
Invisalign Treatment of a Three-Year-Old Child with Bilateral Posterior Scissor Bite and Multisite Upper Airway Obstruction: A Case Report

Abstract
:1. Introduction
2. Materials and Methods
2.1. Diagnosis and Etiology
2.2. Treatment Objectives
2.3. Treatment Alternatives
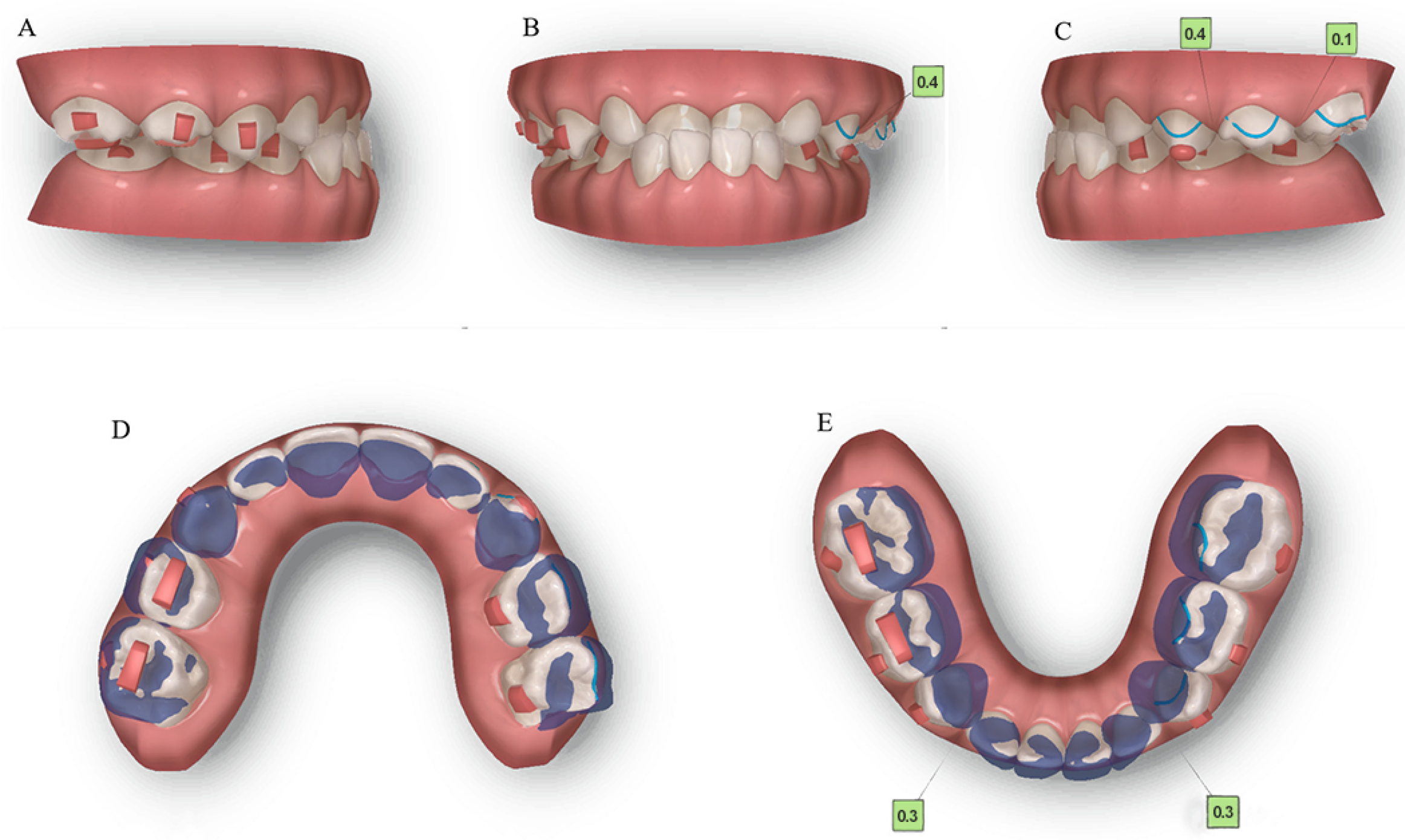
2.4. Treatment Progress
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- King, J.W.; Wallace, J.C. Unilateral Brodie bite treated with distraction osteogenesis. Am. J. Orthod. Dentofac. Orthop. 2004, 125, 500–509. [Google Scholar] [CrossRef]
- Moss, M.L. The function matrix. In Vistas of Orthodontics; Kraus, B.S., Riedel, R.A., Eds.; Lea and Febiger: Philadelphia, PA, USA, 1962; pp. 85–98. [Google Scholar]
- Sullivan, S.S.; Guilleminault, C. Can we avoid development of a narrow upper airway and secondary abnormal breathing during sleep? Lancet Respir. Med. 2017, 5, 843–844. [Google Scholar] [CrossRef] [PubMed]
- Nunes, W.R., Jr.; Di Francesco, R.C. Variation of patterns of malocclusion by site of pharyngeal obstruction in children. Arch. Otolaryngol. Head Neck Surg. 2010, 136, 1116–1120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diouf, J.S.; Ngom, P.I.; Sonko, O.; Diop-Bâ, K.; Badiane, A.; Diagne, F. Influence of tonsillar grade on the dental arch measurements. Am. J. Orthod. Dentofac. Orthop. 2015, 147, 214–220. [Google Scholar] [CrossRef]
- Franco, L.P.; Souki, B.Q.; Cheib, P.L.; Abrão, M.; Pereira, T.B.; Becker, H.M.; Pinto, J.A. Are distinct etiologies of upper airway obstruction in mouth-breathing children associated with different cephalometric patterns? Int. J. Pediatr. Otorhinolaryngol. 2015, 79, 223–228. [Google Scholar] [CrossRef]
- Buschang, P.H.; Chastain, D.; Keylor, C.L.; Crosby, D.; Julien, K.C. Incidence of white spot lesions among patients treated with clear aligners and traditional braces. Angle Orthod. 2019, 89, 359–364. [Google Scholar] [CrossRef] [Green Version]
- d’Apuzzo, F.; Perillo, L.; Carrico, C.K.; Castroflorio, T.; Grassia, V.; Lindauer, S.J.; Shroff, B. Clear aligner treatment: Different perspectives between orthodontists and general dentists. Prog. Orthod. 2019, 20, 10. [Google Scholar] [CrossRef] [Green Version]
- Sfondrini, M.F.; Debiaggi, M.; Zara, F.; Brerra, R.; Comelli, M.; Bianchi, M.; Pollone, S.R.; Scribante, A. Influence of lingual bracket position on microbial and periodontal parameters in vivo. J. Appl. Oral Sci. 2012, 20, 357–361. [Google Scholar] [CrossRef] [Green Version]
- Sun, F.; Ahmed, A.; Wang, L.; Dong, M.; Niu, W. Comparison of oral microbiota in orthodontic patients and healthy individuals. Microb. Pathog. 2018, 123, 473–477. [Google Scholar] [CrossRef]
- Fujioka, M.; Young, L.W.; Girdany, B.R. Radiographic evaluation of adenoidal size in children: Adenoidal-nasopharyngeal ratio. AJR Am. J. Roentgenol. 1979, 133, 401–404. [Google Scholar] [CrossRef]
- Zou, M. The adenoid-nasopharynx ratio: Its clinical value in children. Chin. J. Radiol. 1997, 31, 43–45. (In Chinese) [Google Scholar]
- Tamamura, N.; Kuroda, S.; Sugawara, Y.; Takano-Yamamoto, T.; Yamashiro, T. Use of palatal miniscrew anchorage and lingual multi-bracket appliances to enhance efficiency of molar scissors-bite correction. Angle Orthod. 2009, 79, 577–584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baik, U.B.; Kim, M.R.; Yoon, K.H.; Kook, Y.A.; Park, J.H. Orthodontic uprighting of a horizontally impacted third molar and protraction of mandibular second and third molars into the missing first molar space for a patient with posterior crossbites. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 572–582. [Google Scholar] [CrossRef] [PubMed]
- Harper, D.L. A case report of a Brodie bite. Am. J. Orthod. Dentofac. Orthop. 1995, 108, 201–206. [Google Scholar] [CrossRef]
- O’Brien, K.; Wright, J.; Conboy, F.; Sanjie, Y.; Mandall, N.; Chadwick, S.; Connolly, I.; Cook, P.; Birnie, D.; Hammond, M.; et al. Effectiveness of treatment for Class II malocclusion with the Herbst or twin-block appliances: A randomized, controlled trial. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 128–137. [Google Scholar] [CrossRef]
- O’Brien, K.; Wright, J.; Conboy, F.; Sanjie, Y.; Mandall, N.; Chadwick, S.; Connolly, I.; Cook, P.; Birnie, D.; Hammond, M.; et al. Effectiveness of early orthodontic treatment with the Twin-block appliance: A multicenter, randomized, controlled trial. Part 1: Dental and skeletal effects. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 234–243. [Google Scholar] [CrossRef]
- Tinano, M.M.; Godinho, J.; Becker, H.M.G.; Franco, L.P.; Souki, B.Q. Prevalence of malocclusion in children with upper airway obstruction. Rev. Port. Estomatol. Med. Dent. Cir. Maxilofac. 2017, 58, 199–204. [Google Scholar] [CrossRef] [Green Version]
- Subtelny, J.D. Oral respiration: Facial maldevelopment and corrective dentofacial orthopedics. Angle Orthod. 1980, 50, 147–164. [Google Scholar]
- Harvold, E.P.; Tomer, B.S.; Vargervik, K.; Chierici, G. Primate experiments on oral respiration. Am. J. Orthod. 1981, 79, 359–372. [Google Scholar] [CrossRef]
- Josell, S.D. Habits affecting dental and maxillofacial growth and development. Dent. Clin. N. Am. 1995, 39, 851–860. [Google Scholar] [CrossRef]
- Straub, J.W. Frequency of allergy in orthodontic patients. J. Am. Dent. Assoc. 1994, 31, 334–342. [Google Scholar] [CrossRef]
- Modrzynski, M.; Zawisza, E. An analysis of the incidence of adenoid hypertrophy in allergic children. Int. J. Pediatr. Otorhinolaryngol. 2007, 71, 713–719. [Google Scholar] [CrossRef] [PubMed]
- Cho, K.-S.; Kim, S.H.; Hong, S.-L.; Lee, J.; Mun, S.J.; Roh, Y.E.; Kim, Y.M.; Kim, H.-Y. Local Atopy in Childhood Adenotonsillar Hypertrophy. Am. J. Rhinol. Allergy 2018, 32, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Jin, X.; Han, Y.; Guo, R.; Ni, S.; Zou, J.; Wang, Y.; Li, Y. Correlation between allergy factors and maxillofacial malformation in children with tonsil and adenoid hypertrophy in denture replacement period. J. Otolaryngol. Ophthalmol. Shandong Univ. 2022, 36, 45–50. (In Chinese) [Google Scholar]
- Iwasaki, T.; Sato, H.; Suga, H.; Takemoto, Y.; Inada, E.; Saitoh, I.; Kakuno, E.; Kanomi, R.; Yamasaki, Y. Relationships among nasal resistance, adenoids, tonsils, and tongue posture and maxillofacial form in Class II and Class III children. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 929–940. [Google Scholar] [CrossRef] [PubMed]
- Valera, F.C.; Travitzki, L.V.; Mattar, S.E.; Matsumoto, M.A.; Elias, A.M.; Anselmo-Lima, W.T. Muscular, functional and orthodontic changes in pre school children with enlarged adenoids and tonsils. Int. J. Pediatr. Otorhinolaryngol. 2003, 67, 761–770. [Google Scholar] [CrossRef]
- Primozic, J.; Farcnik, F.; Perinetti, G.; Richmond, S.; Ovsenik, M. The association of tongue posture with the dentoalveolar maxillary and mandibular morphology in Class III malocclusion: A controlled study. Eur. J. Orthod. 2013, 35, 388–393. [Google Scholar] [CrossRef] [Green Version]
- Volk, J.; Kadivec, M.; Mušič, M.M.; Ovsenik, M. Three-dimensional ultrasound diagnostics of tongue posture in children with unilateral posterior crossbite. Am. J. Orthod. Dentofac. Orthop. 2010, 138, 608–612. [Google Scholar] [CrossRef]
- Laskowska, M.; Olczak-Kowalczyk, D.; Zadurska, M.; Czubak, J.; Czubak-Wrzosek, M.; Walerzak, M.; Tyrakowski, M. Evaluation of a relationship between malocclusion and idiopathic scoliosis in children and adolescents. J. Child. Orthop. 2019, 13, 600–606. [Google Scholar] [CrossRef]
- Butera, A.; Gallo, S.; Pascadopoli, M.; Taccardi, D.; Scribante, A. Home Oral Care of Periodontal Patients Using Antimicrobial Gel with Postbiotics, Lactoferrin, and Aloe Barbadensis Leaf Juice Powder vs. Conventional Chlorhexidine Gel: A Split-Mouth Randomized Clinical Trial. Antibiotics 2022, 11, 118. [Google Scholar] [CrossRef]
- Frey, L.; Green, S.; Fabbie, P.; Hockenbury, D.; Foran, M.; Elder, K. The Essential Role of the Com in the Management of Sleep-Disordered Breathing: A Literature Review and Discussion. Int. J. Orofac. Myol. 2014, 40, 42–55. [Google Scholar] [CrossRef]
- Maspero, C.; Prevedello, C.; Giannini, L.; Galbiati, G.; Farronato, G. Atypical swallowing: A review. Minerva Stomatol. 2014, 63, 217–227. (In Italian) [Google Scholar] [PubMed]
- Daglio, S.; Schwitzer, R.; Wüthrich, J. Orthodontic changes in oral dyskinesia and malocclusion under the influence of myofunctional therapy. Int. J. Orofac. Myol. 1993, 19, 15–24. [Google Scholar] [CrossRef]
- Takahashi, O.; Iwasawa, T.; Takahashi, M. Integrating orthodontics and oral myofunctional therapy for patients with oral myofunctional disorders. Int. J. Orofac. Myol. 1995, 21, 66–72. [Google Scholar] [CrossRef]





















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Norm | Pre-Treatment | Post-Treatment | Change |
|---|---|---|---|---|
| Angular (°) | ||||
| SNA | 82.0 ± 3.0 | 75.0 | 76.2 | 1.2 |
| SNB | 78.0 ± 3.0 | 69.7 | 70.8 | 1.1 |
| ANB | 3.0 ± 2.0 | 5.4 | 5.3 | −0.1 |
| Na-S-Ar | 123.0 ± 5.0 | 126.8 | 125.5 | −1.3 |
| Ar-Go′-Me | 123.0 ± 7.0 | 125.9 | 126.9 | 1.0 |
| GoGn-SN | 31.2 ± 3.6 | 38.6 | 40.8 | 2.2 |
| FH-NPo | 85.0 ± 4.0 | 79.5 | 80.9 | 1.4 |
| FH-MP | 26.0 ± 4.0 | 29.6 | 33.0 | 3.4 |
| SN-MP | 30.0 ± 6.0 | 39.8 | 44.8 | 5.0 |
| SN-OP | 19.0 ± 4.0 | 34.1 | 25.9 | −8.2 |
| MP-OP | 11.0 ± 5.0 | 5.8 | 19.0 | 13.2 |
| U1-SN | 106.0 ± 6.0 | 80.2 | 91.3 | 11.1 |
| L1-FH | 55.0 ± 2.0 | 52.2 | 62.7 | 10.5 |
| L1-MP | 97.0 ± 6.0 | 98.2 | 84.4 | −13.8 |
| U1-L1 | 124.0 ± 8.0 | 141.9 | 139.6 | −2.3 |
| Linear (mm) | ||||
| S-N | 71.0 ± 3.0 | 81.1 | 63.4 | −17.7 |
| N-Me | 112.0 ± 7.0 | 123.3 | 100.3 | −23.0 |
| N-Go′ | 95.0 ± 4.0 | 124.9 | 99.7 | −25.2 |
| S-Go′ | 80.0 ± 6.0 | 73.4 | 59.6 | −13.8 |
| Y-axis length | 86.0 ± 6.0 | 117.7 | 94.6 | −23.1 |
| LL-EP | 1.0 ± 2.0 | 6.5 | 3.0 | −3.5 |
| UL-EP | −1.0 ± 1.0 | 4.5 | 4.0 | −0.5 |
| Wits | 0.0 ± 2.0 | −4.7 | 1.0 | 5.7 |
| PNS-R | 25.5 ± 3.0 | 16.8 | 19.0 | 2.2 |
| PNS-UPW | 31.4 ± 4.2 | 22.8 | 22.3 | −0.5 |
| U-MPW | 11.5 ± 2.9 | 15.9 | 14.4 | −1.5 |
| PAS (TB-TPPW) | 13.5 ± 3.4 | 25.1 | 15.1 | −10.0 |
| V-LPW | 17.5 ± 3.3 | 12.2 | 17.5 | −1.2 |
| SPT (SPP-SPA) | 9.7 ± 1.6 | 17.4 | 11.4 | −6.0 |
| H-MP | 9.7 ± 4.5 | 16.8 | 11.0 | −5.8 |
| H-CVP | 39.6 ± 3.5 | 30.6 | 24.1 | −6.5 |
| Ratio (%) | ||||
| FHI (S-Go/N-Me) | 63.0 ± 2.0 | 57.9 | 56.0 | −1.9 |
| Variables | Pre-Treatment | Post-Treatment | Change |
|---|---|---|---|
| Dental arch widths (mm) | |||
| Maxillary | |||
| Intercanine | 31.9 | 33.0 | 1.1 |
| Intermolar | 44.8 | 43.3 | −1.5 |
| Mandibular | |||
| Intercanine | 21.4 | 25.4 | 4.0 |
| Intermolar | 39.2 | 45.6 | 6.4 |
| Basal skeletal widths (mm) | |||
| Maxillary | |||
| Intercanine | 38.7 | 37.0 | −1.7 |
| Intermolar | 55.7 | 53.5 | −2.2 |
| Mandibular | |||
| Intercanine | 27.9 | 30.4 | 2.5 |
| Intermolar | 46.5 | 48.8 | 2.3 |
| Depth of the palatal vault (mm) | |||
| Maxillary | 10.7 | 11.5 | 0.9 |
| Palatal volume (mm3) | |||
| Maxillary | 4020.6 | 3412.3 | −608.3 |
| Palatal surface area (mm2) | |||
| Maxillary | 1034.2 | 1015.6 | −18.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xin, Y.; Zhou, H.; Zhao, Y.; Zhao, L. Invisalign Treatment of a Three-Year-Old Child with Bilateral Posterior Scissor Bite and Multisite Upper Airway Obstruction: A Case Report. J. Clin. Med. 2023, 12, 333. https://doi.org/10.3390/jcm12010333
Xin Y, Zhou H, Zhao Y, Zhao L. Invisalign Treatment of a Three-Year-Old Child with Bilateral Posterior Scissor Bite and Multisite Upper Airway Obstruction: A Case Report. Journal of Clinical Medicine. 2023; 12(1):333. https://doi.org/10.3390/jcm12010333
Chicago/Turabian StyleXin, Yilin, Hongling Zhou, Yifan Zhao, and Lixing Zhao. 2023. "Invisalign Treatment of a Three-Year-Old Child with Bilateral Posterior Scissor Bite and Multisite Upper Airway Obstruction: A Case Report" Journal of Clinical Medicine 12, no. 1: 333. https://doi.org/10.3390/jcm12010333
APA StyleXin, Y., Zhou, H., Zhao, Y., & Zhao, L. (2023). Invisalign Treatment of a Three-Year-Old Child with Bilateral Posterior Scissor Bite and Multisite Upper Airway Obstruction: A Case Report. Journal of Clinical Medicine, 12(1), 333. https://doi.org/10.3390/jcm12010333