

The Association of Placental Abruption and Pediatric Neurological Outcome: A Systematic Review and Meta-Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria, Information Sources, Search Strategy
2.2. Study Selection
2.3. Data Extraction
2.4. Assessment of Risk of Bias
2.5. Data Synthesis
3. Results
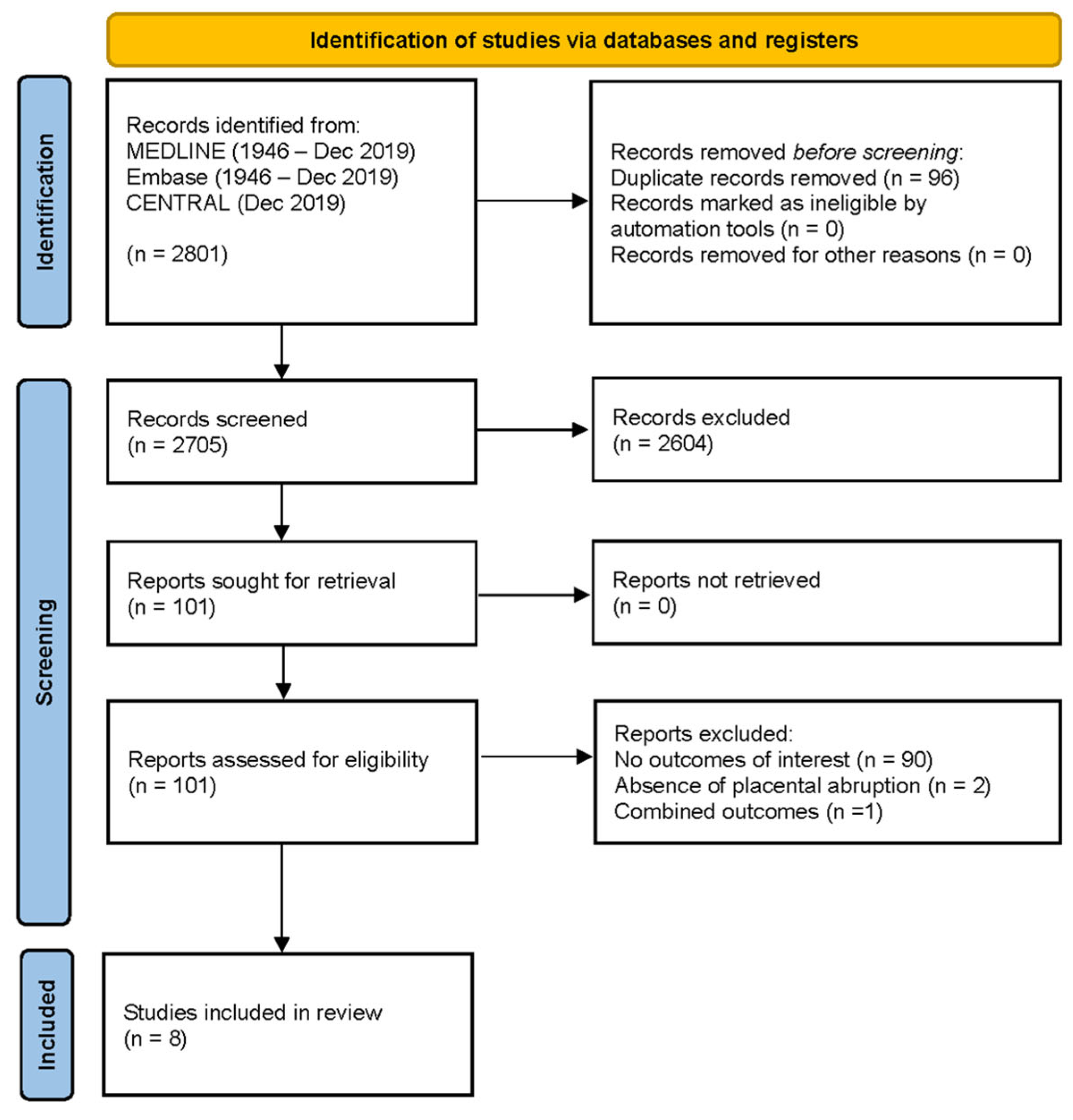
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias of Included Studies
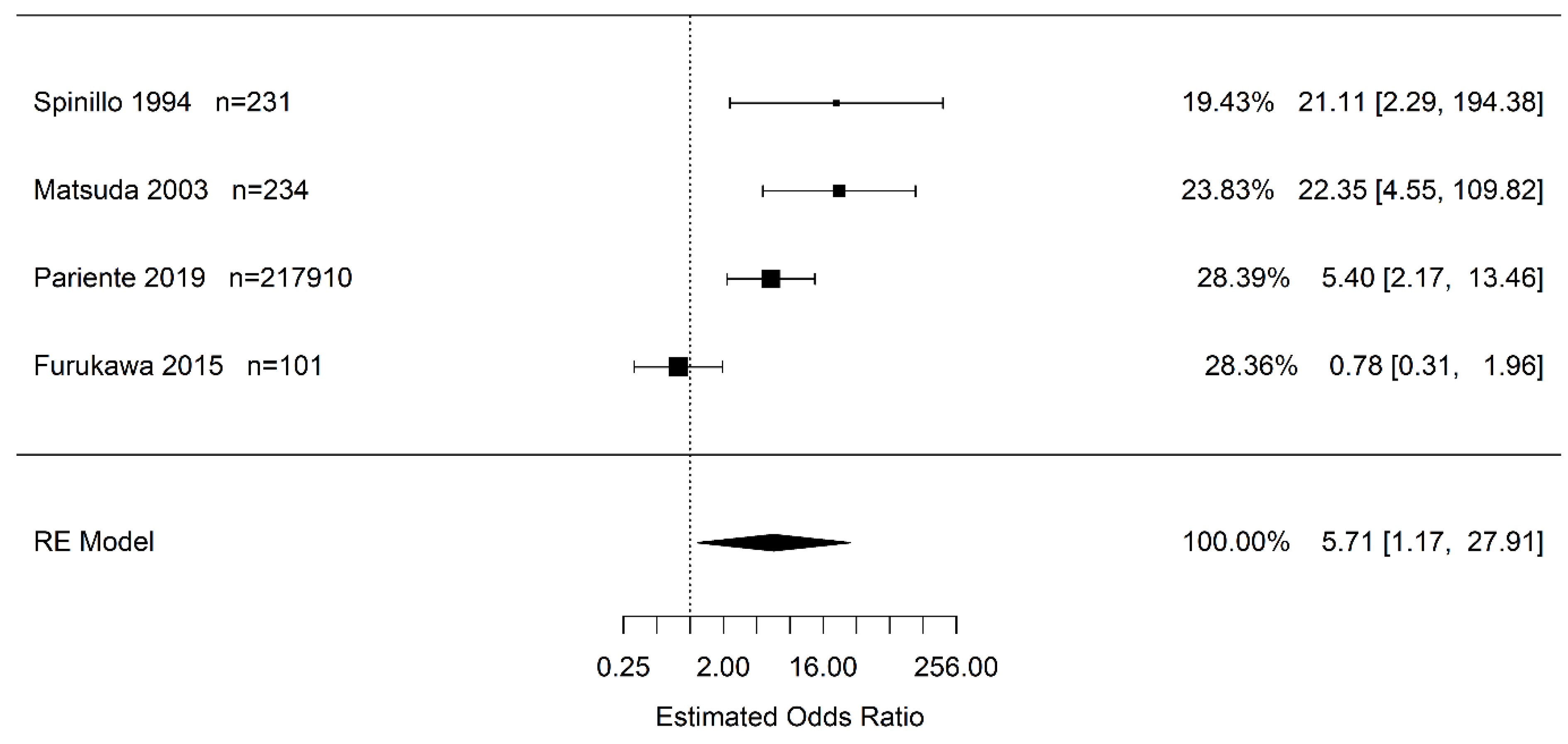
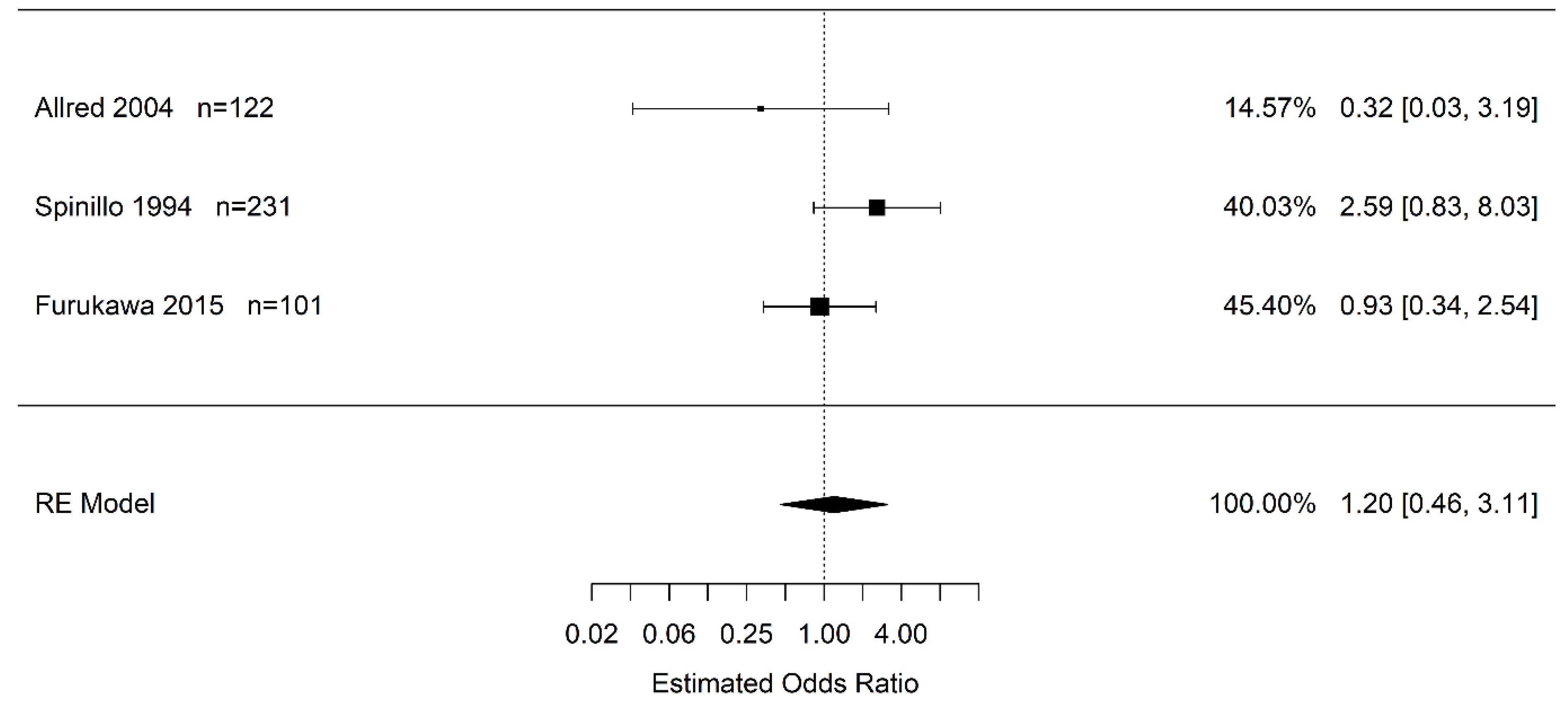
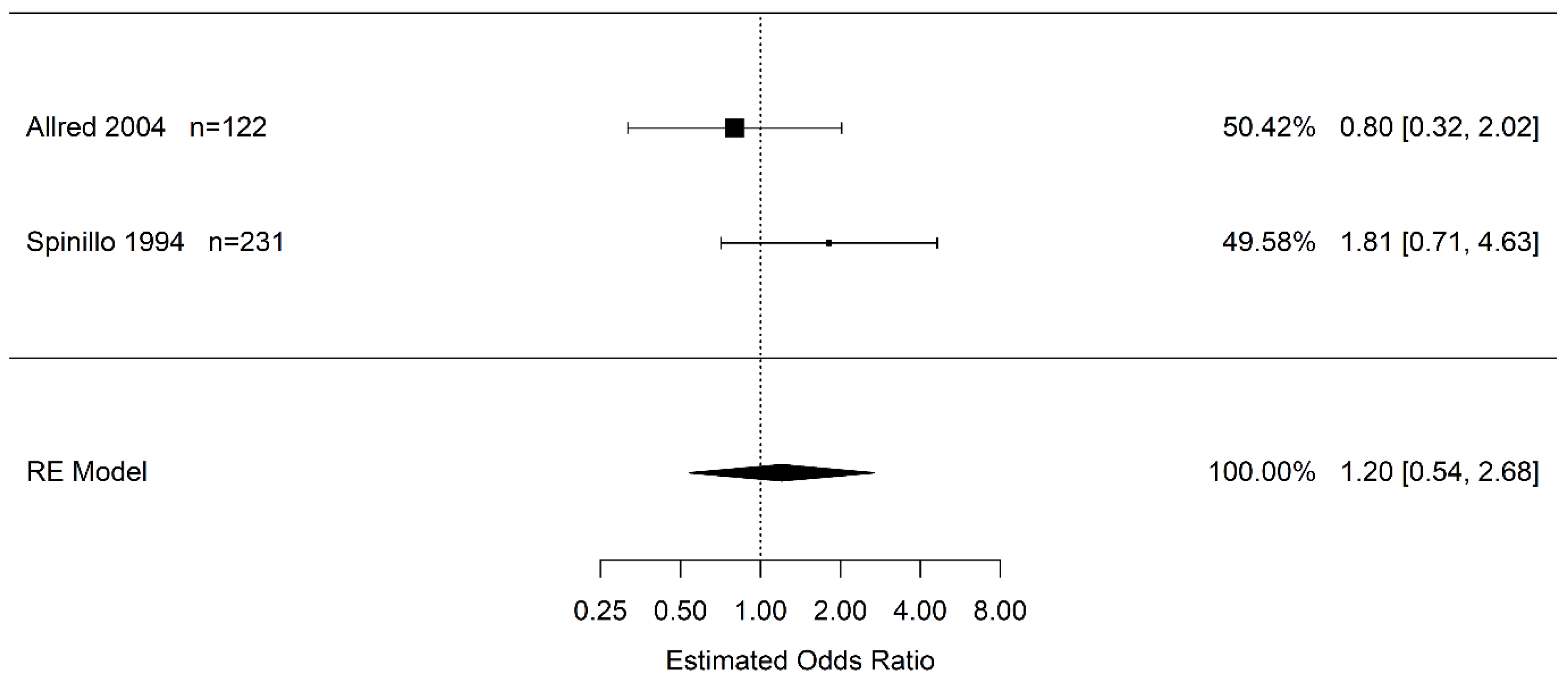
3.4. Synthesis of Results
4. Discussion
4.1. Principal Findings
4.2. Comparison with Existing Literature
4.3. Limitations
4.4. Conclusions and Implications
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ananth, C.V.; Keyes, K.M.; Hamilton, A.; Gissler, M.; Wu, C.; Liu, S.; Luque-Fernandez, M.A.; Skjærven, R.; Williams, M.A.; Tikkanen, M.; et al. An international contrast of rates of placental abruption: An age-period-cohort analysis. PLoS ONE 2015, 10, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Ananth, C.V.; Lavery, J.A.; Vintzileos, A.M.; Skupski, D.W.; Varner, M.; Saade, G.; Biggio, J.; Williams, M.A.; Wapner, R.J.; Wright, J.D. Severe placental abruption: Clinical definition and associations with maternal complications. Am. J. Obstet. Gynecol. 2016, 214, 272.e1–272.e9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oyelese, Y.; Ananth, C.V. Placental Abruption. Obstet. Gynecol. 2006, 108, 1005–1016. [Google Scholar] [CrossRef] [PubMed]
- Räisänen, S.; Gissler, M.; Saari, J.; Kramer, M.; Heinonen, S. Contribution of Risk Factors to Extremely, Very and Moderately Preterm Births—Register-Based Analysis of 1,390,742 Singleton Births. PLoS ONE 2013, 8, e60660. [Google Scholar] [CrossRef] [PubMed]
- Riihimäki, O.; Metsäranta, M.; Ritvanen, A.; Gissler, M.; Luukkaala, T.; Paavonen, J.; Nuutila, M.; Andersson, S.; Tikkanen, M. Increased Prevalence of Major Congenital Anomalies in Births with Placental Abruption. Obstet. Gynecol. 2013, 122, 268–274. [Google Scholar] [CrossRef]
- Redline, R.W. Severe fetal placental vascular lesions in term infants with neurologic impairment. Am. J. Obstet. Gynecol. 2005, 192, 452–457. [Google Scholar] [CrossRef]
- Kayani, S.I.; Walkinshaw, S.A.; Preston, C. Pregnancy outcome in severe placental abruption. BJOG Int. J. Obstet. Gynaecol. 2003, 110, 679–683. [Google Scholar] [CrossRef]
- Bonnar, J. Massive obstetric haemorrhage. Best Pract. Res. Clin. Obstet. Gynaecol. 2000, 14, 1–18. [Google Scholar] [CrossRef] [Green Version]
- López-Llera, M.; de la Luz Espinosa, M.; Arratia, C. Eclampsia and placental abruption: Basic patterns, management and morbidity. Int. J. Gynecol. Obstet. 1988, 27, 335–342. [Google Scholar] [CrossRef]
- Maye, J.P. Placental abruption: A case study. CRNA 1994, 5, 20–21. [Google Scholar]
- Downes, K.L.; Shenassa, E.D.; Grantz, K.L. Neonatal Outcomes Associated with Placental Abruption. Am. J. Epidemiol. 2017, 186, 1319–1328. [Google Scholar] [CrossRef]
- Pariente, G.; Wiznitzer, A.; Sergienko, R.; Mazor, M.; Holcberg, G.; Sheiner, E. Placental abruption: Critical analysis of risk factors and perinatal outcomes. J. Matern. Neonatal Med. 2011, 24, 698–702. [Google Scholar] [CrossRef]
- Riihimäki, O.; Metsäranta, M.; Paavonen, J.; Luukkaala, T.; Gissler, M.; Andersson, S.; Nuutila, M.; Tikkanen, M. Placental Abruption and Child Mortality. Pediatrics 2018, 142, e20173915. [Google Scholar] [CrossRef] [Green Version]
- Ananth, C.V. Placental Abruption and Adverse Perinatal Outcomes. JAMA 1999, 282, 1646. [Google Scholar] [CrossRef] [Green Version]
- DeRoo, L.; Skjærven, R.; Wilcox, A.; Klungsøyr, K.; Wikström, A.-K.; Morken, N.-H.; Cnattingius, S. Placental abruption and long-term maternal cardiovascular disease mortality: A population-based registry study in Norway and Sweden. Eur. J. Epidemiol. 2016, 31, 501–511. [Google Scholar] [CrossRef]
- Adams, T.; Yeh, C.; Bennett-Kunzier, N.; Kinzler, W.L. Long-term maternal morbidity and mortality associated with ischemic placental disease. Semin. Perinatol. 2014, 38, 146–150. [Google Scholar] [CrossRef]
- Pariente, G.; Shoham-Vardi, I.; Kessous, R.; Sherf, M.; Sheiner, E. Placental Abruption as a Significant Risk Factor for Long-term Cardiovascular Mortality in a Follow-up Period of More Than a Decade. Paediatr. Perinat. Epidemiol. 2014, 28, 32–38. [Google Scholar] [CrossRef]
- Ananth, C.V.; Hansen, A.V.; Elkind, M.S.V.; Williams, M.A.; Rich-Edwards, J.W.; Nybo Andersen, A.-M. Cerebrovascular disease after placental abruption. Neurology 2019, 93, e1148–e1158. [Google Scholar] [CrossRef]
- Whitehead, E.; Dodds, L.; Joseph, K.S.; Gordon, K.E.; Wood, E.; Allen, A.C.; Camfield, P.; Dooley, J.M. Relation of Pregnancy and Neonatal Factors to Subsequent Development of Childhood Epilepsy: A Population-Based Cohort Study. Pediatrics 2006, 117, 1298–1306. [Google Scholar] [CrossRef]
- Hasegawa, J.; Ikeda, T.; Toyokawa, S.; Jojima, E.; Satoh, S.; Ichizuka, K.; Tamiya, N.; Nakai, A.; Fujimori, K.; Maeda, T.; et al. Relevant obstetric factors associated with fetal heart rate monitoring for cerebral palsy in pregnant women with hypertensive disorder of pregnancy. J. Obstet. Gynaecol. Res. 2018, 44, 647–654. [Google Scholar] [CrossRef] [Green Version]
- Trønnes, H.; Wilcox, A.J.; Lie, R.T.; Markestad, T.; Moster, D. Risk of cerebral palsy in relation to pregnancy disorders and preterm birth: A national cohort study. Dev. Med. Child Neurol. 2014, 56, 779–785. [Google Scholar] [CrossRef] [PubMed]
- Ichizuka, K.; Toyokawa, S.; Ikenoue, T.; Satoh, S.; Hasegawa, J.; Ikeda, T.; Tamiya, N.; Nakai, A.; Fujimori, K.; Maeda, T.; et al. Risk factors for cerebral palsy in neonates due to placental abruption. J. Obstet. Gynaecol. Res. 2021, 47, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Himmelmann, K.; Ahlin, K.; Jacobsson, B.; Cans, C.; Thorsen, P. Risk factors for cerebral palsy in children born at term. Acta Obstet. Gynecol. Scand. 2011, 90, 1070–1081. [Google Scholar] [CrossRef] [PubMed]
- Pariente, G.; Wainstock, T.; Walfisch, A.; Landau, D.; Sheiner, E. Placental abruption and long-term neurological hospitalisations in the offspring. Paediatr. Perinat. Epidemiol. 2019, 33, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Nelson, D.B.; Lucke, A.M.; McIntire, D.D.; Sánchez, P.J.; Leveno, K.J.; Chalak, L.F. Obstetric antecedents to body-cooling treatment of the newborn infant. Am. J. Obstet. Gynecol. 2014, 211, 155.e1–155.e6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Locatelli, A.; Incerti, M.; Paterlini, G.; Doria, V.; Consonni, S.; Provero, C.; Ghidini, A. Antepartum and Intrapartum Risk Factors for Neonatal Encephalopathy at Term. Am. J. Perinatol. 2010, 27, 649–654. [Google Scholar] [CrossRef] [PubMed]
- Nasiell, J.; Papadogiannakis, N.; Löf, E.; Elofsson, F.; Hallberg, B. Hypoxic ischemic encephalopathy in newborns linked to placental and umbilical cord abnormalities. J. Matern. Neonatal Med. 2016, 29, 721–726. [Google Scholar] [CrossRef]
- Chen, H.-J.; Wei, K.-L.; Zhou, C.-L.; Yao, Y.-J.; Yang, Y.-J.; Fan, X.-F.; Gao, X.-R.; Liu, X.-H.; Qian, J.-H.; Wu, B.-Q.; et al. Incidence of brain injuries in premature infants with gestational age ≤34 weeks in ten urban hospitals in China. World J. Pediatr. 2013, 9, 17–24. [Google Scholar] [CrossRef]
- Dani, C.; Poggi, C.; Bertini, G.; Pratesi, S.; Di Tommaso, M.; Scarselli, G.; Rubaltelli, F.F. Method of delivery and intraventricular haemorrhage in extremely preterm infants. J. Matern. Neonatal Med. 2010, 23, 1419–1423. [Google Scholar] [CrossRef]
- Furukawa, S.; Doi, K.; Furuta, K.; Sameshima, H. The effect of placental abruption on the outcome of extremely premature infants. J. Matern. Neonatal Med. 2015, 28, 705–708. [Google Scholar] [CrossRef]
- Hjern, A.; Thorngren-Jerneck, K. Perinatal complications and socio-economic differences in cerebral palsy in Sweden—A national cohort study. BMC Pediatr. 2008, 8, 49. [Google Scholar] [CrossRef]
- Stelmach, T.; Pisarev, H.; Talvik, T. Ante- and perinatal factors for cerebral palsy: Case-control study in Estonia. J. Child Neurol. 2005, 20, 654–661. [Google Scholar] [CrossRef]
- Kułak, W.; Okurowska-Zawada, B.; Sienkiewicz, D.; Paszko-Patej, G.; Krajewska-Kułak, E. Risk factors for cerebral palsy in term birth infants. Adv. Med. Sci. 2010, 55, 216–221. [Google Scholar] [CrossRef]
- Hasegawa, J.; Toyokawa, S.; Ikenoue, T.; Asano, Y.; Satoh, S.; Ikeda, T.; Ichizuka, K.; Tamiya, N.; Nakai, A.; Fujimori, K.; et al. Relevant Obstetric Factors for Cerebral Palsy: From the Nationwide Obstetric Compensation System in Japan. PLoS ONE 2016, 11, e0148122. [Google Scholar] [CrossRef] [Green Version]
- Ananth, C.; Friedman, A.; Lavery, J.; VanderWeele, T.; Keim, S.; Williams, M. Neurodevelopmental outcomes in children in relation to placental abruption. BJOG Int. J. Obstet. Gynaecol. 2017, 124, 463–472. [Google Scholar] [CrossRef]
- Love, E.R.; Crum, J.; Bhattacharya, S. Independent effects of pregnancy induced hypertension on childhood development: A retrospective cohort study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2012, 165, 219–224. [Google Scholar] [CrossRef]
- Nielsen, L.; Schendel, D.; Grove, J.; Hvidtjørn, D.; Jacobsson, B.; Josiassen, T.; Vestergaard, M.; Uldall, P.; Thorsen, P. Asphyxia-related risk factors and their timing in spastic cerebral palsy. BJOG Int. J. Obstet. Gynaecol. 2008, 115, 1518–1528. [Google Scholar] [CrossRef]
- Downes, K.L.; Grantz, K.L.; Shenassa, E.D. Maternal, Labor, Delivery, and Perinatal Outcomes Associated with Placental Abruption: A Systematic Review. Am. J. Perinatol. 2017, 34, 935–957. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (Updated February 2022). Cochrane. 2022. Available online: www.training.cochrane.org/handbook (accessed on 15 December 2022).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Bramer, W.M.; De Jonge, G.B.; Rethlefsen, M.L.; Mast, F.; Kleijnen, J. A systematic approach to searching: An efficient and complete method to develop literature searches. J. Med. Libr. Assoc. 2018, 106, 531–541. [Google Scholar] [CrossRef] [Green Version]
- Prospero International Prospective Register of Systematic Reviews. Available online: https://www.crd.york.ac.uk/PROSPERO/ (accessed on 20 January 2021).
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)-A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Spinillo, A.; Fazzi, E.; Stronati, M.; Ometto, A.; Iasci, A.; Guaschino, S. Severity of abruptio placentae and neurodevelopmental outcome in low birth weight infants. Early Hum. Dev. 1993, 35, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Spinillo, A.; Fazzi, E.; Stronati, M.; Ometto, A.; Capuzzo, E.; Guaschino, S. Early Morbidity and Neurodevelopmental Outcome in Low-Birthweight Infants Born after Third Trimester Bleeding. Am. J. Perinatol. 1994, 11, 85–90. [Google Scholar] [CrossRef]
- Lv, H.Y.; Wang, Q.L.; Chen, H.Y.; You, Y.J.; Ren, P.S.; Li, L.X. Study on serum Tau protein level and neurodevelopmental outcome of placental abruption with neonatal hypoxic-ischemic encephalopathy. J. Matern. Neonatal Med. 2019, 33, 3887–3893. [Google Scholar] [CrossRef]
- Matsuda, Y.; Maeda, T.; Kouno, S. Comparison of neonatal outcome including cerebral palsy between abruptio placentae and placenta previa. Eur. J. Obstet. Gynecol. Reprod. Biol. 2003, 106, 125–129. [Google Scholar] [CrossRef]
- Page, E.W.; King, E.B.; Merrill, J.A. Abruptio placentae; dangers of delay in delivery. Obstet. Gynecol. 1954, 3, 385–393. [Google Scholar]
- Knab, D.R. Abruptio placentae. An assessment of the time and method of delivery. Obstet. Gynecol. 1978, 52, 625–629. [Google Scholar]
- Allred, L.S.; Batton, D. The Effect of Placental Abruption on the Short-Term Outcome of Premature Infants. Am. J. Perinatol. 2004, 21, 157–162. [Google Scholar] [CrossRef]
- Becher, J.C.; Bell, J.E.; Keeling, J.W.; Liston, W.A.; McIntosh, N.; Wyatt, B. The Scottish Perinatal Neuropathology Study—Clinicopathological correlation in stillbirths. BJOG Int. J. Obstet. Gynaecol. 2006, 113, 310–317. [Google Scholar] [CrossRef]
- Lee, H.; Aronson, J.; Nunan, D.; Collider Bias. Catalogue of Bias. Available online: https://catalogofbias.org/biases/collider-bias/ (accessed on 27 July 2021).
- Joseph, L. Confounding and Collinearity in Multiple Linear Regression. Available online: http://www.medicine.mcgill.ca/epidemiology/joseph/courses/epib-621/confounding.pdf (accessed on 15 December 2022).
- Wells, G.A.; Shea, B.; O’Connell, D.A.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses 2000. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 15 December 2022).
- Sharmin, S.; Kypri, K.; Khanam, M.; Wadolowski, M.; Bruno, R.; Attia, J.; Holliday, E.; Palazzi, K.; Mattick, R.P. Effects of parental alcohol rules on risky drinking and related problems in adolescence: Systematic review and meta-analysis. Drug Alcohol Depend. 2017, 178, 243–256. [Google Scholar] [CrossRef]
- R Core Team R: A Language and Environment for Statistical Computing. 2020. Available online: https://www.R-project.org (accessed on 15 December 2022).
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to perform a meta-analysis with R: A practical tutorial. Evid. Based. Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuda, Y.; Maeda, T.; Kouno, S. Fetal/neonatal outcome in abruptio placentae during preterm gestation. Semin. Thromb. Hemost. 2005, 31, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Deeks, J.J.; Higgins, J.P.T.; Altman, D.G. Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Wiley-Blackwell: Hoboken, NJ, USA, 2021; pp. 241–284. ISBN 9781119536604. Available online: https://onlinelibrary.wiley.com/doi/book/10.1002/9781119536604 (accessed on 15 December 2022).
- May, H.J.; Fasheun, J.A.; Bain, J.M.; Baugh, E.H.; Bier, L.E.; Revah-Politi, A.; Roye, D.P.; Goldstein, D.B.; Carmel, J.B.; Lippa, N.; et al. Genetic testing in individuals with cerebral palsy. Dev. Med. Child Neurol. 2021, 63, 1448–1455. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Sjölander, A.; Johansson, S.; Lu, D.; Razaz, N.; Tedroff, K.; Villamor, E.; Cnattingius, S. Impact of gestational age on risk of cerebral palsy: Unravelling the role of neonatal morbidity. Int. J. Epidemiol. 2021, 50, 1852–1863. [Google Scholar] [CrossRef] [PubMed]
- Yamada, T.; Yamada, T.; Morikawa, M.; Minakami, H. Clinical features of abruptio placentae as a prominent cause of cerebral palsy. Early Hum. Dev. 2012, 88, 861–864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamarca, B. Endothelial dysfunction. An important mediator in the pathophysiology of hypertension during pre-eclampsia. Minerva Ginecol. 2012, 64, 309–320. [Google Scholar]
- du Plessis, A.J.; Volpe, J.J. Perinatal brain injury in the preterm and term newborn. Curr. Opin. Neurol. 2002, 15, 151–157. [Google Scholar] [CrossRef]
- Williams, K.; Singh, A. The correlation of seizures in newborn infants with significant acidosis at birth with umbilical artery cord gas values. Obstet. Gynecol. 2002, 100, 557–560. [Google Scholar] [CrossRef]
- Graham, E.M.; Ruis, K.A.; Hartman, A.L.; Northington, F.J.; Fox, H.E. A systematic review of the role of intrapartum hypoxia-ischemia in the causation of neonatal encephalopathy. Am. J. Obstet. Gynecol. 2008, 199, 587–595. [Google Scholar] [CrossRef]
- Low, J.A.; Simpson, L.L.; Tonni, G.; Chamberlain, S. Limitations in the clinical prediction of intrapartum fetal asphyxia. Am. J. Obstet. Gynecol. 1995, 172, 801–804. [Google Scholar] [CrossRef]
- Matsuda, Y.; Umezaki, H.; Ogawa, M.; Ohwada, M.; Satoh, S.; Nakai, A. Umbilical arterial pH in patients with cerebral palsy. Early Hum. Dev. 2014, 90, 131–135. [Google Scholar] [CrossRef]
- Japan Council for Quality Health Care The Japan Obstetric Compensation System for Cerebral Palsy. In the 6th Recurrence Prevention Report. In Japanese; Tokyo. 2016. Available online: http://www.sanka-hp.jcqhc.or.jp/documents/english/pdf/looking_back_over10years_after_system_was_launched201905.pdf (accessed on 15 December 2022).
- Ananth, C.V.; Wilcox, A.J. Placental abruption and perinatal mortality in the United States. Am. J. Epidemiol. 2001, 153, 332–337. [Google Scholar] [CrossRef] [Green Version]
- Ananth, C.V. Placental Abruption among Singleton and Twin Births in the United States: Risk Factor Profiles. Am. J. Epidemiol. 2001, 153, 771–778. [Google Scholar] [CrossRef]
- Ananth, C.V.; Oyelese, Y.; Prasad, V.; Getahun, D.; Smulian, J.C. Evidence of placental abruption as a chronic process: Associations with vaginal bleeding early in pregnancy and placental lesions. Eur. J. Obstet. Gynecol. Reprod. Biol. 2006, 128, 15–21. [Google Scholar] [CrossRef]
- O’Leary, C.M.; Watson, L.; D’Antoine, H.; Stanley, F.; Bower, C. Heavy maternal alcohol consumption and cerebral palsy in the offspring. Dev. Med. Child Neurol. 2012, 54, 224–230. [Google Scholar] [CrossRef]
- Rasmussen, S.; Irgens, L.M. The effects of smoking and hypertensive disorders on fetal growth. BMC Pregnancy Childbirth 2006, 6, 16. [Google Scholar] [CrossRef] [Green Version]
- Messner, B.; Bernhard, D. Smoking and Cardiovascular Disease. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 509–515. [Google Scholar] [CrossRef] [Green Version]
- Tairy, D.; Weiner, E.; Kovo, M.; Zamir, A.M.; Gandelsman, E.; Levy, M.; Herman, H.G.; Volpert, E.; Schreiber, L.; Bar, J.; et al. Fetal Growth Restriction in Hypertensive vs. Heavy Smoking Women—Placental Pathology, Ultrasound Findings, and Pregnancy Outcomes. Reprod. Sci. 2021, 28, 819–827. [Google Scholar] [CrossRef]
- Hutcheon, J.A.; Lisonkova, S.; Joseph, K.S. Epidemiology of pre-eclampsia and the other hypertensive disorders of pregnancy. Best Pract. Res. Clin. Obstet. Gynaecol. 2011, 25, 391–403. [Google Scholar] [CrossRef]
- Chevallier, M.; Debillon, T.; Pierrat, V.; Delorme, P.; Kayem, G.; Durox, M.; Goffinet, F.; Marret, S.; Ancel, P.Y.; Arnaud, C.; et al. Leading causes of preterm delivery as risk factors for intraventricular hemorrhage in very preterm infants: Results of the EPIPAGE 2 cohort study. Am. J. Obstet. Gynecol. 2017, 216, 518.e1–518.e12. [Google Scholar] [CrossRef]
- Ballabh, P. Pathogenesis and Prevention of Intraventricular Hemorrhage. Clin. Perinatol. 2014, 41, 47–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perlman, J.M. Interruption of Placental Blood Flow during Labor: Potential Systemic and Cerebral Organ Consequences. J. Pediatr. 2011, 158, e1–e4. [Google Scholar] [CrossRef] [PubMed]
- Kumazaki, K.; Nakayama, M.; Sumida, Y.; Ozono, K.; Mushiake, S.; Suehara, N.; Wada, Y.; Fujimura, M. Placental features in preterm infants with periventricular leukomalacia. Pediatrics 2002, 109, 650–655. [Google Scholar] [CrossRef] [PubMed]
- Low, J.A.; Galbraith, R.S.; Muir, D.W.; Killen, H.L.; Pater, E.A.; Karchmar, E.J. Factors associated with motor and cognitive deficits in children after intrapartum fetal hypoxia. Am. J. Obstet. Gynecol. 1984, 148, 533–539. [Google Scholar] [CrossRef] [PubMed]
- Gonen, N.; Levy, M.; Kovo, M.; Schreiber, L.; Noy, L.K.; Volpert, E.; Bar, J.; Weiner, E. Placental Histopathology and Pregnancy Outcomes in “Early” vs. “Late” Placental Abruption. Reprod. Sci. 2021, 28, 351–360. [Google Scholar] [CrossRef] [PubMed]
- Weiner, E.; Feldstein, O.; Tamayev, L.; Grinstein, E.; Barber, E.; Bar, J.; Schreiber, L.; Kovo, M. Placental histopathological lesions in correlation with neonatal outcome in preeclampsia with and without severe features. Pregnancy Hypertens. 2018, 12, 6–10. [Google Scholar] [CrossRef]
- Paules, C.; Youssef, L.; Rovira, C.; Crovetto, F.; Nadal, A.; Peguero, A.; Figueras, F.; Eixarch, E.; Crispi, F.; Miranda, J.; et al. Distinctive patterns of placental lesions in pre-eclampsia vs small-for-gestational age and their association with fetoplacental Doppler. Ultrasound Obstet. Gynecol. 2019, 54, 609–616. [Google Scholar] [CrossRef]
- Sehgal, A.; Dahlstrom, J.E.; Chan, Y.; Allison, B.J.; Miller, S.L.; Polglase, G.R. Placental histopathology in preterm fetal growth restriction. J. Paediatr. Child Health 2019, 55, 582–587. [Google Scholar] [CrossRef]
- Raghavan, R.; Helfrich, B.B.; Cerda, S.R.; Ji, Y.; Burd, I.; Wang, G.; Hong, X.; Fu, L.; Pearson, C.; Daniele Fallin, M.; et al. Preterm birth subtypes, placental pathology findings, and risk of neurodevelopmental disabilities during childhood. Placenta 2019, 83, 17–25. [Google Scholar] [CrossRef]
- Bingham, A.; Gundogan, F.; Rand, K.; Laptook, A.R. Placental findings among newborns with hypoxic ischemic encephalopathy. J. Perinatol. 2019, 39, 563–570. [Google Scholar] [CrossRef]
- Straughen, J.K.; Misra, D.P.; Divine, G.; Shah, R.; Perez, G.; VanHorn, S.; Onbreyt, V.; Dygulska, B.; Schmitt, R.; Lederman, S.; et al. The association between placental histopathology and autism spectrum disorder. Placenta 2017, 57, 183–188. [Google Scholar] [CrossRef]
- Tokuhisa, T.; Ibara, S.; Minakami, H.; Maede, Y.; Ishihara, C.; Matsui, T. Outcome of infants with hypoxic ischemic encephalopathy treated with brain hypothermia. J. Obstet. Gynaecol. Res. 2015, 41, 229–237. [Google Scholar] [CrossRef] [Green Version]
- Broers, T.; King, W.D.; Arbuckle, T.E.; Liu, S. The occurrence of abruptio placentae in Canada: 1990 to 1997. Chronic Dis. Can. 2004, 25, 16–20. [Google Scholar]
- Nalivaeva, N.N.; Turner, A.J.; Zhuravin, I.A. Role of Prenatal Hypoxia in Brain Development, Cognitive Functions, and Neurodegeneration. Front. Neurosci. 2018, 12, 825. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors, Location (Year) | Inclusion Criteria and Dates; Data Source | Sample Size (Abruptions) | Sample Size (Non-Placental Abruption Pregnancies) | Cerebral Palsy (n) | Intraventricular Hemorrhage (n) | Hypoxic Ischemic Encephalopathy (n) | Periventricular Leukomalacia (n) | Histopathological Neuronal Damage (n) | Neonatal Mortality (n) |
|---|---|---|---|---|---|---|---|---|---|
| Cohort studies | |||||||||
| Pariente et al., Israel (2019) [24] | All women delivering at the Soroka University Medical Center (SUMC) from 1991 to 2014; single tertiary centre | 1003 | 216,907 | 8 | Not reported | Not reported | Not reported | Not reported | Not reported |
| Becher et al., Scotland (2006) [51] | All perinatal deaths that were ≥ 24 weeks gestation at birth and ≤ 7 days at time of death from 1996 to 1999; 22 obstetric units | 9 | 182 | Not reported | Not reported | Not reported | Not reported | 5 | Not reported |
| Case control studies | |||||||||
| Lv et al., China (2019) [46] | All neonates with (1) gestational age ≥ 37 weeks and weight ≥ 2500 g; (2) severe asphyxia at birth indicated by 1 min Apgar score ≤ 3 or a 5 min Apgar score ≤ 5; (3) umbilical artery blood pH ≤ 7 at birth; (4) abnormal neurological signs in the first 24 h of life from 2013 to 2017; single site | 18 | 35 | Not reported | Not reported | Case: Moderate HIE: 7Severe HIE: 11 Control: Moderate HIE: 0 Severe HIE: 0 | Not reported | Not reported | Not reported |
| Furukawa et al., Japan (2015) [30] | Infants born at 22 to around 26 weeks of gestation to women with placental abruption from 2000 to 2010; controls were infants born without abruption within 1 week of the non-control gestational age and birth weight of 50 g; single site | 32 | 69 | Case: 9 Control: 23 | Case: Grades III–IV IVH: 7 Control: Grades III–IV IVH: 16 | Not reported | Not reported | Not reported | Case: 6 Control: 8 |
| Allred et al., USA (2004) [50] | Live-born infants between 23 and 32 weeks gestation born to women with placental abruption from 1995 to 1999; controls were infants who did not suffer abruption within 100 g of weight and 1 week of gestation; single site | 61 | 61 | Not reported | Case: Unspecified IVH Grade 1 placental abruption: 6 Grade 2 placental abruption: 4 Grade III–IV IVH Grade 1 placental abruption: 1 Grade 2 placental abruption: 0 Control: Unspecified IVH: 0 Grades III-IV IVH: 3 | Not reported | Case: Grade 2 placental abruption: 1 Control: 0 | Not reported | Not reported |
| Matsuda et al., Italy (2003) [47] | Live singleton births between 26 and 36 weeks of gestation between 1992 and 1999; single site | 42 | 120 | Case: 8 Control: 1 | Not reported | Not reported | Not reported | Not reported | Case: 3 Control: 0 |
| Spinillo et al., Italy (1994) [45] | Singleton, liveborn low birthweight infants from 1983 to 1989; single site (database) | 40 | 154 | Not reported | Case: Grades I–II: 2 Grades III–IV: 5 Control: Grades I–II: 10 Grades III–IV: 6 | Not reported | Case: 2 Control: 1 | Not reported | Case: 4 Control: 19 |
| Spinillo et al., Italy (1993) [44] | Singleton, liveborn low birthweight infants from 1983 to 1989; single site (database) | 40 | 80 | Case: Group 1 placental abruption: 1 Group 2 placental abruption: 1 Group 3 placental abruption: 2 Control: 0 | Case: Grade I-II IVH Group 1 placental abruption: 1 Group 2 placental abruption: 1 Group 3 placental abruption: 1 Grade III–IV IVH:Group 2 placental abruption: 1 Group 3 placental abruption: 3 Control: Grade I–II IVH: 3 Grade III–IV IVH: 1 | Not reported | Case: Group 2 placental abruption: 1 Group 3 placental abruption: 1 Control: 0 | Not reported | Case: Group 1 placental abruption: 1 Group 2 placental abruption: 1 Group 3 placental abruption: 2 Control: 6 |
| Authors, Location (Year) | Mean Maternal Age in Years (SD) | Comorbidities (%) | Parity (%) | Caesarean Delivery (%) |
|---|---|---|---|---|
| Cohort studies | ||||
| Pariente et al., Israel (2019) [24] | Placental abruption: 29.6 (6.2) No placental abruption: 28.2 (5.7) | Placental abruption: Chronic hypertension—3.3 Gestational hypertension—12.3 Pre-eclampsia—10.5 Pre-gestational diabetes mellitus—7.5 Gestational diabetes mellitus—7.5 Smoking—1.4 No placental abruption:Chronic hypertension—1.4 Gestational hypertension—5.2 Pre-eclampsia—4.1 Pre-gestational diabetes mellitus—5.4 Gestational diabetes mellitus—5.5 Smoking—1.1 | Placental abruption: One—23.5 Two—19.2 Three or more—57.2 No placental abruption: One—24.8 Two—22.8 Three or more—52.4 | Placental abruption: 75.8 No placental abruption: 13.8 |
| Becher et al., Scotland (2006) [51] | 28.8 (6.6) | Complicated pregnancy: 64 | Multiple gestation: 7 | N/A |
| Case control studies | ||||
| Lv et al., China (2019) [46] | Placental abruption: 25.7 (20.0, 37.0) (median, min–max) Control: 26.1 (18.0, 39.0) (median, min–max) | Not reported | Not reported | Placental abruption: 38.9 Control: 42.9 |
| Furukawa et al., Japan (2015) [30] | Placental abruption: 29.3 (5.8) Control: 29.9 (4.9) | Placental abruption: Hypertension—1 Control: Hypertension—1 | Placental abruption: Primipara: 41 Control: Primipara: 32 | Placental abruption: 56 Control: 67 |
| Allred et al., USA (2004) [50] | Not reported | Not reported | Not reported | Grade 1 placental abruption: 53 Grade 2 placental abruption: 96 Control group 1: 42 Control group 2: 78 |
| Matsuda et al., Italy (2003) [47] | Placental abruption: 31.5 (5.1) Control: 28.7 (4.4) | Not reported | Placental abruption: Multipara: 42.9 Control: Multipara: 30 | Placental abruption: 90.4 Control: 47.5 |
| Spinillo et al., Italy (1994) [45] | Placental abruption: 26.9 (3.8) Control: 28.3 (4.9) | Placental abruption:Smoking: 32.5 Control: Smoking: 30 | Placental abruption: 1 (20) 2 (27.5) Control: 1 (28.6) 2 (22.1) | Placental abruption: Elective—17.5 Emergency—52.5 Control: Elective—31.2 Emergency—13.6 |
| Spinillo et al., Italy (1993) [44] | Placental abruption: 26.9 (3.8) Control: 28.5 (4.5) | Placental abruption: Smoking—32.5 Control: Smoking—30 | Placental abruption: One—20 Two: 27.5 Control: One—28.6 Two—22.1 | Placental abruption: Elective—17.5 Emergency—52.5 Control: Elective—45 Emergency—10 |
| Authors, Location (Year) | Mean Gestational Age in Weeks (SD) | Mean Birth Weight in g, (SD) | Preterm Delivery (%) | Apgar Scores (%) | Cord Gas pH (%) | Male Sex (%) | Caesarean Delivery (%) |
|---|---|---|---|---|---|---|---|
| Cohort studies | |||||||
| Pariente et al., Israel (2019) [24] | Placental abruption: 36.5 (3.5) Control: 39.1 (1.7) | Placental abruption: 2630 (76) Control: 3224 (48) | Placental abruption: 42.9 Control: 6.2 | Placental abruption: 1 min Apgar < 4: 11.2 5 min Apgar < 4: 0.89 Control: 1 min Apgar < 4: 0.7 5 min Apgar < 4: 0.08 | Not reported | Placental abruption: 53.2 Control: 50.9 | Placental abruption: 75.8 Control: 13.8 |
| Becher et al., Scotland (2006) [51] | 33.4 (5.3) | Not reported | Growth restricted preterm: 23 | Not reported | Not reported | 48 | Not reported |
| Case control studies | |||||||
| Lv et al., China (2019) [46] | Placental abruption: 38.6 (37.0, 41.0) (median, min–max) Control: 39.1 (37.0, 41.0) (median, min–max) | Placental abruption: 3290 (2550, 4100) (median, min–max) Control: 3325 (2500, 4600) (median, min–max) | Not reported | Placental abruption: 1 min Apgar score: 1.91 (1.23, 2.67) (median, min–max) 5 min Apgar score: 3.25 (1.76, 4.51) Control: 1 min Apgar score: 8.48 (7.63, 9.52) (median, min–max) 5 min Apgar score: 9.52 (8.35, 9.61) | Not reported | Placental abruption: 50 Control: 60 | Placental abruption: 38.9 Control: 42.9 |
| Furukawa et al., Japan (2015) [30] | Placental abruption: 24.2 (1.3) Control: 24.2 (1.2) | Placental abruption: 649 (143) Control: 643 (125) | Not reported | Not reported | Cord pH < 7.1 Placental abruption: 0 Control: 3 | Placental abruption: 56 Control: 49 | Placental abruption: 56 Control: 67 |
| Allred et al., USA (2004) [50] | Grade 1 placental abruption: 29.4 (2.6) Grade 2 placental abruption: 27.5 (2.9) Control group 1:29.4 (2.6) Control group 2: 27.6 (2.8) | Grade 1 placental abruption: 1358 (402) Grade 2 placental abruption: 1089 (414) Control group 1: 1369 (388) Control group 2: 1124 (428) | Not reported | Grade 1 placental abruption: Apgar score 3 at 1 min: 8 Apgar score 5 at 5 min: 0 Grade 2 placental abruption: Apgar score 3 at 1 min: 35 Apgar score 5 at 5 min: 17 Control group 1: Apgar score 3 at 1 min: 5 Apgar score 5 at 5 min: 0 Control group 2: Apgar score 3 at 1 min: 13 Apgar score 5 at 5 min: 0 | Cord pH < 7.0: Grade 1 placental abruption: 0 Grade 2 placental abruption: 22 Control: Group 1: 0 Group 2: 0 | Not reported | Grade 1 placental abruption: 53 Grade 2 placental abruption: 96 Control group 1: 42 Control group 2: 78 |
| Matsuda et al., Italy (2003) [47] | Placental Abruption: 31.2 (3.4) Control: 30.5 (3.8) | Placental abruption: 1670 (533) Control: 2010 (583) | Not reported | Placental abruption: Apgar score at 1 min (<7): 46 Apgar score at 5 min (<7): 26.2 Control: Apgar score at 1 min (<7): 19.2 Apgar score at 5 min (<7): 0.8 | Fetal acidemia (<7.0): Placental abruption: 33.3 Control: 0.8 | Not reported | Placental abruption: 90.4 Control: 47.5 |
| Spinillo et al., Italy (1994) [45] | Placental abruption 33.4 (3.4) Control: 32.7 (4.0) | Placental abruption: 1800 (458) Control: 32.7 (4.0) | Not reported | Not reported | Acidemia (pH < 7.2 in the first 12 h): Placental abruption: 30 Control: 16.2 | Not reported | Placental abruption: Elective caesarean—17.5 Emergency caesarean—52.5 Control: Elective caesarean—31.2 Emergency caesarean—13.6 |
| Spinillo et al., Italy (1993) [44] | Grade 1 placental abruption: 33.1 (3.8) Grade 2 placental abruption: 32.9 (43.2) Grade 3 placental abruption: 33.9 (3.3) Control: 33.4 (3.3) | Grade 1 placental abruption: 1801 (476) Grade 2 placental abruption: 1760 (506) Grade 3 placental abruption: 1855 (430) Control: 1811 (553) | Not reported | Grade 1 placental abruption: Apgar score at 1 min 7.2: 2.0 Apgar score at 5 min 8.4: 1.6 Grade 2 placental abruption: Apgar score at 1 min: 6.6 (2.5) Apgar score at 5 min: 7.2 (2.2) Grade 3 placental abruption: Apgar score at 1 min: 5.2 (3.0) Apgar score at 5 min: 6.6 (2.4) Control: Apgar score at 1 min: 7.1 (2.6) Apgar score at 5 min: 8.2 (1.8) | Acidemia (pH < 7.2 in the first 12 h: Grade 1 Placental abruption: 16.7 Grade 2 placental abruption: 16.7 Grade 3 placental abruption: 50.0 Control: 20.0 | Grade 1 placental abruption: 25.0 Grade 2 placental abruption: 50.0 Grade 3 placental abruption: 43.7 Control: 58.8 | Placental abruption: Elective caesarean—17.5 Emergency caesarean—52.5 Controls: Elective caesarean—45 Emergency caesarean—10 |
| Study | Selection | Comparability | Outcome | Quality SCORE | |||||
|---|---|---|---|---|---|---|---|---|---|
| Representativeness of Cases | Selection of Controls | Ascertainment of Abruption | Outcome Assessed Prior to Study | Comparability of Study Groups | Assessment of Outcome | Long Follow-Up | Follow-Up Adequacy | ||
| Allred et al., (2004) [50] | Participants were from one hospital ★ | Derived from same population ★ | Hospital records ★ | No | No mention of matching or adjustment | Record linkage ★ | No | No | Poor |
| Matsuda et al., (2003) [47] | Participants were from one hospital ★ | Derived from same population ★ | Hospital records including imaging and pathology reports ★ | No | Matched/adjusted for confounding factors ★ | Record linkage ★ | No | No | Fair |
| Spinillo et al., (1994) [45] | Participants were from one hospital ★ | Derived from same population ★ | Hospital records including imaging and pathology reports ★ | No | Matched/adjusted for confounding factors ★ | Record linkage ★ | Yes, at least 24 months ★ | Follow-up rate less than 95% and no description of those lost ★ | Good |
| Pariente et al., (2019) [24] | Participants were from one hospital ★ | Derived from same population ★ | Hospital records ★ | No | Matched/adjusted for confounding factors ★ | Record linkage ★ | Yes, at least 24 months ★ | Complete follow-up, that is, all subjects accounted for ★ | Good |
| Furukawa et al., (2015) [30] | Participants were from one hospital ★ | Derived from same population ★ | Hospital records ★ | No | No mention of matching or adjustment | Independent blind assessment ★ | No | No | Poor |
| Becher et al., (2005) [51] | Participants were from several hospitals ★ | Derived from same population ★ | Interview of caregivers—not blinded | No | No mention of matching or adjustment | Independent blind assessment ★ | No | No | Poor |
| Lv et al., (2018) [46] | Participants were from one hospital ★ | Derived from same population ★ | Hospital records including imaging ★ | No | No mention of matching or adjustment | Record linkage ★ | No | No | Poor |
| Spinillo et al., (1993) [44] | Participants were from one hospital ★ | Derived from same population ★ | Hospital records including imaging and pathology reports ★ | No | Matched/adjusted for confounding factors ★ | Record linkage ★ | Yes, at least 24 months ★ | Follow-up rate less than 95% and no description of those lost ★ | Good |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oltean, I.; Rajaram, A.; Tang, K.; MacPherson, J.; Hondonga, T.; Rishi, A.; Toltesi, R.; Gowans, R.; Jahangirnia, A.; Nasr, Y.; et al. The Association of Placental Abruption and Pediatric Neurological Outcome: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 205. https://doi.org/10.3390/jcm12010205
Oltean I, Rajaram A, Tang K, MacPherson J, Hondonga T, Rishi A, Toltesi R, Gowans R, Jahangirnia A, Nasr Y, et al. The Association of Placental Abruption and Pediatric Neurological Outcome: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(1):205. https://doi.org/10.3390/jcm12010205
Chicago/Turabian StyleOltean, Irina, Ajay Rajaram, Ken Tang, James MacPherson, Tadiwanashe Hondonga, Aanchal Rishi, Regan Toltesi, Rachel Gowans, Ashkan Jahangirnia, Youssef Nasr, and et al. 2023. "The Association of Placental Abruption and Pediatric Neurological Outcome: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 1: 205. https://doi.org/10.3390/jcm12010205
APA StyleOltean, I., Rajaram, A., Tang, K., MacPherson, J., Hondonga, T., Rishi, A., Toltesi, R., Gowans, R., Jahangirnia, A., Nasr, Y., Lawrence, S. L., & El Demellawy, D. (2023). The Association of Placental Abruption and Pediatric Neurological Outcome: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 12(1), 205. https://doi.org/10.3390/jcm12010205