
COVID-19-Associated Disease Course Is Shortened in Moderate-to-Severe Atopic Dermatitis Patients Receiving Dupilumab Treatment: A Retrospective Cross-Sectional Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Subjects
2.2. Statistical Analyses
3. Results
3.1. Characteristics of the Study Population
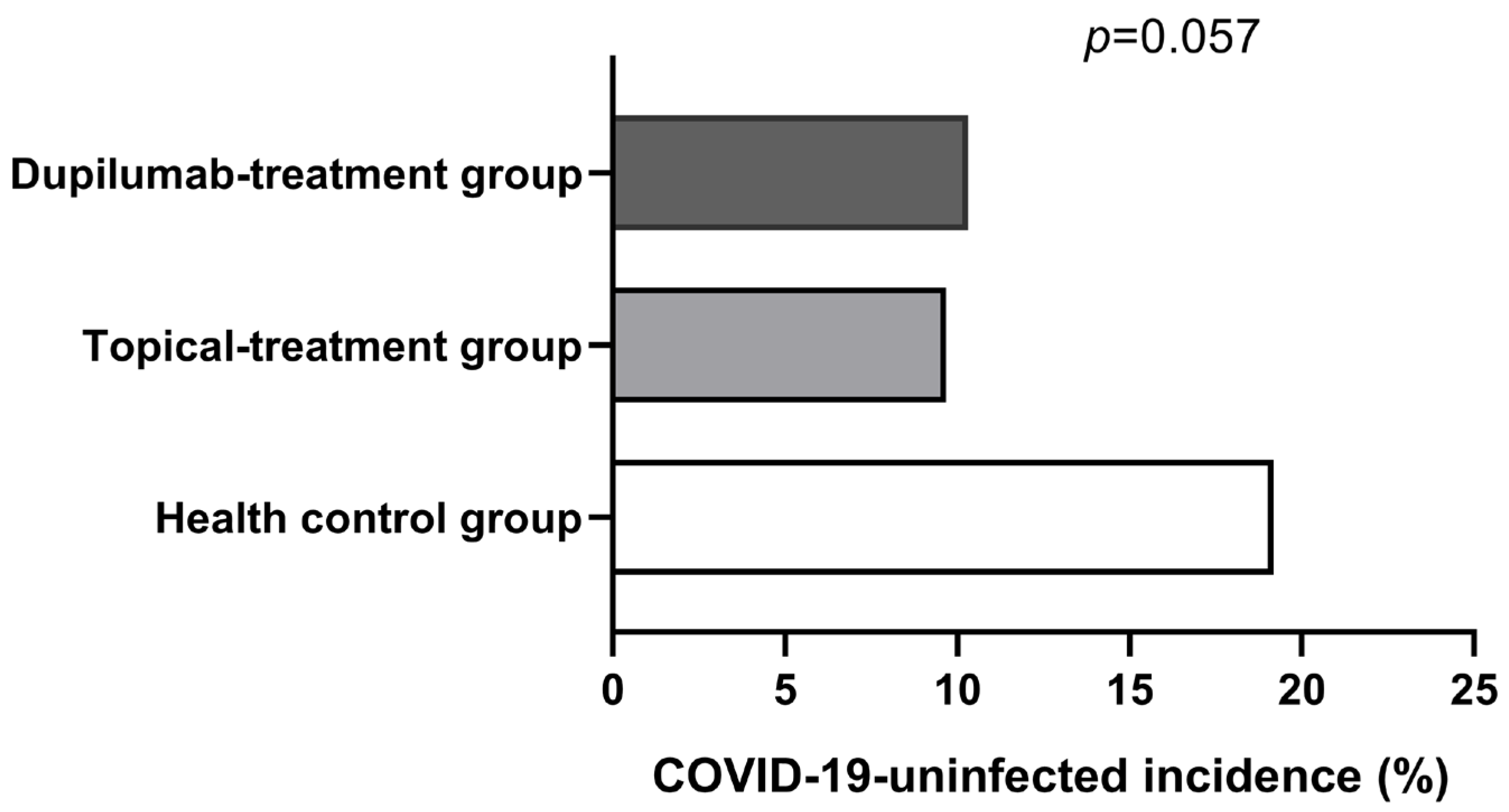
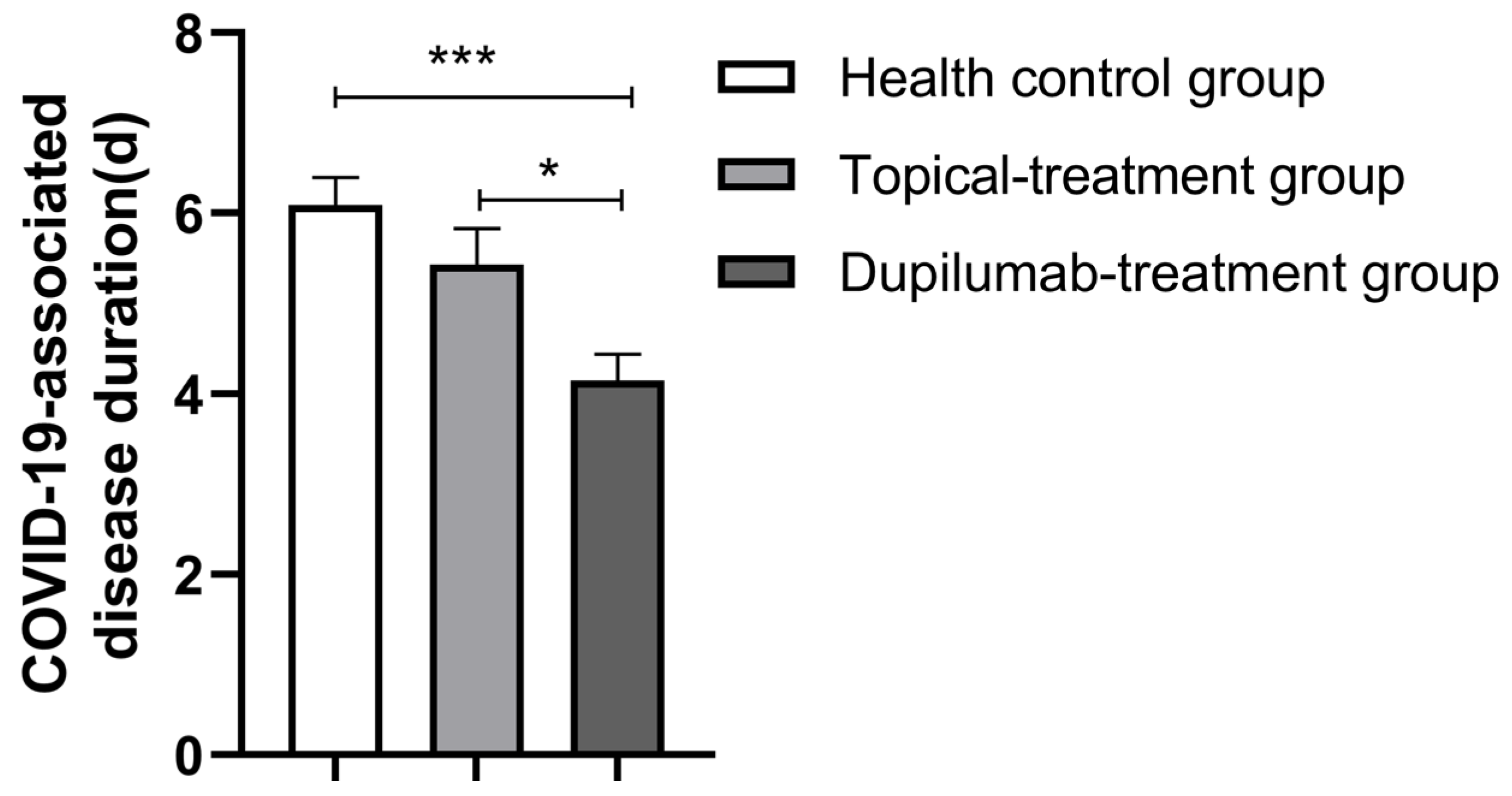
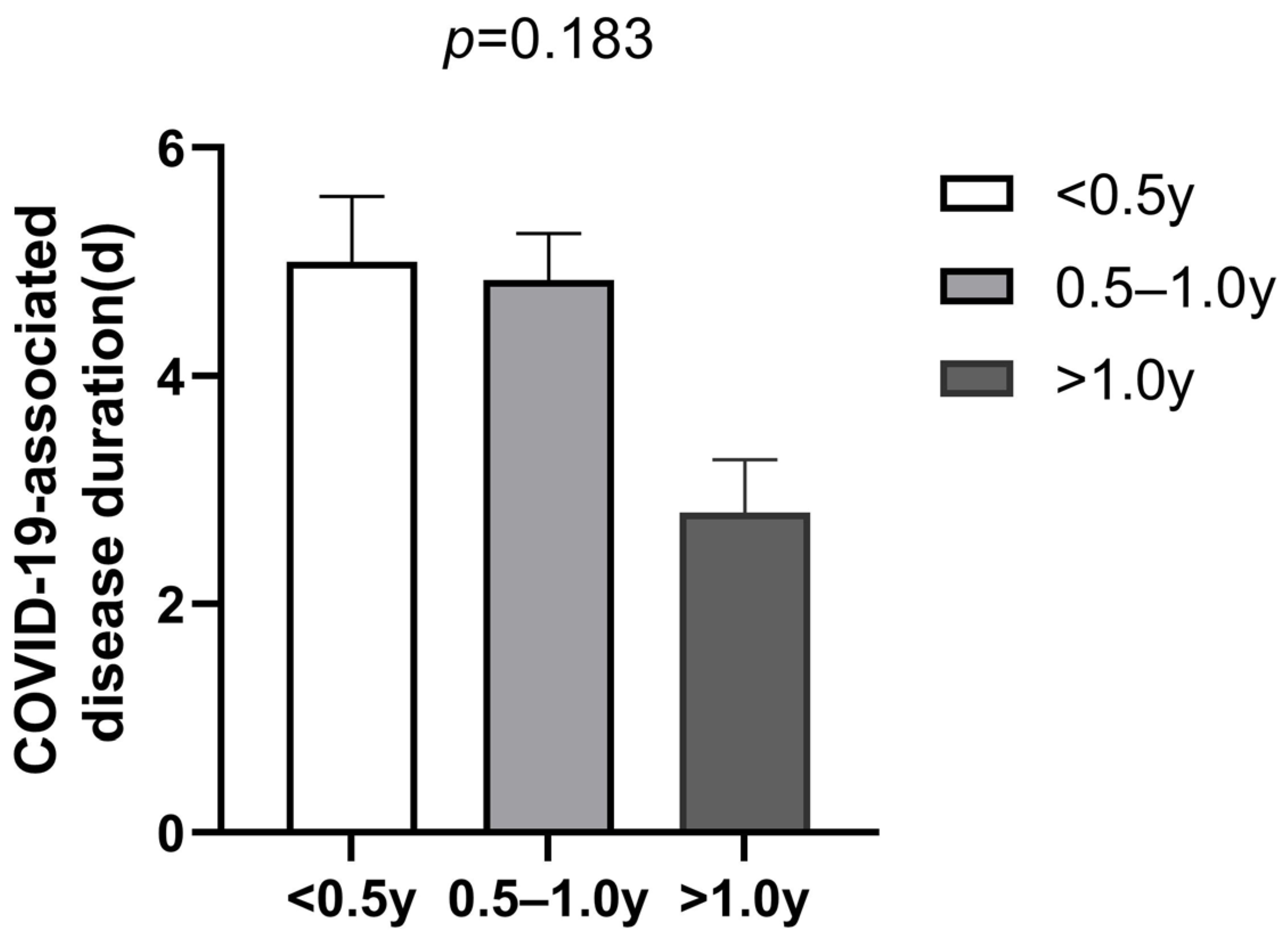
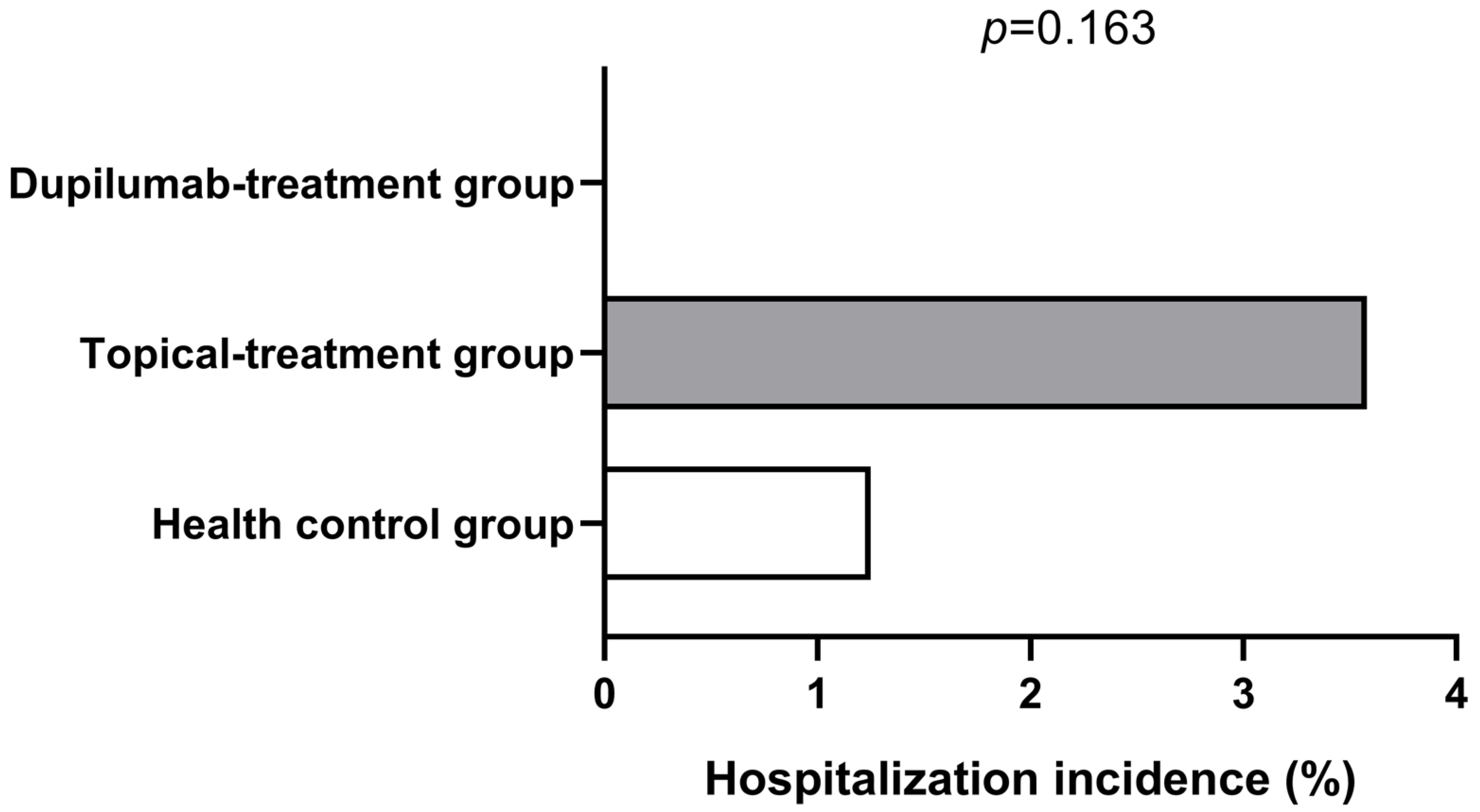
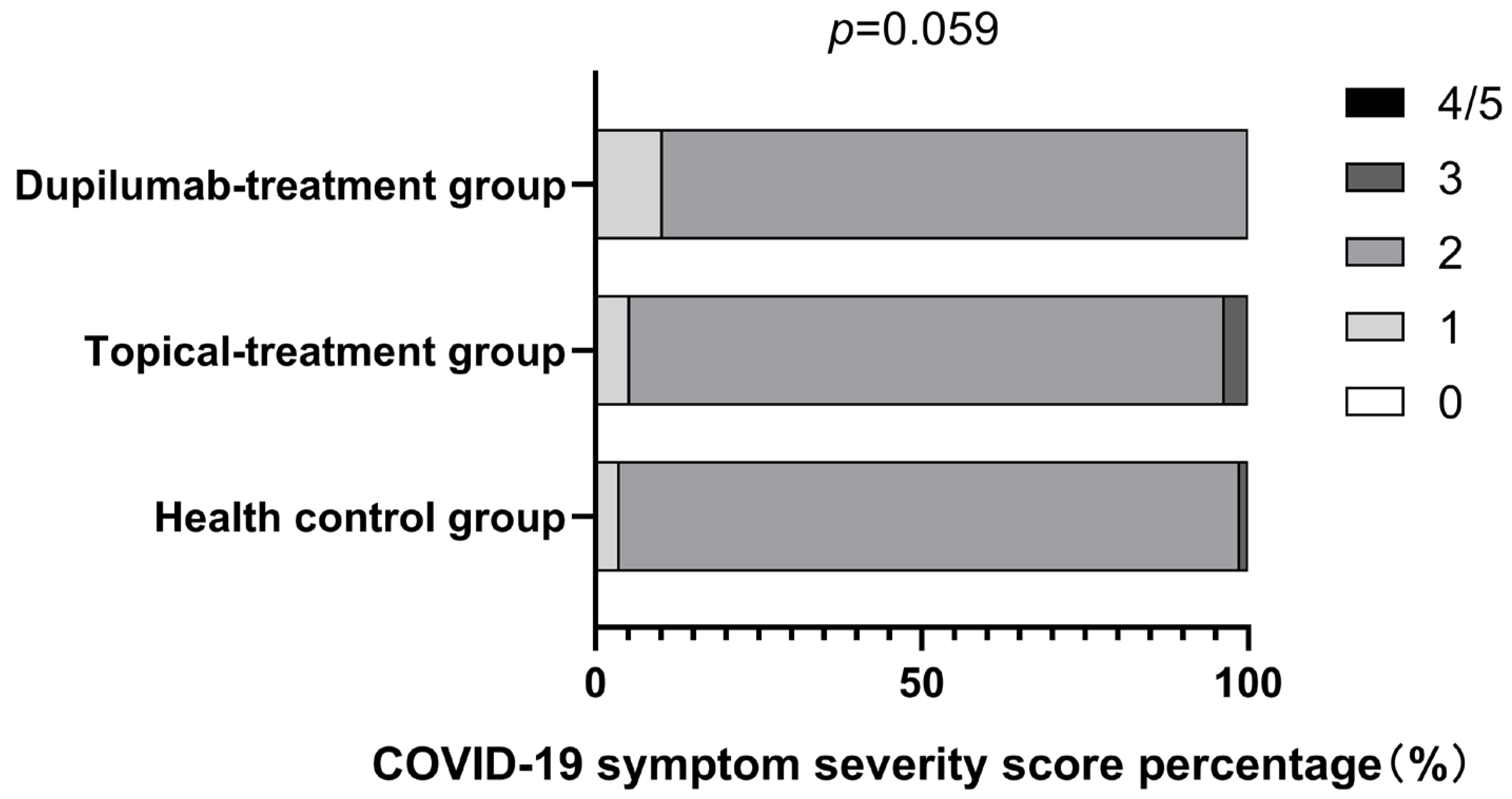
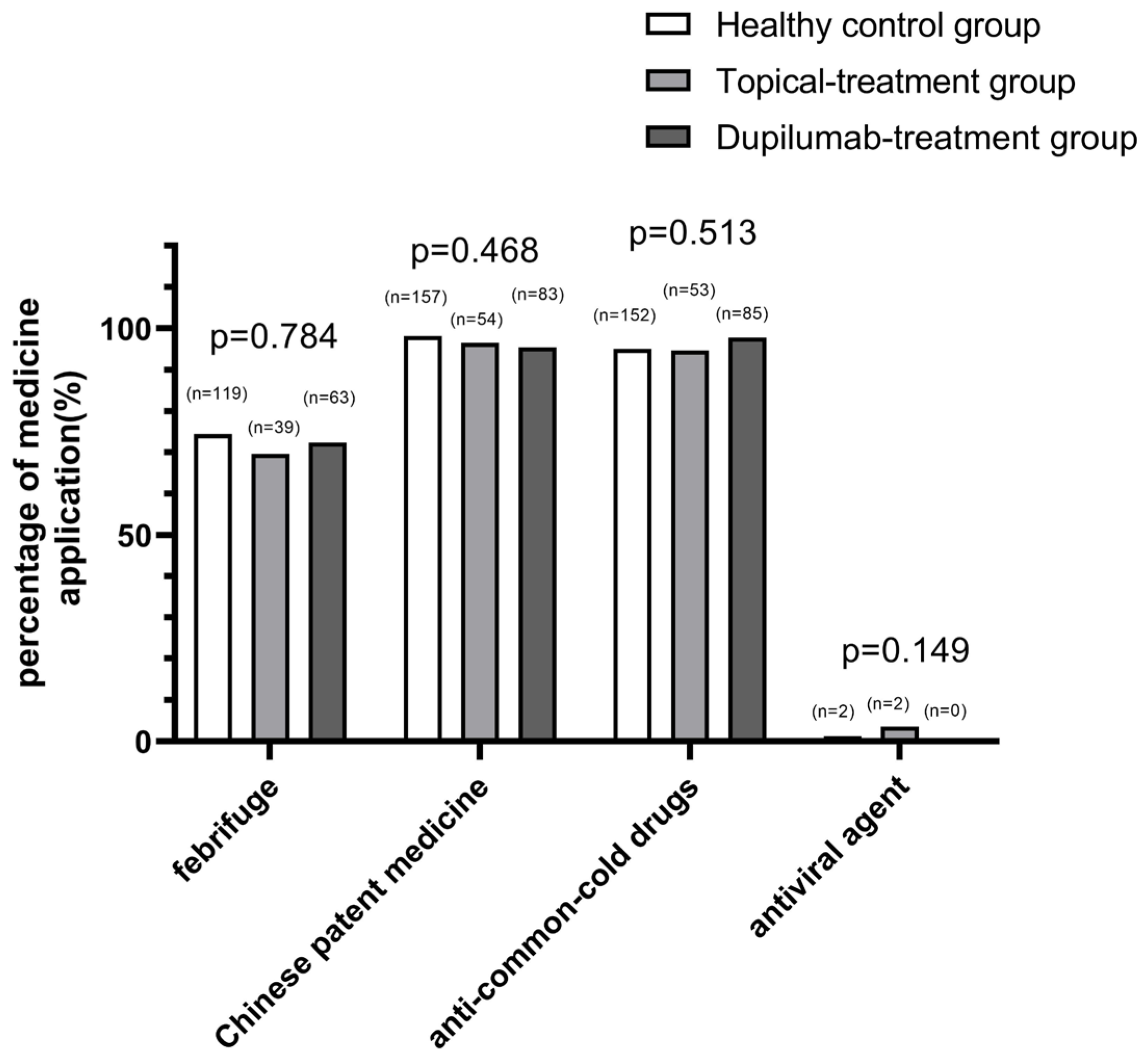
3.2. COVID-19 Severity Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Majumder, J.; Minko, T. Recent Developments on Therapeutic and Diagnostic Approaches for COVID-19. AAPS J. 2021, 23, 14. [Google Scholar] [CrossRef]
- Toor, S.M.; Saleh, R.; Sasidharan, N.V.; Taha, R.Z.; Elkord, E. T-cell responses and therapies against SARS-CoV-2 infection. Immunology 2021, 162, 30–43. [Google Scholar] [CrossRef] [PubMed]
- Azkur, A.K.; Akdis, M.; Azkur, D.; Sokolowska, M.; Van De Veen, W.; Brüggen, M.-C.; O’Mahony, L.; Gao, Y.; Nadeau, K.; Akdis, C.A. Immune response to SARS-CoV-2 and mechanisms of immunopathological changes in COVID-19. Allergy 2020, 75, 1564–1581. [Google Scholar] [CrossRef] [PubMed]
- Hasanvand, A. COVID-19 and the role of cytokines in this disease. Inflammopharmacology 2022, 30, 789–798. [Google Scholar] [CrossRef]
- Vaz, D.P.C.; de Azevedo, M.; Nagashima, S.; Martins, A.P.C.; Malaquias, M.A.C.; Miggiolaro, A.F.R.D.S.; Júnior, J.D.S.M.; Avelino, G.; Carmo, L.A.P.D.; Carstens, L.B.; et al. IL-4/IL-13 remodeling pathway of COVID-19 lung injury. Sci. Rep. 2020, 10, 18689. [Google Scholar]
- Meltendorf, S.; Vogel, K.; Thurm, C.; Prätsch, F.; Reinhold, A.; Färber, J.; Heuft, H.-C.; Kaasch, A.C.; Hachenberg, T.; Weinzierl, S.; et al. IL-13 determines specific IgE responses and SARS-CoV-2 immunity after mild COVID-19 and novel mRNA vaccination. Eur. J. Immunol. 2022, 52, 1972–1979. [Google Scholar] [CrossRef]
- Sidbury, R.; Kodama, S. Atopic dermatitis guidelines: Diagnosis, systemic therapy, and adjunctive care. Clin. Dermatol. 2018, 36, 648–652. [Google Scholar] [CrossRef]
- Cabanillas, B.; Brehler, A.C.; Novak, N. Atopic dermatitis phenotypes and the need for personalized medicine. Curr. Opin. Allergy Clin. Immunol. 2017, 17, 309–315. [Google Scholar] [CrossRef]
- Sroka-Tomaszewska, J.; Trzeciak, M. Molecular Mechanisms of Atopic Dermatitis Pathogenesis. Int. J. Mol. Sci. 2021, 22, 4130. [Google Scholar] [CrossRef]
- Harb, H.; Chatila, T.A. Mechanisms of Dupilumab. Clin. Exp. Allergy 2020, 50, 5–14. [Google Scholar] [CrossRef]
- Seegraber, M.; Srour, J.; Walter, A.; Knop, M.; Wollenberg, A. Dupilumab for treatment of atopic dermatitis. Expert Rev. Clin. Pharm. 2018, 11, 467–474. [Google Scholar] [CrossRef]
- Kridin, K.; Schonmann, Y.; Solomon, A.; Onn, E.; Bitan, D.T.; Weinstein, O.; Cohen, A.D. Risk of COVID-19 and its complications in patients with atopic dermatitis undergoing dupilumab treatment-a population-based cohort study. Immunol. Res. 2022, 70, 106–113. [Google Scholar] [CrossRef]
- Ferrucci, S.; Romagnuolo, M.; Angileri, L.; Berti, E.; Tavecchio, S. Safety of dupilumab in severe atopic dermatitis and infection of COVID-19: Two case reports. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e303–e304. [Google Scholar] [CrossRef]
- Ferrari, M.; Donadu, M.G.; Biondi, G.; Saderi, L.; Sucato, F.; Montesu, M.A.; Ruggiu, P.; Merella, P.; Chessa, C.; Sias, A.; et al. Dupilumab: Direct Cost and Clinical Evaluation in Patients with Atopic Dermatitis. Dermatol. Res. Pract. 2023, 2023, 4592087. [Google Scholar] [CrossRef]
- Hanifin, J.M.; Rajka, G. Diagnostic features of atopic dermatitis. Acta Derm.-Venereol. 1980, 92, 44–47. [Google Scholar] [CrossRef]
- Suárez-Fariñas, M.; Dhingra, N.; Gittler, J.; Shemer, A.; Cardinale, I.; Strong, C.D.G.; Krueger, J.G.; Guttman-Yassky, E. Intrinsic atopic dermatitis shows similar TH2 and higher TH17 immune activation compared with extrinsic atopic dermatitis. J. Allergy Clin. Immunol. 2013, 132, 361–370. [Google Scholar] [CrossRef]
- Donlan, A.N.; Sutherland, T.E.; Marie, C.; Preissner, S.; Bradley, B.T.; Carpenter, R.M.; Sturek, J.M.; Ma, J.Z.; Moreau, G.B.; Donowitz, J.R.; et al. IL-13 is a driver of COVID-19 severity. JCI Insight 2021, 6, e150107. [Google Scholar] [CrossRef]
- Ungar, B.; Glickman, J.W.; Golant, A.K.; Dubin, C.; Marushchak, O.; Gontzes, A.; Mikhaylov, D.; Singer, G.K.; Baum, D.; Wei, N.; et al. COVID-19 Symptoms Are Attenuated in Moderate-to-Severe Atopic Dermatitis Patients Treated with Dupilumab. J. Allergy Clin. Immunol. Pract. 2022, 10, 134–142. [Google Scholar] [CrossRef]
- Anastassopoulou, C.; Gkizarioti, Z.; Patrinos, G.P.; Tsakris, A. Human genetic factors associated with susceptibility to SARS-CoV-2 infection and COVID-19 disease severity. Hum. Genom. 2020, 14, 40. [Google Scholar] [CrossRef]
- Fricke-Galindo, I.; Falfan-Valencia, R. Genetics Insight for COVID-19 Susceptibility and Severity: A Review. Front. Immunol. 2021, 12, 622176. [Google Scholar] [CrossRef]
- Fan, R.; Leasure, A.C.; Damsky, W.; Cohen, J.M. Association between atopic dermatitis and COVID-19 infection: A case-control study in the All of Us research program. JAAD Int. 2022, 6, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Ren, J.; Pang, W.; Luo, Y.; Cheng, D.; Qiu, K.; Rao, Y.; Zheng, Y.; Dong, Y.; Peng, J.; Hu, Y.; et al. Impact of Allergic Rhinitis and Asthma on COVID-19 Infection, Hospitalization, and Mortality. J. Allergy Clin. Immunol. Pract. 2022, 10, 124–133. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.J.; Dong, X.; Liu, G.H.; Gao, Y.D. Risk and Protective Factors for COVID-19 Morbidity, Severity, and Mortality. Clin. Rev. Allergy Immunol. 2023, 64, 90–107. [Google Scholar] [CrossRef] [PubMed]
- Peebles, R.J. IL-13 Protects against SARS-CoV-2? Am. J. Respir Cell Mol. Biol. 2022, 66, 351–352. [Google Scholar] [CrossRef]
- Gao, Y.D.; Ding, M.; Dong, X.; Zhang, J.J.; Azkur, A.K.; Azkur, D.; Gan, H.; Sun, Y.L.; Fu, W.; Li, W.; et al. Risk factors for severe and critically ill COVID-19 patients: A review. Allergy 2021, 76, 428–455. [Google Scholar] [CrossRef]
- David, B.W.; Tarbox, J.A.; Tarbox, M.B. Atopic Dermatitis: Pathophysiology. Adv. Exp. Med. Biol. 2017, 1027, 21–37. [Google Scholar]
- Sasson, J.; Donlan, A.N.; Ma, J.Z.; Haughey, H.; Coleman, R.; Nayak, U.; Mathers, A.J.; Jackson, P.E.H.; Heysell, S.K.; Sturek, J.M.; et al. Safety and Efficacy of Dupilumab for the Treatment of Hospitalized Patients with Moderate to Severe COVID 19: A Phase IIa Trial. medRxiv 2022. [Google Scholar] [CrossRef]
- Wechsler, M.E.; Klion, A.D.; Paggiaro, P.; Nair, P.; Staumont-Salle, D.; Radwan, A.; Johnson, R.R.; Kapoor, U.; Khokhar, F.A.; Daizadeh, N.; et al. Effect of Dupilumab on Blood Eosinophil Counts in Patients with Asthma, Chronic Rhinosinusitis with Nasal Polyps, Atopic Dermatitis, or Eosinophilic Esophagitis. J. Allergy Clin. Immunol. Pract. 2022, 10, 2695–2709. [Google Scholar] [CrossRef]
- Lindsley, A.W.; Schwartz, J.T.; Rothenberg, M.E. Eosinophil responses during COVID-19 infections and coronavirus vaccina tion. J. Allergy Clin. Immunol. 2020, 146, 1–7. [Google Scholar] [CrossRef]
- Lombardi, C.; Bagnasco, D.; Passalacqua, G. COVID-19, Eosinophils, and Biologicals for Severe Asthma. Front. Allergy 2022, 3, 859376. [Google Scholar] [CrossRef]
- Ferastraoaru, D.; Hudes, G.; Jerschow, E.; Jariwala, S.; Karagic, M.; de Vos, G.; Jariwala, S.; Karagic, M.; de Vos, G.; Rosenstreich, D.; et al. Eosinophilia in asthma patients is protective against severe COVID-19 illness. J. Allergy Clin. Immunol. Pract. 2021, 9, 1152–1162. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Status of AD | Topical treatment Group (n = 62) | Dupilumab-Treatment Group (n = 97) | p-Value |
|---|---|---|---|
| Duration of AD, mean (SD), years | 5.85 (4.63) | 5.65 (5.35) | 0.728 |
| TlgE (KU/L) | 1005.05 (1442.82) | 875.77 (1116.76) | 0.942 |
| Phenotypes | 0.550 | ||
| Intrinsic (No) | 22 | 30 | |
| Extrinsic (No) | 40 | 67 |
| Characteristic | Health Control Group (n = 198) | Topical Treatment Group (n = 62) | Dupilumab- Treatment Group (n = 97) | p-Value |
|---|---|---|---|---|
| Age, mean (SD), years | 17.67 (13.11) | 18.92 (14.59) | 18.86 (17.05) | 0.603 |
| ≤17 years old number (percent) | 120 (60.61) | 36 (58.06) | 63 (64.95) | 0.651 |
| ≤17 years old mean (SD), years | 8.24 (4.37) | 7.64 (3.26) | 7.92 (4.08) | 0.721 |
| Gender | 0.825 | |||
| male | 114 (57.58%) | 33 (53.22%) | 54 (55.67%) | |
| female | 84 (56.58%) | 29 (46.78%) | 43 (44.33%) | |
| COVID-19 vaccinated number (percent) | 172 (86.87%) | 49 (79.03%) | 71 (73.20%) | 0.825 |
| COVID-19 vaccine doses for individuals | 2.13 (0.97) # | 1.76 (1.00) ## | 1.65 (1.14) ### | 0.000 |
| With other disorders | ||||
| No | 22 (35.48%) | 31 (31.96%) | 0.646 | |
| Allergic rhinitis | 31 (50%) | 49 (50.52%) | 0.949 | |
| Nasosinusitis | 8 (12.9%) | 9 (9.28 %) | 0.471 | |
| Food allergy | 16 (25.81%) | 34 (35.05%) | 0.221 | |
| Drug allergy | 6 (9.68%) | 3 (3.09%) | 0.161 | |
| Obesity | 1 (1.61%) | 4 (4.12%) | 0.675 | |
| Cardiovascular and cerebrovascular diseases | 1 (1.61%) | 2 (2.06%) | 1.00 | |
| Kidney disease | 3 (4.84%) | 2 (2.06%) | 0.608 | |
| Diabetes mellitus | 0 (0%) | 1 (1.03%) | 1.00 | |
| Tumor | 1 (1.61%) | 1 (1.03%) | 1.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, D.; Wang, Y.; Huang, N.; Li, W.; Chen, H.; Yang, Y.; Zhu, R. COVID-19-Associated Disease Course Is Shortened in Moderate-to-Severe Atopic Dermatitis Patients Receiving Dupilumab Treatment: A Retrospective Cross-Sectional Study. J. Clin. Med. 2023, 12, 3415. https://doi.org/10.3390/jcm12103415
Ma D, Wang Y, Huang N, Li W, Chen H, Yang Y, Zhu R. COVID-19-Associated Disease Course Is Shortened in Moderate-to-Severe Atopic Dermatitis Patients Receiving Dupilumab Treatment: A Retrospective Cross-Sectional Study. Journal of Clinical Medicine. 2023; 12(10):3415. https://doi.org/10.3390/jcm12103415
Chicago/Turabian StyleMa, Dongxia, Yin Wang, Nan Huang, Wenjing Li, Hao Chen, Yaqi Yang, and Rongfei Zhu. 2023. "COVID-19-Associated Disease Course Is Shortened in Moderate-to-Severe Atopic Dermatitis Patients Receiving Dupilumab Treatment: A Retrospective Cross-Sectional Study" Journal of Clinical Medicine 12, no. 10: 3415. https://doi.org/10.3390/jcm12103415
APA StyleMa, D., Wang, Y., Huang, N., Li, W., Chen, H., Yang, Y., & Zhu, R. (2023). COVID-19-Associated Disease Course Is Shortened in Moderate-to-Severe Atopic Dermatitis Patients Receiving Dupilumab Treatment: A Retrospective Cross-Sectional Study. Journal of Clinical Medicine, 12(10), 3415. https://doi.org/10.3390/jcm12103415