
Atrial Function Impairments after Pediatric Cardiac Surgery Evaluated by STE Analysis


 ,
,  ,
,  ,
, 

Abstract
:1. Introduction
2. Methods
Statistical Analysis
3. Results
3.1. Population
3.2. Feasibility
3.3. Comparison vs. Normal Subjects
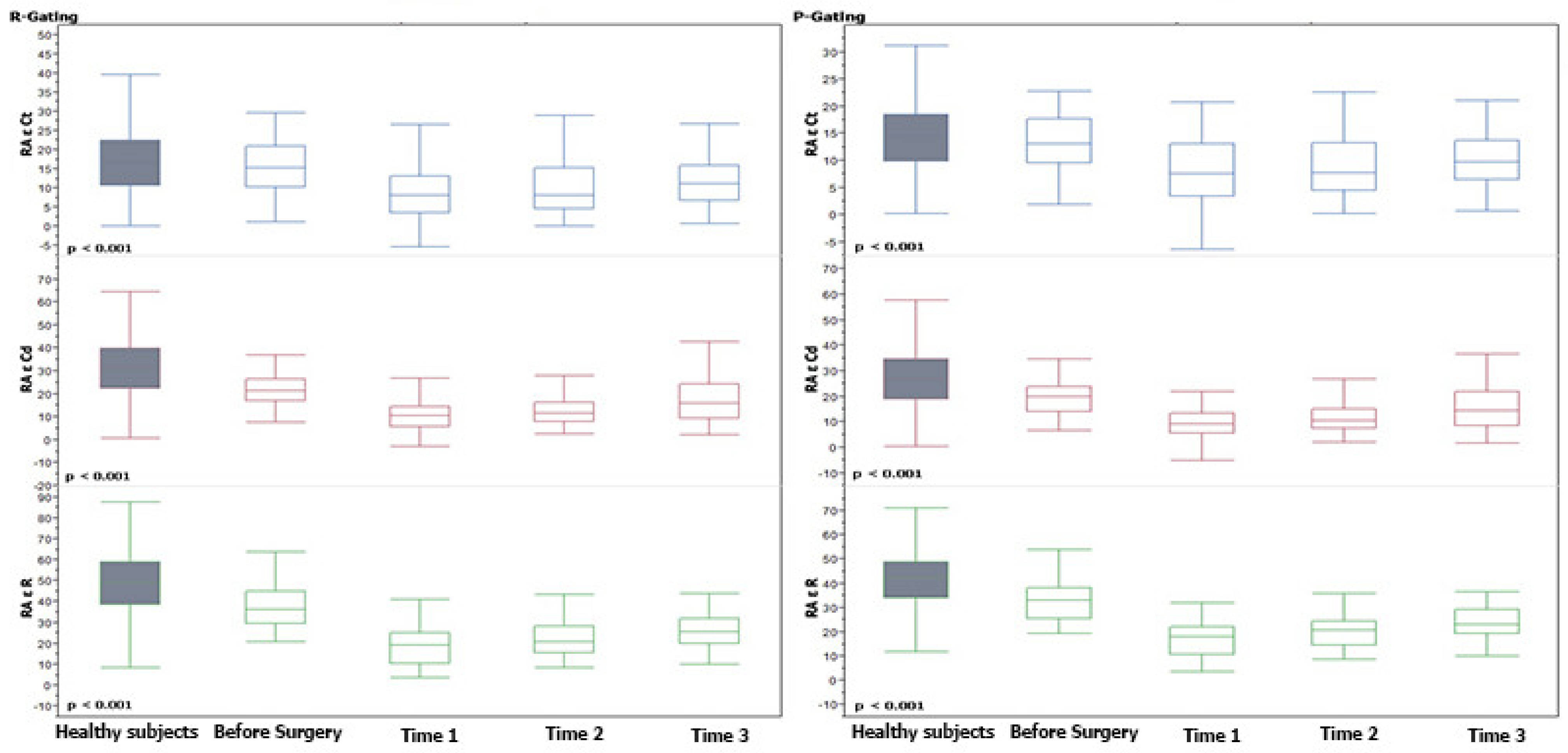
3.4. The Post-Operative Trend for Atrial STE ε
3.5. Comparison of Post-Operative Trend for Atrial STE ε with Pre-Operative Values
3.6. Differences among P- and R-Gating Post-Operative ε Values
3.7. Differences among Age Groups
3.8. Correlation of Atrial Strain with Operative Data and Outcome Parameters
3.9. Correlation of Atrial Strain with Left and Right Ventricular STE
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Avesani, M.; Borrelli, N.; Krupickova, S.; Sabatino, J.; Donne, G.D.; Ibrahim, A.; Piccinelli, E.; Josen, M.; Michielon, G.; Fraisse, A.; et al. Echocardiography and cardiac magnetic resonance in children with repaired tetralogy of Fallot: New insights in cardiac mechanics and exercise capacity. Int. J. Cardiol. 2020, 321, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Cheung, Y.-F.; Yu, C.K.; So, E.K.; Li, V.W.; Wong, W.H. Atrial Strain Imaging after Repair of Tetralogy of Fallot: A Systematic Review. Ultrasound Med. Biol. 2019, 45, 1896–1908. [Google Scholar] [CrossRef] [PubMed]
- Bárczi, A.; Lakatos, B.K.; Szilágyi, M.; Kis, É.; Cseprekál, O.; Fábián, A.; Kovács, A.; Szabó, A.J.; Merkely, B.; Salvi, P.; et al. Subclinical cardiac dysfunction in pediatric kidney transplant recipients identified by speckle-tracking echocardiography. Pediatr. Nephrol. 2022, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Pletzer, S.A.; Atz, A.M.; Chowdhury, S.M. The Relationship between Pre-operative Left Ventricular Longitudinal Strain and Post-operative Length of Stay in Patients Undergoing Arterial Switch Operation Is Age Dependent. Pediatr. Cardiol. 2018, 40, 366–373. [Google Scholar] [CrossRef]
- Perdreau, E.; Séguéla, P.-E.; Jalal, Z.; Perdreau, A.; Mouton, J.-B.; Nelson-Veniard, M.; Guillet, E.; Iriart, X.; Ouattara, A.; Roubertie, F.; et al. Postoperative assessment of left ventricular function by two-dimensional strain (speckle tracking) after paediatric cardiac surgery. Arch. Cardiovasc. Dis. 2016, 109, 599–606. [Google Scholar] [CrossRef]
- Karsenty, C.; Hadeed, K.; Dulac, Y.; Semet, F.; Alacoque, X.; Breinig, S.; Leobon, B.; Acar, P.; Hascoet, S. Two-dimensional right ventricular strain by speckle tracking for assessment of longitudinal right ventricular function after paediatric congenital heart disease surgery. Arch. Cardiovasc. Dis. 2017, 110, 157–166. [Google Scholar] [CrossRef]
- Di Salvo, G.; Drago, M.; Pacileo, G.; Rea, A.; Carrozza, M.; Santoro, G.; Bigazzi, M.C.; Caso, P.; Russo, M.G.; Carminati, M.; et al. Atrial function after surgical and percutaneous closure of atrial septal defect: A strain rate imaging study. J. Am. Soc. Echocardiogr. 2005, 18, 930–933. [Google Scholar] [CrossRef]
- Hajizeinali, A.; Iri, M.; Hosseinsabet, A. Assessment of the Right and Left Atrial Functions at Midterm after Surgical and Device Atrial Septal Defect Closure: A 2-Dimensional Speckle-Tracking Echocardiographic Study. J. Ultrasound Med. 2019, 38, 1979–1993. [Google Scholar] [CrossRef]
- Cantinotti, M.; Scalese, M.; Giordano, R.; Franchi, E.; Assanta, N.; Molinaro, S.; Iervasi, G.; Santoro, G.; Koestenberger, M.; Kutty, S. Left and Right Atrial Strain in Healthy Caucasian Children by Two-Dimensional Speckle-Tracking Echocardiography. J. Am. Soc. Echocardiogr. 2019, 32, 165–168.e3. [Google Scholar] [CrossRef] [Green Version]
- Kutty, S.; Padiyath, A.; Li, L.; Peng, Q.; Rangamani, S.; Schuster, A.; Danford, D.A. Functional Maturation of Left and Right Atrial Systolic and Diastolic Performance in Infants, Children, and Adolescents. J. Am. Soc. Echocardiogr. 2013, 26, 398–409.e2. [Google Scholar] [CrossRef]
- Ghelani, S.J.; Brown, D.W.; Kuebler, J.D.; Perrin, D.; Shakti, D.; Williams, D.N.; Marx, G.R.; Colan, S.D.; Geva, T.; Harrild, D.M. Left Atrial Volumes and Strain in Healthy Children Measured by Three-Dimensional Echocardiography: Normal Values and Maturational Changes. J. Am. Soc. Echocardiogr. 2018, 31, 187–193.e1. [Google Scholar] [CrossRef] [PubMed]
- Marchese, P.; Scalese, M.; Giordano, R.; Assanta, N.; Franchi, E.; Koestenberger, M.; Ravaglioli, A.; Kutty, S.; Cantinotti, M. Pediatric ranges of normality for 2D speckle-tracking echocardiography atrial strain: Differences between p- and r-gating and among new (Atrial Designed) and conventional (Ventricular Specific) software’s. Echocardiography 2021, 38, 2025–2031. [Google Scholar] [CrossRef] [PubMed]
- Badano, L.P.; Kolias, T.J.; Muraru, D.; Abraham, T.P.; Aurigemma, G.; Edvardsen, T.; D’Hooge, J.; Donal, E.; Fraser, A.G.; Marwick, T.; et al. Standardization of left atrial, right ventricular, and right atrial deformation imaging using two-dimensional speckle tracking echocardiography: A consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 591–600. [Google Scholar] [CrossRef] [PubMed]
- Cantinotti, M.; Scalese, M.; Giordano, R.; Franchi, E.; Assanta, N.; Marotta, M.; Viacava, C.; Molinaro, S.; Iervasi, G.; Santoro, G.; et al. Normative Data for Left and Right Ventricular Systolic Strain in Healthy Caucasian Italian Children by Two-Dimensional Speckle-Tracking Echocardiography. J. Am. Soc. Echocardiogr. 2018, 31, 712–720.e6. [Google Scholar] [CrossRef] [PubMed]
- Moustafa, S.; Zuhairy, H.; Youssef, M.A.; Alvarez, N.; Connelly, M.S.; Prieur, T.; Mookadam, F. Right and Left Atrial Dissimilarities in Normal Subjects Explored by Speckle Tracking Echocardiography. Echocardiography 2015, 32, 1392–1399. [Google Scholar] [CrossRef]
- Atas, H.; Kepez, A.; Tigen, K.; Samadov, F.; Ozen, G.; Cincin, A.; Sunbul, M.; Bozbay, M.; Direskeneli, H.; Basaran, Y. Evaluation of left atrial volume and function in systemic sclerosis patients using speckle tracking and real-time three-dimensional echocardiography. Anatol. J. Cardiol. 2016, 16, 316–322. [Google Scholar] [CrossRef]
- De Boer, J.M.; Kuipers, I.M.; Klitsie, L.M.; Blom, N.A.; Ten Harkel, A.D. Decreased biventricular longitudinal strain shortly after congenital heart defect surgery. Echocardiography 2017, 34, 446–452. [Google Scholar] [CrossRef]
- Fung, M.J.; Thomas, L.; Leung, D.Y. Left atrial function: Correlation with left ventricular function and contractile reserve in patients with hypertension. Echocardiography 2018, 35, 1596–1605. [Google Scholar] [CrossRef]
- Ramkumar, S.; Yang, H.; Wang, Y.; Nolan, M.; Negishi, T.; Negishi, K.; Marwick, T.H. Association of the Active and Passive Components of Left Atrial Deformation with Left Ventricular Function. J. Am. Soc. Echocardiogr. 2017, 30, 659–666. [Google Scholar] [CrossRef]
- Loar, R.W.; Pignatelli, R.H.; Morris, S.A.; Colquitt, J.L.; Feagin, D.K.; Denfield, S.W.; Tunuguntla, H.P. Left Atrial Strain Correlates with Elevated Filling Pressures in Pediatric Heart Transplantation Recipients. J. Am. Soc. Echocardiogr. 2020, 33, 504–511.e1. [Google Scholar] [CrossRef]
- Sabatino, J.; Di Salvo, G.; Prota, C.; Bucciarelli, V.; Josen, M.; Paredes, J.; Borrelli, N.; Sirico, D.; Prasad, S.; Indolfi, C.; et al. Left Atrial Strain to Identify Diastolic Dysfunction in Children with Cardiomyopathies. J. Clin. Med. 2019, 8, 1243. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Older (nr 64) | Infant (nr 37) | Neonates (nr 30) | Total (nr 131) | ||
|---|---|---|---|---|---|
| Mean | Mean | Mean | Mean | p | |
| Age (years) | 3.23 ± 3.64 | 0.28 ± 0.13 | 0.03 ± 0.03 | 1.69 ± 2.98 | <0.0001 * |
| BSA (m2) | 0.57 ± 0.31 | 0.28 ± 0.06 | 0.21 ± 0.02 | 0.41 ± 0.28 | <0.0001 * |
| CPB (min) | 1.52 ± 0.75 | 1.6 ± 0.85 | 2.24 ± 1.16 | 1.69 ± 0.91 | <0.0001 * |
| STAT-score | 95.82 ± 46.38 | 93.97 ± 59.22 | 134.11 ± 99.79 | 103.96 ± 66.8 | 0.043 * |
| Extubation Time (days) | 1.09 ± 1.22 | 2.74 ± 2.46 | 5.16 ± 5.77 | 2.48 ± 6.54 | 0.0389 * |
| ICU LOS (days) | 10.19 ± 48.14 | 7.24 ± 7.15 | 10.67 ± 8.05 | 9.5 ± 34.75 | 0.023 * |
| Major complications | 1 § | 2 ° | 3 * | 6 | |
| CHD Numerosity | |||||
| LVVO (nr) | 18 | 17 | 2 | 37 | |
| RVPO (nr) | 20 | 9 | 1 | 30 | |
| TGA (nr) | 0 | 3 | 18 | 21 | |
| LVPO (nr) | 8 | 2 | 9 | 19 | |
| RVVO (nr) | 12 | 3 | 0 | 15 | |
| AVSD (nr) | 6 | 2 | 0 | 7 | |
| Others (nr) | 0 | 1 | 0 | 1 | |
| Total | 64 | 37 | 30 | 131 | |
| Time 1 | Time 2 | Time 3 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| % | Neonates | Infant | Older | Neonates | Infant | Older | Neonates | Infant | Older |
| LARε | 80.0% | 85.2% | 72.1% | 84.8% | 80.0% | 76.0% | 70.4% | 82.1% | 61.9% |
| LACTε | 80.0% | 82.0% | 72.1% | 84.8% | 80.0% | 74.7% | 70.4% | 75.0% | 61.9% |
| RARε | 80.0% | 78.7% | 70.6% | 75.8% | 80.0% | 77.3% | 63.0% | 75.0% | 64.3% |
| RACTε | 80.0% | 75.4% | 70.6% | 75.8% | 76.7% | 74.7% | 63.0% | 67.9% | 61.9% |
| Feasibility | 80.0% | 80.3% | 71.3% | 80.3% | 79.2% | 75.7% | 66.7% | 75.0% | 62.5% |
| Normal Subjects | Pre | Time 1 | Time 2 | Time 3 | |
|---|---|---|---|---|---|
| Mean | Mean | Mean | Mean | Mean | |
| (R-Gating) LA ε R | 52.07 ± 15.87 | 35.21 ± 11.63 | 25.44 ± 12.17 | 29.94 ± 11.24 | 35.29 ± 13.57 |
| (R-Gating) LA ε Cd | 37.82 ± 13.8 | 20.85 ± 10.17 | 15.94 ± 8.48 | 18.21 ± 7.85 | 21.58 ± 9.23 |
| (R-Gating) LA ε Ct | 14.74 ± 7.27 | 13.95 ± 6.28 | 10.65 ± 7.46 | 12.31 ± 7.65 | 13.85 ± 8.79 |
| (P-Gating) LA ε R | 45.19 ± 13.03 | 30.72 ± 9.34 | 22.69 ± 9.62 | 26.46 ± 8.58 | 30.58 ± 10.21 |
| (P-Gating) LA ε Cd | 33.25 ± 12.57 | 18.37 ± 8.87 | 14.7 ± 7.92 | 16.41 ± 7.3 | 19.05 ± 7.82 |
| (P-Gating) LA ε Ct | 12.6 ± 5.41 | 12.36 ± 4.89 | 9.36 ± 5.89 | 10.61 ± 5.65 | 11.68 ± 6.45 |
| (R-Gating) RA ε R | 47.84 ± 16.6 | 38.49 ± 12.77 | 18.96 ± 9.49 | 22.4 ± 8.38 | 28.2 ± 14.71 |
| (R-Gating) RA ε Cd | 31.14 ± 13.66 | 22.72 ± 9.06 | 11.37 ± 6.72 | 13.49 ± 7.92 | 16.59 ± 10.27 |
| (R-Gating) RA ε Ct | 17.25 ± 9.09 | 15.84 ± 7.82 | 8.81 ± 6.64 | 10.19 ± 6.83 | 12.51 ± 7.86 |
| (P-Gating) RA ε R | 40.7 ± 13.15 | 33.22 ± 9.48 | 17,23 ± 7.92 | 20.26 ± 6.93 | 24.56 ± 11.13 |
| (P-Gating) RA ε Cd | 27.04 ± 12.4 | 19.9 ± 7.98 | 10.35 ± 6.55 | 12.64 ± 8.2 | 14.86 ± 9.22 |
| (P-Gating) RA ε Ct | 14.31 ± 6.52 | 13.38 ± 5.8 | 8.15 ± 5.72 | 8.98 ± 5.41 | 10.59 ± 5.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cantinotti, M.; Marchese, P.; Scalese, M.; Franchi, E.; Assanta, N.; Koestenberger, M.; Pizzuto, A.; Pak, V.; Santoro, G.; Jani, V.; et al. Atrial Function Impairments after Pediatric Cardiac Surgery Evaluated by STE Analysis. J. Clin. Med. 2022, 11, 2497. https://doi.org/10.3390/jcm11092497
Cantinotti M, Marchese P, Scalese M, Franchi E, Assanta N, Koestenberger M, Pizzuto A, Pak V, Santoro G, Jani V, et al. Atrial Function Impairments after Pediatric Cardiac Surgery Evaluated by STE Analysis. Journal of Clinical Medicine. 2022; 11(9):2497. https://doi.org/10.3390/jcm11092497
Chicago/Turabian StyleCantinotti, Massimiliano, Pietro Marchese, Marco Scalese, Eliana Franchi, Nadia Assanta, Martin Koestenberger, Alessandra Pizzuto, Vitali Pak, Giuseppe Santoro, Vivek Jani, and et al. 2022. "Atrial Function Impairments after Pediatric Cardiac Surgery Evaluated by STE Analysis" Journal of Clinical Medicine 11, no. 9: 2497. https://doi.org/10.3390/jcm11092497
APA StyleCantinotti, M., Marchese, P., Scalese, M., Franchi, E., Assanta, N., Koestenberger, M., Pizzuto, A., Pak, V., Santoro, G., Jani, V., Kutty, S., & Giordano, R. (2022). Atrial Function Impairments after Pediatric Cardiac Surgery Evaluated by STE Analysis. Journal of Clinical Medicine, 11(9), 2497. https://doi.org/10.3390/jcm11092497