
A Comparison of McGrath Videolaryngoscope versus Macintosh Laryngoscope for Nasotracheal Intubation: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Study Selection
- 1.
- Inclusion CriteriaProspective randomized clinical trials that compared the McGrath videolaryngoscopy and Macintosh laryngoscopy techniques in nasotracheal intubation in adult patients (age ≥ 18 years old) who underwent operations with general anesthesia were included.
- 2.
- Exclusion CriteriaWe excluded manikin trials, cadaver studies, observational studies, studies that involved tracheal intubation during cardiopulmonary resuscitation, double-lumen tubes, pediatric patients (age < 18 years old), and articles that involved nasotracheal intubation with other videolaryngoscopes.
2.3. Outcomes
- 1.
- Primary outcomeThe primary outcomes were the intubation time (from the intranasal placement of the tube to the detection of carbon dioxide via capnography), the rate of classification 1 scores in the Cormack–Lehane classification system, and the first-attempt success rate.
- 2.
- Secondary outcomeThe secondary outcomes were the rate of the use of Magill forceps and the use of the external laryngeal pressure (or backward, upward, or rightward pressure) maneuver.
2.4. Data Extraction
2.5. Data Synthesis
- All of the studies included shared the same methods and units when evaluating the outcomes, such as intubating time, first-attempt success rate, the Cormack–Lehane classification of the quality of the view of the glottis/vocal cord, and the use of Magill forceps during intubation (continuous outcomes needed to share the same unit);
- When evaluating the outcomes, different terms which shared one similar meaning were used: external laryngeal manipulation. Some of the studies used the term “backward–upward–rightward pressure maneuver (BURP maneuver)” or “external laryngeal pressure” to define the same maneuver.
- The studies included used different tools/values to evaluate the outcome of ease of intubation. This kind of outcome was not synthesized and included in our studies.
2.6. Risk of Bias
2.7. Quality Assessment
3. Results
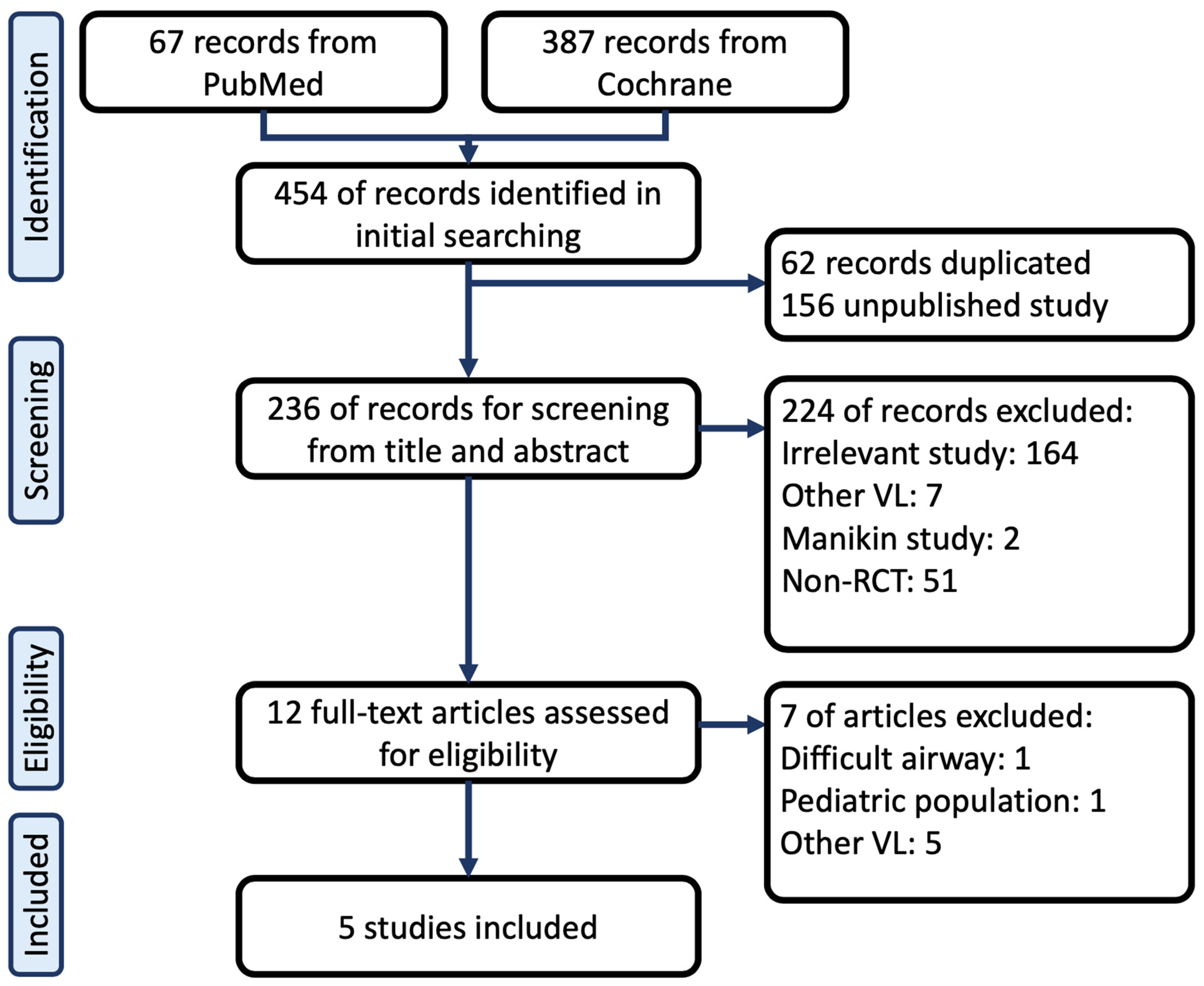
3.1. Searching Result
3.2. Included Studies
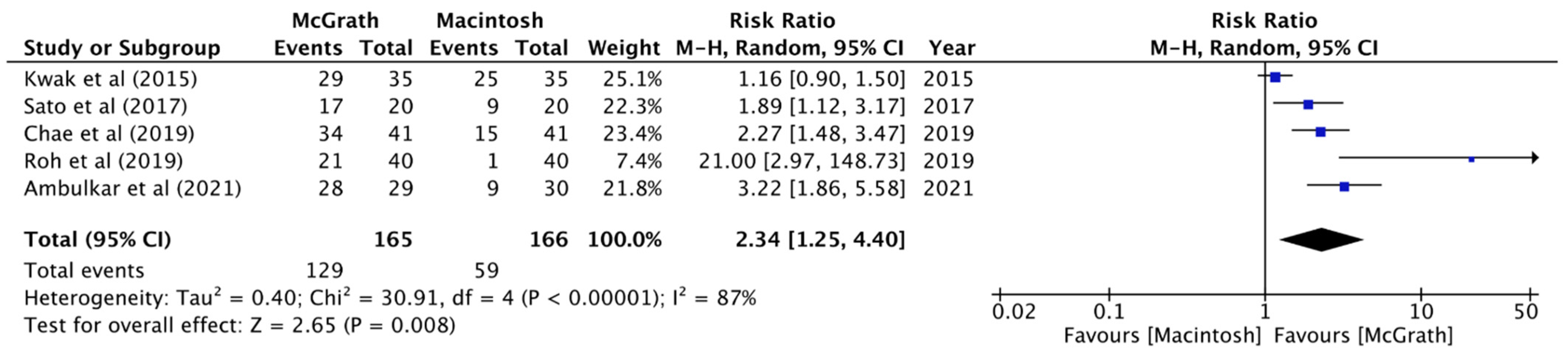
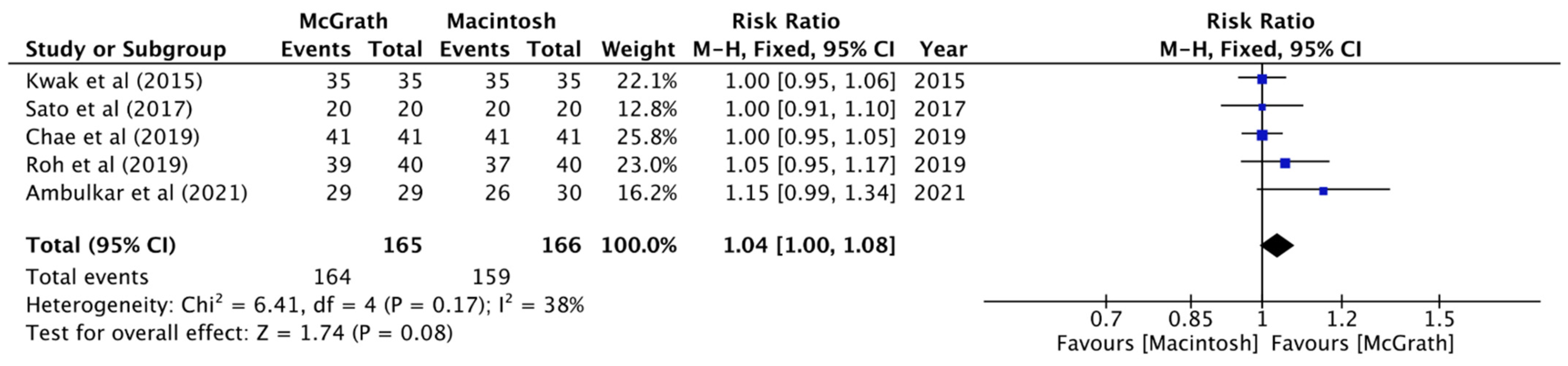
3.3. Result of Primary Outcomes
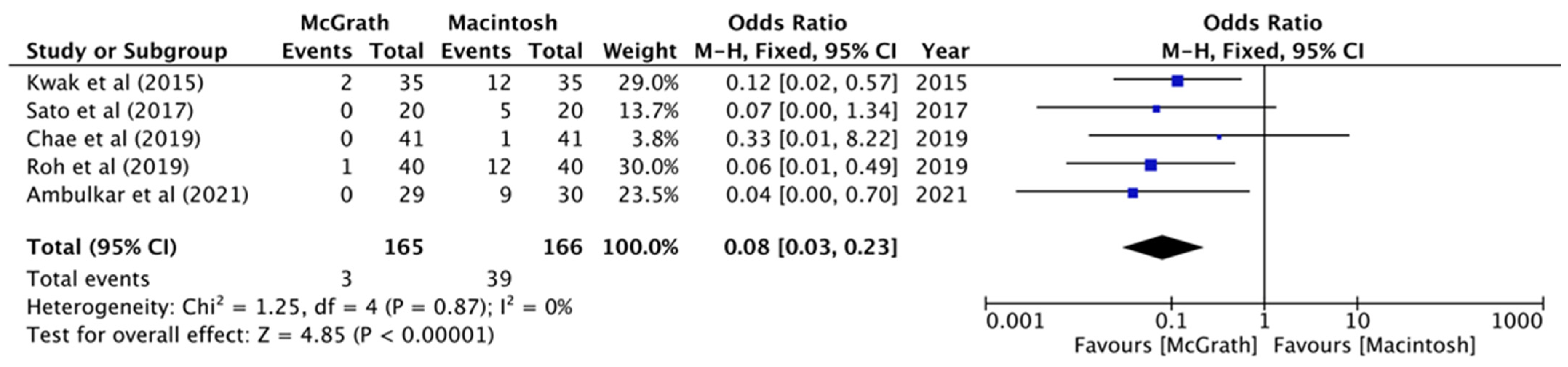
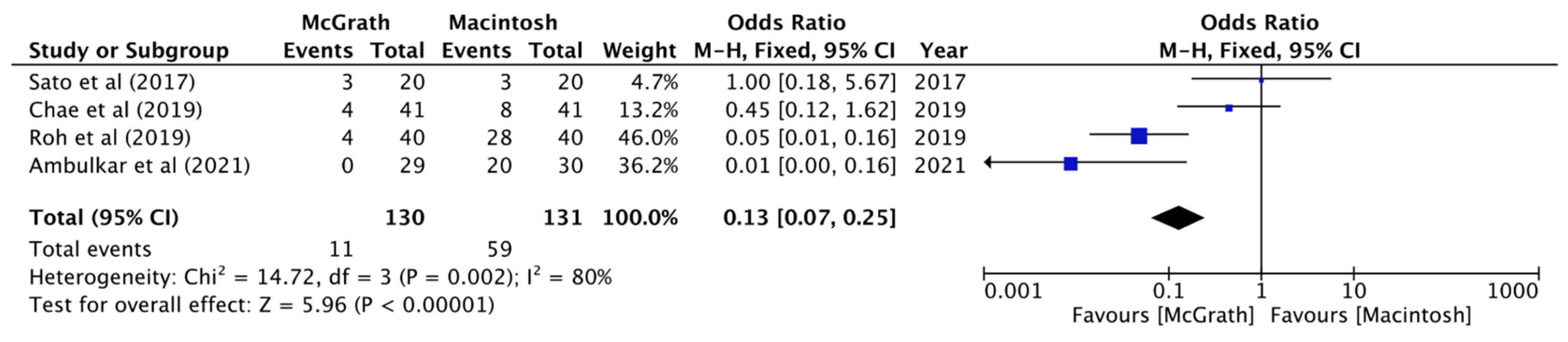
3.4. Result of Secondary Outcomes
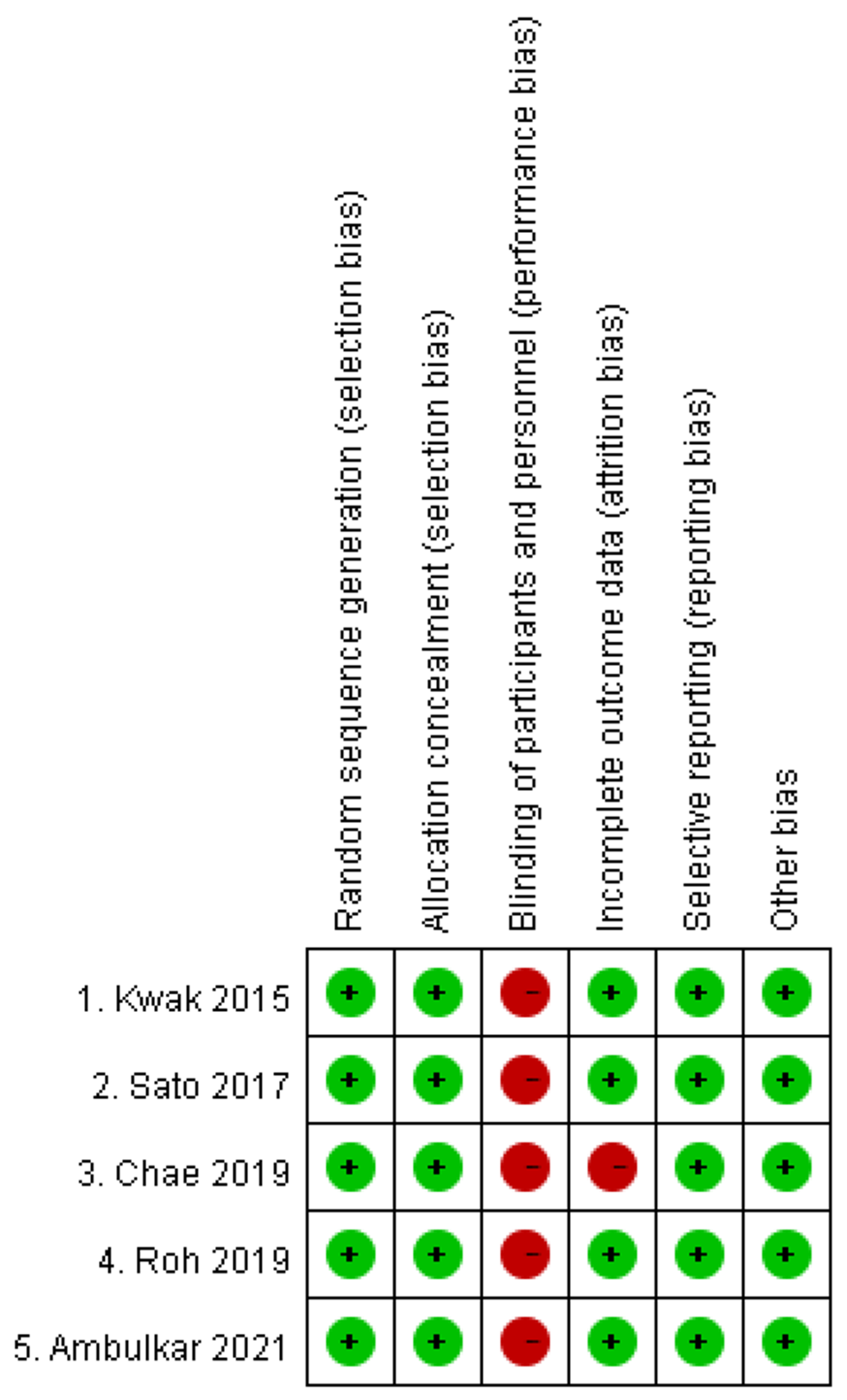
3.5. Risk of Bias
3.6. GRADE Assessment
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kriege, M.; Alflen, C.; Tzanova, I.; Schmidtmann, I.; Piepho, T.; Noppens, R.R. Evaluation of the McGrath MAC and Macintosh laryngoscope for tracheal intubation in 2000 patients undergoing general anaesthesia: The randomised multicentre EMMA trial study protocol. BMJ Open 2017, 7, e016907. [Google Scholar] [CrossRef] [PubMed]
- Hoshijima, H.; Mihara, T.; Maruyama, K.; Denawa, Y.; Takahashi, M.; Shiga, T.; Nagasaka, H. McGrath videolaryngoscope versus Macintosh laryngoscope for tracheal intubation: A systematic review and meta-analysis with trial sequential analysis. J. Clin. Anesth. 2018, 46, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Prasanna, D.; Bhat, S. Nasotracheal Intubation: An Overview. J. Maxillofac. Oral Surg. 2014, 13, 366–372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, J.; Ma, D.-X.; Li, B.; Wu, A.-S.; Xue, F.-S. Videolaryngoscopy versus direct laryngoscopy for nasotracheal intubation: A systematic review and meta-analysis of randomised controlled trials. J. Clin. Anesth. 2019, 52, 6–16. [Google Scholar] [CrossRef]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Updated guidance for trusted systematic reviews: A new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 2019, 10, D142. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 105906. [Google Scholar] [CrossRef]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H.; et al. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- Zhu, H.; Liu, J.; Suo, L.; Zhou, C.; Sun, Y.; Jiang, H. A randomized controlled comparison of non-channeled king vision, McGrath MAC video laryngoscope and Macintosh direct laryngoscope for nasotracheal intubation in patients with predicted difficult intubations. BMC Anesthesiol. 2019, 19, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Yoo, J.Y.; Chae, Y.J.; Lee, Y.B.; Kim, S.; Lee, J.; Kim, D.H. A comparison of the Macintosh laryngoscope, McGrath video laryngoscope, and Pentax Airway Scope in paediatric nasotracheal intubation. Sci. Rep. 2018, 8, 17365. [Google Scholar] [CrossRef]
- Seo, K.H.; Kim, K.M.; John, H.; Jun, J.H.; Han, M.; Kim, S. Comparison of C-MAC D-blade videolaryngoscope and McCoy laryngoscope efficacy for nasotracheal intubation in simulated cervical spinal injury: A prospective randomized comparative study. BMC Anesthesiol. 2020, 20, 1–9. [Google Scholar] [CrossRef]
- Kadapamannil, D.; Rajan, S.; Barua, K.; Tosh, P.; Paul, J.; Kumar, L. Ease of intubation and hemodynamic responses to nasotracheal intubation using C-MAC videolaryngoscope with D blade: A comparison with use of traditional Macintosh laryngoscope. J. Anaesthesiol. Clin. Pharmacol. 2018, 34, 381–385. [Google Scholar] [CrossRef] [PubMed]
- Xue, F.-S.; Li, X.-Y.; Liu, Q.-J.; Liu, H.-P.; Yang, Q.-Y.; Xu, Y.-C.; Liao, X.; Liu, Y. Circulatory responses to nasotracheal intubation: Comparison of GlideScope® videolaryngoscope and Macintosh direct laryngoscope. Chin. Med. J. 2008, 121, 1290–1296. [Google Scholar] [CrossRef] [PubMed]
- Hazarika, H.; Saxena, A.; Meshram, P.; Bhargava, A.K. A randomized controlled trial comparing C Mac D Blade and Macintosh laryngoscope for nasotracheal intubation in patients undergoing surgeries for head and neck cancer. Saudi J. Anaesth. 2018, 12, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Jones, P.M.; Armstrong, K.P.; Armstrong, P.M.; Cherry, R.A.; Harle, C.C.; Hoogstra, J.; Turkstra, T.P. A Comparison of GlideScope® Videolaryngoscopy to Direct Laryngoscopy for Nasotracheal Intubation. Anesth. Analg. 2008, 107, 144–148. [Google Scholar] [CrossRef]
- Kwak, H.-J.; Lee, S.-Y.; Lee, S.-Y.; Cho, S.-H.; Kim, H.-S.; Kim, J.-Y. McGrath Video Laryngoscopy Facilitates Routine Nasotracheal Intubation in Patients Undergoing Oral and Maxillofacial Surgery: A Comparison With Macintosh Laryngoscopy. J. Oral Maxillofac. Surg. 2016, 74, 256–261. [Google Scholar] [CrossRef]
- Sato, A.; Sobue, K.; Kako, E.; Tachi, N.; Okumura, Y.; Kanazawa, M.; Hashimoto, M.; Harada, J.; Boku, A.S. The usefulness of the McGrath MAC laryngoscope in comparison with Airwayscope and Macintosh laryngoscope during routine nasotracheal intubation: A randomaized controlled trial. BMC Anesthesiol. 2017, 17, 160. [Google Scholar] [CrossRef] [Green Version]
- Chae, Y.J.; Kim, D.H.; Park, E.J.; Oh, J.; Yi, I.K. A comparison of McGrath MAC, Pentax AWS, and Macintosh direct laryngoscopes for nasotracheal intubation: A randomized controlled trial. Ther. Clin. Risk Manag. 2019, 15, 1121–1128. [Google Scholar] [CrossRef] [Green Version]
- Roh, G.U.; Kwak, H.J.; Lee, K.C.; Lee, S.Y.; Kim, J.Y. Randomized comparison of McGrath MAC videolaryngoscope, Pentax Airway Scope, and Macintosh direct laryngoscope for nasotracheal intubation in patients with manual in-line stabilization. Can. J. Anaesth. 2019, 66, 1213–1220. [Google Scholar] [CrossRef]
- Ambulkar, R.; Ranganathan, P.; Savarkar, S.; Divatia, J.V. A randomized controlled trial comparing McGRATH series 5 videolaryngoscope with the Macintosh laryngoscope for nasotracheal intubation. J. Anaesthesiol. Clin. Pharmacol. 2020, 36, 477–482. [Google Scholar] [CrossRef]
- Kleine-Brueggeney, M.; Greif, R.; Schoettker, P.; Savoldelli, G.L.; Nabecker, S.; Theiler, L.G. Evaluation of six videolaryngoscopes in 720 patients with a simulated difficult airway: A multicentre randomized controlled trial. Br. J. Anaesth. 2016, 116, 670–679. [Google Scholar] [CrossRef] [Green Version]
- Savoldelli, G.L.; Schiffer, E.; Abegg, C.; Baeriswyl, V.; Clergue, F.; Waeber, J.L. Comparison of the Glidescope®, the McGrath®, the Airtraq® and the Macintosh laryngoscopes in simulated difficult airways*. Anaesthesia 2008, 63, 1358–1364. [Google Scholar] [CrossRef] [PubMed]
- Combes, X.; Dhonneur, G. Difficult tracheal intubation. Br. J. Anaesth. 2010, 104, 260–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, B.J.; Padnos, I.; Mancuso, K.; Christensen, B.J. Comparing Video and Direct Laryngoscopy for Nasotracheal Intubation. Anesth. Prog. 2020, 67, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Yeom, J.H.; Oh, M.K.; Shin, W.J.; Ahn, D.W.; Jeon, W.J.; Cho, S.Y. Randomized comparison of the effectiveness of nasal intubation using a GlideScope video laryngoscope with Magill forceps versus vascular forceps in patients with a normal airway. Can. J. Anaesth. 2017, 64, 1176–1181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, R.; Niu, J.-Y.; Wu, L.-N.; Sun, H.; Sun, P.; Huang, J.-Y.; Yu, J.-M. Comparison of a tube core and Magill forceps for nasotracheal intubation: A randomised controlled trial. Trials 2021, 22, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Flenner, M.; Schindler, E. Complications associated with nasotracheal intubation and proposal of simple countermeasure. Anaesthesiol. Intensive Ther. 2019, 51, 72–73. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Participants | Case Number (MG/ML) | ASA Status | Outcomes | Other Outcomes | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Intubation Time | CL Classification 1 | Successful Rate in 1st Attempt | Magill Forceps Use | BURP Maneuver | ||||||
| Kwak [15] | 2015 | Oral and maxillofacial surgery | 70 (35/35) | 1~2 | V | V | V | V | Ease of intubation, bleeding | |
| Sato [16] | 2017 | Elective oral surgery | 40 (20/20) | 1~2 | V | V | V | V | V | bleeding, esophageal intubation, dental injury |
| Chae [17] | 2019 | Elective oral and maxillofacial surgery | 82 (41/41) | 1~2 | V | V | V | V | V | Nasotracheal intubation difficulty score |
| Roh [18] | 2019 | Dental or maxillofacial surgery | 80 (40/40) | 1~2 | V | V | V | V | V | Bleeding risk, ease of intubaiton |
| Ambulkar [19] | 2021 | Elective head and neck cancer surgery | 59 (29/30) | 1~2 | V | V | V | V | V | Difficulty of intubation |
| Quality Assessment | Summary of Findings | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| No. of Studies | Risk of Bias | Inconsistency | Indirectness | Imprecision | Publication Bias | Number of Patients (%) | Effect | Quality of Evidence | ||
| McGrath | Macintosh | Relative Risk (95% CI) | Absolute Risk | |||||||
| Intubation time | ||||||||||
| 5 | No serious risk of bias *1 | Serious *2 | No serious limitation | No serious limitation | No Serious limitation | 165 | 166 | MD = −10.98 (−2.98~−18.97) | Low | |
| Cormack-Lehane classification 1 | ||||||||||
| 5 | No serious risk of bias *1 | Serious *2 | No serious limitation | No serious limitation | No Serious limitation | 129/165 (78.2%) | 59/166 (35.5) | 2.34 (1.25~4.40) | 44 more per 100 | Very low |
| First attempt successful rate | ||||||||||
| 5 | No serious risk of bias *1 | No serious limitation | No serious limitation | Mild limitation | No Serious limitation | 164/165 (99.4%) | 159/166 (95.8%) | 1.04 (1.00~1.08) | Not Significant | Low |
| Use of Magill forceps | ||||||||||
| 5 | No serious risk of bias *1 | No serious limitation | No serious limitation | No serious limitation | No Serious limitation | 3/165 (1.8%) | 39/166 (23.5%) | OR = 0.08 (0.03–0.23) | 21 less per 100 | Low |
| Backward-upward-rightward Pressure Maneuver | ||||||||||
| 4 | No serious risk of bias *1 | Serious *2 | No serious limitation | No serious limitation | No Serious limitation | 11/130 | 59/131 | OR = 0.13 (0.07–0.25) | 36 less per 100 | Very low |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ho, C.-H.; Chen, L.-C.; Hsu, W.-H.; Lin, T.-Y.; Lee, M.; Lu, C.-W. A Comparison of McGrath Videolaryngoscope versus Macintosh Laryngoscope for Nasotracheal Intubation: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 2499. https://doi.org/10.3390/jcm11092499
Ho C-H, Chen L-C, Hsu W-H, Lin T-Y, Lee M, Lu C-W. A Comparison of McGrath Videolaryngoscope versus Macintosh Laryngoscope for Nasotracheal Intubation: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(9):2499. https://doi.org/10.3390/jcm11092499
Chicago/Turabian StyleHo, Chia-Hao, Li-Chung Chen, Wen-Hao Hsu, Tzu-Yu Lin, Meng Lee, and Cheng-Wei Lu. 2022. "A Comparison of McGrath Videolaryngoscope versus Macintosh Laryngoscope for Nasotracheal Intubation: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 11, no. 9: 2499. https://doi.org/10.3390/jcm11092499
APA StyleHo, C. -H., Chen, L. -C., Hsu, W. -H., Lin, T. -Y., Lee, M., & Lu, C. -W. (2022). A Comparison of McGrath Videolaryngoscope versus Macintosh Laryngoscope for Nasotracheal Intubation: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 11(9), 2499. https://doi.org/10.3390/jcm11092499