
The Association between Vision Impairment and Depression: A Systematic Review of Population-Based Studies

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Search Strategy
2.3. Risk of Bias Assessment
2.4. Statistical Methods
3. Results
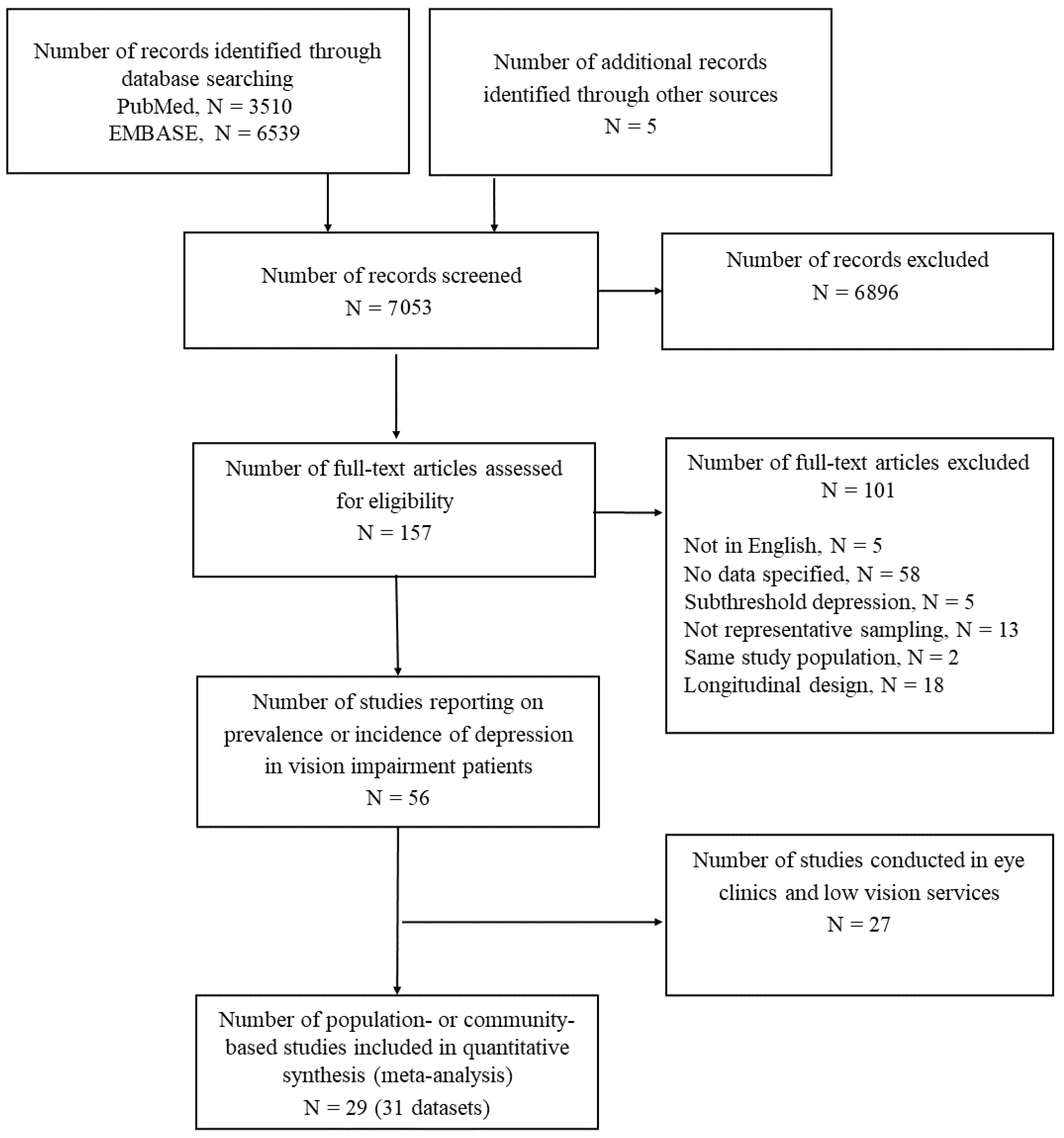
3.1. Results of Searches
3.2. Characteristics of Included Studies
3.3. Findings
3.4. Subgroup Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Ehrlich, J.R.; Ramke, J.; Macleod, D.; Burn, H.; Lee, C.N.; Zhang, J.H.; Waldock, W.; Swenor, B.K.; Gordon, I.; Congdon, N.; et al. Association between vision impairment and mortality: A systematic review and meta-analysis. Lancet Glob. Health 2021, 9, e418–e430. [Google Scholar] [CrossRef]
- Tan, B.K.J.; Man, R.E.K.; Gan, A.T.L.; Fenwick, E.K.; Varadaraj, V.; Swenor, B.K.; Gupta, P.; Wong, T.Y.; Trevisan, C.; Lorenzo-López, L.; et al. Is Sensory Loss an Understudied Risk Factor for Frailty? A Systematic Review and Meta-analysis. J. Gerontol. A. Biol. Sci. Med. Sci. 2020, 75, 2461–2470. [Google Scholar] [CrossRef] [PubMed]
- Evans, J.R.; Fletcher, A.E.; Wormald, R.P. Depression and Anxiety in Visually Impaired Older People. Ophthalmology 2007, 114, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Casten, R.; Rovner, B.W.; Leiby, B.E.; Tasman, W. Depression despite anti-vascular endothelial growth factor treatment of age-related macular degeneration. Arch. Ophthalmol. 2010, 128, 506–508. [Google Scholar] [CrossRef] [Green Version]
- Horowitz, A.; Reinhardt, J.P.; Kennedy, G.J. Major and Subthreshold Depression among Older Adults Seeking Vision Rehabilitation Services. Am. J. Geriatr. Psychiatry 2005, 13, 180–187. [Google Scholar] [CrossRef]
- van der Aa, H.P.A.; Comijs, H.C.; Penninx, B.W.J.H.; van Rens, G.H.M.B.; van Nispen, R.M. Major Depressive and Anxiety Disorders in Visually Impaired Older Adults. Investig. Opthalmol. Vis. Sci. 2015, 56, 849–854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beekman, A.T.F.; Copeland, J.; Prince, M. Review of community prevalence of depression in later life. Br. J. Psychiatry 1999, 174, 307–311. [Google Scholar] [CrossRef]
- Steffens, D.C.; Fisher, G.G.; Langa, K.; Potter, G.G.; Plassman, B.L. Prevalence of depression among older Americans: The Aging, Demographics and Memory Study. Int. Psychogeriatr. 2009, 21, 879–888. [Google Scholar] [CrossRef]
- Maier, A.; Riedel-Heller, S.G.; Pabst, A.; Luppa, M. Risk factors and protective factors of depression in older people 65+. A systematic review. PLoS ONE 2021, 16, e0251326. [Google Scholar] [CrossRef]
- Cherubini, A.; Nistico, G.; Rozzini, R.; Liperoti, R.; Di Bari, M.; Zampi, E.; Ferrannini, L.; Aguglia, E.; Pani, L.; Bernabei, R.; et al. Subthreshold depression in older subjects: An unmet therapeutic need. J. Nutr. Health Aging 2012, 16, 909–913. [Google Scholar] [CrossRef]
- Morichi, V.; Dell’Aquila, G.; Trotta, F.M.; Belluigi, A.; Lattanzio, F.; Cherubini, A. Diagnosing and Treating Depression in Older and Oldest Old. Curr. Pharm. Des. 2015, 21, 1690–1698. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, C. The Greatest Generation Meets Its Greatest Challenge: Vision Loss and Depression in Older Adults. J. Vis. Impair. Blind. 2005, 99, 197–208. [Google Scholar] [CrossRef] [Green Version]
- Van Der Aa, H.P.A.; Margrain, T.H.; Van Rens, G.H.M.B.; Heymans, M.; Van Nispen, R.M.A. Psychosocial interventions to improve mental health in adults with vision impairment: Systematic review and meta-analysis. Ophthalmic Physiol. Opt. 2016, 36, 584–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Nispen, R.M.; Virgili, G.; Hoeben, M.; Langelaan, M.; Klevering, J.; Keunen, J.E.; Van Rens, G.H. Low vision rehabilitation for better quality of life in visually impaired adults. Cochrane Database Syst. Rev. 2020, 1, CD006543. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (Updated February 2022); Cochrane: London, UK, 2022. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Parravano, M.; Petri, D.; Maurutto, E.; Lucenteforte, E.; Menchini, F.; Lanzetta, P.; Varano, M.; van Nispen, R.M.A.; Virgili, G. Association Between Visual Impairment and Depression in Patients Attending Eye Clinics. JAMA Ophthalmol. 2021, 139, 753–761. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. ICD-11 for Mortality and Morbidity Statistics (ICD-11 MMS) 2018 Version. Available online: https://Icd.Who.Int/Browse11/L-M/En (accessed on 21 April 2022).
- Bonifazi, M.; Franchi, M.; Rossi, M.; Moja, L.; Zambelli, A.; Zambon, A.; Corrao, G.; La Vecchia, C.; Zocchetti, C.; Negri, E. Trastuzumab-Related Cardiotoxicity in Early Breast Cancer: A Cohort Study. Oncologist 2013, 18, 795–801. [Google Scholar] [CrossRef] [Green Version]
- Lyu, J.; Kim, H.-Y. Gender-Specific Associations of Sensory Impairments with Depression and Cognitive Impairment in Later Life. Psychiatry Investig. 2018, 15, 926–934. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, T.W.; Surya, S.; Elliott, T.R.; Brossart, D.F.; Burdine, J.N. Depression and health-related quality of life among persons with sensory disabilities in a health professional shortage area. Rehabil. Psychol. 2016, 61, 240–250. [Google Scholar] [CrossRef]
- Bernabei, V.; Morini, V.; Moretti, F.; Marchiori, A.; Ferrari, B.; Dalmonte, E.; De Ronchi, D.; Atti, A.R. Vision and hearing impairments are associated with depressive–anxiety syndrome in Italian elderly. Aging Ment. Health 2011, 15, 467–474. [Google Scholar] [CrossRef]
- Biddulph, J.P.; Iliffe, S.; Kharicha, K.; Harari, D.; Swift, C.; Gillmann, G.; Stuck, A.E. Risk factors for depressed mood amongst a community dwelling older age population in England: Cross-sectional survey data from the PRO-AGE study. BMC Geriatr. 2014, 14, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Capella-McDonnall, M.E. The effects of single and dual sensory loss on symptoms of depression in the elderly. Int. J. Geriatr. Psychiatry 2005, 20, 855–861. [Google Scholar] [CrossRef]
- Carabellese, C.; Appollonio, I.; Rozzini, R.; Bianchetti, A.; Frisoni, G.B.; Frattola, L.; Trabucchi, M. Sensory Impairment and Quality of Life in a Community Elderly Population. J. Am. Geriatr. Soc. 1993, 41, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Nanaware, M.B.; Cheluvaraj, P. Rapid psychological assessment of depression and its relationship with physical health urban elderly. Australas. Med. J. 2016, 9, 211. [Google Scholar] [CrossRef]
- Cho, G.E.; Lim, D.H.; Baek, M.; Lee, H.; Kim, S.J.; Kang, S.W. Visual Impairment of Korean Population: Prevalence and Impact on Mental Health. Investig. Opthalmol. Vis. Sci. 2015, 56, 4375–4381. [Google Scholar] [CrossRef]
- Court, H.; McLean, G.; Guthrie, B.; Mercer, S.W.; Smith, D. Visual impairment is associated with physical and mental comorbidities in older adults: A cross-sectional study. BMC Med. 2014, 12, 181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crews, J.E.; Chou, C.-F.; Sekar, S.; Saaddine, J.B. The Prevalence of Chronic Conditions and Poor Health among People With and Without Vision Impairment, Aged ≥65 Years, 2010–2014. Am. J. Ophthalmol. 2017, 182, 18–30. [Google Scholar] [CrossRef]
- Garin, N.; Olaya, B.; Lara, E.; Moneta, M.V.; Miret, M.; Ayuso-Mateos, J.L.; Haro, J.M. Visual impairment and multimorbidity in a representative sample of the Spanish population. BMC Public Health 2014, 14, 815. [Google Scholar] [CrossRef] [Green Version]
- Guthrie, D.M.; Declercq, A.; Finne-Soveri, H.; Fries, B.E.; Hirdes, J.P. The Health and Well-Being of Older Adults with Dual Sensory Impairment (DSI) in Four Countries. PLoS ONE 2016, 11, e0155073. [Google Scholar] [CrossRef] [Green Version]
- Hamedani, A.G.; VanderBeek, B.L.; Willis, A.W. Blindness and Visual Impairment in the Medicare Population: Disparities and Association with Hip Fracture and Neuropsychiatric Outcomes. Ophthalmic Epidemiol. 2019, 26, 279–285. [Google Scholar] [CrossRef]
- Harada, S.; Nishiwaki, Y.; Michikawa, T.; Kikuchi, Y.; Iwasawa, S.; Nakano, M.; Ishigami, A.; Saito, H.; Takebayashi, T. Gender difference in the relationships between vision and hearing impairments and negative well-being. Prev. Med. 2008, 47, 433–437. [Google Scholar] [CrossRef] [PubMed]
- Hirai, F.E.; Tielsch, J.M.; Klein, B.E.K.; Klein, R.; Obhi, S.S.; Swiderski, K.M.; Brubacher, S.P. Relationship between retinopathy severity, visual impairment and depression in persons with long-term type 1 diabetes. Ophthalmic Epidemiol. 2012, 19, 196–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karlsson, J.S. Self-reports of Psychological Distress in Connection with Various Degrees of Visual Impairment. J. Vis. Impair. Blind. 1998, 92, 483–490. [Google Scholar] [CrossRef]
- Lee, D.J.; Gómez-Marín, O.; Lam, B.L. Current Depression, Lifetime History of Depression, and Visual Acuity in Hispanic Adults. J. Vis. Impair. Blind. 2000, 94, 85–96. [Google Scholar] [CrossRef]
- Loprinzi, P.D.; Smit, E.; Pariser, G. Association among Depression, Physical Functioning, and Hearing and Vision Impairment in Adults with Diabetes. Diabetes Spectr. 2013, 26, 6–15. [Google Scholar] [CrossRef] [Green Version]
- Lupsakko, T.; Mäntyjärvi, M.; Kautiainen, H.; Sulkava, R. Combined hearing and visual impairment and depression in a population aged 75 years and older. Int. J. Geriatr. Psychiatry 2002, 17, 808–813. [Google Scholar] [CrossRef] [PubMed]
- Lyness, J.M.; Niculescu, A.; Tu, X.; Reynolds, C.F., 3rd; Caine, E.D. The Relationship of Medical Comorbidity and Depression in Older, Primary Care Patients. J. Psychosom. Res. 2006, 47, 435–439. [Google Scholar] [CrossRef]
- Park, H.-Y.; Ryu, H.; Kang, H.-Y.; Lee, H.; Kwon, J.-W. Clinical and Economic Burden of Visual Impairment in an Aging Society of South Korea. Asia Pac. J. Public Health 2015, 27, 631–642. [Google Scholar] [CrossRef]
- Rahman, M.S.; Rahman, M.A.; Ali, M.; Rahman, M.S.; Maniruzzaman, M.; Yeasmin, M.A.; Ahmed, N.A.M.F.; Abedin, M.M.; Islam, S.M.S. Determinants of depressive symptoms among older people in Bangladesh. J. Affect. Disord. 2020, 264, 157–162. [Google Scholar] [CrossRef]
- Rovner, B.W.; Ganguli, M. Depression and disability associated with impaired vision: The MoVies Project. J. Am. Geriatr. Soc. 1998, 46, 617–619. [Google Scholar] [CrossRef]
- Schuster, A.K.; Tesarz, J.; Rezapour, J.; Beutel, M.E.; Bertram, B.; Pfeiffer, N. Visual Impairment Is Associated With Depressive Symptoms—Results From the Nationwide German DEGS1 Study. Front. Psychiatry 2018, 9, 114. [Google Scholar] [CrossRef] [PubMed]
- Tsai, S.-Y.; Cheng, C.-Y.; Hsu, W.-M.; Su, T.-P.T.; Liu, J.-H.; Chou, P. Association between visual impairment and depression in the elderly. J. Formos. Med Assoc. 2003, 102, 86–90. [Google Scholar] [PubMed]
- Van Nispen, R.M.A.; Vreeken, H.L.; Comijs, H.C.; Deeg, D.J.H.; Van Rens, G.H.M.B. Role of vision loss, functional limitations and the supporting network in depression in a general population. Acta Ophthalmol. 2015, 94, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Wee, L.E.; Yong, Y.Z.; Chng, M.W.X.; Chew, S.H.; Cheng, L.; Chua, Q.H.A.; Yek, J.J.L.; Lau, L.J.F.; Anand, P.; Hoe, J.T.M.; et al. Individual and area-level socioeconomic status and their association with depression amongst community-dwelling elderly in Singapore. Aging Ment. Health 2014, 18, 628–641. [Google Scholar] [CrossRef]
- Zhang, X.; Bullard, K.M.; Cotch, M.F.; Wilson, M.R.; Rovner, B.W.; McGwin, G.; Owsley, C.; Barker, L.; Crews, J.E.; Saaddine, J.B. Association Between Depression and Functional Vision Loss in Persons 20 Years of Age or Older in the United States, NHANES 2005-2008. JAMA Ophthalmol. 2013, 131, 573–581. [Google Scholar] [CrossRef] [Green Version]
- Wallace, S.; MacTaggart, I.; Banks, L.M.; Polack, S.; Kuper, H. Association of anxiety and depression with physical and sensory functional difficulties in adults in five population-based surveys in low and middle-income countries. PLoS ONE 2020, 15, e0231563. [Google Scholar] [CrossRef]
- Abdoli, N.; Salari, N.; Darvishi, N.; Jafarpour, S.; Solaymani, M.; Mohammadi, M.; Shohaimi, S. The global prevalence of major depressive disorder (MDD) among the elderly: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2022, 132, 1067–1073. [Google Scholar] [CrossRef]
- Hu, T.; Zhao, X.; Wu, M.; Li, Z.; Luo, L.; Yang, C.; Yang, F. Prevalence of depression in older adults: A systematic review and meta-analysis. Psychiatry Res. 2022, 311, 114511. [Google Scholar] [CrossRef]
- Abdolalizadeh, P.; Falavarjani, K.G. Correlation between global prevalence of vision impairment and depressive disorders. Eur. J. Ophthalmol. 2022, 11206721221086152. [Google Scholar] [CrossRef]
- Frank, C.R.; Xiang, X.; Stagg, B.; Ehrlich, J. Longitudinal Associations of Self-reported Vision Impairment with Symptoms of Anxiety and Depression among Older Adults in the United States. JAMA Ophthalmol. 2019, 137, 793–800. [Google Scholar] [CrossRef]
- Liu, W.; Yang, C.; Liu, L.; Kong, G.; Zhang, L. Bidirectional associations of vision loss, hearing loss, and dual sensory loss with depressive symptoms among the middle-aged and older adults in China. J. Affect. Disord. 2022, 301, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, M.V.M.R.; Júnior, H.N.H.-R.; Ribeiro, E.A.N.; Jucá, M.J.; Barbosa, F.T.; De Sousa-Rodrigues, C.F. Association between visual impairment and depression in the elderly: A systematic review. Arq. Bras. Oftalmol. 2015, 78, 197–201. [Google Scholar] [CrossRef] [Green Version]
- Katon, W.J. Clinical and health services relationships between major depression, depressive symptoms, and general medical illness. Biol. Psychiatry 2003, 54, 216–226. [Google Scholar] [CrossRef]
- Lêng, C.H.; Wang, J.-D. Long term determinants of functional decline of mobility: An 11-year follow-up of 5464 adults of late middle aged and elderly. Arch. Gerontol. Geriatr. 2013, 57, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.J.; Gomez-Marin, O.; Lam, B.L.; Zheng, D.D.; Caban, A. Visual Impairment and Morbidity in Community-Residing Adults: The National Health Interview Survey 1986–1996. Ophthalmic Epidemiol. 2005, 12, 13–17. [Google Scholar] [CrossRef]
- Renaud, J.; Bédard, E. Depression in the elderly with visual impairment and its association with quality of life. Clin. Interv. Aging 2013, 8, 931–943. [Google Scholar] [CrossRef] [Green Version]
- Heesterbeek, T.J.; Aa, H.P.A.; Rens, G.H.M.B.; Twisk, J.W.R.; van Nispen, R.M.A. The incidence and predictors of depressive and anxiety symptoms in older adults with vision impairment: A longitudinal prospective cohort study. Ophthalmic Physiol. Opt. 2017, 37, 385–398. [Google Scholar] [CrossRef] [PubMed]
- Keay, L.; Munoz, B.; Turano, K.A.; Hassan, S.E.; Munro, C.A.; Duncan, D.D.; Baldwin, K.; Jasti, S.; Gower, E.W.; West, S.K. Visual and Cognitive Deficits Predict Stopping or Restricting Driving: The Salisbury Eye Evaluation Driving Study (SEEDS). Investig. Opthalmology Vis. Sci. 2009, 50, 107–113. [Google Scholar] [CrossRef]
- Pérès, K.; Matharan, F.; Daien, V.; Nael, V.; Edjolo, A.; Bourdel-Marchasson, I., 1st; Ritchie, K.; Tzourio, C.; Delcourt, C.; Carriere, I. Visual Loss and Subsequent Activity Limitations in the Elderly: The French Three-City Cohort. Am. J. Public Health 2017, 107, 564–569. [Google Scholar] [CrossRef]
- Tsai, D.-C.; Chen, S.-J.; Huang, C.-C.; Yuan, M.-K.; Leu, H.-B. Age-Related Macular Degeneration and Risk of Degenerative Dementia among the Elderly in Taiwan. Ophthalmology 2015, 122, 2327–2335.e2. [Google Scholar] [CrossRef]
- Chung, S.-D.; Ho, J.-D.; Hu, C.-C.; Lin, H.-C.; Sheu, J.-J. Increased Risk of Parkinson Disease Following a Diagnosis of Neovascular Age-Related Macular Degeneration: A Retrospective Cohort Study. Am. J. Ophthalmol. 2014, 157, 464–469.e1. [Google Scholar] [CrossRef] [PubMed]
- Velilla, S.; Garcia-Medina, J.J.; García-Layana, A.; Dolz-Marco, R.; Pons-Vázquez, S.; Pinazo-Duran, M.D.; Gómez-Ulla, F.; Arevalo, J.F.; Díaz-Llopis, M.; Gallego-Pinazo, R. Smoking and Age-Related Macular Degeneration: Review and Update. J. Ophthalmol. 2013, 2013, 895147. [Google Scholar] [CrossRef] [PubMed]
- Adams, M.K.M.; Chong, E.W.; Williamson, E.; Aung, K.Z.; Makeyeva, G.A.; Giles, G.; English, D.; Hopper, J.; Guymer, R.; Baird, P.; et al. 20/20--Alcohol and Age-related Macular Degeneration: The Melbourne Collaborative Cohort Study. Am. J. Epidemiol. 2012, 176, 289–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, D.; Choi, S.; Park, S.M. Effect of smoking cessation on the risk of dementia: A longitudinal study. Ann. Clin. Transl. Neurol. 2018, 5, 1192–1199. [Google Scholar] [CrossRef]
- Ngandu, T.; Lehtisalo, J.; Solomon, A.; Levälahti, E.; Ahtiluoto, S.; Antikainen, R.; Bäckman, L.; Hänninen, T.; Jula, A.; Laatikainen, T.; et al. A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): A randomised controlled trial. Lancet 2015, 385, 2255–2263. [Google Scholar] [CrossRef]
- Bettiol, S.S.; Rose, T.C.; Hughes, C.J.; Smith, L.A. Alcohol Consumption and Parkinson’s Disease Risk: A Review of Recent Findings. J. Park. Dis. 2015, 5, 425–442. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| N° of Studies | N° of Subjects (Range) | |
|---|---|---|
| Overall | 31 | 48,853,780 (218–47,852,342) |
| Country | ||
| United States | 10 | 47,917,779 (484–47,852,342) |
| Europe | 10 | 328,989 (218–291,169) |
| Asia | 9 | 54,220 (254–28,392) |
| Mixed | 2 | 552,792 (2432–550,360) |
| Data source | ||
| Survey | 18 | 622,312 (218–550,360) |
| Administrative database | 3 | 48,162,290 (18,779–47,582,342) |
| Clinical examination | 10 | 69,178 (437–28,392) |
| Criteria for visual impairment | ||
| Self-reported | 15 | 80,100 (400–36,110) |
| BCVA | 12 | 61,030 (218–28,392) |
| ICD | 2 | 47,871,121(18,779–47,852,342) |
| Other criteria | 2 | 841,529 (291,169–550,360) |
| Criteria for depression | ||
| CES-D Scale | 7 | 11,447 (484–2,591) |
| GDS-15 | 6 | 17,118 (254–13,900) |
| PHQ-9 | 4 | 22,782 (567–10,480) |
| Self-reported | 4 | 74,552 (218–36,110) |
| Other criteria | 10 | 48,727,881 (437–47,852,342) |
| N. Subjects (N. Studies) | Pooled Proportion (95% CI) | |
|---|---|---|
| Depression | 929,678 (27) | 0.17 (0.13–0.22) |
| Surveys | 583,563 (17) | 0.19 (0.14–0.27) |
| Clinical Examination | 36,167 (8) | 0.15 (0.10–0.23) |
| Administrative databases | 309,948 (2) | 0.07 (0.03–0.16) |
| p-value * | 0.0664 | |
| Visual Impairment | 48,568,108 (28) | 0.10 (0.07–0.16) |
| Surveys | 611,430 (16) | 0.16 (0.10–0.25) |
| Clinical Examinations | 64,559 (9) | 0.07 (0.03–0.13) |
| Administrative databases | 47,892,290 (3) | 0.03 (0.01–0.07) |
| p-value * | 0.0018 | |
| Depression among visually impaired | 566,156 (21) | 0.27 (0.21–0.33) |
| Surveys | 82,804 (10) | 0.29 (0.22–0.37) |
| Clinical Examinations | 3323 (8) | 0.26 (0.17–0.38) |
| Administrative databases | 480,029 (3) | 0.22 (0.08–0.46) |
| p-value * | 0.7868 | |
| Visual Impairment among depressed | 130,048 (20) | 0.20 (0.13–0.29) |
| Surveys | 89,897 (10) | 0.28 (0.16–0.43) |
| Clinical Examinations | 3459 (8) | 0.15 (0.09–0.25) |
| Administrative databases | 36,692 (2) | 0.08 (0.02–0.33) |
| p-value * | 0.1387 |
| No. of Subjects (No. of Studies) | OR (95 % CI) | I2 | |
|---|---|---|---|
| Unadjusted OR | |||
| Surveys | 617,355 (14) | 1.89 (1.51–2.37) | 89% |
| Clinical Examination | 69,178 (10) | 2.17 (1.76–2.67) | 66% |
| Administrative databases | 48,162,290 (3) | 3.34 (1.01–11.11) | 100% |
| Adjusted OR | |||
| Surveys | 50,437 (8) | 1.75 (1.34–2.30) | 99% |
| Clinical Examinations | 57,352 (4) | 1.17 (1.00–1.37) | 0% |
| Administrative databases | 48,143,511 (2) | 2.47 (0.97–6.33) | 100% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Virgili, G.; Parravano, M.; Petri, D.; Maurutto, E.; Menchini, F.; Lanzetta, P.; Varano, M.; Mariotti, S.P.; Cherubini, A.; Lucenteforte, E. The Association between Vision Impairment and Depression: A Systematic Review of Population-Based Studies. J. Clin. Med. 2022, 11, 2412. https://doi.org/10.3390/jcm11092412
Virgili G, Parravano M, Petri D, Maurutto E, Menchini F, Lanzetta P, Varano M, Mariotti SP, Cherubini A, Lucenteforte E. The Association between Vision Impairment and Depression: A Systematic Review of Population-Based Studies. Journal of Clinical Medicine. 2022; 11(9):2412. https://doi.org/10.3390/jcm11092412
Chicago/Turabian StyleVirgili, Gianni, Mariacristina Parravano, Davide Petri, Erica Maurutto, Francesca Menchini, Paolo Lanzetta, Monica Varano, Silvio Paolo Mariotti, Antonio Cherubini, and Ersilia Lucenteforte. 2022. "The Association between Vision Impairment and Depression: A Systematic Review of Population-Based Studies" Journal of Clinical Medicine 11, no. 9: 2412. https://doi.org/10.3390/jcm11092412
APA StyleVirgili, G., Parravano, M., Petri, D., Maurutto, E., Menchini, F., Lanzetta, P., Varano, M., Mariotti, S. P., Cherubini, A., & Lucenteforte, E. (2022). The Association between Vision Impairment and Depression: A Systematic Review of Population-Based Studies. Journal of Clinical Medicine, 11(9), 2412. https://doi.org/10.3390/jcm11092412