
A Biopsychosocial Evaluation of Post-Acute Outcome of Patients with Severe Brain Lesions Recovering from Coma: An Exploratory Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Outcome Assessment
2.2.1. Variables Collected
2.2.2. Objective Outcome and Evolution
2.2.3. Statistical Analysis
2.2.4. The Patient’s Point of View
3. Results
3.1. Patient Characteristics
3.2. Scale Results
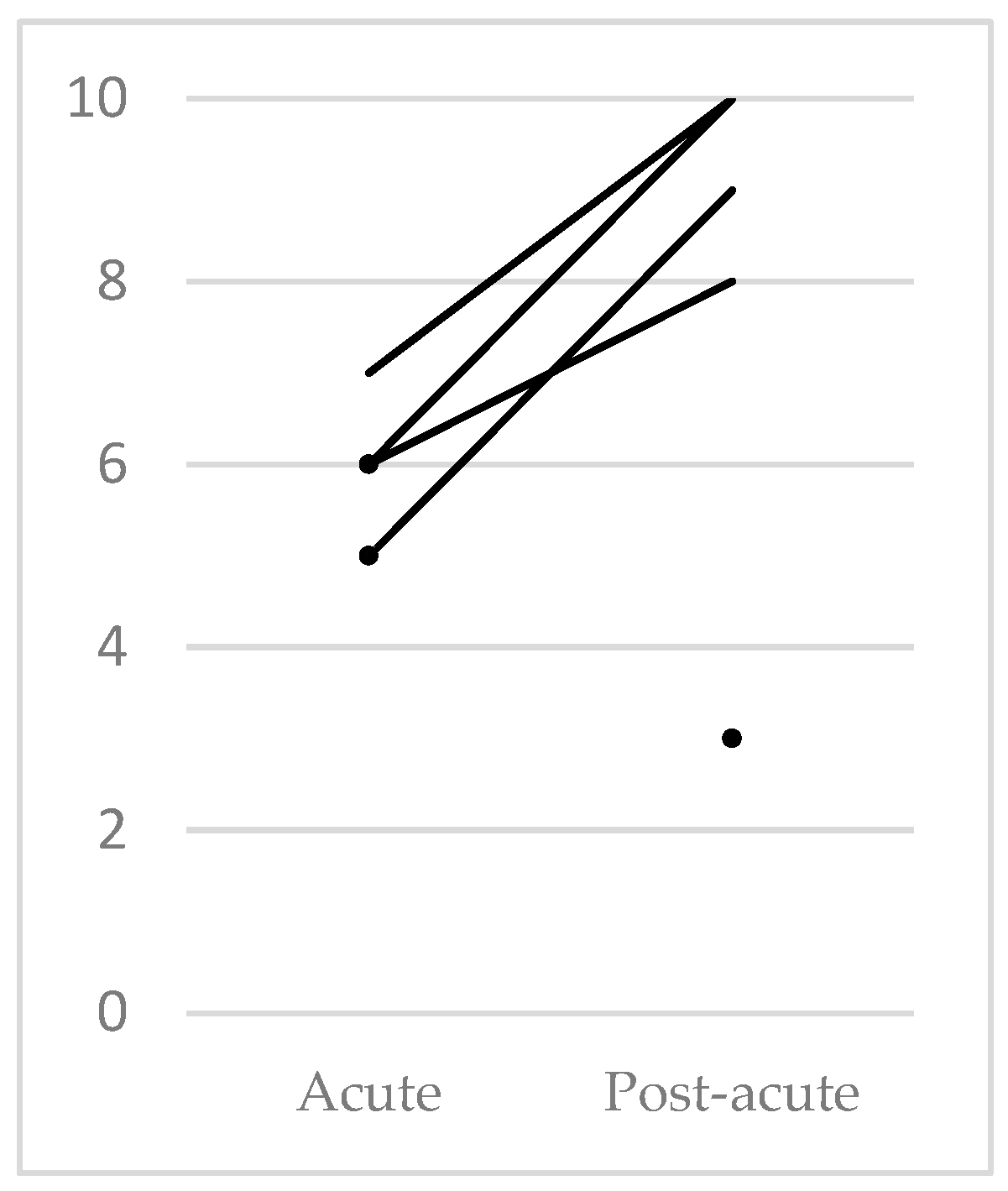
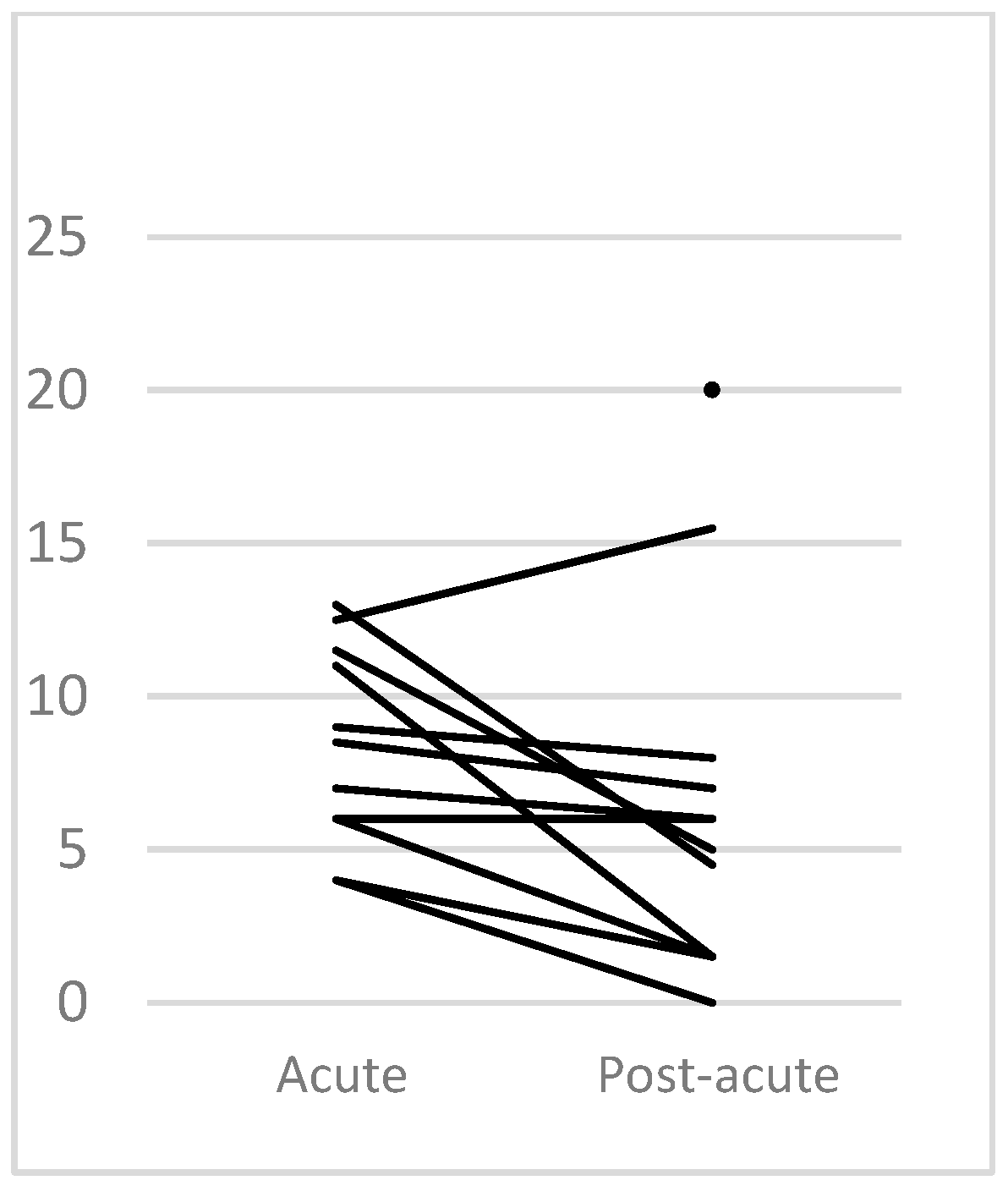
3.2.1. Mental Functions
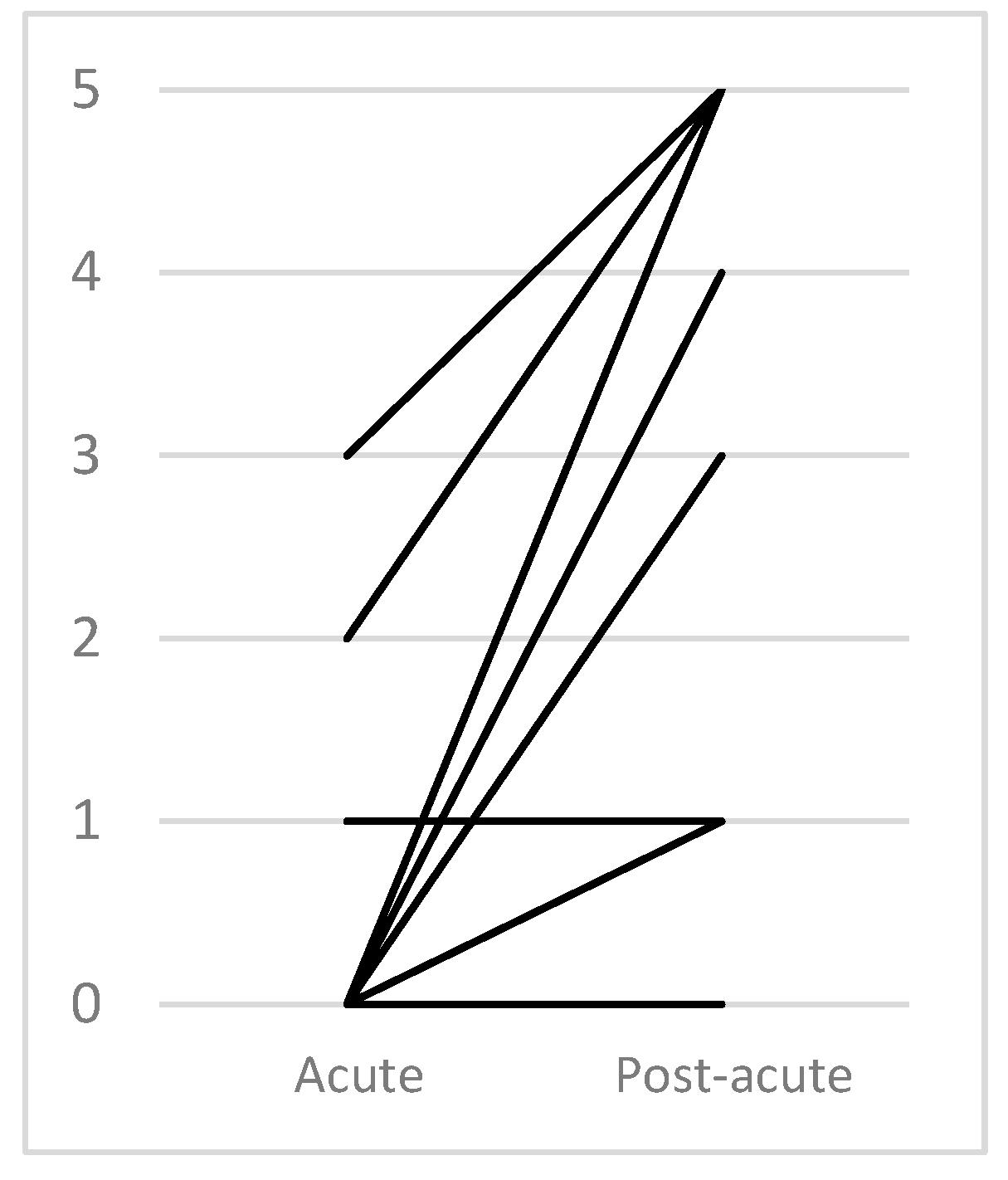
3.2.2. Walking
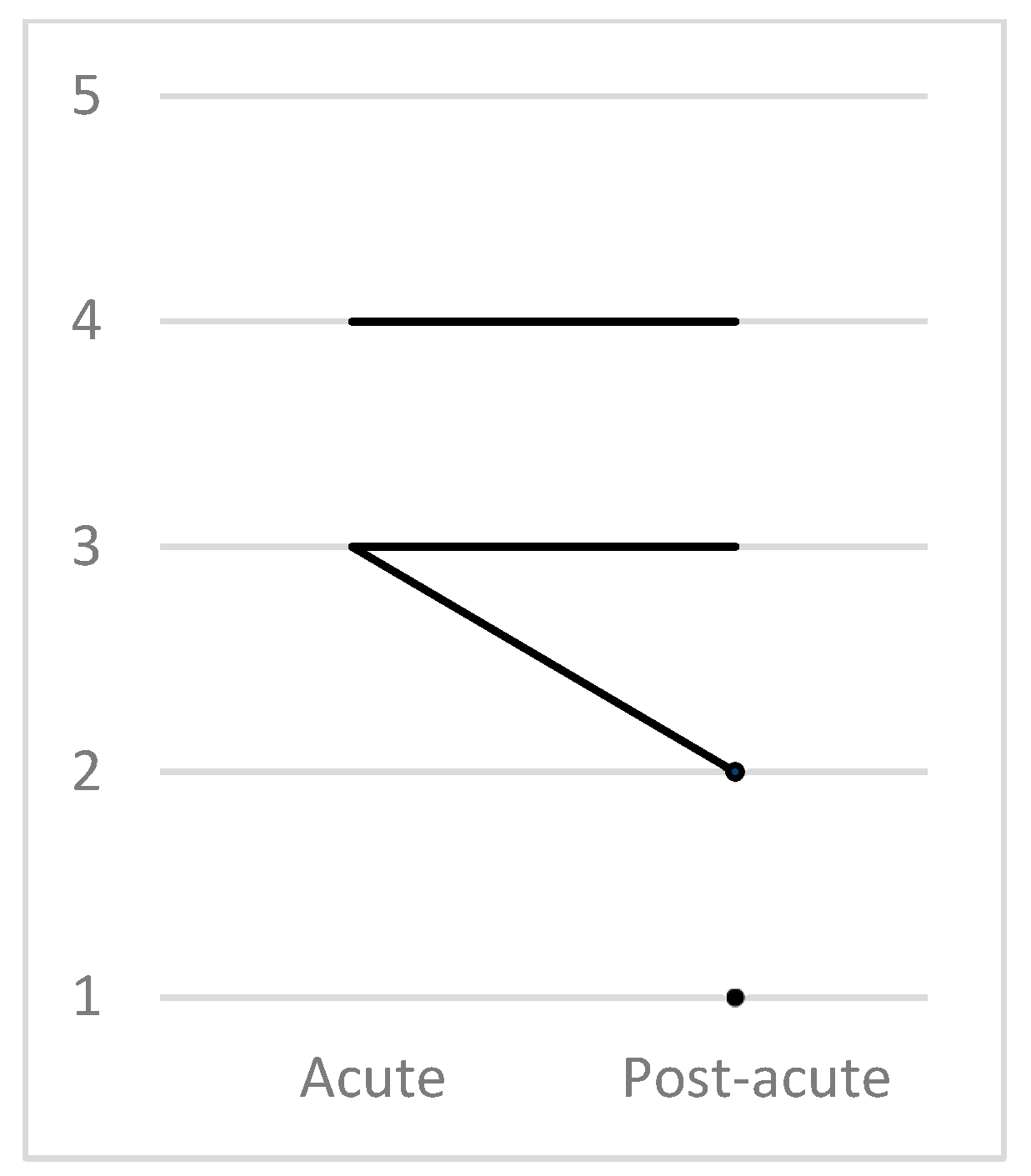
3.2.3. Impact of Injury on Daily life
3.3. Patient Complaints
3.4. Facilitators
4. Discussion
4.1. Patient Characteristics
4.2. Mental Functions
4.2.1. Neurobehavioral Assessment Scale Results
4.2.2. The Patient’s Point of View
4.3. Ambulation
4.3.1. Ambulatory Scale Results
4.3.2. The Patient’s Point of View
4.4. The Impact of Injury on Daily Life
4.4.1. GOS Scale Results
4.4.2. The Patient’s Point of View
4.5. DOC and CMD
4.6. Primary Complaints
Individuality
4.7. Facilitators
4.8. Differences between Clinical Scale Results and a Patient’s Point of View
4.9. Authors’ Suggestions
4.10. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Methodology of QOLIBRI Results

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| A: Satisfaction in thinking abilities | |||||||||
| Patient | A.1 (b140) | A.2 (d310/d330/d350) | A.3 (b144) | A.4 (d175) | A.5 (b164) | A.6 (b1565) | A.7 (b160) | mean | mean [%] |
| 01 | 3 | 5 | 4 | 4 | 4 | 5 | 5 | 4.29 | 82.14 |
| 02 | 4 | 4 | 5 | 4 | 4 | 5 | 4 | 4.29 | 82.14 |
| 03 | 4 | 4 | 3 | - | 5 | 3 | 3 | 3.67 | 66.67 |
| 04 | 5 | 5 | 3 | 5 | 5 | 5 | 4 | 4.57 | 89.29 |
| 05 | 3 | 2 | 2 | 3 | 3 | 3 | 2 | 2.57 | 39.29 |
| 06 | 5 | 5 | 4 | 4 | 5 | 5 | 5 | 4.71 | 92.86 |
| 07 | 3 | 5 | 1 | - | 2 | 4 | 4 | 3.17 | 54.17 |
| 08 | 3 | 3 | 5 | - | 3 | 5 | 5 | 4 | 75 |
| 09 | 2 | 5 | 2 | 5 | 4 | 3 | 3 | 3.43 | 60.71 |
| B: Satisfaction in emotions | |||||||||
| Patient | B.1 (b130) | B.2 (b1301) | B.3 (b180) | B.4 (b1801) | B.5 (nd) | B.6 (b180) | B.7 (nd) | mean | mean [%] |
| 01 | 4 | 4 | 3 | 4 | 4 | 3 | 4 | 3.71 | 67.86 |
| 02 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4.00 | 75.00 |
| 03 | 4 | 4 | 5 | 5 | 5 | 5 | 4 | 4.57 | 89.29 |
| 04 | 2 | 3 | 4 | 4 | 4 | 4 | 3 | 3.43 | 60.71 |
| 05 | 2 | 3 | 3 | 3 | 3 | 3 | 3 | 2.86 | 46.43 |
| 06 | 5 | 5 | 5 | 5 | 5 | 5 | 3 | 4.71 | 92.86 |
| 07 | 5 | 5 | 2 | 5 | 5 | 4 | 1 | 3.86 | 71.43 |
| 08 | 3 | 3 | 3 | 3 | 5 | 3 | 3 | 3.29 | 57.14 |
| 09 | 5 | 4 | 4 | 4 | 5 | 4 | 1 | 3.86 | 71.43 |
| C: Satisfaction in daily life | |||||||||
| Patient | C.1 (d5) | C.2 (d460) | C.3 (d640) | C.4 (d860) | C.5 (d850/d820) | C.6 (d910/d920) | C.7 (nd) | mean | mean [%] |
| 01 | 3 | 3 | 4 | - | 2 | 4 | 4 | 3.33 | 58.33 |
| 02 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5.00 | 100.00 |
| 03 | 4 | 5 | 5 | 4 | - | 5 | 4 | 4.50 | 87.50 |
| 04 | 3 | 3 | 2 | - | 3 | 3 | 4 | 3.00 | 50.00 |
| 05 | 2 | 3 | 4 | 3 | 3 | 2 | 3 | 2.86 | 46.43 |
| 06 | 2 | 3 | 3 | 3 | 4 | 5 | 4 | 3.43 | 60.71 |
| 07 | 4 | 4 | 3 | - | - | 3 | 3 | 3.40 | 60.00 |
| 08 | 1 | 4 | 3 | - | 3 | 4 | 3 | 3.00 | 50.00 |
| 09 | 3 | 1 | 1 | - | 1 | 4 | 3 | 2.17 | 29.17 |
| D: Satisfaction in relations | |||||||||
| Patient | D.1 (b152) | D.2 (d760) | D.3 (d750) | D.4 (d7701) | D.5 (d7702) | D.6 (e4) | mean | mean [%] | |
| 01 | 5 | 5 | 4 | 5 | 5 | 5 | 4.83 | 95.83 | |
| 02 | 5 | 5 | 5 | 5 | 5 | 4 | 4.83 | 95.83 | |
| 03 | 5 | 5 | 5 | 5 | 5 | 5 | 5.00 | 100.00 | |
| 04 | 5 | 5 | 5 | 5 | - | 5 | 5.00 | 100.00 | |
| 05 | 4 | 4 | 3 | 4 | 4 | 4 | 3.83 | 70.83 | |
| 06 | 5 | 5 | 5 | 3 | 1 | 5 | 4.00 | 75.00 | |
| 07 | 4 | 5 | 4 | 5 | 3 | 4 | 4.17 | 79.17 | |
| 08 | 3 | 5 | 2 | 5 | 1 | 5 | 3.50 | 62.50 | |
| 09 | 4 | 4 | 2 | 1 | 1 | 4 | 2.67 | 41.67 | |
| E: Bothered by feelings | |||||||||
| Patient | E.1 (b152) | E.2 (b152) | E.3 (b152) | E.4 (b152) | E.5 (b152) | mean | mean [%] | ||
| 01 | 5 | 3 | 5 | 4 | 3 | 4 | 75 | ||
| 02 | 5 | 4 | 5 | 5 | 5 | 4.8 | 95 | ||
| 03 | 5 | 5 | 5 | 5 | 5 | 5 | 100 | ||
| 04 | 5 | 5 | 5 | 5 | 5 | 5 | 100 | ||
| 05 | 3 | 5 | 5 | 4 | 2 | 3.8 | 70 | ||
| 06 | 5 | 5 | 5 | 5 | 5 | 5 | 100 | ||
| 07 | 4 | 4 | 4 | 5 | 2 | 3.8 | 70 | ||
| 08 | 5 | 5 | 3 | 1 | 5 | 3.8 | 70 | ||
| 09 | 4 | 3 | 3 | 3 | 4 | 3.4 | 60 | ||
| F: Bothered by physical problems | |||||||||
| Patient | F.1 (b1470/b760) | F.2 (nd) | F.3 (b280) | F.4 (b210/b230) | F.5 (nd) | mean | mean [%] | ||
| 01 | 1 | 5 | 5 | 5 | 3 | 3.80 | 70.00 | ||
| 02 | 5 | 3 | 5 | 5 | 4 | 4.40 | 85.00 | ||
| 03 | 2 | 5 | 5 | 4 | 5 | 4.20 | 80.00 | ||
| 04 | 1 | 1 | 5 | 1 | 2.00 | 25.00 | |||
| 05 | 3 | 1 | 4 | 2 | 4 | 2.80 | 45.00 | ||
| 06 | 5 | 3 | 5 | 3 | 3 | 3.80 | 70.00 | ||
| 07 | 3 | - | 3 | 5 | 2 | 3.25 | 56.25 | ||
| 08 | 5 | 5 | 5 | 3 | 3 | 4.20 | 80.00 | ||
| 09 | 5 | 5 | 1 | 5 | 2 | 3.60 | 65.00 | ||
| Patient | Age | Gender |
|---|---|---|
| Patient 1 | 50 | F |
| Patient 2 | 33 | M |
| Patient 3 | 23 | M |
| Patient 4 | 68 | M |
| Patient 5 | 26 | M |
| Patient 6 | 53 | F |
| Patient 7 | 54 | M |
| Patient 8 | 41 | M |
| Patient 9 | 29 | F |
| Patient 10 | 79 | F |
| Patient 11 | 59 | M |
| Patient 12 | 19 | M |
Appendix B
| Patient | Component | Constructs | Domain | ICF Code | Source | ||
|---|---|---|---|---|---|---|---|
| PATIENT01 | Body Functions | B1-Mental Functions | Global | Energy and Drive-Energy Level- | B130 | 0 | Med. let |
| PATIENT01 | Body Functions | B1-Mental Functions | Specific | Attention | B140 | 0 | QOLIBRI + Med. let. |
| PATIENT01 | Body Functions | B1-Mental Functions | Specific | Psychomotor-Control | B147 | 0 | QOLIBRI |
| PATIENT01 | Body Functions | B7-Neuromusculoskeletal and Movement | Muscles | Muscle Power | b730 | 2 | Med. let |
| PATIENT01 | Body Functions | B7-Neuromusculoskeletal and Movement | Movement | Control of voluntary Movement | B760 | QOLIBRI | |
| PATIENT01 | Activities & Participation | D4-Mobility | Walking and moving | Walking | D450 | Med. let. | |
| PATIENT01 | Activities & Participation | D8-Major Life Areas | Work and Employment | Remunerative Employment | D850 | QOLIBRI + Med. let. + interview | |
| PATIENT02 | Body Functions | B2-Sensory Functions and Pain | Hearing and Vestibular | Vestibular | B235 | 1 | Med. let. |
| PATIENT03 | Body Functions | B1-Mental Functions | Specific | Memory | B144 | Med. let. | |
| PATIENT03 | Body Functions | B1-Mental Functions | Specific | Psychomotor-Control | B147 | 0 | QOLIBRI + Med. let. |
| PATIENT03 | Body Functions | B1-Mental Functions | Specific | Thought pace | B160 | 0 | Med. let. |
| PATIENT03 | Body Functions | B7-Neuromusculoskeletal and Movement | Muscles | Muscle Power | B730 | Med. let. | |
| PATIENT03 | Body Functions | B7-Neuromusculoskeletal and Movement | Movement | Control of voluntary Movement | B760 | QOLIBRI | |
| PATIENT03 | Activities & Participation | D8-Major Life Areas | Work and Employment | Acquiring, Keeping and Terminating a Job | D845 | Med. let. | |
| PATIENT03 | Environmental Factors | E3-Support and Relationships | Health Professionals | E355 | Med. let. | ||
| PATIENT04 | Body Functions | B1-Mental Functions | Global | Energy and Drive-Motivation | B130 | 1 | QOLIBRI |
| PATIENT04 | Body Functions | B1-Mental Functions | Global | Energy and Drive-Energy Level- | B130 | 0 | QOLIBRI |
| PATIENT04 | Body Functions | B1-Mental Functions | Specific | Memory | B144 | QOLIBRI | |
| PATIENT04 | Body Functions | B1-Mental Functions | Specific | Psychomotor-Control | B147 | 0 | QOLIBRI |
| PATIENT04 | Body Functions | B2-Sensory Functions and Pain | Seeing | B210 | QOLIBRI + Med. let. | ||
| PATIENT04 | Body Functions | B2-Sensory Functions and Pain | Hearing and Vestibular | Hearing | B230 | QOLIBRI | |
| PATIENT04 | Body Functions | B4-Cardiovascular, Haematological, Immunological and Respiratory | Respiratory | Respiration | B440 | Med. let. | |
| PATIENT04 | Body Functions | B4-Cardiovascular, Haematological, Immunological and Respiratory | Respiratory | Respiratory Muscles | B445 | Med. let. | |
| PATIENT04 | Body Functions | B5-Digestive, Metabolic and Endocrine | Digestive | Ingestion-Swallowing | B510 | 5 | Med. let. |
| PATIENT04 | Body Functions | B5-Digestive, Metabolic and Endocrine | Digestive | Ingestion-Salivation | B510 | 4 | Med. let. |
| PATIENT04 | Body Functions | B7-Neuromusculoskeletal and Movement | Muscles | Muscle Power | B730 | 2 | Med. let. |
| PATIENT04 | Body Functions | B7-Neuromusculoskeletal and Movement | Movement | Control of voluntary Movement | B760 | QOLIBRI | |
| PATIENT04 | Activities & Participation | D4-Mobility | Walking and moving | Walking | D450 | Med. let. | |
| PATIENT04 | Activities & Participation | D4-Mobility | Walking and moving | Moving around in different locations | D460 | QOLIBRI | |
| PATIENT04 | Activities & Participation | D6-Domestic Life | Household tasks | Doing Housework | D640 | QOLIBRI | |
| PATIENT04 | Activities & Participation | D7-Interpersonnal Interactions and Relationships | Particular interpersonal relationships | Family relationships- parent-child | D760 | interview | |
| PATIENT04 | Activities & Participation | D8-Major Life Areas | Work and Employment | Remunerative Employment | D850 | QOLIBRI | |
| PATIENT04 | Activities & Participation | D9-Community, Social & Civic Life | Community Life | D910 | QOLIBRI | ||
| PATIENT04 | Activities & Participation | D9-Community, Social & Civic Life | Recreation and leisure | D920 | QOLIBRI | ||
| PATIENT04 | Activities & Participation | D5-Self Care | Self-care | QOLIBRI | |||
| PATIENT04 | nd | Projecting oneself into the future | QOLIBRI | ||||
| PATIENT04 | nd-gh | Other injuries sustained at time of brain injury | QOLIBRI | ||||
| PATIENT05 | Body Functions | B1-Mental Functions | Global | Energy and Drive | B130 | 0 | QOLIBRI + Med. let. |
| PATIENT05 | Body Functions | B1-Mental Functions | Specific | Attention | B140 | 0 | Med. let. |
| PATIENT05 | Body Functions | B1-Mental Functions | Specific | Memory | B144 | QOLIBRI | |
| PATIENT05 | Body Functions | B1-Mental Functions | Specific | Thought pace | B160 | 0 | QOLIBRI + Med. let. |
| PATIENT05 | Body Functions | B1-Mental Functions | Specific | Higher-level Cognitive- Organization and Planning | B164 | 1 | Med. let. |
| PATIENT05 | Activities & Participation | D3-Communication | Receiving | Receiving-Spoken | D310 | QOLIBRI | |
| PATIENT05 | Activities & Participation | D8-Major Life Areas | Work and Employment | Acquiring, Keeping and Terminating a Job | D845 | Med. let. | |
| PATIENT05 | Activities & Participation | D9-Community, Social & Civic Life | Community Life | D910 | QOLIBRI | ||
| PATIENT05 | Activities & Participation | D9-Community, Social & Civic Life | Recreation and leisure | D920 | QOLIBRI + Med. let. + interview | ||
| PATIENT05 | Activities & Participation | D5-Self Care | Self-Care | QOLIBRI | |||
| PATIENT05 | nd | Projecting oneself into the future | Med. let. | ||||
| PATIENT05 | nd-gh | Other injuries sustained at time of brain injury | QOLIBRI | ||||
| PATIENT06 | Body Functions | B2-Sensory Functions and Pain | Seeing and related | Seeing | B210 | Med. let. | |
| PATIENT06 | Body Functions | B2-Sensory Functions and Pain | Pain | Sensation of Pain | B280 | Med. let. | |
| PATIENT06 | Body Functions | B7-Neuromusculoskeletal and Movement | Muscles | Muscle Power | B730 | 2 | Med. let. |
| PATIENT06 | Activities & Participation | D7-Interpersonnal Interactions and Relationships | Particular interpersonal relationships | Intimate relationships-sexual | D770 | 2 | QOLIBRI |
| PATIENT06 | Activities & Participation | D5-Self Care | Self-Care | QOLIBRI | |||
| PATIENT06 | Body Functions | B4-Cardiovascular, Haematological, Immunological and Respiratory | Unspecified | Unspecified | B429 | Med. let. | |
| PATIENT07 | Body Functions | B1-Mental Functions | Global | Energy and Drive | B130 | 0 | Med. let. |
| PATIENT07 | Body Functions | B1-Mental Functions | Specific | Memory | B144 | QOLIBRI + Med. let. | |
| PATIENT07 | Body Functions | B1-Mental Functions | Specific | Emotions | B152 | QOLIBRI | |
| PATIENT07 | Body Functions | B1-Mental Functions | Specific | Higher-level Cognitive | B164 | QOLIBRI | |
| PATIENT07 | Body Functions | B1-Mental Functions | Specific | Experience of Self and Time | B180 | QOLIBRI | |
| PATIENT07 | Body Functions | B2-Sensory Functions and Pain | Pain | Sensation of Pain | B280 | Med. let. | |
| PATIENT07 | Activities & Participation | D9-Community, Social & Civic Life | Recreation and leisure | D920 | Med. let. | ||
| PATIENT07 | nd | Projecting oneself into the future | QOLIBRI | ||||
| PATIENT08 | Body Functions | B1-Mental Functions | Specific | Affect | B152 | QOLIBRI + Med. let. | |
| PATIENT08 | Body Functions | B2-Sensory Functions and Pain | Seeing and related | Seeing | B210 | Med. let. | |
| PATIENT08 | Activities & Participation | D7-Interpersonnal Interactions and Relationships | Particular interpersonal relationships | Informal Relationships-with Friends | D750 | 0 | QOLIBRI + interview |
| PATIENT08 | Activities & Participation | D7-Interpersonnal Interactions and Relationships | Particular interpersonal relationships | Family relationships | D760 | 0 | interview |
| PATIENT08 | Activities & Participation | D7-Interpersonnal Interactions and Relationships | Particular interpersonal relationships | Intimate relationships-sexual | D770 | 2 | QOLIBRI |
| PATIENT08 | Activities & Participation | D9-Community, Social & Civic Life | Recreation and leisure | D920 | Med. let. | ||
| PATIENT08 | Activities & Participation | D5-Self Care | Self-care | QOLIBRI | |||
| PATIENT08 | Environmental Factors | E3-Support and Relationships | Friends | E320 | interview | ||
| PATIENT08 | nd | Dependency towards others | Med. let. + interview | ||||
| PATIENT09 | Body Functions | B1-Mental Functions | Specific | Attention | B140 | QOLIBRI | |
| PATIENT09 | Body Functions | B1-Mental Functions | Specific | Memory | B144 | QOLIBRI + Med. let. | |
| PATIENT09 | Body Functions | B1-Mental Functions | Specific | Anxiety | B152 | Med. let. | |
| PATIENT09 | Body Functions | B1-Mental Functions | Specific | Affect | B152 | Med. let. | |
| PATIENT09 | Body Functions | B2-Sensory Functions and Pain | Seeing and related | Seeing | B210 | Med. let. | |
| PATIENT09 | Body Functions | B2-Sensory Functions and Pain | Pain | Sensation of Pain | B280 | 10 | QOLIBRI + Med. let. |
| PATIENT09 | Body Functions | B7-Neuromusculoskeletal and Movement | Joints & Bones | Mobility of Joints | B710 | Med. let. | |
| PATIENT09 | Activities & Participation | D4-Mobility | Walking and moving | Moving around in different locations | D460 | QOLIBRI | |
| PATIENT09 | Activities & Participation | D6-Domestic Life | Household tasks | Doing Housework | D640 | QOLIBRI | |
| PATIENT09 | Activities & Participation | D7-Interpersonnal Interactions and Relationships | Particular interpersonal relationships | Informal Relationships-with Friends | D750 | 0 | QOLIBRI + med. let. |
| PATIENT09 | Activities & Participation | D7-Interpersonnal Interactions and Relationships | Particular interpersonal relationships | Intimate relationships-spousal | D770 | 1 | QOLIBRI |
| PATIENT09 | Activities & Participation | D7-Interpersonnal Interactions and Relationships | Particular interpersonal relationships | Intimate relationships-sexual | D770 | 2 | QOLIBRI |
| PATIENT09 | Activities & Participation | D8-Major Life Areas | Education | Higher Education | D830 | QOLIBRI | |
| PATIENT09 | nd | Overall bother by effects of brain injury | QOLIBRI | ||||
| PATIENT09 | nd | Projecting oneself into the future | QOLIBRI + med. let. | ||||
| Patient | Component | Domain | ICF Code | SOURCE |
|---|---|---|---|---|
| PATIENT01 | Environmental factors | Friends | E320 | interview |
| PATIENT01 | Environmental factors | Immediate family | E310 | interview |
| PATIENT01 | Personal factors | Beliefs | interview | |
| PATIENT03 | Environmental factors | Friends | E320 | interview |
| PATIENT03 | Environmental factors | Health Professionals | E355 | Med. let. |
| PATIENT03 | Environmental factors | Immediate family | E310 | Med. let. + interview |
| PATIENT03 | Environmental factors | Products and technology for personal use in daily living | E115 | Med. let. |
| PATIENT04 | Environmental factors | Health Professionals | E355 | |
| PATIENT04 | Environmental factors | Immediate family | E310 | |
| PATIENT04 | Environmental factors | Products and technology for mobility and transportation | E120 | |
| PATIENT05 | Activities & Participation | Religion and spirituality | D930 | interview |
| PATIENT05 | Environmental factors | Friends | E320 | interview |
| PATIENT05 | Environmental factors | Immediate family | E310 | Med. let. + interview |
| PATIENT05 | Environmental factors | Individual attitudes of health professionals | E450 | interview |
| PATIENT05 | Personal factors | Beliefs | interview | |
| PATIENT06 | Activities & Participation | Family relationships | D760 | Med. let. + interview |
| PATIENT06 | Activities & Participation | Religion and spirituality | D930 | interview |
| PATIENT06 | Body Functions | Temperament and personality functions | B126 | interview |
| PATIENT06 | Environmental factors | Friends | E320 | interview |
| PATIENT06 | Environmental factors | Health Professionals | E355 | Med. let. |
| PATIENT06 | Environmental factors | Products and technology for mobility and transportation | E120 | Med. let. |
| PATIENT07 | Activities & Participation | Religion and spirituality | D930 | interview |
| PATIENT07 | Environmental factors | Health Professionals | E355 | Med. let. |
| PATIENT07 | Environmental factors | Immediate family | E310 | Med. let. + interview |
| PATIENT08 | Activities & Participation | Religion and spirituality | D930 | interview |
| PATIENT08 | Body Functions | Temperament and personality functions | B126 | Med. let. + interview |
| PATIENT08 | Environmental factors | Health Professionals | E355 | Med. let. |
| PATIENT08 | Environmental factors | Immediate family | E310 | Med. let. + interview |
| PATIENT08 | Environmental factors | Products and technology for mobility and transportation | E120 | Med. let. |
| PATIENT09 | Activities & Participation | Religion and spirituality | D930 | interview |
| PATIENT09 | Environmental factors | Acquaintances, peers, colleagues, neighbours and community members | E325 | interview |
| PATIENT09 | Environmental factors | Health Professionals | E355 | Med. let. |
| PATIENT09 | Environmental factors | Immediate family | E310 | Med. let. + interview |
| PATIENT09 | Environmental factors | Products and technology for mobility and transportation | E120 | Med. let. |
Appendix C
| Body functions | B1-Mental Functions (n = 7) | B2-Sensory Functions and Pain (n = 6) | B4-Cardiovascular and Respiratory (n = 2) | B5-Digestive (n = 1) | B7-Neuromusculoskeletal and Movement (n = 5) | |||||||||
| Domain | n | Domain | n | Domain | n | Domain | n | Domain | n | |||||
| B144-Memory | 5 | B210-Seeing | 4 | B440-Respiratory | 1 | Ingestion | 1 | B730-Muscle Power | 4 | |||||
| B130-Energy and Drive | 4 | B280-Sensation of Pain | 3 | B445-Respiratory Muscles | 1 | B760-Control of voluntary Movement | 3 | |||||||
| B140-Attention | 3 | B230-Hearing | 1 | B429-Oedema | 1 | B710-Mobility of Joints | 1 | |||||||
| B147-Psychomotor-Control | 3 | B235-Vestibular | 1 | |||||||||||
| B152-Emotional Functions | 3 | |||||||||||||
| B160-Thought-pace | 2 | |||||||||||||
| B164-Higher-level Cognitive | 2 | |||||||||||||
| B180-Experience of Self and Time | 1 | |||||||||||||
| Activity and Participation | D3-Communication (n = 1) | D4-Mobility (n = 3) | D5-Self Care (n = 4) | D6-Domestic Life (n = 2) | D7-Interpersonnal Interractions and Relationships (n = 4) | D8-Major Life Areas (n = 5) | D9-Community, Social & Civic Life (n = 4) | |||||||
| Domain | n | Domain | n | Domain | n | Domain | n | Domain | n | Domain | n | Domain | n | |
| Receiving-Spoken | 1 | Walking | 2 | nd | 4 | Doing House-work | 2 | Intimate relationships | 3 | Work and Employ-ment | 4 | Commun-ity Life | 2 | |
| Moving around in different locations | 2 | Informal Relationships-with Friends | 2 | Education | 1 | Recrea-tion and leisure | 4 | |||||||
| Family relationships | 2 | |||||||||||||
| Environmental factors | E3-Support and Relationships (n = 2) | |||||||||||||
| Friends | 1 | |||||||||||||
| Health Professionals | 1 | |||||||||||||
| nd | Nd (n = 5) | |||||||||||||
| Projecting oneself into the future | 4 | |||||||||||||
| Other injuries sustained at time of brain injury | 2 | |||||||||||||
| Dependency towards others | 1 | |||||||||||||
| Overall bother by effects of brain injury | 1 | |||||||||||||
| Domain | n |
|---|---|
| Immediate family | 7 |
| Health Professionals | 6 |
| Religion and spirituality | 5 |
| Products and technology for mobility and transportation | 4 |
| Friends | 4 |
| Beliefs | 2 |
| Temperament and personality functions | 2 |
| Individual attitudes of health professionals | 1 |
| Acquaintances, peers colleagues, neighbours and community members | 1 |
| Products and technology for personal use in daily living | 1 |
| Family relationships | 1 |
Appendix D
| GOSE Score | n |
|---|---|
| 4 Vegetative state | 1 |
| 3.2 Lower severe disability | 4 |
| 3.1 Upper severe disability | 2 |
| 2.2 Lower moderate disability | 3 |
| 2.1 Upper moderate disability | 1 |
| 1.2 Lower good recovery | 0 |
| 1.1 Upper good recovery | 1 |
References
- Pignat, J.-M.; Mauron, E.; Jöhr, J.; de Keranflec’H, C.G.; Van De Ville, D.; Preti, M.G.; Meskaldji, D.E.; Hömberg, V.; Laureys, S.; Draganski, B.; et al. Outcome Prediction of Consciousness Disorders in the Acute Stage Based on a Complementary Motor Behavioural Tool. PLoS ONE 2016, 11, e0156882. [Google Scholar] [CrossRef] [PubMed]
- Edlow, B.L.; Chatelle, C.; Spencer, C.A.; Chu, C.J.; Bodien, Y.G.; O’connor, K.L.; Hirschberg, R.E.; Hochberg, L.R.; Giacino, J.T.; Rosenthal, E.S.; et al. Early detection of consciousness in patients with acute severe traumatic brain injury. Brain 2017, 140, 2399–2414. [Google Scholar] [CrossRef] [PubMed]
- Pincherle, A.; Rossi, F.; Jöhr, J.; Dunet, V.; Ryvlin, P.; Oddo, M.; Schiff, N.; Diserens, K. Early discrimination of cognitive motor dissociation from disorders of consciousness: Pitfalls and clues. J. Neurol. 2020, 268, 178–188. [Google Scholar] [CrossRef] [PubMed]
- Jöhr, J.; Halimi, F.; Pasquier, J.; Pincherle, A.; Schiff, N.; Diserens, K. Recovery in cognitive motor dissociation after severe brain injury: A cohort study. PLoS ONE 2020, 15, e0228474. [Google Scholar] [CrossRef] [PubMed]
- Koskinen, S.; Hokkinen, E.-M.; Wilson, L.; Sarajuuri, J.; Von Steinbüchel, N.; Truelle, J.-L. Comparison of subjective and objective assessments of outcome after traumatic brain injury using the International Classification of Functioning, Disability and Health (ICF). Disabil. Rehabil. 2011, 33, 2464–2478. [Google Scholar] [CrossRef]
- Borgen, I.M.H.; Løvstad, M.; Andelic, N.; Hauger, S.; Sigurdardottir, S.; Søberg, H.L.; Sveen, U.; Forslund, M.V.; Kleffelgård, I.; Lindstad, M.; et al. Traumatic brain injury—needs and treatment options in the chronic phase: Study protocol for a randomized controlled community-based intervention. Trials 2020, 21, 294. [Google Scholar] [CrossRef]
- Wright, C.J.; Zeeman, H.; Biezaitis, V. Holistic Practice in Traumatic Brain Injury Rehabilitation: Perspectives of Health Practitioners. PLoS ONE 2016, 11, e0156826. [Google Scholar] [CrossRef]
- Von Steinbüchel, N.; Wilson, L.; Gibbons, H.; Hawthorne, G.; Höfer, S.; Schmidt, S.; Bullinger, M.; Maas, A.; Neugebauer, E.; Powell, J.; et al. Quality of Life after Brain Injury (QOLIBRI): Scale Development and Metric Properties. J. Neurotrauma 2010, 27, 1167–1185. [Google Scholar] [CrossRef]
- Katerndahl, D.A. Impact of Spiritual Symptoms and Their Interactions on Health Services and Life Satisfaction. Ann. Fam. Med. 2008, 6, 412–420. [Google Scholar] [CrossRef]
- Sulmasy, D.P. A Biopsychosocial-Spiritual Model for the Care of Patients at the End of Life. Gerontol. 2002, 42, 24–33. [Google Scholar] [CrossRef]
- World Health Organization. International Classification of Functioning, Disability and Health: ICF; World Health Organization: Geneva, Switzerland, 2001.
- Threats, T.T.; Worrall, L. Classifying communication disability using the ICF. Adv. Speech Lang. Pathol. 2004, 6, 53–62. [Google Scholar] [CrossRef]
- Laureys, S.; Celesia, G.G.; Cohadon, F.; Lavrijsen, J.; León-Carrión, J.; Sannita, W.G.; Sazbon, L.; Schmutzhard, E.; Von Wild, K.R.; Zeman, A.; et al. Unresponsive wakefulness syndrome: A new name for the vegetative state or apallic syndrome. BMC Med. 2010, 8, 68. [Google Scholar] [CrossRef] [PubMed]
- Giacino, J.T.; Ashwal, S.; Childs, N.; Cranford, R.; Jennett, B.; Katz, D.I.; Kelly, J.P.; Rosenberg, J.H.; Whyte, J.; Zafonte, R.D.; et al. The minimally conscious state: Definition and diagnostic criteria. Neurology 2002, 58, 349–353. [Google Scholar] [CrossRef] [PubMed]
- Bruno, M.-A.; Vanhaudenhuyse, A.; Thibaut, A.; Moonen, G.; Laureys, S. From unresponsive wakefulness to minimally conscious PLUS and functional locked-in syndromes: Recent advances in our understanding of disorders of consciousness. J. Neurol. 2011, 258, 1373–1384. [Google Scholar] [CrossRef] [PubMed]
- Schiff, N.D. Cognitive Motor Dissociation Following Severe Brain Injuries. JAMA Neurol. 2015, 72, 1413–1415. [Google Scholar] [CrossRef] [PubMed]
- Claassen, J.; Doyle, K.; Matory, A.; Couch, C.; Burger, K.M.; Velazquez, A.; Okonkwo, J.U.; King, J.-R.; Park, S.; Agarwal, S.; et al. Detection of Brain Activation in Unresponsive Patients with Acute Brain Injury. N. Engl. J. Med. 2019, 380, 2497–2505. [Google Scholar] [CrossRef]
- Jöhr, J.; Aureli, V.; Meyer, I.; Cossu, G.; Diserens, K. Clinical Cognitive Motor Dissociation: A Case Report Showing How Pitfalls Can Hinder Early Clinical Detection of Awareness. Brain Sci. 2022, 12, 157. [Google Scholar] [CrossRef]
- Lin, K.; Wroten, M. Ranchos Los Amigos. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2021. Available online: http://www.ncbi.nlm.nih.gov/books/NBK448151/ (accessed on 7 March 2022).
- Rappaport, M.; Hall, K.M.; Hopkins, K.; Belleza, T.; Cope, D.N. Disability rating scale for severe head trauma: Coma to community. Arch. Phys. Med. Rehabil. 1982, 63, 118–123. [Google Scholar]
- Krch, D.; Lequerica, A.H. The factor structure of the Disability Rating Scale in individuals with traumatic brain injury. Disabil. Rehabil. 2017, 41, 98–103. [Google Scholar] [CrossRef]
- COMBI The Center for Outcome Measurment in Brain Injur-Disability Rating Scale. Available online: https://www.tbims.org/combi/drs/ (accessed on 8 March 2022).
- Viosca, E.; Martínez, J.L.; Almagro, P.L.; Gracia, A.; González, C. Proposal and Validation of a New Functional Ambulation Classification Scale for Clinical Use. Arch. Phys. Med. Rehabil. 2005, 86, 1234–1238. [Google Scholar] [CrossRef]
- Jennett, B.; Bond, M. Assessment of outcome after severe brain damage: A Practical Scale. Lancet 1975, 305, 480–484. [Google Scholar] [CrossRef] [PubMed]
- Fayol, P.; Carrière, H.; Habonimana, D.; Preux, P.-M.; Dumond, J.-J. Version française de l’entretien structuré pour l’échelle de devenir de Glasgow (GOS): Recommandations et premières études de validation. Ann. Réadapt Médecine Phys. 2004, 47, 142–156. [Google Scholar] [CrossRef] [PubMed]
- Cieza, A.; Brockow, T.; Ewert, T.; Amman, E.; Kollerits, B.; Chatterji, S.; Üstün, T.B.; Stucki, G. Linking Health-Status Measurements to the International Classification of Functioning, Disability and Health. J. Rehabil. Med. 2002, 34, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Cieza, A.; Geyh, S.; Chatterji, S.; Kostanjsek, N.; Üstün, B.; Stucki, G. ICF linking rules: An update based on lessons learned. J. Rehabil. Med. 2005, 37, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Gorbunova, A.; Zeldovich, M.; Voormolen, D.C.; Krenz, U.; Polinder, S.; Haagsma, J.A.; Hagmayer, Y.; Covic, A.; Real, R.G.L.; Asendorf, T.; et al. Reference Values of the QOLIBRI from General Population Samples in the United Kingdom and The Netherlands. J. Clin. Med. 2020, 9, 2100. [Google Scholar] [CrossRef]
- Nakase-Richardson, R.; Whyte, J.; Giacino, J.T.; Pavawalla, S.; Barnett, S.D.; Yablon, S.A.; Sherer, M.; Kalmar, K.; Hammond, F.M.; Greenwald, B.; et al. Longitudinal Outcome of Patients with Disordered Consciousness in the NIDRR TBI Model Systems Programs. J. Neurotrauma 2012, 29, 59–65. [Google Scholar] [CrossRef]
- Dever, A.; Powell, D.; Graham, L.; Mason, R.; Das, J.; Marshall, S.J.; Vitorio, R.; Godfrey, A.; Stuart, S. Gait Impairment in Traumatic Brain Injury: A Systematic Review. Sensors 2022, 22, 1480. [Google Scholar] [CrossRef]
- U.S. Food and Drugs Administration. Public Workshop: Evaluating Inclusion and Exclusion Criteria in Clinical Trials. The National Press Club 2018. Available online: https://www.fda.gov/media/134754/download (accessed on 8 March 2022).
- Dikmen, S.S.; Machamer, J.E.; Powell, J.M.; Temkin, N.R. Outcome 3 to 5 years after moderate to severe traumatic brain injury. Arch. Phys. Med. Rehabil. 2003, 84, 1449–1457. [Google Scholar] [CrossRef]
- Stocchetti, N.; Zanier, E.R. Chronic impact of traumatic brain injury on outcome and quality of life: A narrative review. Crit. Care 2016, 20, 148. [Google Scholar] [CrossRef]
- Edlow, B.L.; Claassen, J.; Schiff, N.D.; Greer, D.M. Recovery from disorders of consciousness: Mechanisms, prognosis and emerging therapies. Nat. Rev. Neurol. 2020, 17, 135–156. [Google Scholar] [CrossRef]
- Rasmussen, M.S.; Andelic, N.; Pripp, A.H.; Nordenmark, T.H.; Soberg, H.L. The effectiveness of a family-centred intervention after traumatic brain injury: A pragmatic randomised controlled trial. Clin. Rehabil. 2021, 35, 1428–1441. [Google Scholar] [CrossRef] [PubMed]
- Hawthorne, G.; Gruen, R.L.; Kaye, A.H. Traumatic Brain Injury and Long-Term Quality of Life: Findings from an Australian Study. J. Neurotrauma 2009, 26, 1623–1633. [Google Scholar] [CrossRef] [PubMed]
- Gasquoine, P.G. Blissfully unaware: Anosognosia and anosodiaphoria after acquired brain injury. Neuropsychol. Rehabil. 2015, 26, 261–285. [Google Scholar] [CrossRef] [PubMed]





| SCALE | LCF-r | DRS | FAC | GOS | |||||
|---|---|---|---|---|---|---|---|---|---|
| Patient | Disorder Type | Acute | Post-Acute | Acute | Post-Acute | Acute | Post-Acute | Acute | Post-Acute |
| 1 | c-CMD | 6 | 10 | 11 | 1.5 | 0 | 4 | 3 | 2 |
| 2 | c-CMD | 7 | 10 | 4 | 0 | 2 | 5 | - | 1 |
| 3 | c-CMD | 6 | 10 | 6 | 1.5 | 0 | 5 | 3 | 2 |
| 4 | c-CMD | 7 | 10 | 6 | 6 | 1 | 1 | 3 | 3 |
| 5 | c-CMD | 7 | 10 | 4 | 1.5 | 3 | 5 | - | 2 |
| 6 | c-CMD | 7 | 10 | 7 | 6 | 0 | 1 | 3 | 3 |
| 7 | c-CMD | 5 | 9 | 13 | 4.5 | 0 | 3 | 3 | 2 |
| 8 | c-CMD | 6 | 8 | 8.5 | 7 | 1 | 1 | 3 | 3 |
| 9 | c-CMD | 5 | 9 | 11.5 | 5 | 0 | 3 | 3 | 3 |
| 10 | c-CMD | 5 | - | 12.5 | 15.5 | 0 | 1 | 3 | 3 |
| 11 | c-CMD | 6 | - | 9 | 8 | 0 | 0 | 3 | 3 |
| 12 | DOC | - | 3 | - | 20 | 0 | 0 | 4 | 4 |
| LCF-r | DRS | FAC | GOS | ||||
|---|---|---|---|---|---|---|---|
| Post-acute phase | |||||||
| Median: | 10 | Median | 5.50 | Median | 2.00 | Mean | 2.58 |
| Interquartile Range | 1.25 | Interquartile Range | 6.25 | Interquartile Range | 3.75 | Range | 3.00 |
| Evolution (Post-acute—Acute) | |||||||
| Mean: | 3.33 | Mean | −3.27 | Mean | 1.83 | Mean | 0.00 |
| Range: | 2.00 | SD | 3.78 | Range | 5.00 | Interquartile range | 1.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
La Framboise, N.F.; Rochat, E.; Diserens, K. A Biopsychosocial Evaluation of Post-Acute Outcome of Patients with Severe Brain Lesions Recovering from Coma: An Exploratory Study. J. Clin. Med. 2023, 12, 3572. https://doi.org/10.3390/jcm12103572
La Framboise NF, Rochat E, Diserens K. A Biopsychosocial Evaluation of Post-Acute Outcome of Patients with Severe Brain Lesions Recovering from Coma: An Exploratory Study. Journal of Clinical Medicine. 2023; 12(10):3572. https://doi.org/10.3390/jcm12103572
Chicago/Turabian StyleLa Framboise, Noah F., Etienne Rochat, and Karin Diserens. 2023. "A Biopsychosocial Evaluation of Post-Acute Outcome of Patients with Severe Brain Lesions Recovering from Coma: An Exploratory Study" Journal of Clinical Medicine 12, no. 10: 3572. https://doi.org/10.3390/jcm12103572
APA StyleLa Framboise, N. F., Rochat, E., & Diserens, K. (2023). A Biopsychosocial Evaluation of Post-Acute Outcome of Patients with Severe Brain Lesions Recovering from Coma: An Exploratory Study. Journal of Clinical Medicine, 12(10), 3572. https://doi.org/10.3390/jcm12103572