
Are EPA and DHA Derivatives Involved in IBD Remission?

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
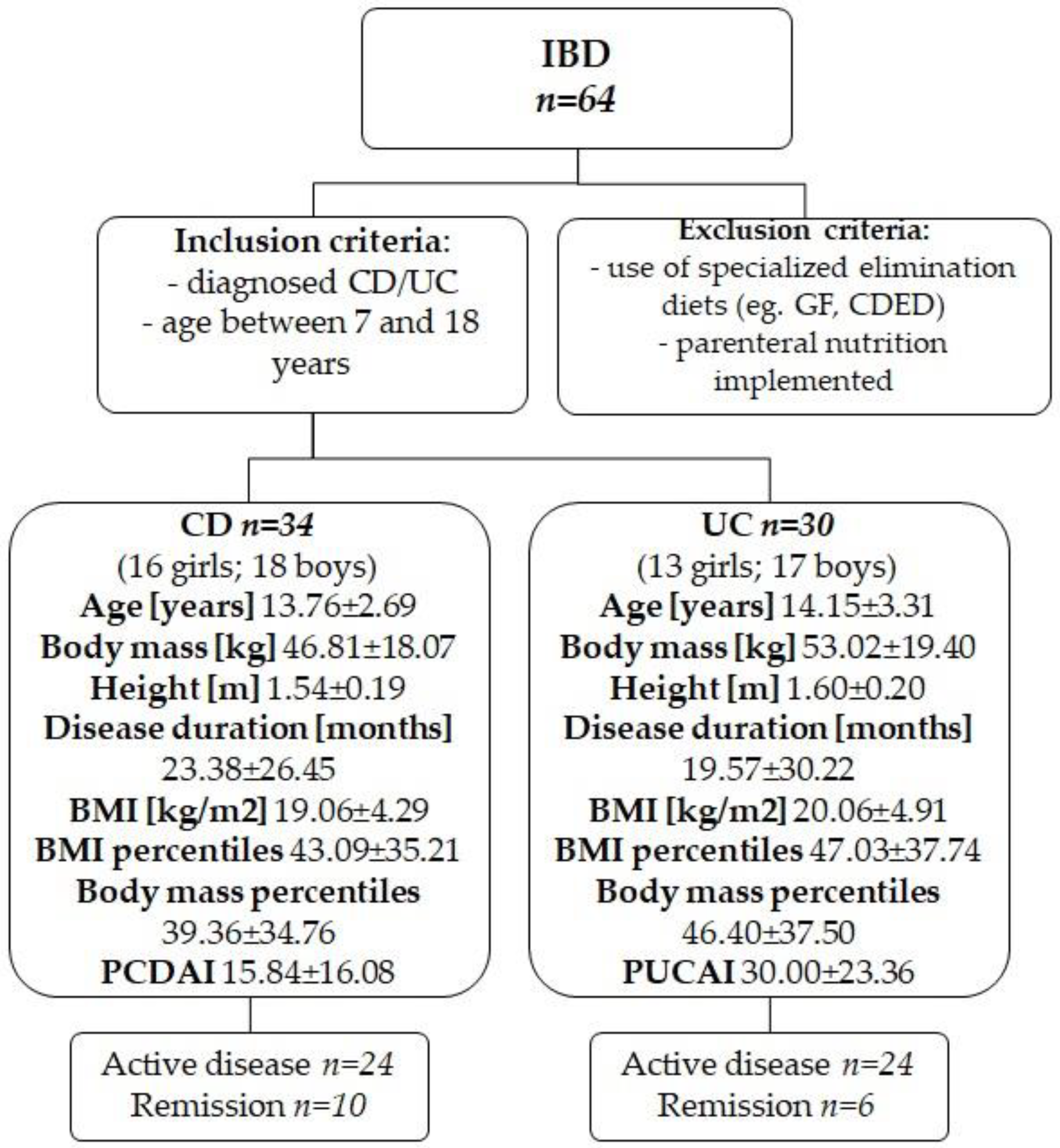
2.1. Characteristics and Division of the Study Group
2.2. Anthropometric Measurements
2.3. Sample Collection
2.4. Extraction of Eicosanoids
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sýkora, J.; Pomahačová, R.; Kreslová, M.; Cvalínová, D.; Štych, P.; Schwarz, J. Current Global Trends in the Incidence of Pediatric-Onset Inflammatory Bowel Disease. World J. Gastroenterol. 2018, 24, 2741–2763. [Google Scholar] [CrossRef] [PubMed]
- Kikut, J.; Konecka, N.; Ziętek, M.; Szczuko, M. Inflammatory Bowel Disease Etiology: Current Knowledge. Pteridines 2018, 29, 206–214. [Google Scholar] [CrossRef]
- Ungaro, F.; Rubbino, F.; Danese, S.; D’Alessio, S. Actors and Factors in the Resolution of Intestinal Inflammation: Lipid Mediators as a New Approach to Therapy in Inflammatory Bowel Diseases. Front. Immunol. 2017, 8, 1331. [Google Scholar] [CrossRef] [PubMed]
- Camba-Gómez, M.; Gualillo, O.; Conde-Aranda, J. New Perspectives in the Study of Intestinal Inflammation: Focus on the Resolution of Inflammation. Int. J. Mol. Sci. 2021, 22, 2605. [Google Scholar] [CrossRef]
- Patterson, E.; Wall, R.; Fitzgerald, G.F.; Ross, R.P.; Stanton, C. Health Implications of High Dietary Omega-6 Polyunsaturated Fatty Acids. J. Nutr. Metab. 2012, 2012, 539426. [Google Scholar] [CrossRef]
- Serhan, C.N.; Petasis, N.A. Resolvins and Protectins in Inflammation-Resolution. Chem. Rev. 2011, 111, 5922–5943. [Google Scholar] [CrossRef] [Green Version]
- Schwanke, R.C.; Marcon, R.; Bento, A.F.; Calixto, J.B. EPA- and DHA-Derived Resolvins’ Actions in Inflammatory Bowel Disease. Eur. J. Pharmacol. 2016, 785, 156–164. [Google Scholar] [CrossRef]
- Serhan, C.N.; Chiang, N.; Dalli, J. The Resolution Code of Acute Inflammation: Novel Pro-Resolving Lipid Mediators in Resolution. Semin. Immunol. 2015, 27, 200–215. [Google Scholar] [CrossRef] [Green Version]
- Ungaro, F.; Tacconi, C.; Massimino, L.; Corsetto, P.A.; Correale, C.; Fonteyne, P.; Piontini, A.; Garzarelli, V.; Calcaterra, F.; Della Bella, S.; et al. MFSD2A Promotes Endothelial Generation of Inflammation-Resolving Lipid Mediators and Reduces Colitis in Mice. Gastroenterology 2017, 153, 1363–1377.e6. [Google Scholar] [CrossRef] [Green Version]
- Serhan, C.N. Pro-Resolving Lipid Mediators Are Leads for Resolution Physiology. Nature 2014, 510, 92–101. [Google Scholar] [CrossRef] [Green Version]
- Vong, L.; Ferraz, J.G.P.; Panaccione, R.; Beck, P.L.; Wallace, J.L. A Pro-Resolution Mediator, Prostaglandin D2, Is Specifically up-Regulated in Individuals in Long-Term Remission from Ulcerative Colitis. Proc. Natl. Acad. Sci. USA 2010, 107, 12023–12027. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, S.; Wan, M.; Huang, W.; Stanton, R.C.; Xu, Y. Maresins: Specialized Proresolving Lipid Mediators and Their Potential Role in Inflammatory-Related Diseases. Mediat. Inflamm. 2018, 2018, e2380319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neurath, M.F. Cytokines in Inflammatory Bowel Disease. Nat. Rev. Immunol. 2014, 14, 329–342. [Google Scholar] [CrossRef] [PubMed]
- Weylandt, K.H.; Kang, J.X.; Wiedenmann, B.; Baumgart, D.C. Lipoxins and Resolvins in Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2007, 13, 797–799. [Google Scholar] [CrossRef]
- Kułaga, Z.; Różdżyńska-Świątkowska, A.; Grajda, A.; Gurzkowska, B.; Wojtyło, M.; Góźdź, M.; Świąder-Leśniak, A.; Litwin, M. Percentile charts for growth and nutritional status assessment in Polish children and adolescents from birth to 18 year of age. Stand. Med. Pediatr. 2015, 12, 119–135. [Google Scholar]
- Charpentier, C.; Chan, R.; Salameh, E.; Mbodji, K.; Ueno, A.; Coëffier, M.; Guérin, C.; Ghosh, S.; Savoye, G.; Marion-Letellier, R. Dietary N-3 PUFA May Attenuate Experimental Colitis. Mediat. Inflamm. 2018, 2018, e8430614. [Google Scholar] [CrossRef]
- Kikut, J.; Konecka, N.; Ziętek, M.; Kulpa, D.; Szczuko, M. Diet Supporting Therapy for Inflammatory Bowel Diseases. Eur. J. Nutr. 2021, 60, 2275–2291. [Google Scholar] [CrossRef]
- Becker, F.; Romero, E.; Goetzmann, J.; Hasselschwert, D.L.; Dray, B.; Vanchiere, J.; Fontenot, J.; Yun, J.W.; Norris, P.C.; White, L.; et al. Endogenous Specialized Proresolving Mediator Profiles in a Novel Experimental Model of Lymphatic Obstruction and Intestinal Inflammation in African Green Monkeys. Am. J. Pathol. 2019, 189, 1953–1972. [Google Scholar] [CrossRef]
- Pearl, D.S.; Masoodi, M.; Eiden, M.; Brümmer, J.; Gullick, D.; McKeever, T.M.; Whittaker, M.A.; Nitch-Smith, H.; Brown, J.F.; Shute, J.K.; et al. Altered Colonic Mucosal Availability of N-3 and n-6 Polyunsaturated Fatty Acids in Ulcerative Colitis and the Relationship to Disease Activity. J. Crohns Colitis 2014, 8, 70–79. [Google Scholar] [CrossRef]
- Masoodi, M.; Pearl, D.S.; Eiden, M.; Shute, J.K.; Brown, J.F.; Calder, P.C.; Trebble, T.M. Altered Colonic Mucosal Polyunsaturated Fatty Acid (PUFA) Derived Lipid Mediators in Ulcerative Colitis: New Insight into Relationship with Disease Activity and Pathophysiology. PLoS ONE 2013, 8, e76532. [Google Scholar] [CrossRef] [Green Version]
- Gobbetti, T.; Dalli, J.; Colas, R.A.; Canova, D.F.; Aursnes, M.; Bonnet, D.; Alric, L.; Vergnolle, N.; Deraison, C.; Hansen, T.V.; et al. Protectin D1n-3 DPA and Resolvin D5n-3 DPA Are Effectors of Intestinal Protection. Proc. Natl. Acad. Sci. USA 2017, 114, 3963–3968. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quiros, M.; Feier, D.; Birkl, D.; Agarwal, R.; Zhou, D.W.; García, A.J.; Parkos, C.A.; Nusrat, A. Resolvin E1 Is a Pro-Repair Molecule That Promotes Intestinal Epithelial Wound Healing. Proc. Natl. Acad. Sci. USA 2020, 117, 9477–9482. [Google Scholar] [CrossRef] [PubMed]
- Günay, S.; Taşova, F.; Yılmaz, H.E.; Paköz, Z.B.; Çekiç, C. Serum Resolvin E1 Levels and Its Relationship with Disease Activity in Ulcerative Colitis. Gastroenterol. Res. Pract. 2019, 2019, 6258327. [Google Scholar] [CrossRef] [PubMed]
- Zhu, S.; Li, S. Expression of endogenous heme oxygenase-1/carbon monoxide system and resolvin E1 in the patients of Crohn disease. Chin. J. Postgrad. Med. 2019, 309–313. [Google Scholar]
- Ishida, T.; Yoshida, M.; Arita, M.; Nishitani, Y.; Nishiumi, S.; Masuda, A.; Mizuno, S.; Takagawa, T.; Morita, Y.; Kutsumi, H.; et al. Resolvin E1, an Endogenous Lipid Mediator Derived from Eicosapentaenoic Acid, Prevents Dextran Sulfate Sodium Induced Colitis. Inflamm. Bowel Dis. 2010, 16, 87–95. [Google Scholar] [CrossRef] [Green Version]
- Campbell, E.L.; Louis, N.A.; Tomassetti, S.E.; Canny, G.O.; Arita, M.; Serhan, C.N.; Colgan, S.P. Resolvin E1 Promotes Mucosal Surface Clearance of Neutrophils: A New Paradigm for Inflammatory Resolution. FASEB J. 2007, 21, 3162–3170. [Google Scholar] [CrossRef] [Green Version]
- Bento, A.F.; Claudino, R.F.; Dutra, R.C.; Marcon, R.; Calixto, J.B. Omega-3 Fatty Acid-Derived Mediators 17(R)-Hydroxy Docosahexaenoic Acid, Aspirin-Triggered Resolvin D1 and Resolvin D2 Prevent Experimental Colitis in Mice. J. Immunol. 2011, 187, 1957–1969. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.; Choo, J.; Kim, S.J.; Heo, G.; Pothoulakis, C.; Kim, Y.-H.; Im, E. Analysis of endogenous lipids during intestinal wound healing. PLoS ONE 2017, 12, e0183028. [Google Scholar] [CrossRef] [Green Version]
- Colas, R.A.; Shinohara, M.; Dalli, J.; Chiang, N.; Serhan, C.N. Identification and Signature Profiles for Pro-Resolving and Inflammatory Lipid Mediators in Human Tissue. Am. J. Physiol.-Cell Physiol. 2014, 307, C39–C54. [Google Scholar] [CrossRef] [Green Version]
- Liu, M.; Boussetta, T.; Makni-Maalej, K.; Fay, M.; Driss, F.; El-Benna, J.; Lagarde, M.; Guichardant, M. Protectin DX, a Double Lipoxygenase Product of DHA, Inhibits Both ROS Production in Human Neutrophils and Cyclooxygenase Activities. Lipids 2014, 49, 49–57. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
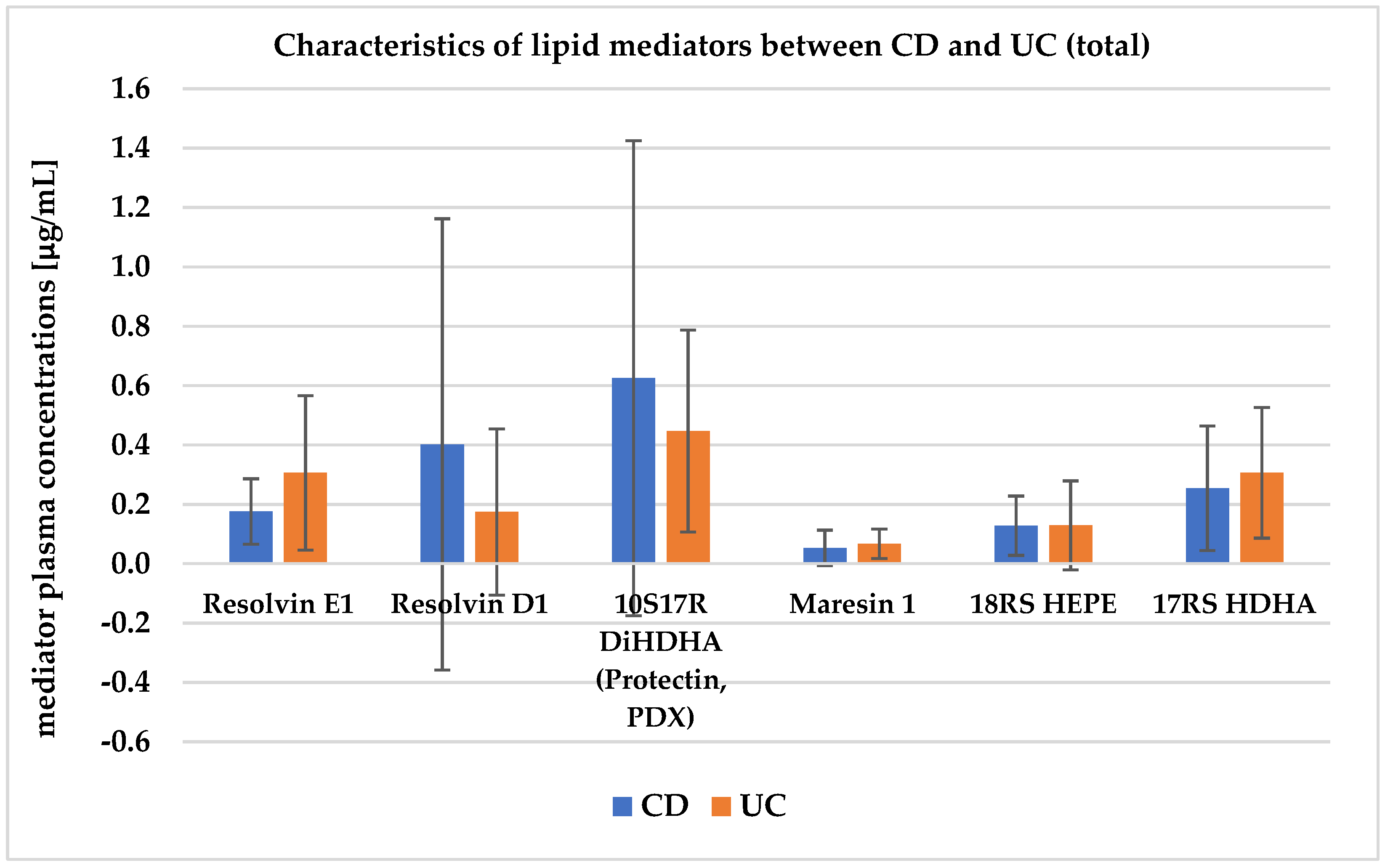
| Lipid Mediators (μg/mL) | CD n = 34 | UC n = 30 | p-Value |
|---|---|---|---|
| Resolvin E1 | 0.176 ± 0.11 | 0.306 ± 0.26 | 0.014 * |
| Resolvin D1 | 0.402 ± 0.76 | 0.174 ± 0.28 | 0.150 |
| 10S17R DiHDHA (Protectin, PDX) | 0.625 ± 0.80 | 0.447 ± 0.34 | 0.299 |
| Maresin 1 | 0.053 ± 0.06 | 0.067 ± 0.05 | 0.337 |
| 18RS HEPE | 0.128 ± 0.10 | 0.129 ± 0.15 | 0.966 |
| 17RS HDHA | 0.254 ± 0.21 | 0.306 ± 0.22 | 0.364 |
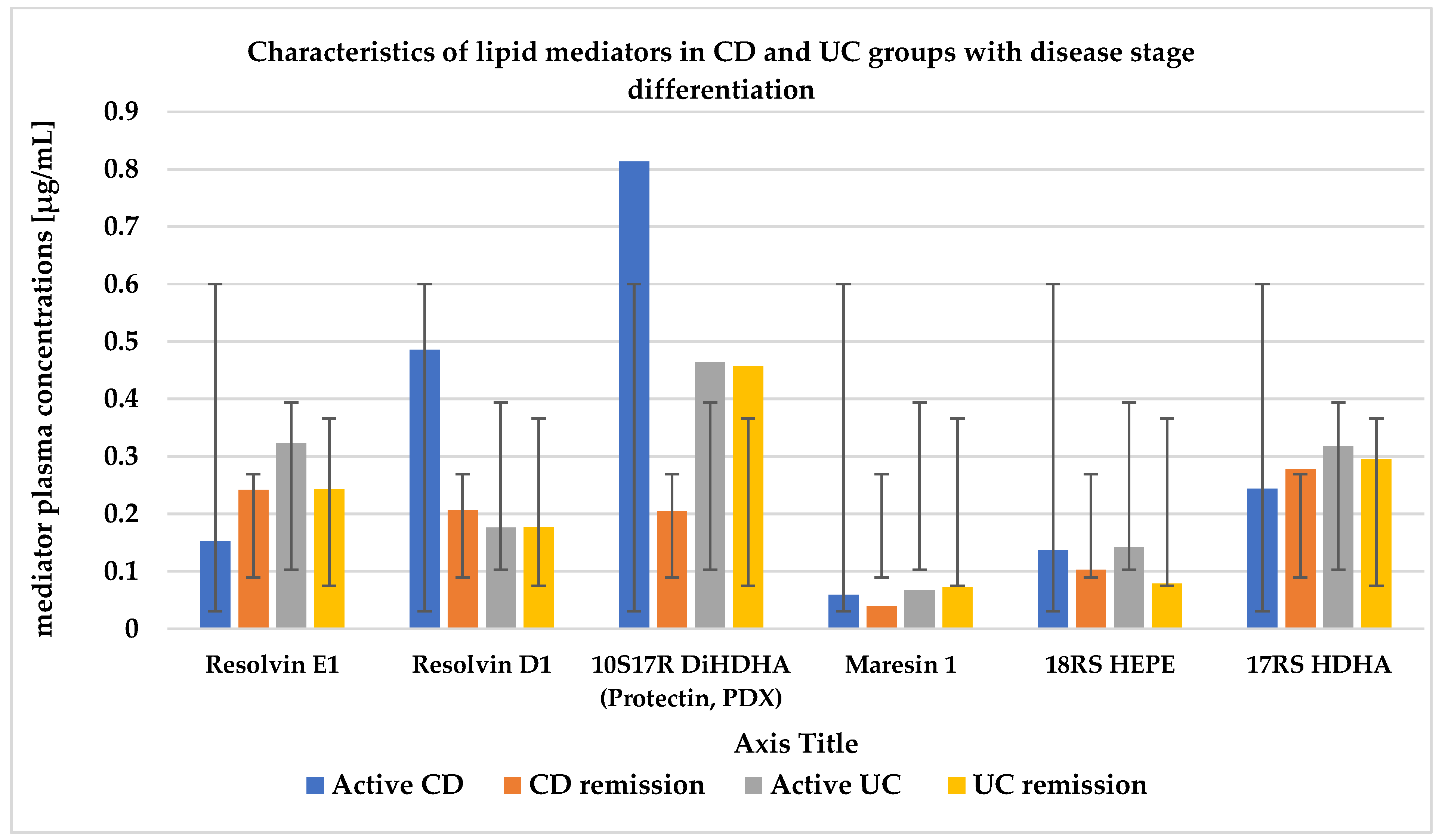
| Lipid Mediators (μg/mL) | Active CD n = 24 | CD Remission n = 10 | p-Value | Active UC n = 24 | UC Remission n = 6 | p-Value | p-Value CD vs. UC Active | p-Value CD vs. UC Remission |
|---|---|---|---|---|---|---|---|---|
| Resolvin E1 | 0.153 ± 0.08 | 0.242 ± 0.16 | 0.167 | 0.323 ± 0.29 | 0.243 ± 0.13 | 0.788 | 0.011 * | 0.958 |
| Resolvin D1 | 0.486 ± 0.89 | 0.207 ± 0.24 | 0.944 | 0.176 ± 0.29 | 0.177 ± 0.23 | 0.864 | 0.137 | 0.713 |
| 10S17R DiHDHA (Protectin, PDX) | 0.813 ± 0.91 | 0.205 ± 0.21 | 0.046 * | 0.464 ± 0.35 | 0.457 ± 0.34 | 0.341 | 0.105 | 0.014 * |
| Maresin 1 | 0.059 ± 0.07 | 0.039 ± 0.04 | 0.796 | 0.068 ± 0.05 | 0.072 ± 0.05 | 0.864 | 0.585 | 0.156 |
| 18RS HEPE | 0.137 ± 0.11 | 0.103 ± 0.07 | 0.439 | 0.142 ± 0.16 | 0.079 ± 0.04 | 0.213 | 0.906 | 0.564 |
| 17RS HDHA | 0.244 ± 0.17 | 0.278 ± 0.30 | 0.656 | 0.318 ± 0.21 | 0.295 ± 0.27 | 0.643 | 0.217 | 0.713 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kikut, J.; Drozd, A.; Mokrzycka, M.; Grzybowska-Chlebowczyk, U.; Ziętek, M.; Szczuko, M. Are EPA and DHA Derivatives Involved in IBD Remission? J. Clin. Med. 2022, 11, 2388. https://doi.org/10.3390/jcm11092388
Kikut J, Drozd A, Mokrzycka M, Grzybowska-Chlebowczyk U, Ziętek M, Szczuko M. Are EPA and DHA Derivatives Involved in IBD Remission? Journal of Clinical Medicine. 2022; 11(9):2388. https://doi.org/10.3390/jcm11092388
Chicago/Turabian StyleKikut, Justyna, Arleta Drozd, Małgorzata Mokrzycka, Urszula Grzybowska-Chlebowczyk, Maciej Ziętek, and Małgorzata Szczuko. 2022. "Are EPA and DHA Derivatives Involved in IBD Remission?" Journal of Clinical Medicine 11, no. 9: 2388. https://doi.org/10.3390/jcm11092388
APA StyleKikut, J., Drozd, A., Mokrzycka, M., Grzybowska-Chlebowczyk, U., Ziętek, M., & Szczuko, M. (2022). Are EPA and DHA Derivatives Involved in IBD Remission? Journal of Clinical Medicine, 11(9), 2388. https://doi.org/10.3390/jcm11092388