
Prone Position Ventilation in Severe ARDS due to COVID-19: Comparison between Prolonged and Intermittent Strategies
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Outcomes
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- ARDS Definition Task Force; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; Tonetti, T.; Protti, A.; Langer, T.; Girardis, M.; Bellani, G.; Laffey, J.; Carrafiello, G.; Carsana, L.; Rizzuto, C.; et al. Pathophysiology of COVID-19-associated acute respiratory distress syndrome: A multicentre prospective observational study. Lancet Respir. Med. 2020, 8, 1201–1208. [Google Scholar] [CrossRef] [PubMed]
- Gattinoni, L.; Chiumello, D.; Rossi, S. COVID-19 pneumonia: ARDS or not? Crit. Care 2020, 24, 154. [Google Scholar] [CrossRef] [PubMed]
- Guérin, C.; Reignier, J.; Richard, J.C.; Beuret, P.; Gacouin, A.; Boulain, T.; Mercier, E.; Badet, M.; Mercat, A.; Baudin, O.; et al. Prone positioning in severe acute respiratory distress syndrome. N. Engl. J. Med. 2013, 368, 2159–2168. [Google Scholar] [CrossRef] [PubMed]
- Gattinoni, L.; Taccone, P.; Carlesso, E.; Marini, J.J. Prone position in acute respiratory distress syndrome. Rationale, indications, and limits. Am. J. Respir. Crit. Care Med. 2013, 188, 1286–1293. [Google Scholar] [CrossRef] [PubMed]
- Guérin, C.; Albert, R.K.; Beitler, J.; Gattinoni, L.; Jaber, S.; Marini, J.J.; Munshi, L.; Papazian, L.; Pesenti, A.; Vieillard-Baron, A.; et al. Prone position in ARDS patients: Why, when, how and for whom. Intensive Care Med. 2020, 46, 2385–2396. [Google Scholar] [CrossRef]
- Griffiths, M.J.D.; McAuley, D.F.; Perkins, G.D.; Barrett, N.; Blackwood, B.; Boyle, A.; Chee, N.; Connolly, B.; Dark, P.; Finney, S.; et al. Guidelines on the management of acute respiratory distress syndrome. BMJ Open Respir. Res. 2019, 6, e000420. [Google Scholar] [CrossRef]
- Langer, T.; Brioni, M.; Guzzardella, A.; Carlesso, E.; Cabrini, L.; Castelli, G.; Dalla Corte, F.; De Robertis, E.; Favarato, M.; Forastieri, A.; et al. Prone position in intubated, mechanically ventilated patients with COVID-19: A multi-centric study of more than 1000 patients. Crit. Care 2021, 25, 128. [Google Scholar] [CrossRef]
- Mathews, K.S.; Soh, H.; Shaefi, S.; Wang, W.; Bose, S.; Coca, S.; Gupta, S.; Hayek, S.S.; Srivastava, A.; Brenner, S.K.; et al. Prone Positioning and Survival in Mechanically Ventilated Patients with Coronavirus Disease 2019-Related Respiratory Failure. Crit. Care Med. 2021, 49, 1026–1037. [Google Scholar] [CrossRef]
- Le, M.Q.; Rosales, R.; Shapiro, L.T.; Huang, L.Y. The DownSide of Prone Positioning: The Case of a Coronavirus 2019 Survivor. Am. J. Phys. Med. Rehabil. 2020, 99, 870–872. [Google Scholar] [CrossRef]
- Douglas, I.S.; Rosenthal, C.A.; Swanson, D.D.; Hiller, T.; Oakes, J.; Bach, J.; Whelchel, C.; Pickering, J.; George, T.; Kearns, M.; et al. Safety and Outcomes of Prolonged Usual Care Prone Position Mechanical Ventilation to Treat Acute Coronavirus Disease 2019 Hypoxemic Respiratory Failure. Crit. Care Med. 2021, 49, 490–502. [Google Scholar] [CrossRef] [PubMed]
- Carsetti, A.; Damia Paciarini, A.; Marini, B.; Pantanetti, S.; Adrario, E.; Donati, A. Prolonged prone position ventilation for SARS-CoV-2 patients is feasible and effective. Crit. Care 2020, 24, 225. [Google Scholar] [CrossRef] [PubMed]
- Jochmans, S.; Mazerand, S.; Chelly, J.; Pourcine, F.; Sy, O.; Thieulot-Rolin, N.; Ellrodt, O.; Mercier Des Rochettes, E.; Michaud, G.; Serbource-Goguel, J.; et al. Duration of prone position sessions: A prospective cohort study. Ann. Intensive Care 2020, 10, 66. [Google Scholar] [CrossRef]
- Bellani, G.; Laffey, J.G.; Pham, T.; Fan, E.; Brochard, L.; Esteban, A.; Gattinoni, L.; van Haren, F.; Larsson, A.; McAuley, D.F.; et al. Epidemiology, Patterns of Care, and Mortality for Patients with Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA 2016, 315, 788–800. [Google Scholar] [CrossRef] [PubMed]
- Ferrando, C.; Suarez-Sipmann, F.; Mellado-Artigas, R.; Hernández, M.; Gea, A.; Arruti, E.; Aldecoa, C.; Martínez-Pallí, G.; Martínez-González, M.A.; Slutsky, A.S.; et al. Clinical features, ventilatory management, and outcome of ARDS caused by COVID-19 are similar to other causes of ARDS. Intensive Care Med. 2020, 46, 2200–2211. [Google Scholar] [CrossRef]
- COVID-ICU Group on behalf of the REVA Network and the COVID-ICU Investigators. Clinical characteristics and day-90 outcomes of 4244 critically ill adults with COVID-19: A prospective cohort study. Intensive Care Med. 2021, 47, 60–73. [Google Scholar] [CrossRef]
- Harcombe, C.J. Nursing patients with ARDS in the prone position. Nurs. Stand. 2004, 18, 33–39. [Google Scholar] [CrossRef]
- Scaramuzzo, G.; Gamberini, L.; Tonetti, T.; Zani, G.; Ottaviani, I.; Mazzoli, C.A.; Capozzi, C.; Giampalma, E.; Bacchi Reggiani, M.L.; Bertellini, E.; et al. Sustained oxygenation improvement after first prone positioning is associated with liberation from mechanical ventilation and mortality in critically ill COVID-19 patients: A cohort study. Ann. Intensive Care 2021, 11, 63. [Google Scholar] [CrossRef]
- Okin, D.; Huang, C.Y.; Alba, G.A.; Jesudasen, S.J.; Dandawate, N.A.; Gavralidis, A.; Chang, L.L.; Moin, E.E.; Ahmad, I.; Witkin, A.S.; et al. Prolonged prone position ventilation is associated with reduced mortality in intubated COVID-19 patients. Chest 2022, 163, 533–542. [Google Scholar] [CrossRef]
- Singh, R.; Rathore, S.S.; Khan, H.; Karale, S.; Chawla, Y.; Iqbal, K.; Bhurwal, A.; Tekin, A.; Jain, N.; Mehra, I.; et al. Association of Obesity with COVID-19 Severity and Mortality: An Updated Systemic Review, Meta-Analysis, and Meta-Regression. Front. Endocrinol. 2022, 13, 780872. [Google Scholar] [CrossRef]
- De Jong, A.; Molinari, N.; Sebbane, M.; Prades, A.; Futier, E.; Jung, B.; Chanques, G.; Jaber, S. Feasibility and effectiveness of prone position in morbidly obese patients with ARDS: A case-control clinical study. Chest 2013, 143, 1554–1561. [Google Scholar] [CrossRef] [PubMed]
- Walter, T.; Zucman, N.; Mullaert, J.; Thiry, I.; Gernez, C.; Roux, D.; Ricard, J.D. Extended prone positioning duration for COVID-19-related ARDS: Benefits and detriments. Crit. Care 2022, 26, 208. [Google Scholar] [CrossRef] [PubMed]
- Brugliera, L.; Filippi, M.; Del Carro, U.; Butera, C.; Bianchi, F.; Castellazzi, P.; Cimino, P.; Capodaglio, P.; Monti, G.; Mortini, P.; et al. Nerve Compression Injuries After Prolonged Prone Position Ventilation in Patients with SARS-CoV-2: A Case Series. Arch. Phys. Med. Rehabil. 2021, 102, 359–362. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Group | |||
|---|---|---|---|
| SPP n = 26 | PPP n = 37 | p | |
| Gender, n (%) | |||
| Males | 15 (57.7) | 25 (67.6) | 0.42 |
| Females | 11 (42.3) | 12 (32.4) | |
| Age, mean (SD) | 66.5 (9.7) | 61.5 (15.1) | 0.14 |
| BMI, mean (SD) | 30.5 (5.5) | 33.4 (7.0) | 0.08 |
| BMI | |||
| Normal (18.5–24.9 kg/m2) | 1 (3.8) | 0 (0) | 0.049 |
| Overweight (25–29.9 kg/m2) | 15 (57.7) | 12 (33.3) | |
| Obese (>30 kg/m2) | 10 (38.5) | 24 (66.7) | |
| APACHE II, mean (SD) | 19.3 (3.8) | 19.5 (7.1) | 0.89 |
| Tocilizumab, n (%) | 17 (65%) | 21 (57%) | 0.49 |
| Vt (ml), median (IQR) | 425 (375–450) | 425 (375–475) | 0.59 |
| Vt (ml/PBW), median (IQR) | 6.3 (6.2–6.7) | 6.3 (6.2–6.7) | 0.78 |
| RR, median (IQR) | 27.5 (25–32) | 30 (27–32) | 0.24 |
| Time to proning, h, median (IQR) | 22.5 (16–48) | 20 (10–48) | 0.59 |
| Duration of 1st PP cycle, h, median (IQR) | 20 (20–22) | 46 (40–48) | <0.001 |
| Cumulative duration of proning, h, mean (SD) | 42.42 (22.27) | 70.22 (38.29) | 0.001 |
| Group | P/F Ratio (mmHg) | p 2 | ||||||
|---|---|---|---|---|---|---|---|---|
| Baseline | During | |||||||
| Mean (SD) | Mean (SD) | Mean (SD) | During vs. Baseline | After vs. During | After vs. Baseline | p 3 | ||
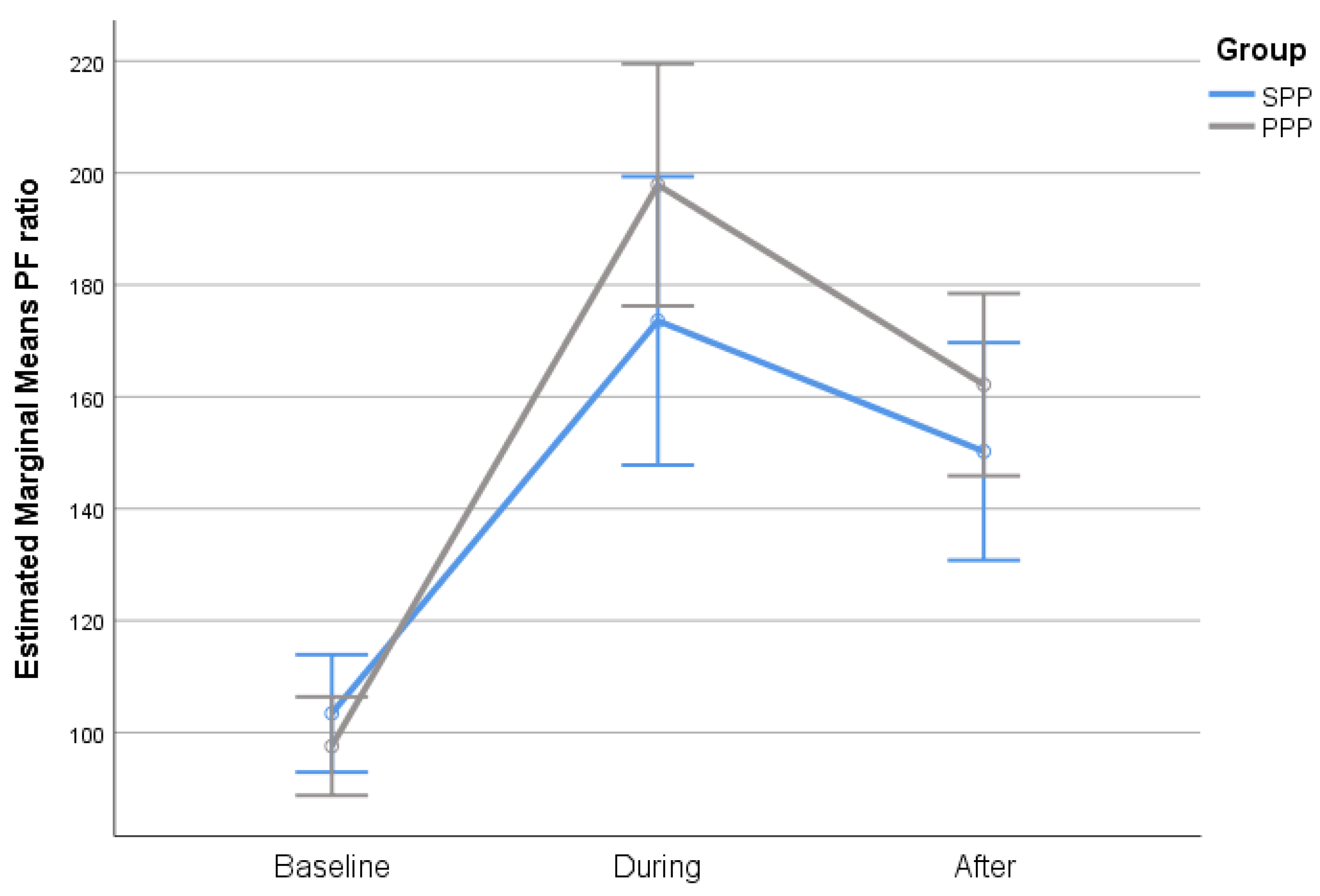
| Total sample | SPP | 103.4 (25.8) | 173.6 (59) | 150.2 (32) | <0.001 | 0.09 | <0.001 | 0.13 |
| PPP | 97.6 (27.4) | 197.9 (70.1) | 162.2 (58.8) | <0.001 | <0.001 | <0.001 | ||
| p 1 | 0.39 | 0.15 | 0.35 | |||||
| Obese | SPP | 105.1 (29.2) | 176.5 (67.9) | 152.8 (25.2) | 0.002 | 0.69 | 0.004 | 0.43 |
| PPP | 95.8 (27.1) | 194.6 (67.8) | 156.7 (48.7) | <0.001 | 0.014 | <0.001 | ||
| p 1 | 0.38 | 0.48 | 0.81 | |||||
| Baseline | During | After | p 2 | |||||
|---|---|---|---|---|---|---|---|---|
| Group | Mean (SD) | Mean (SD) | Mean (SD) | During vs. Baseline | After vs. During | After vs. Baseline | p 3 | |
| PaCO2 (mmHg) | SPP | 50.9 (8.8) | 47.8 (7.5) | 48.3 (6.3) | 0.22 | >0.99 | 0.46 | 0.95 |
| PPP | 50.8 (10.6) | 47.6 (7.1) | 48.5 (7.9) | 0.08 | >0.99 | 0.39 | ||
| p 1 | 0.97 | 0.89 | 0.92 | |||||
| PEEP (cm H2O) | SPP | 12 (2.7) | 11.1 (2.8) | 11.2 (2.6) | 0.012 | >0.99 | 0.02 | 0.49 |
| PPP | 12.3 (2.4) | 11.6 (2.6) | 11.2 (2.2) | 0.018 | 0.29 | <0.001 | ||
| p1 | 0.64 | 0.49 | 0.99 | |||||
| Pplat (cm H2O) | SPP | 25.3 (3.6) | 23.6 (3.2) | 23.9 (3.3) | 0.009 | >0.99 | 0.09 | 0.65 |
| PPP | 25.5 (3.4) | 23.9 (3.5) | 23.5 (3.3) | 0.003 | >0.99 | 0.002 | ||
| p1 | 0.84 | 0.77 | 0.68 | |||||
| DP (cm H2O) | SPP | 13.4 (3.9) | 12.2 (2.4) | 12.2 (2.8) | 0.16 | >0.99 | 0.27 | 0.82 |
| PPP | 12.9 (3.2) | 12.1 (2.4) | 12.2 (2.6) | 0.25 | >0.99 | 0.50 | ||
| p 1 | 0.62 | 0.82 | 0.92 | |||||
| Cstat (mL/cm H2O) | SPP | 35.8 (10.2) | 36.9 (11.6) | 36.8 (10.7) | >0.99 | >0.99 | >0.99 | 0.75 |
| PPP | 35.2 (9.5) | 37.6 (9.3) | 36.4 (8.8) | 0.22 | 0.84 | >0.99 | ||
| p 1 | 0.81 | 0.77 | 0.87 | |||||
| Group | |||
|---|---|---|---|
| SPP n = 26 | PPP n = 37 | p | |
| 28-day survival, n (%) | 0.25 | ||
| No | 9 (34.6) | 8 (21.6) | |
| Yes | 17 (65.4) | 29 (78.4) | |
| Number of cycles, median (IQR) | 2 (1–3) | 1 (1–2) | 0.12 |
| Complications, n (%) | >0.99 | ||
| No | 21 (80.8) | 29 (78.4) | |
| Yes | 5 (19.2) | 8 (21.6) | |
| Group | ||||
|---|---|---|---|---|
| SPP (n = 10) | PPP (n = 24) | |||
| Median | Median | p | ||
| 28-day survival | No | 4 (40) | 5 (20.8) | 0.39 |
| Yes | 6 (60) | 19 (79.2) | ||
| Number of cycles, median (IQR) | 2 (2–3) | 1 (1–2) | 0.19 | |
| OR (95% CI) | p | |
|---|---|---|
| Number of cycles | 0.27 (0.12–0.63) | 0.002 |
| APACHE II | 0.78 (0.66–0.92) | 0.003 |
| PaCO2 baseline (mmHg) | 0.92 (0.86–0.99) | 0.031 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karlis, G.; Markantonaki, D.; Kakavas, S.; Bakali, D.; Katsagani, G.; Katsarou, T.; Kyritsis, C.; Karaouli, V.; Athanasiou, P.; Daganou, M. Prone Position Ventilation in Severe ARDS due to COVID-19: Comparison between Prolonged and Intermittent Strategies. J. Clin. Med. 2023, 12, 3526. https://doi.org/10.3390/jcm12103526
Karlis G, Markantonaki D, Kakavas S, Bakali D, Katsagani G, Katsarou T, Kyritsis C, Karaouli V, Athanasiou P, Daganou M. Prone Position Ventilation in Severe ARDS due to COVID-19: Comparison between Prolonged and Intermittent Strategies. Journal of Clinical Medicine. 2023; 12(10):3526. https://doi.org/10.3390/jcm12103526
Chicago/Turabian StyleKarlis, George, Despina Markantonaki, Sotirios Kakavas, Dimitra Bakali, Georgia Katsagani, Theodora Katsarou, Christos Kyritsis, Vasiliki Karaouli, Paraskevi Athanasiou, and Mary Daganou. 2023. "Prone Position Ventilation in Severe ARDS due to COVID-19: Comparison between Prolonged and Intermittent Strategies" Journal of Clinical Medicine 12, no. 10: 3526. https://doi.org/10.3390/jcm12103526
APA StyleKarlis, G., Markantonaki, D., Kakavas, S., Bakali, D., Katsagani, G., Katsarou, T., Kyritsis, C., Karaouli, V., Athanasiou, P., & Daganou, M. (2023). Prone Position Ventilation in Severe ARDS due to COVID-19: Comparison between Prolonged and Intermittent Strategies. Journal of Clinical Medicine, 12(10), 3526. https://doi.org/10.3390/jcm12103526