
Acute Effects of Sedentary Behavior on Ankle Torque Assessed with a Custom-Made Electronic Dynamometer

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collection
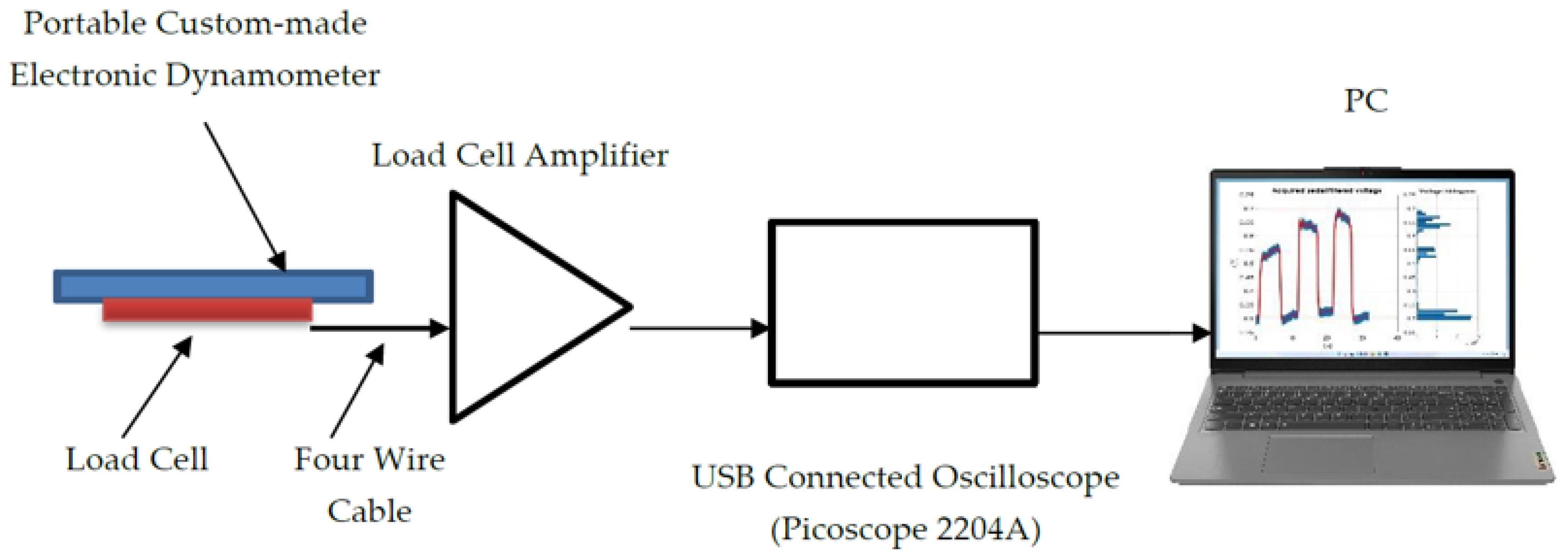
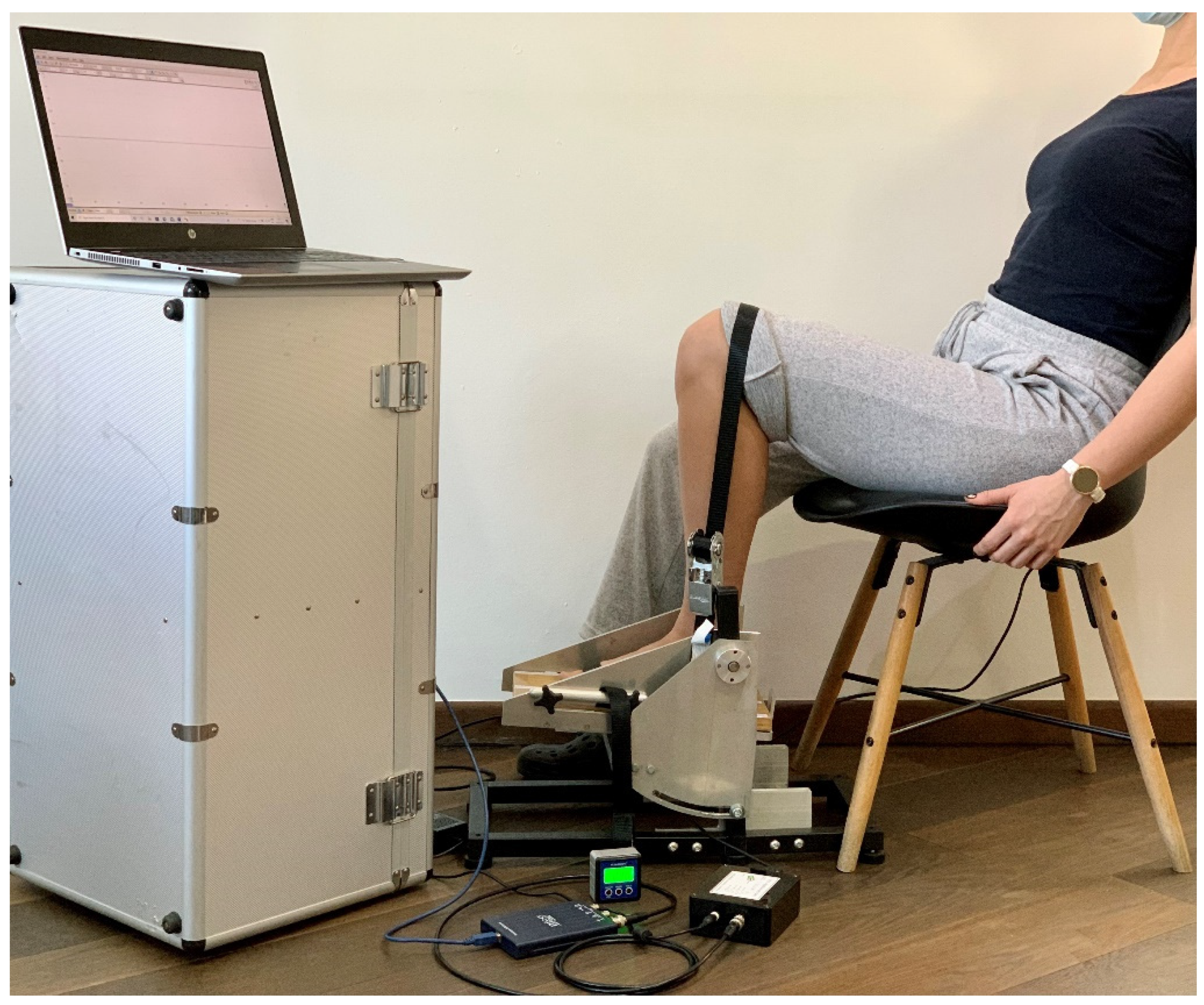
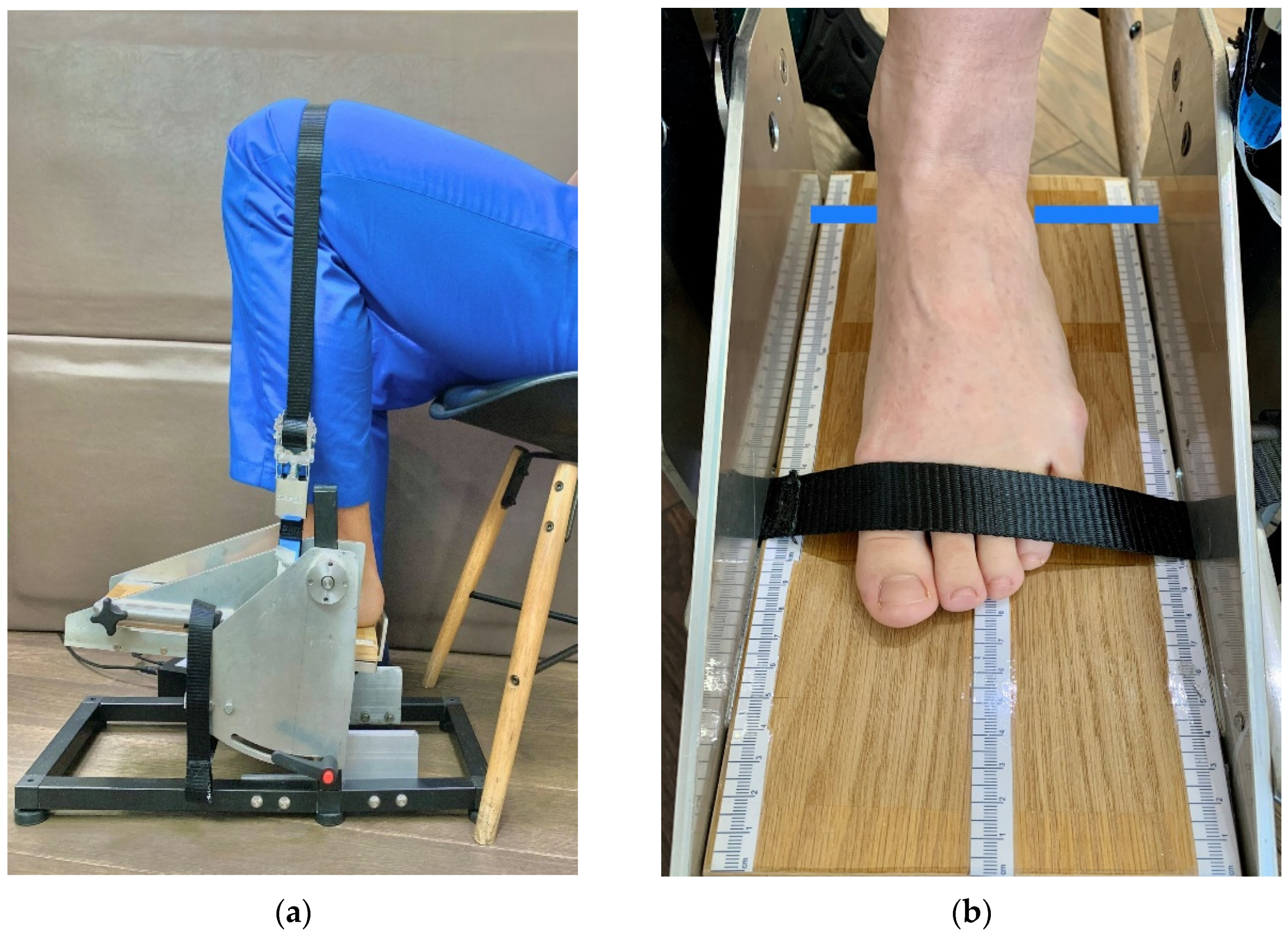
2.3. Description of the Measurement System and Measurement Procedure
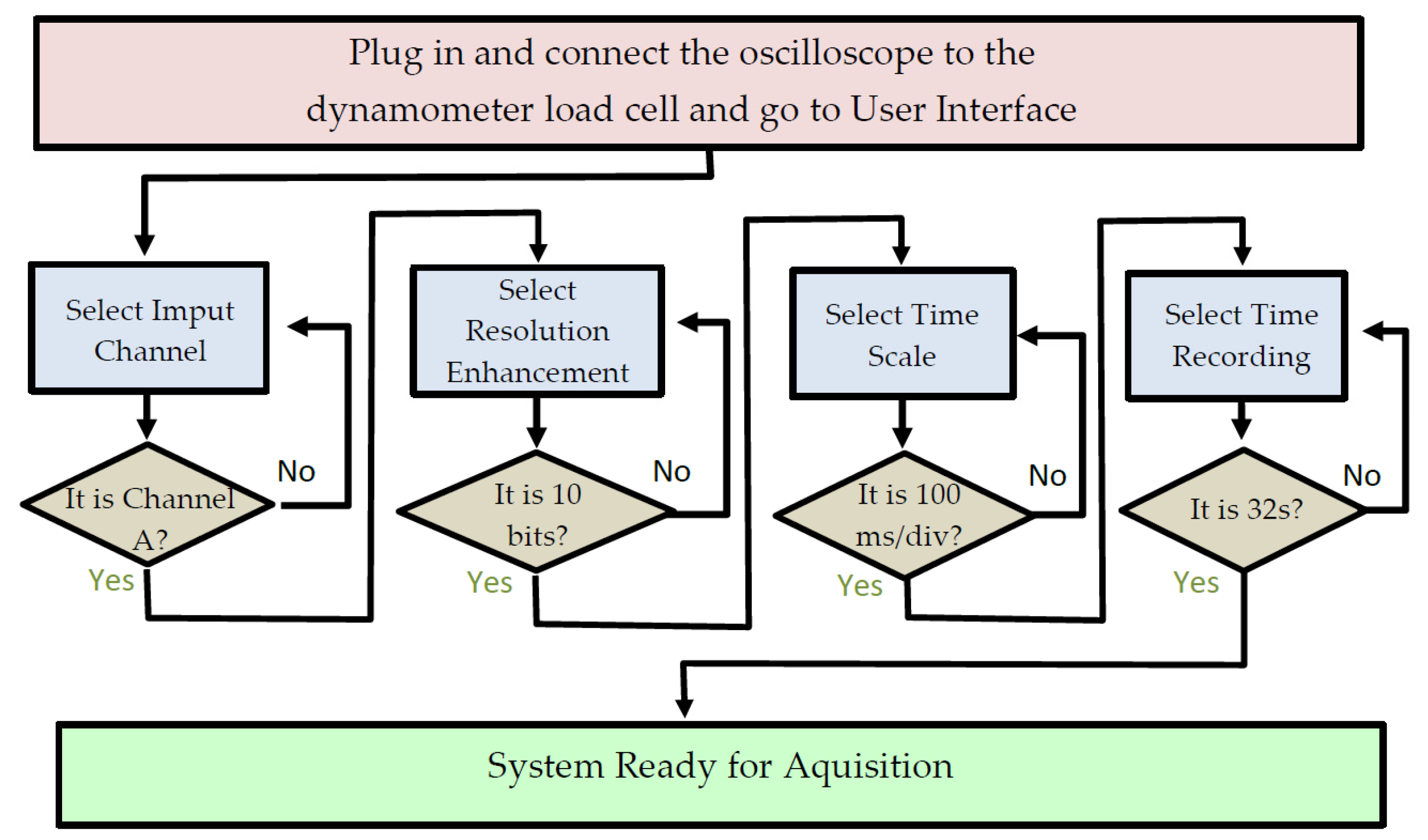
2.3.1. Measurement System Description
2.3.2. Methods of Participant Preparation for Measurement Procedure
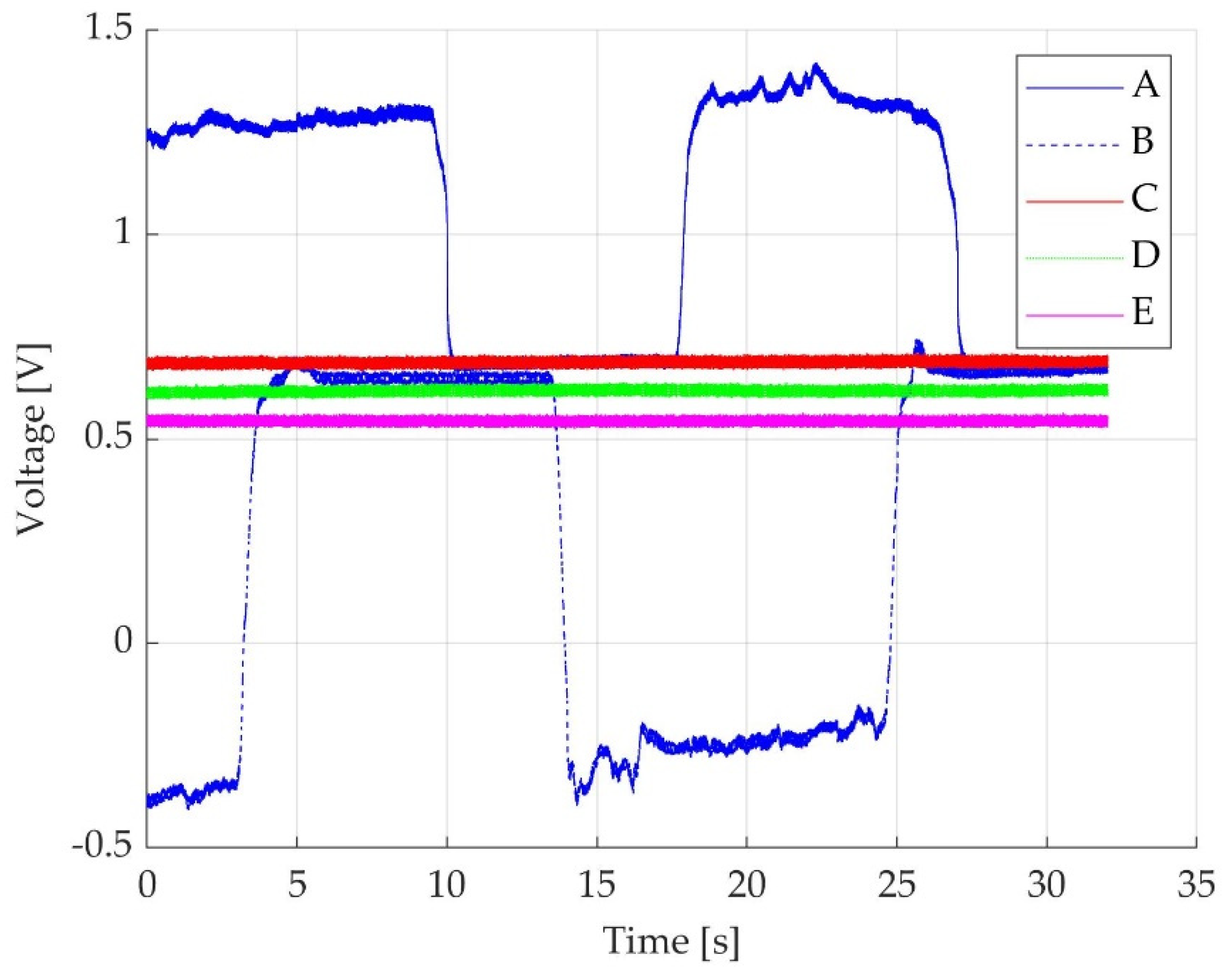
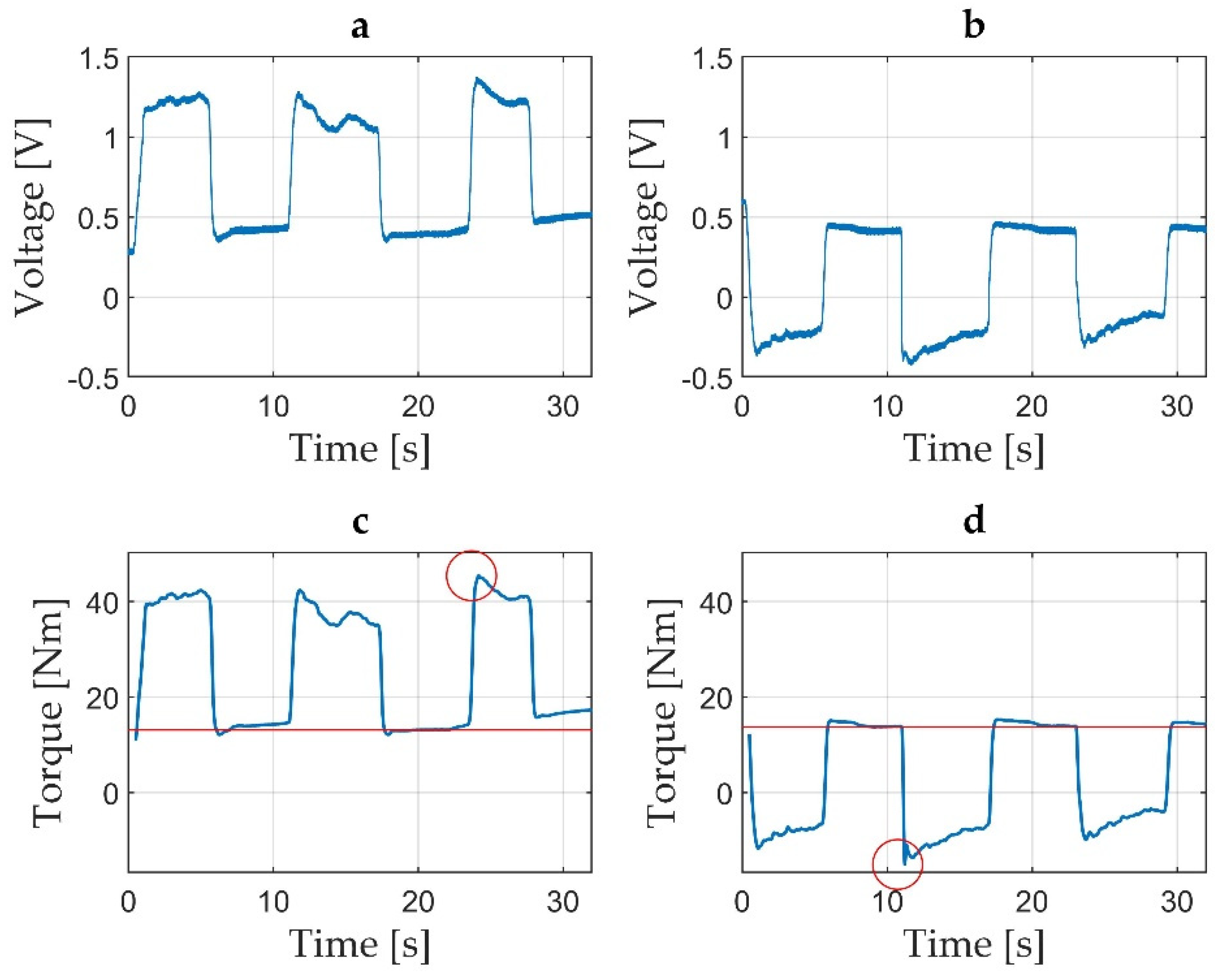
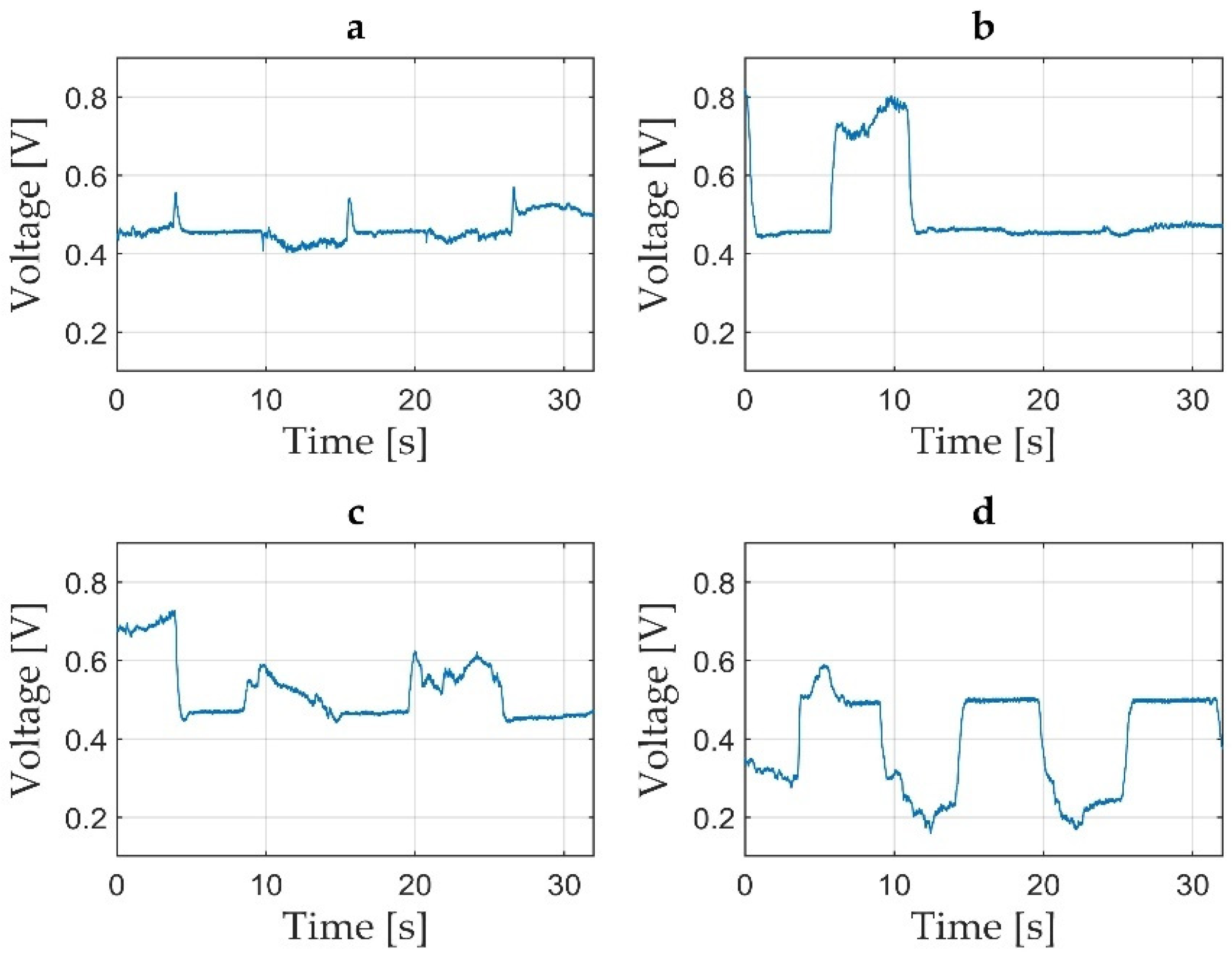
2.3.3. Methods for Validation of Acquired Data
2.4. Other Clinical and Functional Performed Tests
2.5. Statistical Analysis
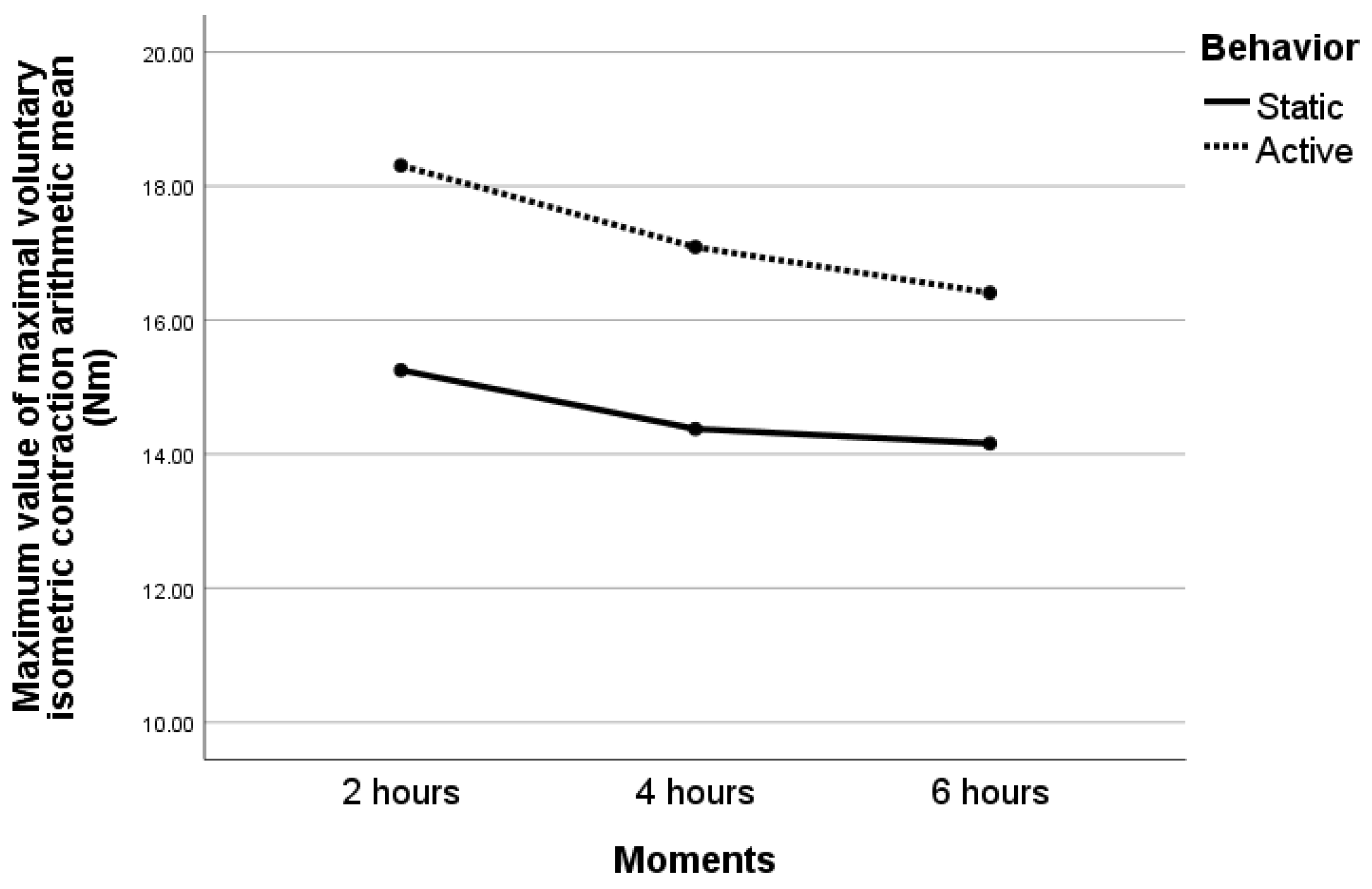
3. Results
3.1. Participant’s Characteristics
3.2. Clinical Measurements Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126–131. [Google Scholar] [PubMed]
- Physical Inactivity. Available online: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/3416 (accessed on 4 March 2022).
- Adult Physical Inactivity Prevalence Maps by Race/Ethnicity. Available online: https://www.cdc.gov/physicalactivity/data/inactivity-prevalence-maps/index.html (accessed on 4 March 2022).
- Tudor-Locke, C.; Craig, C.L.; Brown, W.J.; Clemes, S.A.; De Cocker, K.; Giles-Corti, B.; Hatano, Y.; Inoue, S.; Matsudo, S.M.; Mutrie, N.; et al. How many steps/day are enough? For adults. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tudor-Locke, C.; Hatano, Y.; Pangrazi, R.P.; Kang, M. Revisiting “how many steps are enough?”. Med. Sci. Sports Exerc. 2008, 40, 537–543. [Google Scholar] [CrossRef] [Green Version]
- Nayor, M.; Chernofsky, A.; Spartano, N.L.; Tanguay, M.; Blodgett, J.B.; Murthy, V.L.; Malhotra, R.; Houstis, N.E.; Velagaleti, R.S.; Murabito, J.M.; et al. Physical activity and fitness in the community: The Framingham Heart Study. Eur. Heart J. 2021, 42, 4565–4575. [Google Scholar] [CrossRef] [PubMed]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World; World Health Organization: Geneva, Switzerland, 2018. Available online: https://apps.who.int/iris/handle/10665/272722 (accessed on 6 March 2022).
- Van der Velde, J.H.P.M.; Koster, A.; Van der Berg, J.D.; Sep, S.J.S.; Van der Kallen, C.J.H.; Dagnelie, P.C.; Schram, M.T.; Henry, R.M.A.; Eussen, S.J.P.M.; Van Dongen, M.C.J.M.; et al. Sedentary Behavior, Physi-cal Activity, and Fitness-The Maastricht Study. Med. Sci. Sports Exerc. 2017, 49, 1583–1591. [Google Scholar] [CrossRef]
- Tucker, J.M.; Welk, G.J.; Beyler, N.K. Physical activity in U.S.: Adults’ compliance with the physical activity guidelines for Americans. Am. J. Prev. Med. 2011, 40, 454–461. [Google Scholar] [CrossRef]
- Owen, N.; Healy, G.N.; Matthews, C.E.; Dunstan, D.W. Too much sitting: The population health science of sedentary behavior. Exerc. Sport Sci. Rev. 2010, 38, 105–113. [Google Scholar] [CrossRef]
- Lee, I.M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T. Lancet Physical Activity Series Working Group. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef] [Green Version]
- Sedentary Behaviour Research Network. Letter to the editor: Standardized use of the terms “sedentary” and “sedentary behaviours”. Appl. Physiol. Nutr. Metab. 2012, 37, 540–542. [Google Scholar] [CrossRef] [Green Version]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef] [Green Version]
- Loprinzi, P.D.; Herod, S.M.; Cardinal, B.J.; Noakes, T.D. Physical activity and the brain: A review of this dynamic, bi-directional relationship. Brain Res. 2013, 20, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Schuna, J.M., Jr.; Johnson, W.D.; Tudor-Locke, C. Adult self-reported and objectively monitored physical activity and sedentary behavior: NHANES 2005-2006. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamilton, M.T.; Healy, G.N.; Dunstan, D.W.; Zderic, T.W.; Owen, N. Too Little Exercise and Too Much Sitting: Inactivity Physiology and the Need for New Recommendations on Sedentary Behavior. Curr. Cardiovasc. Risk Rep. 2008, 2, 292–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Healy, G.N.; Clark, B.K.; Winkler, E.A.; Gardiner, P.A.; Brown, W.J.; Matthews, C.E. Measurement of adults’ sedentary time in population-based studies. Am. J. Prev. Med. 2011, 41, 216–227. [Google Scholar] [CrossRef] [Green Version]
- Wilmot, E.G.; Edwardson, C.L.; Achana, F.A.; Davies, M.J.; Gorely, T.; Gray, L.J.; Khunti, K.; Yates, T.; Biddle, S.J. Sedentary time in adults and the association with diabetes, cardiovascular disease and death: Systematic review and meta-analysis. Diabetologia 2012, 55, 2895–2905. [Google Scholar] [CrossRef]
- Hamilton, M.T.; Hamilton, D.G.; Zderic, T.W. Sedentary behavior as a mediator of type 2 diabetes. Med. Sport Sci. 2014, 60, 11–26. [Google Scholar]
- Brocklebank, L.A.; Falconer, C.L.; Page, A.S.; Perry, R.; Cooper, A.R. Accelerometer-measured sedentary time and cardiometabolic biomarkers: A systematic review. Prev. Med. 2015, 76, 92–102. [Google Scholar] [CrossRef] [Green Version]
- Saunders, T.J.; Larouche, R.; Colley, R.C.; Tremblay, M.S. Acute sedentary behaviour and markers of cardiometabolic risk: A systematic review of intervention studies. J. Nutr. Metab. 2012, 2012, 712435. [Google Scholar] [CrossRef]
- Howard, B.J.; Fraser, S.F.; Sethi, P.; Cerin, E.; Hamilton, M.T.; Owen, N.; Dunstan, D.W.; Kingwell, B.A. Impact on hemostatic parameters of interrupting sitting with intermittent activity. Med. Sci. Sports Exerc. 2013, 45, 1285–1291. [Google Scholar] [CrossRef]
- Dunstan, D.W.; Kingwell, B.A.; Larsen, R.; Healy, G.N.; Cerin, E.; Hamilton, M.T.; Shaw, J.E.; Bertovic, D.A.; Zimmet, P.Z.; Salmon, J.; et al. Breaking up prolonged sitting reduces postprandial glucose and insulin responses. Diabetes Care 2012, 35, 976–983. [Google Scholar] [CrossRef] [Green Version]
- Spittaels, H.; Van Cauwenberghe, E.; Verbestel, V.; De Meester, F.; Van Dyck, D.; Verloigne, M.; Haerens, L.; Deforche, B.; Cardon, G.; De Bourdeaudhuij, I. Objectively measured sedentary time and physical activity time across the lifespan: A cross-sectional study in four age groups. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 149. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, M.T. The role of skeletal muscle contractile duration throughout the whole day: Reducing sedentary time and promoting universal physical activity in all people. J. Physiol. 2018, 596, 1331–1340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raichlen, D.A.; Pontzer, H.; Zderic, T.W.; Harris, J.A.; Mabulla, A.Z.P.; Hamilton, M.T.; Wood, B.M. Sitting, squatting, and the evolutionary biology of human inactivity. Proc. Natl. Acad. Sci. USA 2020, 117, 7115–7121. [Google Scholar] [CrossRef]
- Duvivier, B.M.; Schaper, N.C.; Hesselink, M.K.; van Kan, L.; Stienen, N.; Winkens, B.; Koster, A.; Savelberg, H.H. Breaking sitting with light activities vs structured exercise: A randomised crossover study demonstrating benefits for glycaemic control and insulin sensitivity in type 2 diabetes. Diabetologia 2017, 60, 490–498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stephens, B.R.; Granados, K.; Zderic, T.W.; Hamilton, M.T.; Braun, B. Effects of 1 day of inac-tivity on insulin action in healthy men and women: Interaction with energy intake. Metabolism 2011, 60, 941–949. [Google Scholar] [CrossRef]
- Berg, H.E.; Dudley, G.A.; Haggmark, T.; Ohlsen, H.; Tesch, P.A. Effects of lower limb unloading on skeletal muscle mass and function in humans. J. Appl. Physiol. 1991, 70, 1882–1885. [Google Scholar] [CrossRef] [PubMed]
- Hather, B.M.; Adams, G.R.; Tesch, P.A.; Dudley, G.A. Skeletal muscle responses to lower limb suspension in humans. J. Appl. Physiol. 1992, 72, 1493–1498. [Google Scholar] [CrossRef] [Green Version]
- Henshaw, F.R.; Bostan, L.E.; Worsley, P.R.; Bader, D.L. Evaluating the effects of sedentary behaviour on plantar skin health in people with diabetes. J. Tissue Viability 2020, 9, 277–283. [Google Scholar] [CrossRef]
- Caplan, N.; Forbes, A.; Radha, S.; Stewart, S.; Ewen, A.; St Clair Gibson, A.; Kader, D. Effects of 1 week of unilateral ankle immobilization on plantar-flexor strength, balance, and walking speed: A pilot study in asymptomatic volunteers. J. Sport Rehabil. 2015, 24, 156–162. [Google Scholar] [CrossRef]
- Reeves, N.D.; Maganaris, C.N.; Ferretti, G.; Narici, M.V. Influence of 90-day simulated microgravity on human tendon mechanical properties and the effect of resistive countermeasures. J. Appl. Physiol. 2005, 98, 2278–2286. [Google Scholar] [CrossRef] [PubMed]
- Berg, H.E.; Larsson, L.; Tesch, P.A. Lower limb skeletal muscle function after 6 wk of bed rest. J. Appl. Physiol. 1997, 82, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M.T.; Hamilton, D.G.; Zderic, T.W. Exercise physiology versus inactivity physiology: An essential concept for understanding lipoprotein lipase regulation. Exerc. Sport Sci. Rev. 2004, 32, 161–166. [Google Scholar] [CrossRef]
- Hamilton, M.T.; Hamilton, D.G.; Zderic, T.W. Role of low energy expenditure and sitting in obesity, metabolic syndrome, type 2 diabetes, and cardiovascular disease. Diabetes 2007, 56, 2655–2667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soysa, A.; Hiller, C.; Refshauge, K.; Burns, J. Importance and challenges of measuring intrinsic foot muscle strength. J. Foot Ankle Res. 2012, 5, 29. [Google Scholar] [CrossRef] [Green Version]
- Arinci Incel, N.; Genc, H.; Erdem, H.R.; Yorgancioglu, Z.R. Muscle imbalance in hallux valgus: An electromyographic study. Am. J. Phys. Med. Rehabil. 2003, 82, 345–349. [Google Scholar] [CrossRef]
- Goldmann, J.-P.; Brüggemann, G.-P. The potential of human toe flexor muscles to produce force. J. Anat. 2012, 221, 187–194. [Google Scholar] [CrossRef] [Green Version]
- Drăgoi, I.I.; Popescu, F.G.; Petrița, T.; Tatu, R.F.; Bondor, C.I.; Tatu, C.; Bowling, F.L.; Reeves, N.D.; Ionac, M. A Custom-Made Lower Limb Dynamometer for Assessing Ankle Joint Torque in Humans: Calibration and Measurement Procedures. Sensors 2022, 22, 135. [Google Scholar] [CrossRef]
- Dragoi, I.I.; Popescu, F.G.; Petrita, T.; Alexa, F.; Tatu, R.F.; Bondor, C.I.; Tatu, C.; Bowling, F.L.; Reeves, N.D.; Ionac, M. A Custom-Made Electronic Dynamometer for Evaluation of Peak Ankle Torque after COVID-19. Sensors 2022, 22, 2073. [Google Scholar] [CrossRef] [PubMed]
- Tudor-Locke, C.; Bassett, D.R., Jr. How many steps/day are enough? Preliminary pedometer indices for public health. Sports Med. 2004, 34, 1–8. [Google Scholar] [CrossRef]
- Research Solutions (Alsager) LTD Overview—Find and Update Company Information—GOV.UK. Available online: https://find-and-update.company-information.service.gov.uk/company/07746832 (accessed on 16 October 2021).
- PicoScope Model 2204A, Manufactured by Pico Technology, St Neots, UK. Available online: https://www.picotech.com/ (accessed on 16 October 2021).
- PC Oscilloscope, Data Logger & RF Products|Pico Technology. Available online: https://www.picotech.com/ (accessed on 10 January 2022).
- MATLAB, Version 9.9.0.1570001 (R2020b); Update 4. 2020. Available online: https://www.mathworks.com/products/matlab.html (accessed on 18 February 2022).
- Microsoft Corporation. Microsoft Excel. Available online: https://www.microsoft.com/en-us/microsoft-365/excel (accessed on 26 October 2021).
- Landin, D.; Thompson, M.; Reid, M. Knee and Ankle Joint Angles Influence the Plantarflexion Torque of the Gastrocnemius. J. Clin. Med. Res. 2015, 7, 602–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), and the Extended Group for EWGSOP2. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohannon, R.W.; Magasi, S.R.; Bubela, D.J.; Wang, Y.-C.; Gershon, R.C. Grip and knee extension muscle strength reflect a common construct among adults. Muscle Nerve 2012, 46, 555–558. [Google Scholar] [CrossRef] [PubMed]
- Hand Grip Dynamometer MAP-KERN & SOHN GmbH (kern-sohn.com). Available online: https://www.kern-sohn.com/shop/en/medical-scales/hand-grip-dynamometers/MAP/ (accessed on 10 February 2022).
- Kim, S.; Kim, M.; Lee, Y.; Kim, B.; Yoon, T.Y.; Won, C.W. Calf Circumference as a Simple Screening Marker for Diagnosing Sarcopenia in Older Korean Adults: The Korean Frailty and Aging Cohort Study (KFACS). J. Korean Med. Sci. 2018, 33, e151. [Google Scholar] [CrossRef] [PubMed]
- Andre, H.I.; Carnide, F.; Borja, E.; Ramalho, F.; Santos-Rocha, R.; Veloso, A.P. Calf-raise senior: A new test for assessment of plantar flexor muscle strength in older adults: Protocol, validity, and reliability. Clin. Interv. Aging 2016, 11, 1661–1674. [Google Scholar] [CrossRef] [Green Version]
- Andre, H.I.; Moniz-Pereira, V.; Ramalho, F.; Santos-Rocha, R.; Veloso, A.; Carnide, F. Respon-siveness of the Calf-Raise Senior test in community-dwelling older adults undergoing an exercise intervention program. PLoS ONE 2020, 15, e0231556. [Google Scholar] [CrossRef]
- Hébert-Losier, K.; Newsham-West, R.J.; Schneiders, A.G.; Sullivan, S.J. Raising the standards of the calf-raise test: A systematic review. J. Sci. Med. Sport 2009, 12, 594–602. [Google Scholar] [CrossRef] [Green Version]
- Johansson, J.; Strand, B.H.; Morseth, B.; Hopstock, L.A.; Grimsgaard, S. Differences in sarcopenia prevalence between upper-body and lower-body based EWGSOP2 muscle strength criteria: The Tromsø study 2015–2016. BMC Geriatr. 2020, 20, 461. [Google Scholar] [CrossRef]
- IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0; IBM Corp.: Armonk, NY, USA, 2017. [Google Scholar]
- Ding, Y.; Cao, Y.; Duffy, V.G.; Zhang, X. It is Time to Have Rest: How do Break Types Affect Muscular Activity and Perceived Discomfort During Prolonged Sitting Work. Saf. Health Work. 2020, 11, 207–214. [Google Scholar] [CrossRef]
- Hou, Z.C.; Miao, X.; Ao, Y.F.; Hu, Y.L.; Jiao, C.; Guo, Q.W.; Xie, X.; Zhao, F.; Pi, Y.B.; Li, N.; et al. Characteristics and predictors of muscle strength deficit in mechanical ankle instability. BMC Musculoskelet. Disord. 2020, 21, 730. [Google Scholar] [CrossRef]
- Strath, S.J.; Kaminsky, L.A.; Ainsworth, B.E.; Ekelund, U.; Freedson, P.S.; Gary, R.A.; Richardson, C.R.; Smith, D.T.; Swartz, A.M. American Heart Association Physical Activity Committee of the Council on Lifestyle and Cardiometabolic Health and Cardiovascular, Exercise, Cardiac Rehabilitation and Prevention Committee of the Council on Clinical Cardiology, and Council. Guide to the assessment of physical activity: Clinical and research applications: A scientific statement from the American Heart Association. Circulation 2013, 128, 2259–2279. [Google Scholar] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Arithmetic Mean ± Standard Deviation (n = 8) 1 |
|---|---|
| Age (years) | 35.88 ± 12.65 |
| Male, no. 7 (%) | 3 (37.5) |
| Foot length (cm) | 25.36 ± 2.56 |
| BMI 2 (kg/m2) | 25.02 ± 4.43 |
| Average no. 7 of daily steps (steps/day) | 6125 ± 2279.57 |
| AHGS 3 (kg) | 28.01 ± 10.62 |
| ACC 4 (cm) | 37.25 ± 3.17 |
| CRST 5 (no. 7 of repetitions) | 57.25 ± 17.69 |
| Muscle pain during CRST 5 (no. 7 of repetitions) | 42.75 ± 21.37 |
| Muscle fatigue during CRST 5 (no. 7 of repetitions) | 40.5 ± 10.57 |
| ACRT 6 (no. 7 of repetitions) | 30.44 ± 4.92 |
| Chair raise test bilateral | 41.88 ± 13.44 |
| Muscle pain ACRT 6 (no. 7 of repetitions) | 23.38 ± 5.71 |
| Muscle fatigue ACRT 6 (no. 7 of repetitions) | 25.31 ± 3.95 |
| Flexion | Foot | Degree | Time Moment | dMVIC * (Nm) | p ** between Moments | p ** between Active and Static | |
|---|---|---|---|---|---|---|---|
| Static (n = 8) | Active (n = 8) | ||||||
| Dorsi | Left | −5 | 2 | 17.78 ± 12.21 | 21.97 ± 14.05 | 0.087 | 0.560 |
| 4 | 18.01 ± 10.1 | 21.35 ± 10.99 | |||||
| 6 | 16.89 ± 11.08 | 19.01 ± 10.39 | |||||
| 0 | 2 | 19.10 ± 12.40 | 26.11 ± 14.10 | 0.172 | 0.459 | ||
| 4 | 18.01 ± 9.83 | 19.7 ± 10.82 | |||||
| 6 | 18.02 ± 13.15 | 18.91 ± 11.96 | |||||
| 5 | 2 | 20.2 ± 8.44 | 21.57 ± 11.03 | 0.150 | 0.632 | ||
| 4 | 17.67 ± 8.22 | 19.73 ± 9.88 | |||||
| 6 | 18.30 ± 12.15 | 17.24 ± 11.47 | |||||
| Right | −5 | 2 | 17.72 ± 12.33 | 23.99 ± 13.29 | 0.469 | 0.269 | |
| 4 | 18.46 ± 10.71 | 21.16 ± 11.66 | |||||
| 6 | 17.60 ± 11.63 | 22.27 ± 12.01 | |||||
| 0 | 2 | 15.76 ± 10.17 | 21.43 ± 12.85 | 0.098 | 0.783 | ||
| 4 | 14.49 ± 8.19 | 21.32 ± 12.37 | |||||
| 6 | 13.53 ± 9.56 | 18.44 ± 10.41 | |||||
| 5 | 2 | 18.53 ± 10.5 | 21.58 ± 13 | 0.324 | 0.381 | ||
| 4 | 16.26 ± 11.22 | 21.48 ± 12.03 | |||||
| 6 | 15.29 ± 10.43 | 21.45 ± 14.04 | |||||
| Plantar | Left | −5 | 2 | 14.7 ± 7.5 | 19.41 ± 11.31 | 0.922 | 0.267 |
| 4 | 15.1 ± 7.88 | 18.50 ± 9.82 | |||||
| 6 | 16.17 ± 8.50 | 17.10 ± 11 | |||||
| 0 | 2 | 2.63 ± 5.10 | 5.95 ± 7.91 | 0.535 | 0.227 | ||
| 4 | 3.17 ± 5.72 | 3.26 ± 6.99 | |||||
| 6 | 3.83 ± 7.06 | 3.55 ± 7.66 | |||||
| 5 | 2 | 17.84 ± 4.93 | 21.19 ± 17.43 | 0.340 | 0.313 | ||
| 4 | 15.51 ± 4.72 | 20.48 ± 13.28 | |||||
| 6 | 20.32 ± 13.75 | 19.50 ± 12.81 | |||||
| Right | −5 | 2 | 18.15 ± 9.38 | 20.50 ± 13.48 | 0.821 | 0.682 | |
| 4 | 18.10 ± 8.26 | 18.59 ± 11.04 | |||||
| 6 | 16.59 ± 9.91 | 19.33 ± 14.99 | |||||
| 0 | 2 | 3.49 ± 5.61 | 2.05 ± 1.21 | 0.752 | 0.188 | ||
| 4 | 3.52 ± 5.87 | 1.71 ± 2.53 | |||||
| 6 | 2.43 ± 4.78 | 2.31 ± 2.76 | |||||
| 5 | 2 | 21.17 ± 8.10 | 20.69 ± 13.70 | 0.308 | 0.356 | ||
| 4 | 17.9 ± 6.37 | 20.57 ± 12.59 | |||||
| 6 | 16.87 ± 6.47 | 20.36 ± 14.47 | |||||
| Parameters | Pearson/Spearman Coefficient of Correlation | p |
|---|---|---|
| Age (years) | 0.229 | 0.586 |
| BMI 1 (kg/m2) | 0.580 | 0.132 |
| Foot length (cm) | 0.483 | 0.226 |
| Average no. 6 of daily steps (steps/day) | −0.313 * | 0.450 |
| AHGS 2 (kg) | 0.573 | 0.137 |
| ACC 3 (cm) | 0.359 * | 0.382 |
| CRST 4 (no. 6 of repetitions) | 0.535 | 0.171 |
| Muscle pain during CRST 4 (no. 6 of repetitions) | 0.569 | 0.141 |
| Muscle fatigue during CRST 4 (no. 6 of repetitions) | 0.365 | 0.373 |
| ACRT 5 (no. 6 of repetitions) | 0.411 | 0.360 |
| Chair raise test bilateral | 0.048 | 0.911 |
| Muscle pain ACRT 5 (no. 6 of repetitions) | −0.252 * | 0.585 |
| Muscle fatigue ACRT 5 (no. 6 of repetitions) | −0.131 | 0.779 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dragoi, I.I.; Popescu, F.G.; Petrita, T.; Alexa, F.; Barac, S.; Bondor, C.I.; Pauncu, E.-A.; Bowling, F.L.; Reeves, N.D.; Ionac, M. Acute Effects of Sedentary Behavior on Ankle Torque Assessed with a Custom-Made Electronic Dynamometer. J. Clin. Med. 2022, 11, 2474. https://doi.org/10.3390/jcm11092474
Dragoi II, Popescu FG, Petrita T, Alexa F, Barac S, Bondor CI, Pauncu E-A, Bowling FL, Reeves ND, Ionac M. Acute Effects of Sedentary Behavior on Ankle Torque Assessed with a Custom-Made Electronic Dynamometer. Journal of Clinical Medicine. 2022; 11(9):2474. https://doi.org/10.3390/jcm11092474
Chicago/Turabian StyleDragoi, Iulia Iovanca, Florina Georgeta Popescu, Teodor Petrita, Florin Alexa, Sorin Barac, Cosmina Ioana Bondor, Elena-Ana Pauncu, Frank L. Bowling, Neil D. Reeves, and Mihai Ionac. 2022. "Acute Effects of Sedentary Behavior on Ankle Torque Assessed with a Custom-Made Electronic Dynamometer" Journal of Clinical Medicine 11, no. 9: 2474. https://doi.org/10.3390/jcm11092474
APA StyleDragoi, I. I., Popescu, F. G., Petrita, T., Alexa, F., Barac, S., Bondor, C. I., Pauncu, E. -A., Bowling, F. L., Reeves, N. D., & Ionac, M. (2022). Acute Effects of Sedentary Behavior on Ankle Torque Assessed with a Custom-Made Electronic Dynamometer. Journal of Clinical Medicine, 11(9), 2474. https://doi.org/10.3390/jcm11092474