3,3.2) | 16 | 50 | 0.8 (0.3,2.6) | 17 | 35.3 | 0.5 (0.2,1.6) |
| Working | 52 | 21.2 | 0.6 (0.2,1.5) | 50 | 56 | 1.1 (0.5,2.4) | 52 | 48.1 | 0.9 (0.4,1.9) |
| Other | 13 | 7.7 | 0.2 (0.0,1.6) | 10 | 90 | 7.6 (0.9,64.6) | 13 | 61.5 | 1.5 (0.4,5.4) |
| Marital status | p = 0.051 | p = 0.365 | p = 0.014 | ||||||
| Married or cohabiting | 150 | 28 | ref | 142 | 59.9 | ref | 150 | 44.7 | ref |
| Single, divorced, or widowed | 39 | 12.8 | 0.4 (0.1,1.0) | 35 | 51.4 | 0.7 (0.3,1.5) | 39 | 66.7 | 2.5 (1.2,5.2) |
| Change in Smoking | p = 0.476 | p = 0.668 | p = 0.136 | ||||||
| Nonsmoker at baseline–nonsmoker at follow-up | 133 | 23.3 | ref | 125 | 59.2 | ref | 133 | 51.9 | ref |
| Smoker at baseline–nonsmoker at follow-up | 13 | 38.5 | 2.1 (0.6,6.7) | 11 | 45.5 | 0.6 (0.2,2.0) | 13 | 38.5 | 0.6 (0.2,1.9) |
| Smoker at baseline–smoker at follow-up | 15 | 26.7 | 1.2 (0.4,4.0) | 15 | 60 | 1.0 (0.3,3.1) | 15 | 26.7 | 0.3 (0.1,1.1) |
| Change in alcohol use | p = 0.627 | p = 0.774 | p = 0.038 | ||||||
| No alcohol at all | 16 | 37.5 | ref | 13 | 53.8 | ref | 16 | 75 | ref |
| Same or decreased | 75 | 26.7 | 0.6 (0.2,1.9) | 72 | 61.1 | 1.3 (0.4,4.4) | 75 | 40 | 0.2 (0.1,0.8) |
| Increased | 51 | 25.5 | 0.6 (0.2,1.9) | 47 | 55.3 | 1.1 (0.3,3.6) | 51 | 45.1 | 0.3 (0.1,1.0) |
| Change in BMI | p = 0.328 | p = 0.791 | p = 0.329 | ||||||
| BMI same or decreased | 105 | 27.6 | ref | 96 | 57.3 | ref | 105 | 52.4 | ref |
| MI increased | 84 | 21.4 | 0.7 (0.4,1.4) | 81 | 59.3 | 1.1 (0.6,2.0) | 84 | 45.2 | 0.8 (0.4,1.3) |
| Change in sexual interest | p ≤ 0.001 | p ≤ 0.001 | p = 0.025 | ||||||
| Increased | 21 | 28.6 | ref | 20 | 65 | ref | 21 | 61.9 | ref |
| No change | 105 | 35.2 | 1.4 (0.5,3.8) | 97 | 46.4 | 0.5 (0.2,1.3) | 105 | 40 | 0.4 (0.2,1.1) |
| Decreased | 57 | 5.3 | 0.1 (0.0,0.6) | 55 | 76.4 | 1.7 (0.6,5.3) | 57 | 59.6 | 0.9 (0.3,2.5) |
| Change in Beck BDI-I | p ≤ 0.001 | p = 0.118 | p = 0.024 | ||||||
| Same or decreased | 97 | 35.1 | ref | 93 | 52.7 | ref | 97 | 41.2 | ref |
| Increased | 92 | 14.1 | 0.3 (0.1,0.6) | 84 | 64.3 | 1.6 (0.9,3.0) | 92 | 57.6 | 1.9 (1.1,3.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saramies, J.; Koiranen, M.; Auvinen, J.; Uusitalo, H.; Hussi, E.; Becker, S.; Keinänen-Kiukaanniemi, S.; Tuomilehto, J.; Suija, K. A Natural History of Erectile Dysfunction in Elderly Men: A Population-Based, Twelve-Year Prospective Study. J. Clin. Med. 2022, 11, 2146. https://doi.org/10.3390/jcm11082146
Saramies J, Koiranen M, Auvinen J, Uusitalo H, Hussi E, Becker S, Keinänen-Kiukaanniemi S, Tuomilehto J, Suija K. A Natural History of Erectile Dysfunction in Elderly Men: A Population-Based, Twelve-Year Prospective Study. Journal of Clinical Medicine. 2022; 11(8):2146. https://doi.org/10.3390/jcm11082146
Chicago/Turabian StyleSaramies, Jouko, Markku Koiranen, Juha Auvinen, Hannu Uusitalo, Esko Hussi, Sebastian Becker, Sirkka Keinänen-Kiukaanniemi, Jaakko Tuomilehto, and Kadri Suija. 2022. "A Natural History of Erectile Dysfunction in Elderly Men: A Population-Based, Twelve-Year Prospective Study" Journal of Clinical Medicine 11, no. 8: 2146. https://doi.org/10.3390/jcm11082146
APA StyleSaramies, J., Koiranen, M., Auvinen, J., Uusitalo, H., Hussi, E., Becker, S., Keinänen-Kiukaanniemi, S., Tuomilehto, J., & Suija, K. (2022). A Natural History of Erectile Dysfunction in Elderly Men: A Population-Based, Twelve-Year Prospective Study. Journal of Clinical Medicine, 11(8), 2146. https://doi.org/10.3390/jcm11082146