
Bracket Transfer Accuracy with the Indirect Bonding Technique—A Systematic Review and Meta-Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Literature Search and Study Selection Process
2.3. Data Extraction
2.4. Risk of Bias Assessment in Included Studies
2.5. Meta-Analysis and Synthesis of Results
3. Results
3.1. Literature Search Results
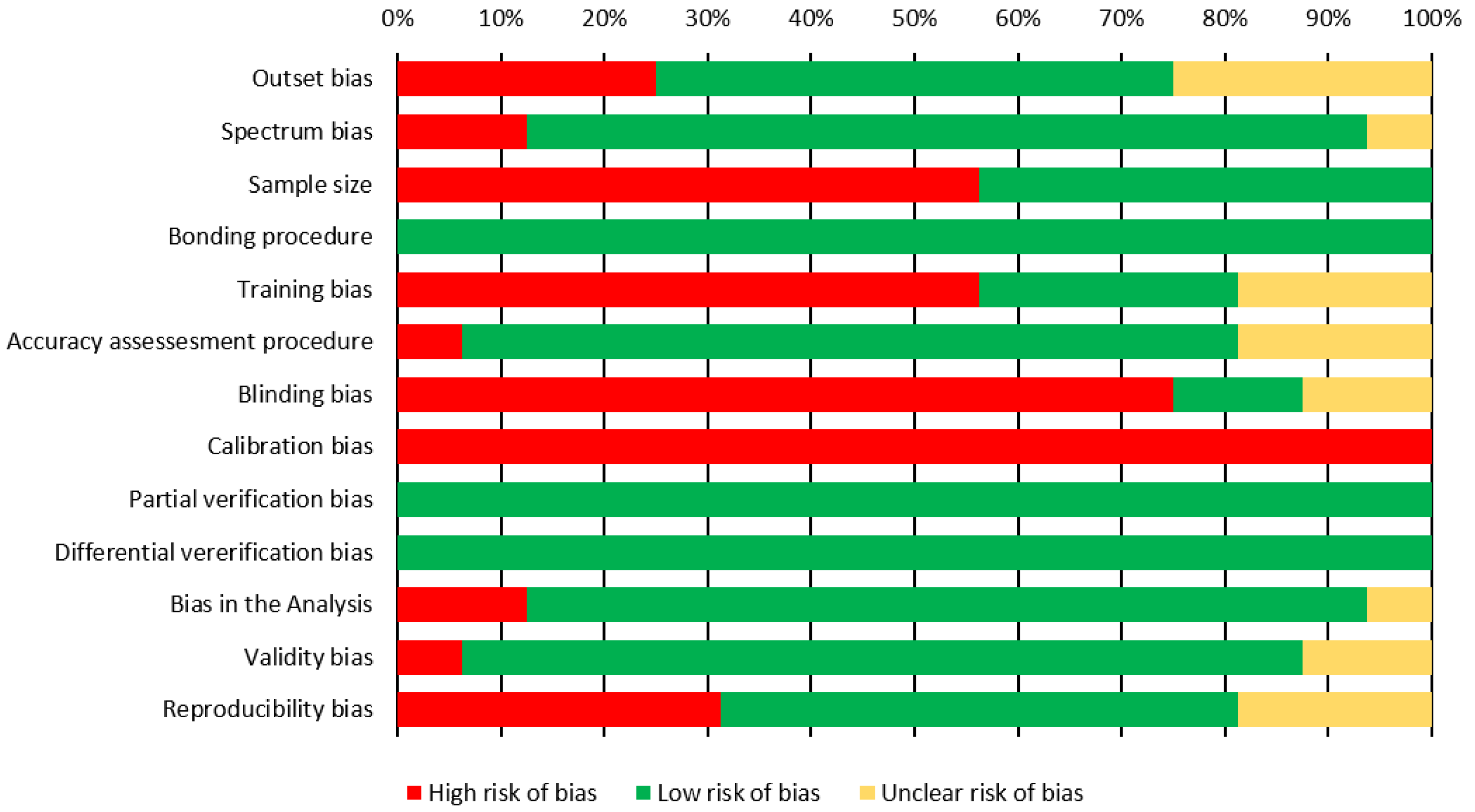
3.2. Results of the Risk of Bias Assessment
3.3. Study Characteristics and Results of Individual Studies
3.3.1. Study Characteristics and Results of the In Vivo Studies Not Included in the Quantitative Synthesis
3.3.2. Study Characteristics of the Ex vivo Studies Included in the Quantitative Synthesis
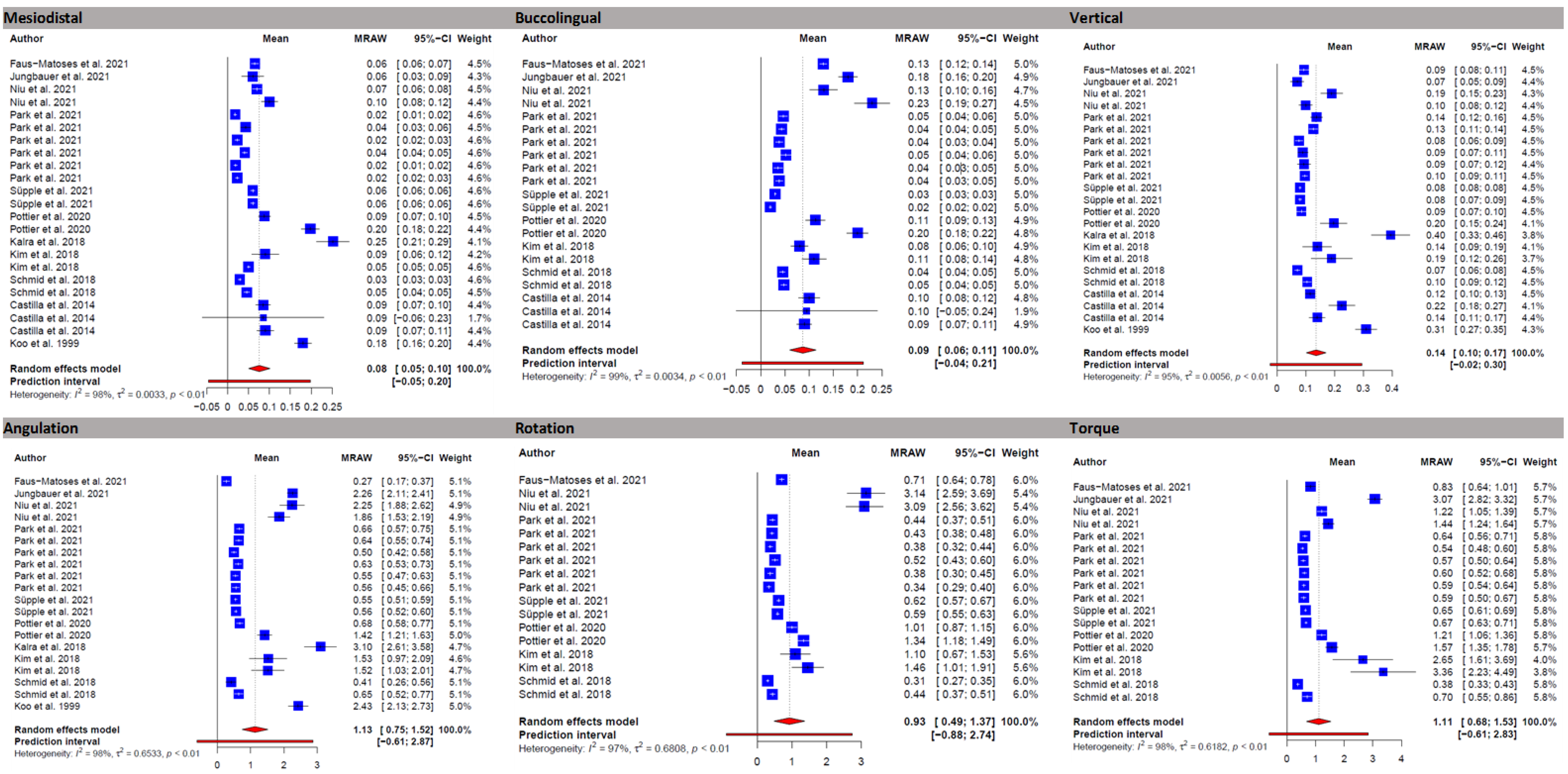
3.4. Results of the Meta-Analysis
3.5. Linear Mean Transfer Errors
3.6. Angular Mean Transfer Errors
4. Discussion
4.1. Overall
4.2. Tooth Groups
4.3. Side Differences and Differences between Upper and Lower Jaw
4.4. Tray Materials
4.5. Accuracy Assessment Method
5. Strengths and Limitations
6. Clinical Implications
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Andrews, L.F. The straight-wire appliance, origin, controversy, commentary. J. Clin. Orthod. 1976, 10, 99–114. [Google Scholar] [PubMed]
- Andrews, L.F. The straight-wire appliance, explained and compared. J. Clin. Orthod. 1976, 10, 174–195. [Google Scholar] [PubMed]
- Fukuyo, K.; Nishii, Y.; Nojima, K.; Yamaguchi, H. A comparative study in three methods of bracket placement. Orthod. Waves 2004, 63, 63–70. [Google Scholar]
- Birdsall, J.; Hunt, N.P.; Sabbah, W.; Moseley, H.C. Accuracy of positioning three types of self-ligating brackets compared with a conventionally ligating bracket. J. Orthod. 2012, 39, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.W.; Koroluk, L.; Ko, C.C.; Zhang, K.; Chen, M.; Nguyen, T. Effectiveness and efficiency of a CAD/CAM orthodontic bracket system. Am. J. Orthod. Dentofac. Orthop. 2015, 148, 1067–1074. [Google Scholar] [CrossRef] [Green Version]
- Garino, F.; Garino, G.B. Computer-aided interactive indirect bonding. Prog. Orthod. 2005, 6, 214–223. [Google Scholar]
- Grunheid, T.; Lee, M.S.; Larson, B.E. Transfer accuracy of vinyl polysiloxane trays for indirect bonding. Angle Orthod. 2016, 86, 468–474. [Google Scholar] [CrossRef] [Green Version]
- Aguirre, M.J.; King, G.J.; Waldron, J.M. Assessment of bracket placement and bond strength when comparing direct bonding to indirect bonding techniques. Am. J. Orthod. 1982, 82, 269–276. [Google Scholar] [CrossRef]
- Carlson, S.K.; Johnson, E. Bracket positioning and resets: Five steps to align crowns and roots consistently. Am. J. Orthod. Dentofac. Orthop. 2001, 119, 76–80. [Google Scholar] [CrossRef]
- Castilla, A.E.; Crowe, J.J.; Moses, J.R.; Wang, M.; Ferracane, J.L.; Covell, D.A.J. Measurement and comparison of bracket transfer accuracy of five indirect bonding techniques. Angle Orthod. 2014, 84, 607–614. [Google Scholar] [CrossRef] [Green Version]
- El-Timamy, A.M.; El-Sharaby, F.A.; Eid, F.H.; Mostafa, Y.A. Three-dimensional imaging for indirect-direct bonding. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 928–931. [Google Scholar] [CrossRef] [Green Version]
- Guenthner, T.A.; Larson, B.E. Indirect bonding: A technique for precision and efficiency. Semin. Orthod. 2007, 13, 58–63. [Google Scholar] [CrossRef]
- Suárez, C.; Vilar, T. The effect of constant height bracket placement on marginal ridge levelling using digitized models. Eur. J. Orthod. 2010, 32, 100–105. [Google Scholar] [CrossRef] [Green Version]
- Israel, M.; Kusnoto, B.; Evans, C.A.; BeGole, E. A comparison of traditional and computer-aided bracket placement methods. Angle Orthod. 2011, 81, 828–835. [Google Scholar] [CrossRef]
- Silverman, E.; Cohen, M.; Gianelly, A.A.; Dietz, V.S. A universal direct bonding system for both metal and plastic brackets. Am. J. Orthod. 1972, 62, 236–244. [Google Scholar] [CrossRef]
- Yildirim, K.; Saglam-Aydinatay, B. Comparative assessment of treatment efficacy and adverse effects during nonextraction orthodontic treatment of class I malocclusion patients with direct and indirect bonding: A parallel randomized clinical trial. Am. J. Orthod. Dentofac. Orthop. 2018, 154, 26.e1–34.e1. [Google Scholar] [CrossRef]
- Shpack, N.; Geron, S.; Floris, I.; Davidovitch, M.; Brosh, T.; Vardimon, A.D. Bracket placement in lingual vs. labial systems and direct vs. indirect bonding. Angle Orthod. 2007, 77, 509–517. [Google Scholar] [CrossRef] [Green Version]
- Koo, B.C.; Chung, C.-H.; Vanarsdall, R.L. Comparison of the accuracy of bracket placement between direct and indirect bonding techniques. Am. J. Orthod. Dentofac. Orthop. 1999, 116, 346–351. [Google Scholar] [CrossRef]
- Bousema, E.J.; Koops, E.A.; van Dijk, P.; Dijkstra, P.U. Association Between Subjective Tinnitus and Cervical Spine or Temporomandibular Disorders: A Systematic Review. Trends Heart 2018, 22, 2331216518800640. [Google Scholar] [CrossRef]
- Nichols, D.A.; Gardner, G.; Carballeyra, A.D. Reproducibility of bracket positioning in the indirect bonding technique. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 770–776. [Google Scholar] [CrossRef] [Green Version]
- Dellinger, E.L. A scientific assessment of the straight-wire appliance. Am. J. Orthod. 1978, 73, 290–299. [Google Scholar] [CrossRef]
- Miethke, R.R.; Melsen, B. Effect of variation in tooth morphology and bracket position on first and third order correction with preadjusted appliances. Am. J. Orthod. Dentofac. Orthop. 1999, 116, 329–335. [Google Scholar] [CrossRef]
- Germane, N.; Bentley, B.E.J.; Isaacson, R.J. Three biologic variables modifying faciolingual tooth angulation by straight-wire appliances. Am. J. Orthod. Dentofac. Orthop. 1989, 96, 312–319. [Google Scholar] [CrossRef]
- Li, Y.; Mei, L.; Wei, J.; Yan, X.; Zhang, X.; Zheng, W.; Li, Y. Effectiveness, efficiency and adverse effects of using direct or indirect bonding technique in orthodontic patients: A systematic review and meta-analysis. BMC Oral Health 2019, 19, 137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duarte, M.E.A.; Gribel, B.F.; Spitz, A.; Artese, F.; Miguel, J.A.M. Reproducibility of digital indirect bonding technique using three-dimensional (3D) models and 3D-printed transfer trays. Angle Orthod. 2019, 90, 92–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xue, C.; Xu, H.; Guo, Y.; Xu, L.; Dhami, Y.; Wang, H.; Liu, Z.; Ma, J.; Bai, D. Accurate bracket placement using a computer-aided design and computer-aided manufacturing–guided bonding device: An in vivo study. Am. J. Orthod. Dentofac. Orthop. 2020, 157, 269–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pottier, T.; Brient, A.; Turpin, Y.L.; Chauvel, B.; Meuric, V.; Sorel, O.; Brezulier, D. Accuracy evaluation of bracket repositioning by indirect bonding: Hard acrylic CAD/CAM versus soft one-layer silicone trays, an in vitro study. Clin. Oral Investig. 2020, 24, 3889–3897. [Google Scholar] [CrossRef]
- Jungbauer, R.; Breunig, J.; Schmid, A.; Hüfner, M.; Kerberger, R.; Rauch, N.; Proff, P.; Drescher, D.; Becker, K. Transfer accuracy of two 3D printed trays for indirect bracket bonding—An in vitro pilot study. Appl. Sci. 2021, 11, 6013. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Richardson, W.S.; Wilson, M.C.; Nishikawa, J.; Hayward, R.S. The well-built clinical question: A key to evidence-based decisions. ACP J. Club 1995, 123, A12–A13. [Google Scholar] [CrossRef]
- Lefebvre, C.; Glanville, J.; Briscoe, S.; Featherstone, R.; Littlewood, A.; Marshall, C.; Metzendorf, M.-I.; Noel-Storr, A.; Paynter, R.; Rader, T.; et al. Chapter 4: Searching for and selecting studies. In Cochrane Handbook for Systematic Reviews of Interventions version 6.3; Updated February 2022; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: London, UK, 2022. [Google Scholar]
- Niu, Y.; Zeng, Y.; Zhang, Z.; Xu, W.; Xiao, L. Comparison of the transfer accuracy of two digital indirect bonding trays for labial bracket bonding. Angle Orthod. 2021, 91, 67–73. [Google Scholar] [CrossRef]
- Drevon, D.; Fursa, S.R.; Malcolm, A.L. Intercoder reliability and validity of webplotdigitizer in extracting graphed data. Behav. Modif. 2017, 41, 323–339. [Google Scholar] [CrossRef]
- Kühnisch, J.; Janjic Rankovic, M.; Kapor, S.; Schüler, I.; Krause, F.; Michou, S.; Ekstrand, K.; Eggmann, F.; Neuhaus, K.W.; Lussi, A.; et al. Identifying and avoiding risk of bias in caries diagnostic studies. J. Clin. Med. 2021, 10, 3223. [Google Scholar] [CrossRef]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M.; QUADAS-2 Group. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Harrer, M.; Cuijpers, P.; Furukawa, T.A.; Ebert, D.D. Doing Meta-Analysis with R: A Hands-on Guide; CRC Press: Boca Raton, FL, USA, 2021. [Google Scholar]
- Wickham, H.; Averick, M.; Bryan, J.; Chang, W.; McGowan, L.D.A.; François, R.; Grolemund, G.; Hayes, A.; Henry, L.; Hester, J.; et al. Welcome to the Tidyverse. J. Open Source Softw. 2019, 4, 1686. [Google Scholar] [CrossRef]
- Wickham, H.; François, R.; Henry, L.; Müller, K. A Grammar of Data Manipulation [R package dplyr Version 1.0.2], 2020.
- Wilkinson, L. ggplot2: Elegant Graphics for Data Analysis by WICKHAM, H. Biometrics 2011, 67, 678–679. [Google Scholar] [CrossRef]
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to perform a meta-analysis with R: A practical tutorial. Évid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef] [Green Version]
- Veroniki, A.A.; Jackson, D.; Viechtbauer, W.; Bender, R.; Bowden, J.; Knapp, G.; Kuss, O.; Higgins, J.P.T.; Langan, D.; Salanti, G. Methods to estimate the between-study variance and its uncertainty in meta-analysis. Res. Synth. Methods 2016, 7, 55–79. [Google Scholar] [CrossRef] [Green Version]
- Knapp, G.; Hartung, J. Improved tests for a random effects meta-regression with a single covariate. Stat. Med. 2003, 22, 2693–2710. [Google Scholar] [CrossRef]
- Park, J.-H.; Choi, J.-Y.; Oh, S.H.; Kim, S.-H. Three-dimensional digital superimposition of orthodontic bracket position by using a computer-aided transfer jig system: An accuracy analysis. Sensors 2021, 21, 5911. [Google Scholar] [CrossRef]
- Park, J.H.; Choi, J.Y.; Kim, S.H.; Kim, S.J.; Lee, K.J.; Nelson, G. Three-dimensional evaluation of the transfer accuracy of a bracket jig fabricated using computer-aided design and manufacturing to the anterior dentition: An in vitro study. Korean J. Orthod. 2021, 51, 375–386. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Chun, Y.S.; Kim, M. Accuracy of bracket positions with a CAD/CAM indirect bonding system in posterior teeth with different cusp heights. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 298–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmid, J.; Brenner, D.; Recheis, W.; Hofer-Picout, P.; Brenner, M.; Crismani, A.G. Transfer accuracy of two indirect bonding techniques-an in vitro study with 3D scanned models. Eur. J. Orthod. 2018, 40, 549–555. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, V.; Batra, P.; Sharma, K.; Raghavan, S.; Gandhi, V.; Srivastava, A. A comparative assessment of transfer accuracy of two indirect bonding techniques in patients undergoing fixed mechanotherapy: A randomised clinical trial. J. Orthod. 2021, 48, 13–23. [Google Scholar] [CrossRef]
- Hodge, T.M.; Dhopatkar, A.A.; Rock, W.P.; Spary, D.J. A randomized clinical trial comparing the accuracy of direct versus indirect bracket placement. J. Orthod. 2004, 31, 132–137. [Google Scholar] [CrossRef]
- Süpple, J.; von Glasenapp, J.; Hofmann, E.; Jost-Brinkmann, P.G.; Koch, P.J. Accurate bracket placement with an indirect bonding method using digitally designed transfer models printed in different orientations-an in vitro study. J. Clin. Med. 2021, 10, 2002. [Google Scholar] [CrossRef]
- Faus-Matoses, I.; Guinot Barona, C.; Zubizarreta-Macho, Á.; Paredes-Gallardo, V.; Faus-Matoses, V. A novel digital technique for measuring the accuracy of an indirect bonding technique using fixed buccal multibracket appliances. J. Pers. Med. 2021, 11, 932. [Google Scholar] [CrossRef]
- Kalra, R.K.; Mittal, S.; Gandikota, C.; Sehgal, V.; Gupta, R.; Bali, Z. Comparison of accuracy of bracket placement by direct and indirect bonding techniques using digital processing—An in-vitro study. J. Clin. Diagn. Res. 2018, 12, 7–11. [Google Scholar] [CrossRef]
- Armstrong, D.; Shen, G.; Petocz, P.; Darendeliler, M.A. A comparison of accuracy in bracket positioning between two techniques—Localizing the centre of the clinical crown and measuring the distance from the incisal edge. Eur. J. Orthod. 2007, 29, 430–436. [Google Scholar] [CrossRef] [Green Version]
- Archambault, A.; Lacoursiere, R.; Badawi, H.; Major, P.W.; Carey, J.; Flores-Mir, C. Torque expression in stainless steel orthodontic brackets. A systematic review. Angle Orthod. 2010, 80, 201–210. [Google Scholar] [CrossRef]
- Dalstra, M.; Eriksen, H.; Bergamini, C.; Melsen, B. Actual versus theoretical torsional play in conventional and self-ligating bracket systems. J. Orthod. 2015, 42, 103–113. [Google Scholar] [CrossRef]
- Arreghini, A.; Lombardo, L.; Mollica, F.; Siciliani, G. Torque expression capacity of 0.018 and 0.022 bracket slots by changing archwire material and cross section. Prog. Orthod. 2014, 15, 53. [Google Scholar] [CrossRef] [Green Version]
- Dörfer, S.; König, M.; Jost-Brinkmann, P.G. Übertragungsgenauigeit beim indirekten Platzieren von Brackets. Kieferorthoädie 2006, 20, 91–103. [Google Scholar]
- Hoffmann, L.; Sabbagh, H.; Wichelhaus, A.; Kessler, A. Bracket transfer accuracy with two different three-dimensional printed transfer trays vs. silicone transfer trays. Angle Orthod. 2022, 92, 364–371. [Google Scholar] [CrossRef]
- Donatelli, R.E.; Lee, S.J. How to report reliability in orthodontic research: Part 1. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 156–161. [Google Scholar] [CrossRef] [Green Version]
- Wellek, S. A critical evaluation of the current “p-value controversy”. Biom. J. 2017, 59, 854–872. [Google Scholar] [CrossRef]
- Rücker, G.; Schwarzer, G. Beyond the forest plot: The drapery plot. Res. Synth. Methods 2021, 12, 13–19. [Google Scholar] [CrossRef]
- Czolgosz, I.; Cattaneo, P.M.; Cornelis, M.A. Computer-aided indirect bonding versus traditional direct bonding of orthodontic brackets: Bonding time, immediate bonding failures, and cost-minimization. A randomized controlled trial. Eur. J. Orthod. 2021, 43, 144–151. [Google Scholar] [CrossRef]
- Bozelli, J.V.; Bigliazzi, R.; Barbosa, H.A.; Ortolani, C.L.; Bertoz, F.A.; Faltin Junior, K. Comparative study on direct and indirect bracket bonding techniques regarding time length and bracket detachment. Dental Press. J. Orthod. 2013, 18, 51–57. [Google Scholar] [CrossRef]
- Weber, D.J., II.; Koroluk, L.D.; Phillips, C.; Nguyen, T.; Proffit, W.R. Clinical effectiveness and efficiency of customized vs. Conventional preadjusted bracket systems. J. Clin. Orthod. 2013, 47, 261–266. [Google Scholar]
- Deahl, S.T.; Salome, N.; Hatch, J.P.; Rugh, J.D. Practice-based comparison of direct and indirect bonding. Am. J. Orthod. Dentofac. Orthop. 2007, 132, 738–742. [Google Scholar] [CrossRef]
- Brignardello-Petersen, R. There may be no difference in failure and orthodontic bracket placement accuracy when using a direct or indirect bonding technique. J. Am. Dent. Assoc. 2020, 151, e7. [Google Scholar] [CrossRef]
- De Oliveira, N.S.; Rossouw, E.; Lages, E.M.B.; Macari, S.; Pretti, H. Influence of clinical experience on accuracy of virtual orthodontic attachment bonding in comparison with the direct procedure. Angle Orthod. 2019, 89, 734–741. [Google Scholar] [CrossRef] [Green Version]
- El Nigoumi, A. Assessing the Accuracy of Indirect Bonding with 3D Scanning Technology. J. Clin. Orthod. 2016, 50, 613–619. [Google Scholar]
- Gayake, P.V.; Chitko, S.S.; Sutrave, N.; Gaikwad, P.M. The direct way of indirect bonding—the combined effect. Int. J. Orthod. Milwaukee 2013, 24, 15–17. [Google Scholar]
- Hiro, T.; Iglesia, F.; Andreu, P. Indirect bonding technique in lingual orthodontics: The HIRO system. Prog. Orthod. 2008, 9, 34–45. [Google Scholar]
- Mazzeo, F.; Marchese, E.; Assumma, V.; Sepe, J.; Perillo, L. A new device (FAQ.FIX®) for orthodontic bracket placement in straight wire technique. Prog. Orthod. 2013, 14, 23. [Google Scholar] [CrossRef] [Green Version]
- Mohlhenrich, S.C.; Alexandridis, C.; Peters, F.; Kniha, K.; Modabber, A.; Danesh, G.; Fritz, U. Three-dimensional evaluation of bracket placement accuracy and excess bonding adhesive depending on indirect bonding technique and bracket geometry: An in-vitro study. Head Face Med. 2020, 16, 17. [Google Scholar] [CrossRef] [PubMed]
- Mota Júnior, S.L.; de Andrade Vitral, J.; Schmitberger, C.A.; Machado, D.B.; Avelar, J.C.; Fraga, M.R.; da Silva Campos, M.J.; Vitral, R.W. Evaluation of the vertical accuracy of bracket placement with the Boone gauge. Am. J. Orthod. Dentofacial Orthop. 2015, 148, 821–826. [Google Scholar] [CrossRef] [PubMed]
- Mota Júnior, S.L.; Campos, M.; Schmitberger, C.A.; Vitral, J.A.; Fraga, M.R.; Vitral, R.W.F. Evaluation of the prototype of a new bracket-positioning gauge. Dental Press J. Orthod. 2018, 23, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Nojima, L.I.; Araújo, A.S.; Alves Júnior, M. Indirect orthodontic bonding—A modified technique for improved efficiency and precision. Dental Press J. Orthod. 2015, 20, 109–117. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, N.S.; Gribel, B.F.; Neves, L.S.; Lages, E.M.B.; Macari, S.; Pretti, H. Comparison of the accuracy of virtual and direct bonding of orthodontic accessories. Dental Press J. Orthod. 2019, 24, 46–53. [Google Scholar] [CrossRef]
- Schubert, K.; Halbich, T.; Jost-Brinkmann, P.G.; Müller-Hartwich, R. Precision of indirect bonding of lingual brackets using the Quick Modul System (QMS)®. J. Orofac. Orthop. 2013, 74, 6–17. [Google Scholar] [CrossRef]
- Shin, S.H.; Lee, K.J.; Kim, S.J.; Yu, H.S.; Kim, K.M.; Hwang, C.J.; Cha, J.Y. Accuracy of bracket position using thermoplastic and 3D-printed indirect bonding trays. Int. J. Comput. Dent. 2021, 24, 133–145. [Google Scholar]
- Wendl, B.; Droschl, H.; Muchitsch, P. Indirect bonding--a new transfer method. Eur. J. Orthod. 2008, 30, 100–107. [Google Scholar] [CrossRef]
- Zhang, Y.; Yang, C.; Li, Y.; Xia, D.; Shi, T.; Li, C. Comparison of three-dimensional printing guides and double-layer guide plates in accurate bracket placement. BMC Oral Health 2020, 20, 127. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Domain | Search Term |
|---|---|
| Field | orthodont* |
| AND | |
| Intervention | bonding |
| AND | |
| Outcome | positioning differences OR accuracy OR transfer accuracy OR ideal bracket placement OR accurate bracket positioning OR accurat* |
| Database | Search Strategies | Results |
|---|---|---|
| PubMed | orthodont* [All Fields] AND bonding [All Fields] AND ((positioning [All Fields] differences [All Fields]) OR accuracy [All Fields] OR (transfer [All Fields] accuracy [All Fields]) OR (ideal [All Fields] bracket [All Fields] placement [All Fields]) OR (accurate bracket [All Fields] positioning [All Fields]) [All Fields] OR accurat* [All Fields]) | 218 |
| Embase | orthodont*.mp. AND bonding.mp. AND ((positioning differences).mp. OR accuracy.mp. OR (transfer accuracy).mp. OR (ideal bracket placement).mp. OR (accurate bracket positioning).mp. OR accurat*.mp.) | 101 |
| Web of Science | orthodont* AND bonding AND (positioning differences OR accuracy OR transfer accuracy OR ideal bracket placement OR accurate bracket positioning OR accurat*) | 187 |
| Scopus | TITLE-ABS-KEY (orthodont* AND bonding AND (“positioning differences” OR “positioning difference” OR accurac* OR “transfer accuracy” OR “ideal bracket placement” OR “ideal bracket placements” OR “accurate bracket positioning” OR accurat*)) | 125 |
| Total | 312 |
| Study Details | Sample Details | Bonding Procedure (Indirect) | Transfer Accuracy Assessment | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Author (Year) | Type of Study | Sample Size Calculation/Method | No. of Assessed Brackets | No. of Bonding Clinicians | Type of IDB Tray | Bonded Subject (s)/Object (s) | Data for Reference Model(s) | Tray Construction | Type of Brackets | No. of Examiners | Measuring Method |
| Total/I/C/PM/M | |||||||||||
| Jungbauer et al. [28], 2021 | ex vivo | Yes | 280/80/40/80/80 | NR | 3D printed (soft) | bonding on plaster or printed model | impression | Virtual model, Rapid prototyping | conventional | NR | Scan + Software |
| 280/80/40/80/80 | 3D printed (hard) | bonding on plaster or printed model | impression | Virtual model, Rapid prototyping | |||||||
| Park et al. [43], 2021 | ex vivo | No | 506/147/79/122/158 | 1 | 3D printed | bonding on plaster or printed model | model scan | Virtual model, Rapid prototyping | self-ligating | 1 | Scan + Software |
| Park et al. [44], 2021 | ex vivo | Yes | 225/NR | 1 | 3D printed | bonding on plaster or printed model | model scan | Virtual model, Rapid prototyping | self-ligating | 1 | Scan + Software |
| Faus-Matoses et al. [50], 2021 | ex vivo | No | 335/NR | NR | 3D printed | bonding on plaster or printed model | scan | Virtual model, Rapid prototyping | self-ligating | NR | Scan + Software |
| Niu et al. [32], 2021 | ex vivo | Yes | 108/37/10 19/32/20 | NR | 3D printed | bonding on plaster or printed model | intraoral scan | Virtual model, Rapid prototyping | conventional | NR | Scan + Software |
| Yes | 104/31/18/35/20 | NR | Vacuum Form | bonding on plaster or printed model | intraoral scan | Virtual model, Rapid prototyping | conventional | NR | Scan + Software | ||
| Süpple et al. [49], 2021 | ex vivo | No | 729/210/107/207/205 | NR | Vacuum Form (group H) | bonding on plaster or printed model | scan | Virtual model, Rapid prototyping | conventional | NR | Scan + Software |
| No | 724/209/106/206/203 | Vacuum Form | bonding on plaster or printed model | scan | Model and laboratory process | conventional | NR | Scan + Software | |||
| (group V) | |||||||||||
| Pottier et al. [27], 2020 | ex vivo | Yes | 97/38/20/39/- | 1 | Silicone | bonding on plaster or printed model | intraoral scan | Virtual model, Rapid prototyping | conventional | 1 | Scan + Software |
| Yes | 98/40/19/39/- | 3D printed tray | bonding on plaster or printed model | intraoral scan | Virtual model, Rapid prototyping | conventional | 1 | Scan + Software | |||
| Kalra et al. [51], 2018 | ex vivo | No | 100/20/10/20/0 | 5 | Vacuum Form | bonding on plaster or printed model | impression | Model cast and laboratory process | conventional | NR | Photography |
| Kim et al. [45], 2018 | ex vivo | No | 60/-/-/40/20 | 1 | 3D printed tray | bonding on plaster or printed model | model scan | Virtual model, Rapid prototyping | conventional | NR | Scan + Software |
| 30/-/-/20/10 | |||||||||||
| No | 60/-/-/40/20 | 3D printed tray | bonding on plaster or printed model | model scan | Virtual model, Rapid prototyping | conventional | NR | Scan + Software | |||
| 30/-/-/20/10 | |||||||||||
| Schmid et al. [46], 2018 | ex vivo | Yes | 132/54/24/54/- | 1 | Silicone | bonding on plaster or printed model | impression | Model cast and laboratory process | conventional | NR | Scan + Software |
| Yes | 134/52/29/53/- | 1 | Vacuum form | bonding on plaster or printed model | impression | Model cast and laboratory process | conventional | NR | Scan + Software | ||
| Castilla et al. [10], 2014 | ex vivo | No | 296/98/50/98/50 | NR | Double PVS | bonding on plaster or printed model | impression | Model cast and laboratory process | conventional | NR | Photography, digital caliper |
| 60/20/10/20/10 | |||||||||||
| No | 296/98/50/98/50 | PVS putty | bonding on plaster or printed model | impression | Model cast and laboratory process | conventional | NR | Photography, digital caliper | |||
| 60/20/10/20/1 | |||||||||||
| No | 296/98/50/98/50 | PVS-VF | bonding on plaster or printed model | impression | Model cast and laboratory process | conventional | NR | Photography, digital caliper | |||
| 60/20/10/20/10 | |||||||||||
| No | 296/98/50/98/50 | Double Vacuum Form | bonding on plaster or printed model | impression | Model cast and laboratory process | conventional | NR | Photography, digital caliper | |||
| 58/20/10/18/10 | |||||||||||
| No | 296/98/50/98/50 | Single Vacuum Form | bonding on plaster or printed model | impression | Model cast and laboratory process | conventional | NR | Photography, digital caliper | |||
| 58/18/10/20/10 | |||||||||||
| Koo et al. [18], 1999 | ex vivo | No | 180/72/26/72/0 | 9 | Silicone | bonding on plaster or printed model | impression | Model cast and laboratory process | conventional | NR | Photography |
| Chaudhary et al. [47], 2021 | in vivo | Yes | 300/120/60/120/0 | NR | 3D printed | bonding on patient | intraoral scan | Virtual model, Rapid prototyping | conventional | NR | Scan + Software |
| Yes | 300/120/60/120/0 | PVS | bonding on patient | intraoral scan | Model cast and laboratory process | conventional | NR | Scan + Software | |||
| Xue et al. [26], 2020 | in vivo | Yes | 205/71/36/62/36 | 1 | 3D printed tray | digital or virtual bonding procedure | intraoral scan | Virtual model, Rapid prototyping | conventional | NR | Scan + Software |
| Grünheid et al. [7], 2016 | in vivo | No | 136/54/26/46/10 | 4 | Silicone | Bonding on patient | impression | Model cast and laboratory process | conventional | 1 | CBCT + Software |
| Hodge et al. [48], 2004 | in vivo | Yes | 156/104/52/0/0 | NR | Vacuum Form | Bonding on patient | impression | Model cast and laboratory process | conventional | NR | Photography, acetate copies |
| Analyzed Parameters | Mesiodistal | Buccolingual | Vertical | Angulation | Rotation | Torque | |
|---|---|---|---|---|---|---|---|
| Overall accuracy | |||||||
| n | 23 | 21 | 23 | 20 | 10 | 10 | |
| MTE (95% CI) | 0.08 (0.05; 0.10) | 0.09 (0.06; 0.11) | 0.14 (0.10; 0.17) | 1.13 (0.75; 1.52) | 0.93 (0.49; 1.37) | 1.11 (0.68; 1.53) | |
| Prediction interval | [−0.05; 0.20] | [−0.04; 0.21] | [−0.02; 0.30] | [−0.61; 2.87] | [−0.88; 2.74] | [−0.61; 2.83] | |
| Tooth group comparison | |||||||
| Incisors | n | 14 | 12 | 14 | 14 | 8 | 12 |
| MTE (95% CI) | 0.09 (0.05; 0.12) | 0.14 (0.07; 0.21) | 0.15 (0.10; 0.20) | 1.43 (0.97; 1.89) | 0.74 (0.43; 1.05) | 1.63 (0.95; 2.32) | |
| Prediction interval | [−0.04; 0.22] | [−0.11; 0.40] | [−0.09; 0.39] | [−0.32; 3.18] | [−0.18; 1.66] | [−0.81; 4.08] | |
| Canines | n | 14 | 12 | 14 | 14 | 8 | 12 |
| MTE (95% CI) | 0.09 (0.05; 0.13) | 0.13 (0.07; 0.19) | 0.15 (0.09; 0.24) | 1.95 (1.15; 2.75) | 0.90 (0.47; 1.32) | 2.11 (1.13;3.09) | |
| Prediction interval | [−0.04; 0.22] | [−0.09; 0.34] | [−0.09; 0.40] | [−1.07; 4.97] | [−0.35; 2.15] | [−1.36; 5.58] | |
| Premolars | n | 16 | 14 | 16 | 16 | 16 | 10 |
| MTE (95% CI) | 0.09 (0.05; 0.13) | 0.10 (0.06; 0.14) | 0.13 (0.10;0.17) | 0.13 (0.10; 0.17) | 1.46 (0.97;1.94) | 0.95 (0.37; 1.53) | |
| Prediction interval | [−0.06; 0.24] | [−0.05; 0.24] | [−0.01; 0.27] | [−0.01; 0.27] | [−0.45; 3.36] | [−0.81; 2.71] | |
| Molars | n | 10 | 10 | 10 | 10 | 6 | 10 |
| MTE (95% CI) | 0.06 (0.04; 0.08) | 0.09 (−0.04; 0.13) | 0.11 (0.04; 0.18) | 1.47 (0.70; 2.23) | 0.69 (0.32; 1.06) | 2.29 (1.20; 3.38) | |
| Prediction interval | [0.01; 0.11] | [−0.04; 0.21] | [−0.08; 0.31] | [−0.99; 3.92] | [−0.26; 1.64] | [−1.24; 5.82] | |
| Left vs. Right | |||||||
| Left | n | 5 | 3 | 5 | 2 | - | - |
| MTE (95% CI) | 0.14 (0.04; 0.24) | 0.11 (0.06; 0.17) | 0.22 (0.10; 0.35) | 2.91 (−1.59; 7.41) | |||
| Prediction interval | [−0.14; 0.42] | [−0.12; 0.35] | [−0.13; 0.57] | - | |||
| Right | n | 5 | 3 | 5 | 2 | - | - |
| MTE (95% CI) | 0.14 (0.05; 0.22) | 0.10 (0.02; 0.17) | 0.23 (0.04; 0.42) | 2.66 (2.59; 2.72) | |||
| Prediction interval | [−0.10: 0.37] | [−0.29; 0.48] | [−0.30; 0.76] | ||||
| Upper vs. Lower | |||||||
| Upper | n | 9 | 7 | 9 | 6 | 4 | 4 |
| MTE (95% CI) | 0.10 (0.05; 0.16) | 0.09 (0.02; 0.15) | 0.18 (0.09; 0.26) | 1.26 (0.00; 2.53) | 0.59 (−0.49; 1.6) | 0.73 (−0.50; 1.96) | |
| Prediction interval | [−0.08; 0.29] | [−0.10; 0.27] | [−0.10; 0.45] | [−2.34; 4.86] | [−2.67; 3.85] | [−2.97; 4.43] | |
| Lower | n | 4 | 2 | 4 | 4 | 2 | 2 |
| MTE (95% CI) | 0.12 (−0.09; 0.33) | 0.01 (−0.04; 0.05) | 0.22 (−0.00; 0.44) | 1.49 (−1.10; 4.08) | 0.01 (−0.09;0.10) | 0.18 (0.01; 0.35) | |
| Prediction interval | [−0.52; 0.76] | [−0.10; 0.45]- | [−6.32; 9.31] | ||||
| 3D accuracy assessment vs. Photography | |||||||
| 3D | n | 18 | 18 | 18 | 18 | 17 | 18 |
| MTE (95% CI) | 0.06 (0.04; 0.08) | 0.09 (0.05; 0.12) | 0.11 (0.09; 0.13) | 0.95 (0.63; 1.27) | 0.93 (0.49; 1.37) | 1.11 (0.68; 1.53) | |
| Prediction interval | [−0.03; 0.15] | [−0.05; 0.22] | [0.03; 0.18] | [−0.42; 2.32] | [−0.88; 2.74] | [−0.61; 2.83] | |
| Photography | n | 7 | 5 | 7 | 2 | - | - |
| MTE (95% CI) | 0.12 (0.06; 0.18) | 0.09 (0.09; 0.10) | 0.22 (0.12; 0.31) | 2.74 (−1.50; 6.97) | |||
| Prediction interval | [−0.05; 0.30] | [ 0.09; 0.10] | [−0.07; 0.50] | - | |||
| Type of tray | |||||||
| 3D printed | n | 13 | 13 | 4 | 13 | 11 | 13 |
| MTE (95% CI) | 0.06 (0.03; 0.09) | 0.10 (0.06; 0.13) | 0.12 (0.09; 0.15) | 1.14 (0.69; 1.60) | 0.90 (0.36; 1.45) | 1.42 (0.76; 2.09) | |
| Prediction interval | [−0.05; 0.16] | [−0.04; 0.24] | [ 0.02; 0.21] | [−0.57; 2.86] | [−0.94; 2.75] | [−1.01; 3.86] | |
| Silicone | n | 4 | 3 | 4 | 3 | 2 | 2 |
| MTE (95% CI) | 0.10 (0.00; 0.19) | 0.08 (−0.01; 0.18) | 0.14 (−0.03; 0.32) | 1.17 (−1.55; 3.88) | 0.66 (−3.82; 5.13) | 0.79 (−4.47; 6.05) | |
| Prediction interval | [−0.20; 0.39] | [−0.44; 0.61] | [−0.38; 0.67] | [−14.17; 17.12] | |||
| Combined Silicone/Vacuum Form | n | 1 | 1 | 1 | - | - | - |
| MTE (95% CI) | 0.09 (0.07; 0.11) | 0.09 (0.07; 0.11) | 0.14 (0.11; 0.17) | ||||
| Prediction interval | - | - | - | ||||
| Vacuum Form | n | 6 | 5 | 6 | 5 | 4 | 4 |
| MTE (95% CI) | 0.10 (0.02; 0.18) | 0.08 (−0.03; 0.19) | 0.16 (0.03; 0.29) | 1.32 (−0.06; 2.71) | 1.16 (−0.84; 3.16) | 0.86 (0.26;1.46) | |
| Prediction interval | [−0.13; 0.33] | [−0.22; 0.39] | [−0.20; 0.52] | [−2.52; 5.17] | [−4.80; 7.13] | [−0.92; 2.63] | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sabbagh, H.; Khazaei, Y.; Baumert, U.; Hoffmann, L.; Wichelhaus, A.; Janjic Rankovic, M. Bracket Transfer Accuracy with the Indirect Bonding Technique—A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 2568. https://doi.org/10.3390/jcm11092568
Sabbagh H, Khazaei Y, Baumert U, Hoffmann L, Wichelhaus A, Janjic Rankovic M. Bracket Transfer Accuracy with the Indirect Bonding Technique—A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(9):2568. https://doi.org/10.3390/jcm11092568
Chicago/Turabian StyleSabbagh, Hisham, Yeganeh Khazaei, Uwe Baumert, Lea Hoffmann, Andrea Wichelhaus, and Mila Janjic Rankovic. 2022. "Bracket Transfer Accuracy with the Indirect Bonding Technique—A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 11, no. 9: 2568. https://doi.org/10.3390/jcm11092568
APA StyleSabbagh, H., Khazaei, Y., Baumert, U., Hoffmann, L., Wichelhaus, A., & Janjic Rankovic, M. (2022). Bracket Transfer Accuracy with the Indirect Bonding Technique—A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 11(9), 2568. https://doi.org/10.3390/jcm11092568