
Abnormal Dorsal Caudate Activation Mediated Impaired Cognitive Flexibility in Mild Traumatic Brain Injury


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Neuropsychological Tests
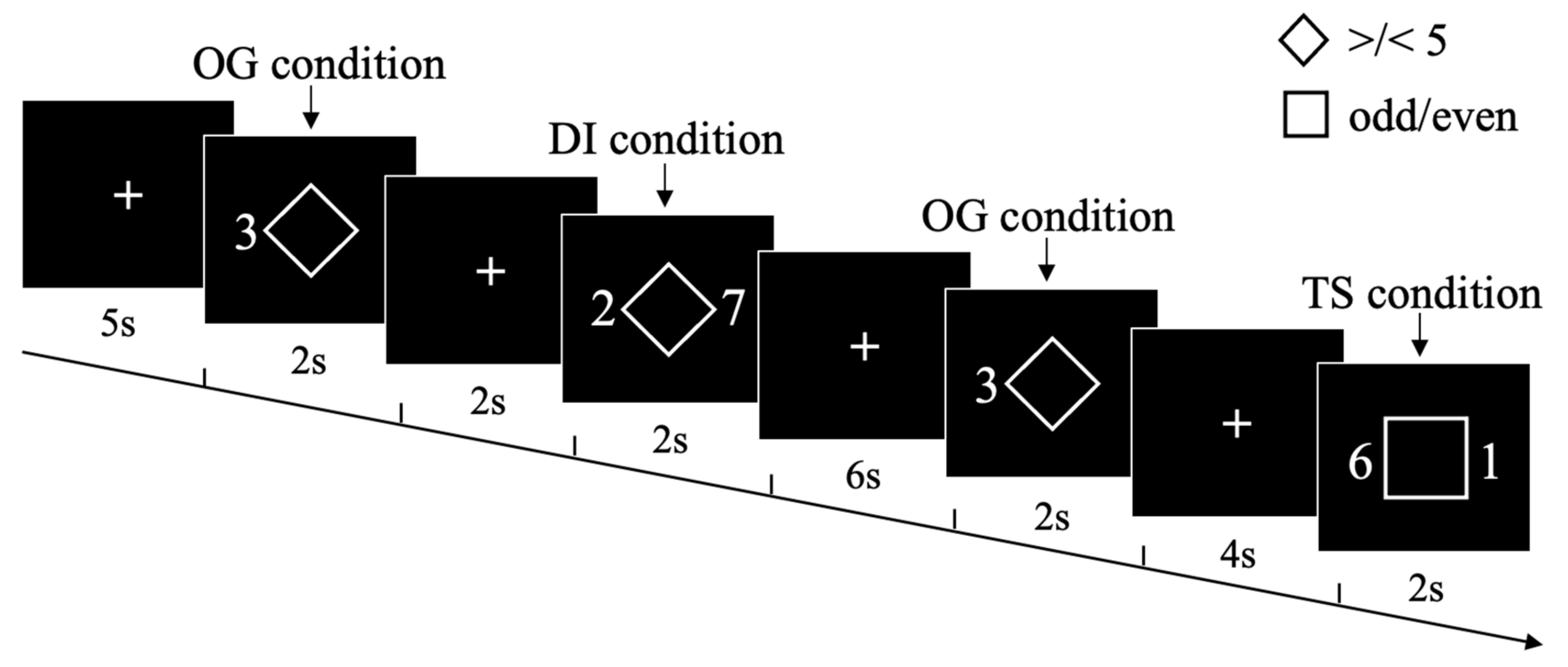
2.3. Experimental Design and Procedures
2.4. fMRI Data Acquisition
2.5. Statistical Analysis of Behavioral Data
2.6. fMRI Data Preprocessing and Statistical Analysis
2.7. Relationship between Abnormal Activation, Behavioral and Neuropsychological Measures in mTBI
2.8. Mediation Analysis between Abnormal Dorsal Caudate Activation and Cognitive Flexibility in mTBI
3. Results
3.1. Demographics and Neuropsychological Assessment
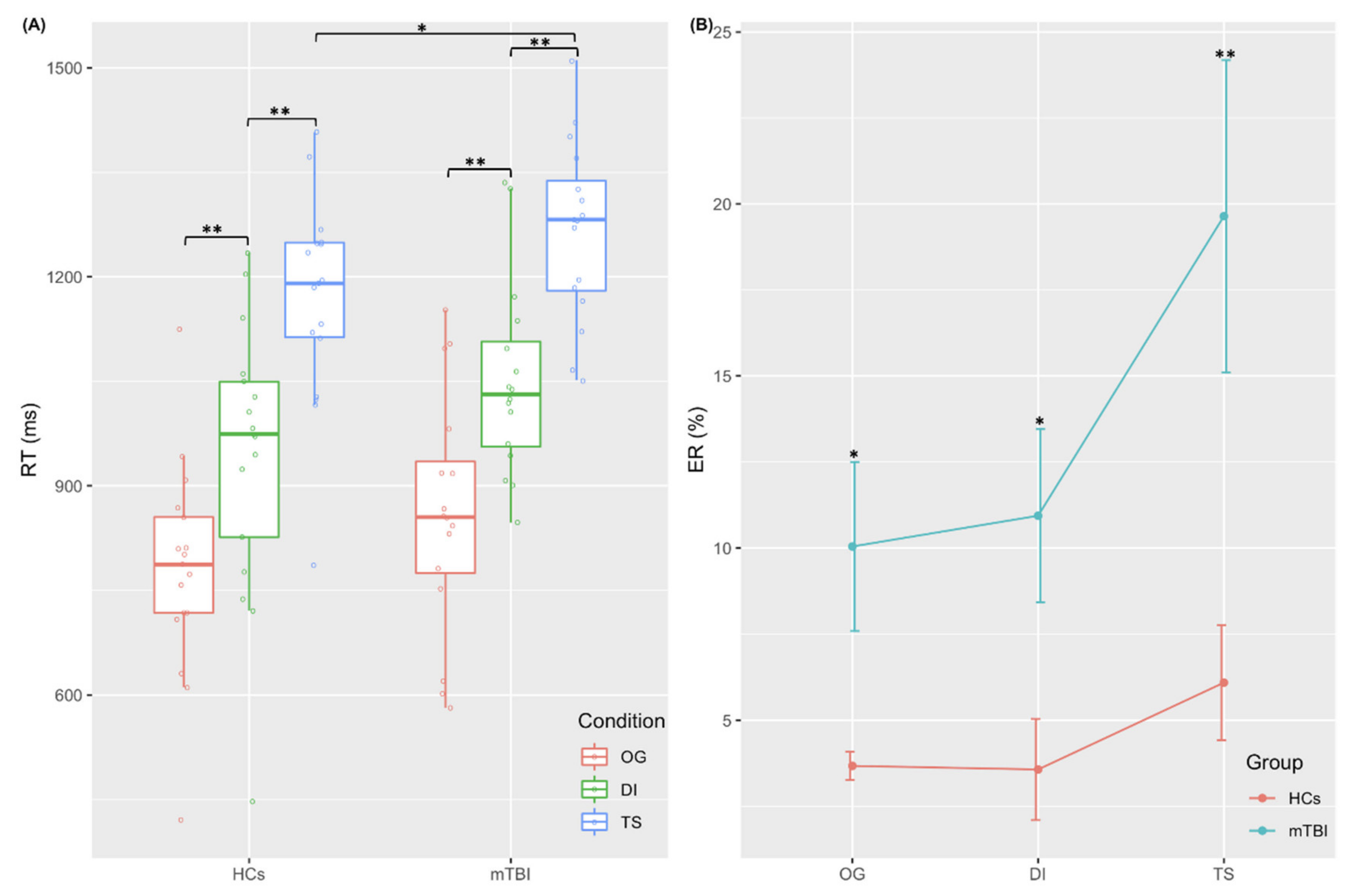
3.2. fMRI Behavioral Performance
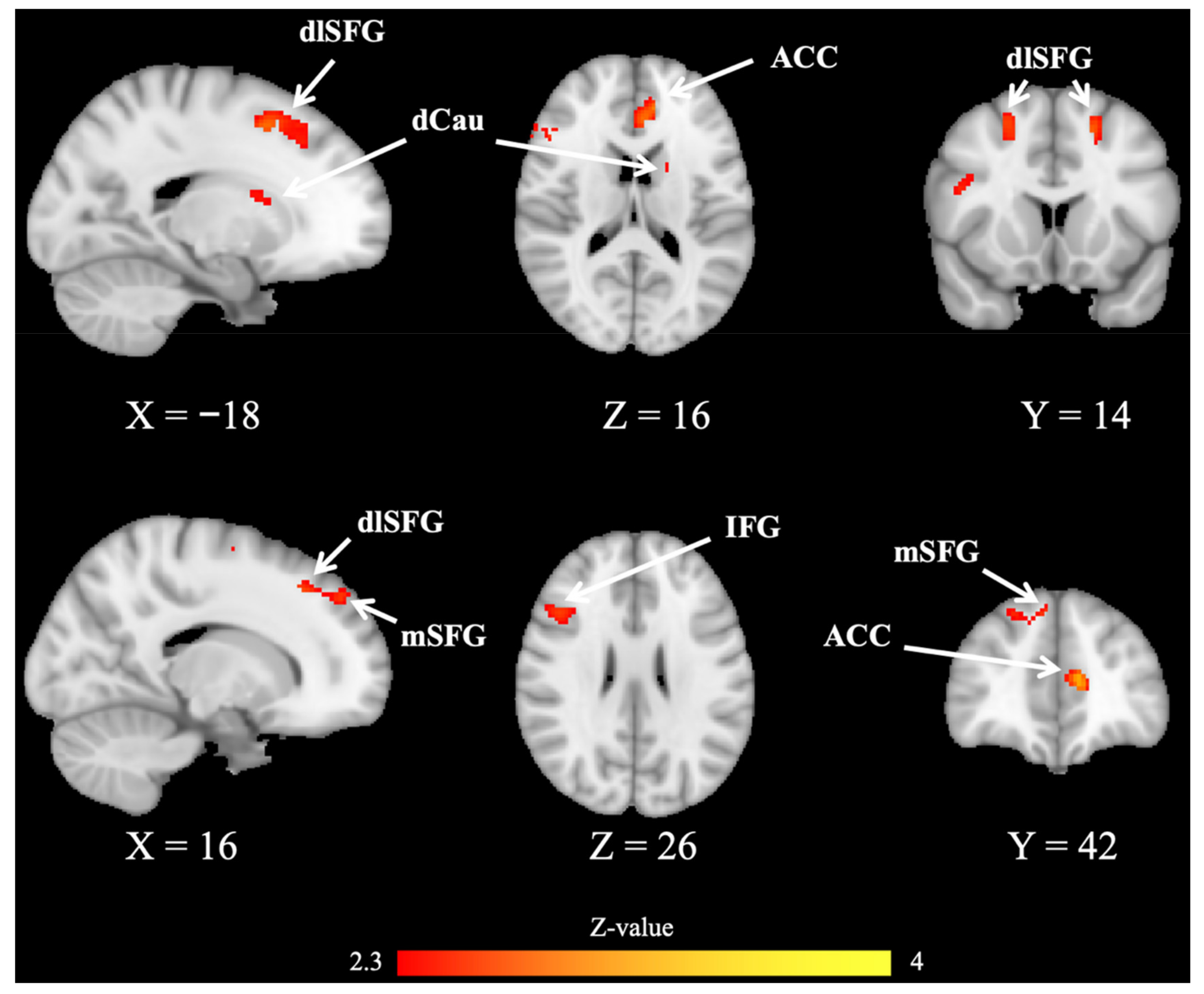
3.3. fMRI Brain Imaging Results
3.4. Relationship between Abnormal Activation, Behavioral and Neuropsychological Measures in mTBI
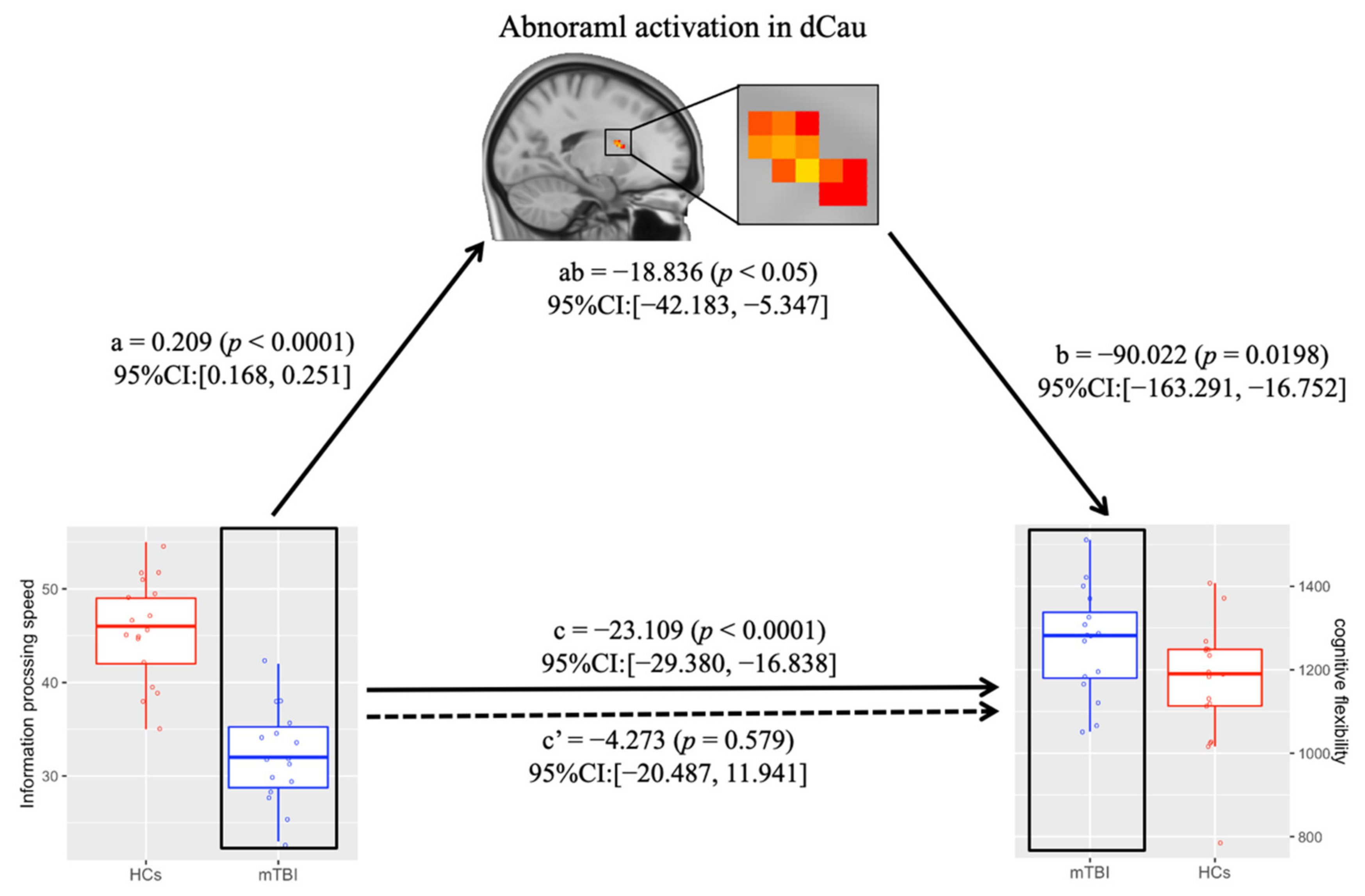
3.5. Abnormal Dorsal Caudate Activation Mediates the Relationship between Information Processing Speed and Cognitive Flexibility in mTBI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Xu, H.; Tao, Y.; Zhu, P.; Li, D.; Zhang, M.; Bai, G.; Yin, B. Restoration of aberrant shape of caudate sub-regions associated with cognitive function improvement in mild traumatic brain injury. J. Neurotrauma 2022, 39, 348–357. [Google Scholar] [CrossRef] [PubMed]
- Bruns, J., Jr.; Hauser, W.A. The epidemiology of traumatic brain injury: A review. Epilepsia 2003, 44, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Capizzi, A.; Woo, J.; Verduzco-Gutierrez, M. Traumatic Brain Injury: An Overview of Epidemiology, Pathophysiology, and Medical Management. Med. Clin. N. Am. 2020, 104, 213–238. [Google Scholar] [CrossRef] [PubMed]
- Holm, L.; Cassidy, J.D.; Carroll, L.J.; Borg, J. Neurotrauma Task Force on Mild Traumatic Brain Injury of the WHO Collaborating Centre. Summary of the WHO Collaborating Centre for Neurotrauma Task Force on Mild Traumatic Brain Injury. J. Rehabil. Med. 2005, 37, 137–141. [Google Scholar] [CrossRef] [Green Version]
- Gilbert, S.J.; Burgess, P.W. Executive function. Curr. Biol. 2008, 18, R110–R114. [Google Scholar] [CrossRef] [Green Version]
- Friedman, N.P.; Robbins, T.W. The role of prefrontal cortex in cognitive control and executive function. Neuropsychopharmacology 2022, 47, 72–89. [Google Scholar] [CrossRef]
- Ridderinkhof, K.R.; Ullsperger, M.; Crone, E.A.; Nieuwenhuis, S. The role of the medial frontal cortex in cognitive control. Science 2004, 306, 443–447. [Google Scholar] [CrossRef]
- Chamberlain, S.R.; Fineberg, N.A.; Blackwell, A.D.; Robbins, T.W.; Sahakian, B.J. Motor inhibition and cognitive flexibility in obsessive-compulsive disorder and trichotillomania. Am. J. Psychiatry 2006, 163, 1282–1284. [Google Scholar] [CrossRef]
- Chamberlain, S.R.; Fineberg, N.A.; Menzies, L.A.; Blackwell, A.D.; Bullmore, E.T.; Robbins, T.W.; Sahakian, B.J. Impaired cognitive flexibility and motor inhibition in unaffected first-degree relatives of patients with obsessive-compulsive disorder. Am. J. Psychiatry 2007, 164, 335–338. [Google Scholar] [CrossRef]
- Ersche, K.D.; Barnes, A.; Jones, P.S.; Morein-Zamir, S.; Robbins, T.W.; Bullmore, E.T. Abnormal structure of frontostriatal brain systems is associated with aspects of impulsivity and compulsivity in cocaine dependence. Brain 2011, 134, 2013–2024. [Google Scholar] [CrossRef] [Green Version]
- Moreno-Lopez, L.; Catena, A.; Fernandez-Serrano, M.J.; Delgado-Rico, E.; Stamatakis, E.A.; Perez-Garcia, M.; Verdejo-Garcia, A. Trait impulsivity and prefrontal gray matter reductions in cocaine dependent individuals. Drug Alcohol Depend. 2012, 125, 208–214. [Google Scholar] [CrossRef]
- Vaghi, M.M.; Vertes, P.E.; Kitzbichler, M.G.; Apergis-Schoute, A.M.; van der Flier, F.E.; Fineberg, N.A.; Sule, A.; Zaman, R.; Voon, V.; Kundu, P.; et al. Specific Frontostriatal Circuits for Impaired Cognitive Flexibility and Goal-Directed Planning in Obsessive-Compulsive Disorder: Evidence From Resting-State Functional Connectivity. Biol. Psychiatry 2017, 81, 708–717. [Google Scholar] [CrossRef] [Green Version]
- Fagerholm, E.D.; Hellyer, P.J.; Scott, G.; Leech, R.; Sharp, D.J. Disconnection of network hubs and cognitive impairment after traumatic brain injury. Brain 2015, 138, 1696–1709. [Google Scholar] [CrossRef] [Green Version]
- Wylie, G.R.; Dobryakova, E.; DeLuca, J.; Chiaravalloti, N.; Essad, K.; Genova, H. Cognitive fatigue in individuals with traumatic brain injury is associated with caudate activation. Sci. Rep. 2017, 7, 8973. [Google Scholar] [CrossRef]
- Leunissen, I.; Coxon, J.P.; Caeyenberghs, K.; Michiels, K.; Sunaert, S.; Swinnen, S.P. Subcortical volume analysis in traumatic brain injury: The importance of the fronto-striato-thalamic circuit in task switching. Cortex 2014, 51, 67–81. [Google Scholar] [CrossRef]
- Leunissen, I.; Coxon, J.P.; Caeyenberghs, K.; Michiels, K.; Sunaert, S.; Swinnen, S.P. Task switching in traumatic brain injury relates to cortico-subcortical integrity. Hum. Brain Mapp. 2014, 35, 2459–2469. [Google Scholar] [CrossRef]
- Grant, D.A.; Berg, E.A. A behavioral analysis of degree of reinforcement and ease of shifting to new responses in a Weigl-type card-sorting problem. J. Exp. Psychol. 1948, 38, 404–411. [Google Scholar] [CrossRef]
- Ozen, L.J.; Fernandes, M.A. Effects of “diagnosis threat” on cognitive and affective functioning long after mild head injury. J. Int. Neuropsychol. Soc. 2011, 17, 219–229. [Google Scholar] [CrossRef] [Green Version]
- Suhr, J.A.; Gunstad, J. “Diagnosis Threat”: The effect of negative expectations on cognitive performance in head injury. J. Clin. Exp. Neuropsychol. 2002, 24, 448–457. [Google Scholar] [CrossRef]
- Dobryakova, E.; Boukrina, O.; Wylie, G.R. Investigation of Information Flow During a Novel Working Memory Task in Individuals with Traumatic Brain Injury. Brain Connect. 2015, 5, 433–441. [Google Scholar] [CrossRef]
- Fischer-Baum, S.; Miozzo, M.; Laiacona, M.; Capitani, E. Perseveration during verbal fluency in traumatic brain injury reflects impairments in working memory. Neuropsychology 2016, 30, 791–799. [Google Scholar] [CrossRef] [PubMed]
- Sandry, J.; DeLuca, J.; Chiaravalloti, N. Working memory capacity links cognitive reserve with long-term memory in moderate to severe TBI: A translational approach. J. Neurol. 2015, 262, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Bonnelle, V.; Ham, T.E.; Leech, R.; Kinnunen, K.M.; Mehta, M.A.; Greenwood, R.J.; Sharp, D.J. Salience network integrity predicts default mode network function after traumatic brain injury. Proc. Natl. Acad. Sci. USA 2012, 109, 4690–4695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharp, D.J.; Beckmann, C.F.; Greenwood, R.; Kinnunen, K.M.; Bonnelle, V.; De Boissezon, X.; Powell, J.H.; Counsell, S.J.; Patel, M.C.; Leech, R. Default mode network functional and structural connectivity after traumatic brain injury. Brain 2011, 134, 2233–2247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armbruster, D.J.; Ueltzhoffer, K.; Basten, U.; Fiebach, C.J. Prefrontal cortical mechanisms underlying individual differences in cognitive flexibility and stability. J. Cogn. Neurosci. 2012, 24, 2385–2399. [Google Scholar] [CrossRef] [Green Version]
- Armbruster-Genc, D.J.; Ueltzhoffer, K.; Fiebach, C.J. Brain Signal Variability Differentially Affects Cognitive Flexibility and Cognitive Stability. J. Neurosci. 2016, 36, 3978–3987. [Google Scholar] [CrossRef] [Green Version]
- Sekutowicz, M.; Schmack, K.; Steimke, R.; Paschke, L.; Sterzer, P.; Walter, H.; Stelzel, C. Striatal activation as a neural link between cognitive and perceptual flexibility. Neuroimage 2016, 141, 393–398. [Google Scholar] [CrossRef]
- Hartmann, T.; Weisz, N. An Introduction to the Objective Psychophysics Toolbox. Front. Psychol. 2020, 11, 585437. [Google Scholar] [CrossRef]
- Brainard, D.H. The Psychophysics Toolbox. Spat. Vis. 1997, 10, 433–436. [Google Scholar] [CrossRef] [Green Version]
- Woolrich, M.W.; Ripley, B.D.; Brady, M.; Smith, S.M. Temporal autocorrelation in univariate linear modeling of FMRI data. NeuroImage 2001, 14, 1370–1386. [Google Scholar] [CrossRef] [Green Version]
- Xu, H.; Chen, Y.; Tao, Y.; Zhang, Y.; Zhao, T.; Wang, M.; Fan, L.; Zheng, Y.; Guo, C. Modulation effect of acupuncture treatment on chronic neck and shoulder pain in female patients: Evidence from periaqueductal gray-based functional connectivity. CNS Neurosci. Ther. 2022, 28, 714–723. [Google Scholar] [CrossRef]
- Woolrich, M.W.; Behrens, T.E.; Beckmann, C.F.; Jenkinson, M.; Smith, S.M. Multilevel linear modelling for FMRI group analysis using Bayesian inference. NeuroImage 2004, 21, 1732–1747. [Google Scholar] [CrossRef]
- Chen, G.; Saad, Z.S.; Nath, A.R.; Beauchamp, M.S.; Cox, R.W. FMRI group analysis combining effect estimates and their variances. NeuroImage 2012, 60, 747–765. [Google Scholar] [CrossRef] [Green Version]
- Hayes, A.F.; Preacher, K.J. Statistical mediation analysis with a multicategorical independent variable. Br. J. Math. Stat. Psychol. 2014, 67, 451–470. [Google Scholar] [CrossRef]
- Preacher, K.J.; Rucker, D.D.; Hayes, A.F. Addressing Moderated Mediation Hypotheses: Theory, Methods, and Prescriptions. Multivar. Behav. Res. 2007, 42, 185–227. [Google Scholar] [CrossRef]
- Esechie, A.; Bhardwaj, A.; Masel, T.; Raji, M. Neurocognitive sequela of burn injury in the elderly. J. Clin. Neurosci. 2019, 59, 1–5. [Google Scholar] [CrossRef]
- Pollicina, I.; Maniaci, A.; Lechien, J.R.; Iannella, G.; Vicini, C.; Cammaroto, G.; Cannavicci, A.; Magliulo, G.; Pace, A.; Cocuzza, S.; et al. Neurocognitive Performance Improvement after Obstructive Sleep Apnea Treatment: State of the Art. Behav. Sci. 2021, 11, 180. [Google Scholar] [CrossRef]
- Alvarez, J.A.; Emory, E. Executive function and the frontal lobes: A meta-analytic review. Neuropsychol. Rev. 2006, 16, 17–42. [Google Scholar] [CrossRef]
- Cummings, J.L. Frontal-subcortical circuits and human behavior. J. Psychosom Res. 1998, 44, 627–628. [Google Scholar] [CrossRef]
- Mega, M.S.; Cummings, J.L. Frontal-subcortical circuits and neuropsychiatric disorders. J. Neuropsychiatry Clin. Neurosci. 1994, 6, 358–370. [Google Scholar] [CrossRef]
- Wager, T.D.; Davidson, M.L.; Hughes, B.L.; Lindquist, M.A.; Ochsner, K.N. Prefrontal-subcortical pathways mediating successful emotion regulation. Neuron 2008, 59, 1037–1050. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reverberi, C.; Toraldo, A.; D’Agostini, S.; Skrap, M. Better without (lateral) frontal cortex? Insight problems solved by frontal patients. Brain 2005, 128, 2882–2890. [Google Scholar] [CrossRef] [PubMed]
- Shimamura, A.P.; Janowsky, J.S.; Squire, L.R. Memory for the temporal order of events in patients with frontal lobe lesions and amnesic patients. Neuropsychologia 1990, 28, 803–813. [Google Scholar] [CrossRef]
- Hahn, B.; Ross, T.J.; Stein, E.A. Cingulate activation increases dynamically with response speed under stimulus unpredictability. Cereb. Cortex 2007, 17, 1664–1671. [Google Scholar] [CrossRef] [Green Version]
- Kaiser, R.H.; Andrews-Hanna, J.R.; Wager, T.D.; Pizzagalli, D.A. Large-Scale Network Dysfunction in Major Depressive Disorder: A Meta-analysis of Resting-State Functional Connectivity. JAMA Psychiatry 2015, 72, 603–611. [Google Scholar] [CrossRef]
- Small, D.M.; Gitelman, D.R.; Gregory, M.D.; Nobre, A.C.; Parrish, T.B.; Mesulam, M.M. The posterior cingulate and medial prefrontal cortex mediate the anticipatory allocation of spatial attention. NeuroImage 2003, 18, 633–641. [Google Scholar] [CrossRef]
- Xu, H.; Seminowicz, D.A.; Krimmel, S.R.; Zhang, M.; Gao, L.; Wang, Y. Altered Structural and Functional Connectivity of Salience Network in Patients with Classic Trigeminal Neuralgia. J. Pain 2022, in press. [CrossRef]
- Kemp, J.M.; Powell, T.P. The cortico-striate projection in the monkey. Brain 1970, 93, 525–546. [Google Scholar] [CrossRef]
- Yeterian, E.H.; Van Hoesen, G.W. Cortico-striate projections in the rhesus monkey: The organization of certain cortico-caudate connections. Brain Res. 1978, 139, 43–63. [Google Scholar] [CrossRef]
- Ham, T.E.; de Boissezon, X.; Leff, A.; Beckmann, C.; Hughes, E.; Kinnunen, K.M.; Leech, R.; Sharp, D.J. Distinct frontal networks are involved in adapting to internally and externally signaled errors. Cereb. Cortex 2013, 23, 703–713. [Google Scholar] [CrossRef]
- Heyder, K.; Suchan, B.; Daum, I. Cortico-subcortical contributions to executive control. Acta Psychol. 2004, 115, 271–289. [Google Scholar] [CrossRef]
- Kerns, J.G.; Cohen, J.D.; MacDonald, A.W., 3rd; Cho, R.Y.; Stenger, V.A.; Carter, C.S. Anterior cingulate conflict monitoring and adjustments in control. Science 2004, 303, 1023–1026. [Google Scholar] [CrossRef] [Green Version]
- Shenhav, A.; Botvinick, M.M.; Cohen, J.D. The expected value of control: An integrative theory of anterior cingulate cortex function. Neuron 2013, 79, 217–240. [Google Scholar] [CrossRef] [Green Version]
- O’Reilly, R.C.; Frank, M.J. Making working memory work: A computational model of learning in the prefrontal cortex and basal ganglia. Neural. Comput. 2006, 18, 283–328. [Google Scholar] [CrossRef]
- Wiecki, T.V.; Frank, M.J. A computational model of inhibitory control in frontal cortex and basal ganglia. Psychol. Rev. 2013, 120, 329–355. [Google Scholar] [CrossRef] [Green Version]
- Xu, H.; Wang, X.; Chen, Z.; Bai, G.; Yin, B.; Wang, S.; Sun, C.; Gan, S.; Wang, Z.; Cao, J.; et al. Longitudinal Changes of Caudate-Based Resting State Functional Connectivity in Mild Traumatic Brain Injury. Front. Neurol. 2018, 9, 467. [Google Scholar] [CrossRef] [Green Version]
- De Simoni, S.; Jenkins, P.O.; Bourke, N.J.; Fleminger, J.J.; Hellyer, P.J.; Jolly, A.E.; Patel, M.C.; Cole, J.H.; Leech, R.; Sharp, D.J. Altered caudate connectivity is associated with executive dysfunction after traumatic brain injury. Brain 2018, 141, 148–164. [Google Scholar] [CrossRef] [Green Version]
- Wylie, G.R.; Flashman, L.A. Understanding the interplay between mild traumatic brain injury and cognitive fatigue: Models and treatments. Concussion 2017, 2, CNC50. [Google Scholar] [CrossRef]
- Dajani, D.R.; Uddin, L.Q. Demystifying cognitive flexibility: Implications for clinical and developmental neuroscience. Trends Neurosci. 2015, 38, 571–578. [Google Scholar] [CrossRef] [Green Version]
- McCabe, D.P.; Roediger, H.L.; McDaniel, M.A.; Balota, D.A.; Hambrick, D.Z. The relationship between working memory capacity and executive functioning: Evidence for a common executive attention construct. Neuropsychology 2010, 24, 222–243. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| mTBI Patients (n = 16) | HCs (n = 17) | t/χ2 Test | p-Value | |
|---|---|---|---|---|
| Demographic characteristics | ||||
| Age (years) | 25.8 ± 2.8 | 27.8 ± 3.3 | −1.897 | 0.067 |
| Sex (F/M) | 6/10 | 5/12 | 0.243 | 0.622 |
| Handedness (L/R) | 0/16 | 0/17 | ||
| Education level (years) | 13.9 ± 1.3 | 13.6 ± 1.6 | 0.316 | 0.754 |
| Time post injury (days) | 2.7 ± 1.3 | - | - | - |
| Injury severity (n(%)) | ||||
| GCS = 15 | 16(100%) | - | - | - |
| loss of conscious < 30 min | 16(100%) | - | - | - |
| post-traumatic amnesia < 24 h | 16(100%) | - | - | - |
| Injury causes (n(%)) | ||||
| Traffic accident | 6(37.5%) | - | - | - |
| Fall | 5(31.2%) | - | - | - |
| Assault | 3(18.8%) | - | - | - |
| Others | 2(12.5%) | - | - | - |
| Information processing speed | ||||
| TMA-A score | 50.0 ± 8.8 | 48.6 ± 8.1 | 0.461 | 0.648 |
| DSC score | 32.2 ± 5.1 | 45.7 ± 5.5 | −7.343 | p < 0.001 |
| Working memory | ||||
| FDS score | 8.5 ± 0.8 | 7.9 ± 1.1 | 1.874 | 0.07 |
| BDS score | 4.3 ± 0.8 | 3.8 ± 0.8 | 2.036 | 0.051 |
| Self-reported symptom | ||||
| ISI score | 7.1 ± 2.1 | 2.1 ± 1.1 | 8.704 | p < 0.01 |
| HIT score | 48.1 ± 4.3 | 38.6 ± 6.1 | 5.091 | p < 0.01 |
| Brain Regions | Hemisphere | BA | Peak MNI Coordinates | Z-Value | Size (Voxels) | ||
|---|---|---|---|---|---|---|---|
| x | y | z | |||||
| dCau | L | NA | −18 | 8 | 14 | 2.638 | 112 |
| dlSFG | L | 8 | −18 | 10 | 50 | 3.005 | 177 |
| R | 6, 8 | 20 | −6 | 64 | 3.295 | 421 | |
| mSFG | R | 91 | 8 | 46 | 42 | 3.201 | 154 |
| IFG | R | 44, 45 | 44 | 10 | 20 | 3.109 | 268 |
| ACC | L | 32 | −10 | 40 | 12 | 3.549 | 210 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, H.; Zhang, X.; Bai, G. Abnormal Dorsal Caudate Activation Mediated Impaired Cognitive Flexibility in Mild Traumatic Brain Injury. J. Clin. Med. 2022, 11, 2484. https://doi.org/10.3390/jcm11092484
Xu H, Zhang X, Bai G. Abnormal Dorsal Caudate Activation Mediated Impaired Cognitive Flexibility in Mild Traumatic Brain Injury. Journal of Clinical Medicine. 2022; 11(9):2484. https://doi.org/10.3390/jcm11092484
Chicago/Turabian StyleXu, Hui, Xiuping Zhang, and Guanghui Bai. 2022. "Abnormal Dorsal Caudate Activation Mediated Impaired Cognitive Flexibility in Mild Traumatic Brain Injury" Journal of Clinical Medicine 11, no. 9: 2484. https://doi.org/10.3390/jcm11092484
APA StyleXu, H., Zhang, X., & Bai, G. (2022). Abnormal Dorsal Caudate Activation Mediated Impaired Cognitive Flexibility in Mild Traumatic Brain Injury. Journal of Clinical Medicine, 11(9), 2484. https://doi.org/10.3390/jcm11092484