
Larissa Heart Failure Risk Score and Mode of Death in Acute Heart Failure: Insights from REALITY-AHF

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Definitions
2.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Study Outcomes
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ziaeian, B.; Fonarow, G.C. Epidemiology and aetiology of heart failure. Nat. Rev. Cardiol. 2016, 13, 368–378. [Google Scholar] [CrossRef] [PubMed]
- Groenewegen, A.; Rutten, F.H.; Mosterd, A.; Hoes, A.W. Epidemiology of heart failure. Eur. J. Heart Fail. 2020, 22, 1342–1356. [Google Scholar] [CrossRef] [PubMed]
- Roger, V.L. Epidemiology of Heart Failure: A Contemporary Perspective. Circ. Res. 2021, 128, 1421–1434. [Google Scholar] [CrossRef]
- Loungani, R.S.; Teerlink, J.R.; Metra, M.; Allen, L.A.; Butler, J.; Carson, P.E.; Chen, C.W.; Cotter, G.; Davison, B.A.; Eapen, Z.J.; et al. Cause of Death in Patients with Acute Heart Failure: Insights From RELAX-AHF-2. JACC Heart Fail. 2020, 8, 999–1008. [Google Scholar] [CrossRef]
- Xanthopoulos, A.; Giamouzis, G.; Tryposkiadis, K.; Paraskevopoulou, E.; Karagiannis, G.; Patsilinakos, S.; Parissis, J.; Farmakis, D.; Butler, J.; Skoularigis, J.; et al. A simple score for early risk stratification in acute heart failure. Int. J. Cardiol. 2016, 230, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Xanthopoulos, A.; Tryposkiadis, K.; Giamouzis, G.; Konstantinou, D.; Giannakoulas, G.; Karvounis, H.; Kattan, M.W.; Skoularigis, J.; Parissis, J.; Starling, R.C.; et al. Larissa Heart Failure Risk Score: A proposed simple score for risk stratification in chronic heart failure. Eur. J. Heart Fail. 2017, 20, 614–616. [Google Scholar] [CrossRef]
- Kitai, T.; Xanthopoulos, A.; Tang, W.W.; Kaji, S.; Furukawa, Y.; Oishi, S.; Akiyama, E.; Suzuki, S.; Yamamoto, M.; Kida, K.; et al. Validation of the Larissa Heart Failure Risk Score for risk stratification in acute heart failure. Int. J. Cardiol. 2019, 307, 119–124. [Google Scholar] [CrossRef]
- Matsue, Y.; Damman, K.; Voors, A.A.; Kagiyama, N.; Yamaguchi, T.; Kuroda, S.; Okumura, T.; Kida, K.; Mizuno, A.; Oishi, S.; et al. Time-to-Furosemide Treatment and Mortality in Patients Hospitalized with Acute Heart Failure. J. Am. Coll. Cardiol. 2017, 69, 3042–3051. [Google Scholar] [CrossRef]
- Kitai, T.; Tang, W.H.W.; Xanthopoulos, A.; Murai, R.; Yamane, T.; Kim, K.; Oishi, S.; Akiyama, E.; Suzuki, S.; Yamamoto, M.; et al. Impact of early treatment with intravenous vasodilators and blood pressure reduction in acute heart failure. Open Heart 2018, 5, e000845. [Google Scholar] [CrossRef]
- Kagiyama, N.; Matsue, Y. The time-to-treatment concept in acute heart failure: Lessons and implications from REALITY-AHF. Anatol. J. Cardiol. 2018, 20, 125–129. [Google Scholar] [CrossRef]
- Spinar, J.; Jarkovsky, J.; Spinarova, L.; Mebazaa, A.; Gayat, E.; Vitovec, J.; Linhart, A.; Widimsky, P.; Miklik, R.; Zeman, K.; et al. AHEAD score—Long-term risk classification in acute heart failure. Int. J. Cardiol. 2015, 202, 21–26. [Google Scholar] [CrossRef]
- Chen, Y.J.; Sung, S.H.; Cheng, H.M.; Huang, W.M.; Wu, C.L.; Huang, C.J.; Hsu, P.F.; Yeh, J.S.; Guo, C.Y.; Yu, W.C.; et al. Performance of AHEAD Score in an Asian Cohort of Acute Heart Failure with Either Preserved or Reduced Left Ventricular Systolic Function. J. Am. Heart Assoc. 2017, 6, e004297. [Google Scholar] [CrossRef] [PubMed]
- Vaduganathan, M.; Patel, R.B.; Shah, S.J.; Butler, J. Sudden cardiac death in heart failure with preserved ejection fraction: A target for therapy? Heart Fail. Rev. 2016, 21, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Rohde, L.E.; Chatterjee, N.A.; Vaduganathan, M.; Claggett, B.; Packer, M.; Desai, A.S.; Zile, M.; Rouleau, J.; Swedberg, K.; Lefkowitz, M.; et al. Sacubitril/Valsartan and Sudden Cardiac Death According to Implantable Cardioverter-Defibrillator Use and Heart Failure Cause: A PARADIGM-HF Analysis. JACC Heart Fail. 2020, 8, 844–855. [Google Scholar] [CrossRef]
- Odajima, S.; Tanaka, H.; Fujimoto, W.; Kuroda, K.; Yamashita, S.; Imanishi, J.; Iwasaki, M.; Todoroki, T.; Okuda, M.; Hayashi, T.; et al. Efficacy of Renin-angiotensin-aldosterone-system inhibitors for heart failure with preserved ejection fraction and left ventricular hypertrophy -from the KUNIUMI Registry Acute Cohort. J. Cardiol. 2022, 79, 703–710. [Google Scholar] [CrossRef]
- Saku, K.; Yokota, S.; Nishikawa, T.; Kinugawa, K. Interventional heart failure therapy: A new concept fighting against heart failure. J. Cardiol. 2021, 80, 101–109. [Google Scholar] [CrossRef]
- Oates, C.P.; Santos-Gallego, C.G.; Smith, A.; Basyal, B.; Moss, N.; Kawamura, I.; Musikantow, D.R.; Turagam, M.K.; Miller, M.A.; Whang, W.; et al. SGLT2 inhibitors reduce sudden cardiac death risk in heart failure: Meta-analysis of randomized clinical trials. J. Cardiovasc. Electrophysiol. 2023, 34, 1277–1285. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Anker, S.D.; Anand, I.; Linker, D.T.; Sullivan, M.D.; Cleland, J.G.; Carson, P.E.; Maggioni, A.P.; Mann, D.L.; Pitt, B.; et al. Prediction of mode of death in heart failure: The Seattle Heart Failure Model. Circulation 2007, 116, 392–398. [Google Scholar] [CrossRef] [PubMed]
- Desai, A.S.; Vaduganathan, M.; Cleland, J.G.; Claggett, B.L.; Barkoudah, E.; Finn, P.; McCausland, F.R.; Yilmaz, M.B.; Lefkowitz, M.; Shi, V.; et al. Mode of Death in Patients with Heart Failure and Preserved Ejection Fraction: Insights From PARAGON-HF Trial. Circ. Heart Fail. 2021, 14, e008597. [Google Scholar] [CrossRef]
- Rohde, L.E.; Vaduganathan, M.; Claggett, B.L.; Polanczyk, C.A.; Dorbala, P.; Packer, M.; Desai, A.S.; Zile, M.; Rouleau, J.; Swedberg, K.; et al. Dynamic changes in cardiovascular and systemic parameters prior to sudden cardiac death in heart failure with reduced ejection fraction: A PARADIGM-HF analysis. Eur. J. Heart Fail. 2021, 23, 1346–1356. [Google Scholar] [CrossRef]
- Canepa, M.; Fonseca, C.; Chioncel, O.; Laroche, C.; Crespo-Leiro, M.G.; Coats, A.J.; Mebazaa, A.; Piepoli, M.F.; Tavazzi, L.; Maggioni, A.P.; et al. Performance of Prognostic Risk Scores in Chronic Heart Failure Patients Enrolled in the European Society of Cardiology Heart Failure Long-Term Registry. JACC: Heart Fail. 2018, 6, 452–462. [Google Scholar] [CrossRef] [PubMed]
- Agostoni, P.; Corrà, U.; Cattadori, G.; Veglia, F.; La Gioia, R.; Scardovi, A.B.; Emdin, M.; Metra, M.; Sinagra, G.; Limongelli, G.; et al. Metabolic exercise test data combined with cardiac and kidney indexes, the MECKI score: A multiparametric approach to heart failure prognosis. Int. J. Cardiol. 2013, 167, 2710–2718. [Google Scholar] [CrossRef] [PubMed]
- Salvioni, E.; Bonomi, A.; Re, F.; Mapelli, M.; Mattavelli, I.; Vitale, G.; Sarullo, F.M.; Palermo, P.; Veglia, F.; Agostoni, P. The MECKI score initiative: Development and state of the art. Eur. J. Prev. Cardiol. 2020, 27, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Tung, Y.-C.; Chang, G.-M.; Chang, H.-Y.; Yu, T.-H. Relationship between Early Physician Follow-Up and 30-Day Readmission after Acute Myocardial Infarction and Heart Failure. PLoS ONE 2017, 12, e0170061. [Google Scholar] [CrossRef] [PubMed]
- Miró, O.; Rossello, X.; Platz, E.; Masip, J.; Gualandro, D.M.; Peacock, W.F.; Price, S.; Cullen, L.; DiSomma, S.; de Oliveira, M.T., Jr.; et al. Risk stratification scores for patients with acute heart failure in the Emergency Department: A systematic review. Eur. Heart J. Acute Cardiovasc. Care 2020, 9, 375–398. [Google Scholar] [CrossRef]
- O’Connor, C.M.; Abraham, W.T.; Albert, N.M.; Clare, R.; Stough, W.G.; Gheorghiade, M.; Greenberg, B.H.; Yancy, C.W.; Young, J.B.; Fonarow, G.C. Predictors of mortality after discharge in patients hospitalized with heart failure: An analysis from the Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF). Am. Heart J. 2008, 156, 662–673. [Google Scholar] [CrossRef]
- Scrutinio, D.; Ammirati, E.; Guida, P.; Passantino, A.; Raimondo, R.; Guida, V.; Braga, S.S.; Pedretti, R.; Lagioia, R.; Frigerio, M.; et al. Clinical utility of N-terminal pro-B-type natriuretic peptide for risk stratification of patients with acute decompensated heart failure. Derivation and validation of the ADHF/NT-proBNP risk score. Int. J. Cardiol. 2013, 168, 2120–2126. [Google Scholar] [CrossRef]
- Scrutinio, D.; Ammirati, E.; Guida, P.; Passantino, A.; Raimondo, R.; Guida, V.; Sarzi Braga, S.; Canova, P.; Mastropasqua, F.; Frigerio, M.; et al. The ADHF/NT-proBNP risk score to predict 1-year mortality in hospitalized patients with advanced decompensated heart failure. J. Heart Lung Transpl. 2014, 33, 404–411. [Google Scholar] [CrossRef]
- Okazaki, H.; Shirakabe, A.; Hata, N.; Yamamoto, M.; Kobayashi, N.; Shinada, T.; Tomita, K.; Tsurumi, M.; Matsushita, M.; Yamamoto, Y.; et al. New scoring system (APACHE-HF) for predicting adverse outcomes in patients with acute heart failure: Evaluation of the APACHE II and Modified APACHE II scoring systems. J. Cardiol. 2014, 64, 441–449. [Google Scholar] [CrossRef]
- O’Connor, C.M.; Hasselblad, V.; Mehta, R.H.; Tasissa, G.; Califf, R.M.; Fiuzat, M.; Rogers, J.G.; Leier, C.V.; Stevenson, L.W. Triage After Hospitalization with Advanced Heart Failure: The ESCAPE (Evaluation Study of Congestive Heart Failure and Pulmonary Artery Catheterization Effectiveness) Risk Model and Discharge Score. J. Am. Coll. Cardiol. 2010, 55, 872–878. [Google Scholar] [CrossRef]
- Rogers, J.K.; Pocock, S.J.; McMurray, J.J.; Granger, C.B.; Michelson, E.L.; Östergren, J.; Pfeffer, M.A.; Solomon, S.D.; Swedberg, K.; Yusuf, S. Analysing recurrent hospitalizations in heart failure: A review of statistical methodology, with application to CHARM-Preserved. Eur. J. Heart Fail. 2013, 16, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.H.; Levy, W.; Welch, K.B.; Neuberg, G.W.; O’Connor, C.M.; Carson, P.E.; Miller, A.B.; Ghali, J.K. Association Between Bilirubin and Mode of Death in Severe Systolic Heart Failure. Am. J. Cardiol. 2013, 111, 1192–1197. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e876–e894. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | LHFRS = 0, 1 n = 789 | LHFRS = 2–4 n = 574 | p Value |
|---|---|---|---|
| Age (mean (SD)) | 78.47 (12.10) | 75.56 (12.90) | <0.001 |
| Males, n (%) | 430 (54.5) | 339 (59.1) | 0.105 |
| Systolic Blood Pressure (mean (SD)) | 154.90 (35.67) | 135.47 (33.20) | <0.001 |
| Diastolic Blood Pressure (mean (SD)) | 85.74 (25.67) | 78.86 (22.63) | <0.001 |
| Heart Rate (mean (SD)) | 96.98 (27.80) | 96.56 (28.48) | 0.784 |
| Ambulance, n (%) | 452 (57.3) | 306 (53.3) | 0.16 |
| De novo HF, n (%) | 400 (50.7) | 247 (43.0) | 0.006 |
| Symptom onset (%) | 0.013 | ||
| 6 h | 188 (23.8) | 108 (18.8) | |
| ≤2 days | 190 (24.1) | 122 (21.3) | |
| >2 days | 411 (52.1) | 344 (59.9) | |
| ECG rhythm (%) | 0.001 | ||
| Sinus rhythm | 446 (56.5) | 268 (46.7) | |
| Atrial fibrillation | 262 (33.2) | 239 (41.6) | |
| Other | 81 (10.3) | 67 (11.7) | |
| Echo visual estimation of LVEF (%) | <0.001 | ||
| <35 | 243 (32.3) | 256 (46.7) | |
| 35–50 | 228 (30.3) | 141 (25.7) | |
| >50 | 281 (37.4) | 151 (27.6) | |
| Heart Failure Symptoms/Signs | |||
| Jugular Venous Distension, n (%) | 428 (54.7) | 319 (56.2) | 0.623 |
| Orthopnea, n (%) | 471 (59.8) | 290 (50.5) | 0.001 |
| Rales, n (%) | 512 (64.9) | 355 (62.0) | 0.291 |
| Peripheral edema, n (%) | 531 (67.3) | 393 (68.6) | 0.658 |
| Pulmonary edema, n (%) | 594 (75.3) | 378 (65.9) | <0.001 |
| Comorbidities/Risk factors | |||
| Hypertension, n (%) | 789 (100.0) | 131 (22.8) | <0.001 |
| Diabetes Mellitus, n (%) | 305 (38.7) | 193 (33.6) | 0.065 |
| Coronary Artery Disease, n (%) | 213 (27.0) | 224 (39.0) | <0.001 |
| Peripheral Arterial Disease, n (%) | 64 (8.1) | 39 (6.8) | 0.421 |
| Chronic Obstructive Pulmonary Disease, n (%) | 78 (9.9) | 53 (9.2) | 0.756 |
| Smoker, n (%) | 287 (36.4) | 212 (37.0) | 0.858 |
| Laboratory Variables | |||
| Hemoglobin (mean (SD)) | 11.83 (2.23) | 11.56 (2.36) | 0.033 |
| RDW-CV (mean (SD)) | 14.56 (1.64) | 15.56 (2.30) | <0.001 |
| White Blood Cells (median [IQR]) | 7800 [5900, 10,400] | 7000 [5500, 9300] | <0.001 |
| Glucose (mean (SD)) | 166.65 (75.96) | 157.20 (76.26) | 0.026 |
| Blood Urine Nitrogen (median [IQR]) | 24.50 [17.80, 34.60] | 25 [18.42, 36] | 0.288 |
| Creatinine (median [IQR]) | 1.13 [0.86, 1.64] | 1.12 [0.85, 1.58] | 0.585 |
| Estimated Glomerular Filtration Rate (mean (SD)) | 55.17 (25.14) | 58.00 (26.22) | 0.044 |
| Aspartate Aminotransferase (median [IQR]) | 30 [23, 44] | 33 [23, 49] | 0.068 |
| Alanine Aminotransferase (median [IQR]) | 21 [14, 34] | 22 [14, 37] | 0.286 |
| Na+ (mean (SD)) | 139.20 (4.61) | 138.28 (4.44) | <0.001 |
| CRP (median [IQR]) | 0.58 [0.19, 2.26] | 0.75 [0.22, 2.04] | 0.175 |
| Medications at admission | |||
| ACE-inhibitors, n (%) | 135 (17.1) | 99 (17.2) | 1 |
| Angiotensin Receptor Blockers, n (%) | 296 (37.5) | 121 (21.1) | <0.001 |
| Beta Blockers, n (%) | 330 (42.0) | 280 (49.0) | 0.013 |
| Mineralocorticoid Antagonists, n (%) | 131 (16.6) | 171 (29.8) | <0.001 |
| Loop diuretics, n (%) | 376 (48.1) | 332 (57.9) | <0.001 |
| Medications at discharge | |||
| ACE-inhibitors, n (%) | 246 (32.8) | 193 (36.2) | 0.220 |
| Angiotensin Receptor Blockers, n (%) | 284 (37.8) | 119 (22.3) | <0.001 |
| Beta Blockers, n (%) | 546 (72.4) | 395 (73.8) | 0.616 |
| Mineralocorticoid Antagonists, n (%) | 318 (42.1) | 264 (49.3) | 0.012 |
| Loop diuretics, n (%) | 640 (84.7) | 460 (85.7) | 0.674 |
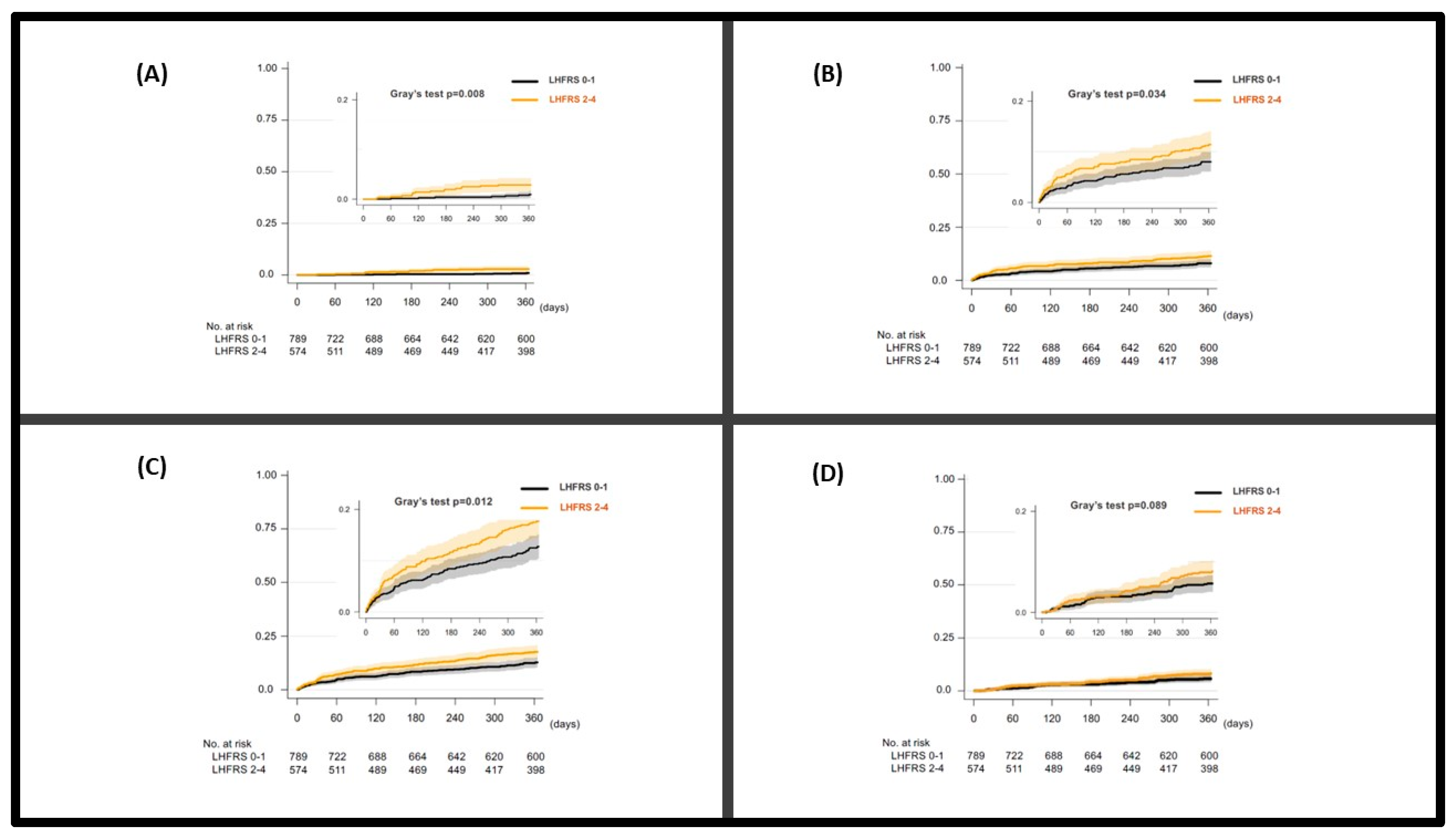
| Sudden Cardiac Death | ||||||
|---|---|---|---|---|---|---|
| Groups | Unadjusted | Adjusted for AHEAD Score | ||||
| HR | 95% CI | p Value | HR | 95% CI | p Value | |
| AHEAD score | 1.33 | 1.02–1.72 | 0.033 | 1.23 | 0.93–1.63 | 0.15 |
| LARISSA Score 0,1 | 1 (Reference) | 1 (Reference) | ||||
| LARISSA Score 2–4 | 3.14 | 1.29–7.61 | 0.008 | 3.15 | 1.30–7.65 | 0.011 |
| Heart Failure Death | ||||||
| Groups | Unadjusted | Adjusted for AHEAD score | ||||
| HR | 95% CI | p value | HR | 95% CI | p value | |
| AHEAD score | 1.43 | 1.24–1.64 | <0.001 | 1.38 | 1.18–1.60 | <0.001 |
| LARISSA Score 0,1 | 1 (Reference) | 1 (Reference) | ||||
| LARISSA Score 2–4 | 1.46 | 1.03–2.07 | 0.034 | 1.48 | 1.04–2.09 | 0.03 |
| Cardiovascular Death | ||||||
| Groups | Unadjusted | Adjusted for AHEAD score | ||||
| HR | 95% CI | p value | HR | 95% CI | p value | |
| AHEAD score | 1.38 | 1.23–1.54 | <0.001 | 1.32 | 1.17–1.49 | <0.001 |
| LARISSA Score 0,1 | 1 (Reference) | 1 (Reference) | ||||
| LARISSA Score 2–4 | 1.43 | 1.08–1.89 | 0.012 | 1.44 | 1.09–1.91 | 0.01 |
| Non-cardiovascular Death | ||||||
| Groups | Unadjusted | Adjusted for AHEAD score | ||||
| HR | 95% CI | p value | HR | 95% CI | p value | |
| AHEAD score | 1.26 | 1.09–1.47 | 0.002 | 1.28 | 1.13–1.42 | 0.003 |
| LARISSA Score 0,1 | 1 (Reference) | 1 (Reference) | ||||
| LARISSA Score 2–4 | 1.44 | 0.95–2.18 | 0.089 | 1.44 | 0.95–2.19 | 0.087 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xanthopoulos, A.; Bourazana, A.; Matsue, Y.; Fujimoto, Y.; Oishi, S.; Akiyama, E.; Suzuki, S.; Yamamoto, M.; Kida, K.; Okumura, T.; et al. Larissa Heart Failure Risk Score and Mode of Death in Acute Heart Failure: Insights from REALITY-AHF. J. Clin. Med. 2023, 12, 3722. https://doi.org/10.3390/jcm12113722
Xanthopoulos A, Bourazana A, Matsue Y, Fujimoto Y, Oishi S, Akiyama E, Suzuki S, Yamamoto M, Kida K, Okumura T, et al. Larissa Heart Failure Risk Score and Mode of Death in Acute Heart Failure: Insights from REALITY-AHF. Journal of Clinical Medicine. 2023; 12(11):3722. https://doi.org/10.3390/jcm12113722
Chicago/Turabian StyleXanthopoulos, Andrew, Angeliki Bourazana, Yuya Matsue, Yudai Fujimoto, Shogo Oishi, Eiichi Akiyama, Satoshi Suzuki, Masayoshi Yamamoto, Keisuke Kida, Takahiro Okumura, and et al. 2023. "Larissa Heart Failure Risk Score and Mode of Death in Acute Heart Failure: Insights from REALITY-AHF" Journal of Clinical Medicine 12, no. 11: 3722. https://doi.org/10.3390/jcm12113722
APA StyleXanthopoulos, A., Bourazana, A., Matsue, Y., Fujimoto, Y., Oishi, S., Akiyama, E., Suzuki, S., Yamamoto, M., Kida, K., Okumura, T., Giamouzis, G., Skoularigis, J., Triposkiadis, F., & Kitai, T. (2023). Larissa Heart Failure Risk Score and Mode of Death in Acute Heart Failure: Insights from REALITY-AHF. Journal of Clinical Medicine, 12(11), 3722. https://doi.org/10.3390/jcm12113722