
Effect of Intravenous Dexamethasone Dose on the Occurrence of Rebound Pain after Axillary Plexus Block in Ambulatory Surgery
 , and
, and
Abstract
:1. Introduction
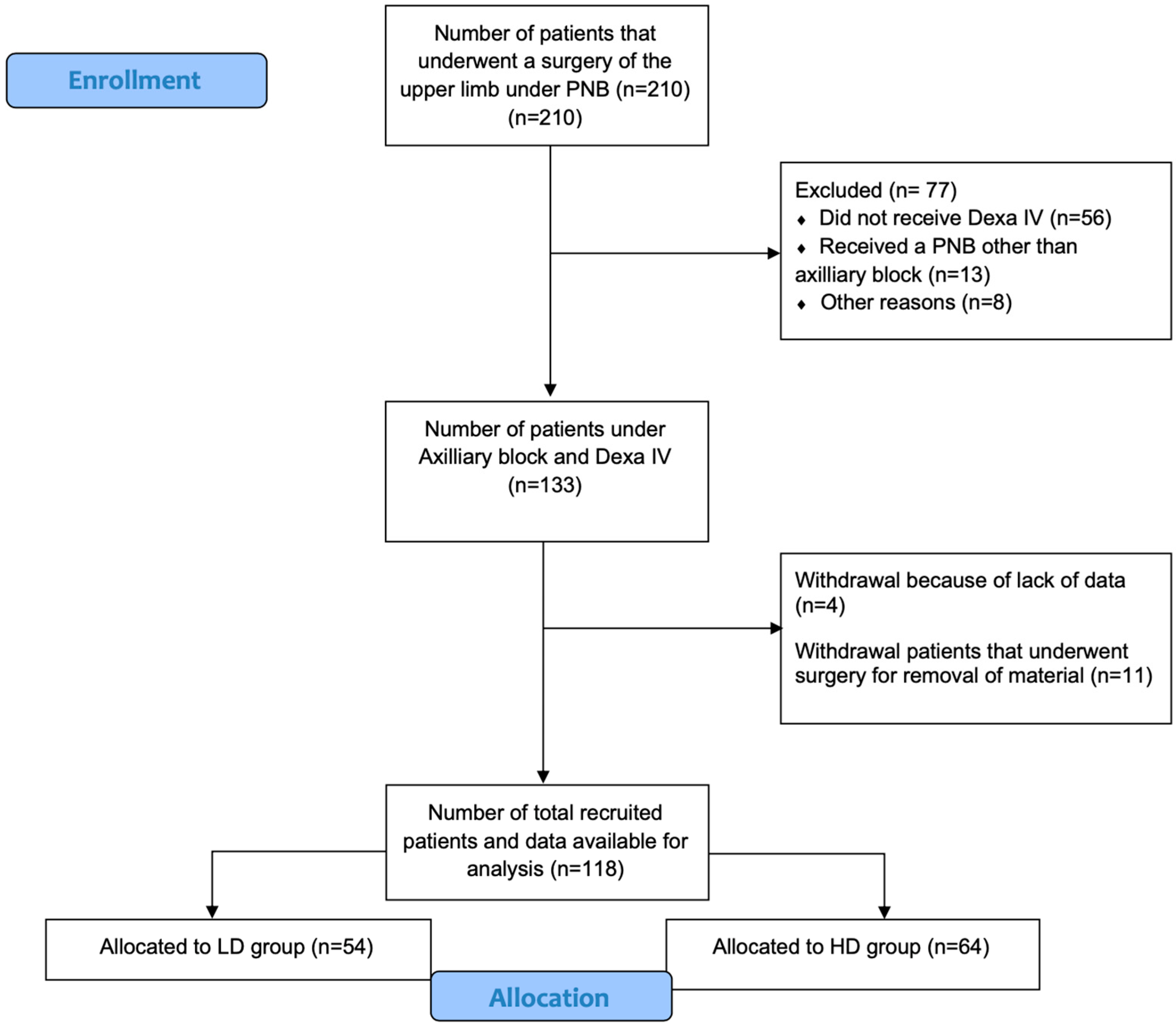
2. Materials and Methods
2.1. Recruitment
2.2. Data Collection
2.3. Statistical Analysis
2.3.1. Power Analysis
2.3.2. Data Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kolny, M.; Stasiowski, M.J.; Zuber, M.; Marciniak, R.; Chabierska, E.; Pluta, A.; Jałowiecki, P.; Byrczek, T. Randomized, comparative study of the effectiveness of three different techniques of interscalene brachial plexus block using 0.5% ropivacaine for shoulder arthroscopy. Anaesthesiol. Intensive Ther. 2017, 49, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Hade, A.D.; Okano, S.; Pelecanos, A.; Chin, A. Factors associated with low levels of patient satisfaction following peripheral nerve block. Anaesth. Intensive Care 2021, 49, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Lavand’homme, P. Rebound pain after regional anesthesia in the ambulatory patient. Curr. Opin. Anaesthesiol. 2018, 31, 679–684. [Google Scholar] [CrossRef] [PubMed]
- Dada, O.; Gonzalez Zacarias, A.; Ongaigui, C.; Echeverria-Villalobos, M.; Kushelev, M.; Bergese, S.D.; Moran, K. Does Rebound Pain after Peripheral Nerve Block for Orthopedic Surgery Impact Postoperative Analgesia and Opioid Consumption? A Narrative Review. Int. J. Environ. Res. Public Health 2019, 16, 3257. [Google Scholar] [CrossRef] [Green Version]
- Barry, G.S.; Bailey, J.G.; Sardinha, J.; Brousseau, P.; Uppal, V. Factors associated with rebound pain after peripheral nerve block for ambulatory surgery. Br. J. Anaesth. 2021, 126, 862–871. [Google Scholar] [CrossRef] [PubMed]
- Touil, N.; Pavlopoulou, A.; Barbier, O.; Libouton, X.; Lavand’homme, P. Evaluation of intraoperative ketamine on the prevention of severe rebound pain upon cessation of peripheral nerve block: A prospective randomised, double-blind, placebo-controlled study. Br. J. Anaesth. 2022, 128, 734–741. [Google Scholar] [CrossRef]
- Myles, P.S.; Corcoran, T. Benefits and Risks of Dexamethasone in Noncardiac Surgery. Anesthesiology 2021, 135, 895–903. [Google Scholar] [CrossRef]
- Albrecht, E.; Kern, C.; Kirkham, K.R. A systematic review and meta-analysis of perineural dexamethasone for peripheral nerve blocks. Anaesthesia 2015, 70, 71–83. [Google Scholar] [CrossRef]
- Desai, N.; El-Boghdadly, K.; Albrecht, E. Peripheral nerve blockade and novel analgesic modalities for ambulatory anesthesia. Curr. Opin. Anaesthesiol. 2020, 33, 760–767. [Google Scholar] [CrossRef]
- Kirkham, K.R.; Albrecht, E. Perineural or intravenous dexamethasone in interscalene brachial plexus block. Br. J. Anaesth. 2020, 124, 15–17. [Google Scholar] [CrossRef]
- Woo, J.H.; Lee, H.J.; Oh, H.W.; Lee, J.W.; Baik, H.J.; Kim, Y.J. Perineural dexamethasone reduces rebound pain after ropivacaine single injection interscalene block for arthroscopic shoulder surgery: A randomized controlled trial. Reg. Anesth. Pain Med. 2021, 46, 965–970. [Google Scholar] [CrossRef] [PubMed]
- Fang, J.; Shi, Y.; Du, F.; Xue, Z.; Cang, J.; Miao, C.; Zhang, X. The effect of perineural dexamethasone on rebound pain after ropivacaine single-injection nerve block: A randomized controlled trial. BMC Anesthesiol. 2021, 21, 47. [Google Scholar] [CrossRef] [PubMed]
- Holmberg, A.; Hassellund, S.S.; Draegni, T.; Nordby, A.; Ottesen, F.S.; Gulestøl, A.; Raeder, J. Analgesic effect of intravenous dexamethasone after volar plate surgery for distal radius fracture with brachial plexus block anaesthesia: A prospective, double-blind randomised clinical trial. Anaesthesia 2020, 75, 1448–1460. [Google Scholar] [CrossRef] [PubMed]
- Quartana, P.J.; Buenaver, L.F.; Edwards, R.R.; Klick, B.; Haythornthwaite, J.A.; Smith, M.T. Pain catastrophizing and salivary cortisol responses to laboratory pain testing in temporomandibular disorder and healthy participants. J. Pain 2010, 11, 186–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Oliveira, G.S., Jr.; Almeida, M.D.; Benzon, H.T.; McCarthy, R.J. Perioperative single dose systemic dexamethasone for postoperative pain: A meta-analysis of randomized controlled trials. Anesthesiology 2011, 115, 575–588. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, K.; Nishigami, T.; Mibu, A.; Manfuku, M.; Yono, S.; Yukioka, M.; Miki, K. Cutoff Value for Short Form of Central Sensitization Inventory. Pain. Pract. 2020, 20, 269–276. [Google Scholar] [CrossRef]
- Bouhassira, D.; Attal, N.; Alchaar, H.; Boureau, F.; Brochet, B.; Bruxelle, J.; Cunin, G.; Fermanian, J.; Ginies, P.; Grun-Overdyking, A.; et al. Comparison of pain syndromes associated with nervous or somatic lesions and development of a new neuropathic pain diagnostic questionnaire (DN4). Pain 2005, 114, 29–36. [Google Scholar] [CrossRef]
- Garnaud, B.; Mares, O.; L’Hermite, J.; Vialles, N.; Gricourt, Y.; Lannelongue, A.; Lefrant, J.Y.; Cuvillon, P. Multimodal oral analgesia strategy after ambulatory arthroscopic shoulder surgery: Case series using adaptive therapeutic approaches by sequential analysis. J. Shoulder Elbow Surg. 2021, 30, 250–257. [Google Scholar] [CrossRef]
- Albrecht, E.; Reynvoet, M.; Fournier, N.; Desmet, M. Dose-response relationship of perineural dexamethasone for interscalene brachial plexus block: A randomised, controlled, triple-blind trial. Anaesthesia 2019, 74, 1001–1008. [Google Scholar] [CrossRef]
- Woo, J.H.; Kim, Y.J.; Kim, D.Y.; Cho, S. Dose-dependency of dexamethasone on the analgesic effect of interscalene block for arthroscopic shoulder surgery using ropivacaine 0.5%: A randomised controlled trial. Eur. J. Anaesthesiol. 2015, 32, 650–655. [Google Scholar] [CrossRef] [Green Version]
- Zorrilla-Vaca, A.; Li, J. Dexamethasone Injected Perineurally is More Effective than Administered Intravenously for Peripheral Nerve Blocks: A Meta-Analysis of Randomized Controlled Trials. Clin. J. Pain 2018, 34, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Desmet, M.; Vanneste, B.; Reynvoet, M.; Van Cauwelaert, J.; Verhelst, L.; Pottel, H.; Missant, C.; Van de Velde, M. A randomised controlled trial of intravenous dexamethasone combined with interscalene brachial plexus blockade for shoulder surgery. Anaesthesia 2015, 70, 1180–1185. [Google Scholar] [CrossRef] [PubMed]
- Marhofer, P.; Columb, M.; Hopkins, P.M.; Greher, M.; Marhofer, D.; Bienzle, M.; Zeitlinger, M. Dexamethasone as an adjuvant for peripheral nerve blockade: A randomised, triple-blinded crossover study in volunteers. Br. J. Anaesth. 2019, 122, 525–531. [Google Scholar] [CrossRef] [Green Version]
- Short, A.; El-Boghdadly, K.; Clarke, H.; Komaba, T.; Jin, R.; Chin, K.J.; Chan, V. Effect of intravenous dexamethasone on the anaesthetic characteristics of peripheral nerve block: A double-blind, randomised controlled, dose-response volunteer study. Br. J. Anaesth. 2020, 124, 92–100. [Google Scholar] [CrossRef]
- Desmet, M.; Braems, H.; Reynvoet, M.; Plasschaert, S.; Van Cauwelaert, J.; Pottel, H.; Carlier, S.; Missant, C.; Van de Velde, M.I.V. and perineural dexamethasone are equivalent in increasing the analgesic duration of a single-shot interscalene block with ropivacaine for shoulder surgery: A prospective, randomized, placebo-controlled study. Br. J. Anaesth. 2013, 111, 445–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newman, H.; Shih, Y.V.; Varghese, S. Resolution of inflammation in bone regeneration: From understandings to therapeutic applications. Biomaterials 2021, 277, 121114. [Google Scholar] [CrossRef] [PubMed]
- Kidd, B.L.; Urban, L.A. Mechanisms of inflammatory pain. Br. J. Anaesth. 2001, 87, 3–11. [Google Scholar] [CrossRef] [Green Version]
- Edwards, R.R.; Kronfli, T.; Haythornthwaite, J.A.; Smith, M.T.; McGuire, L.; Page, G.G. Association of catastrophizing with interleukin-6 responses to acute pain. Pain 2008, 140, 135–144. [Google Scholar] [CrossRef] [Green Version]
- Corcoran, T.B.; O’Loughlin, E.; Chan, M.T.V.; Ho, K.M. Perioperative ADministration of Dexamethasone And blood Glucose concentrations in patients undergoing elective non-cardiac surgery—The randomised controlled PADDAG trial. Eur. J. Anaesthesiol. 2021, 38, 932–942. [Google Scholar] [CrossRef]
- Crandell, J.T. Perineal pruritus after the administration of iv dexamethasone. Can. J. Anaesth. 2004, 51, 398. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Control Group (n = 55) | DEXA Group (n = 118) | p Value | |
|---|---|---|---|
| Age (years) | 52 ± 18 | 45 ± 16 | 0.428 |
| Sex ratio (female/male) (n) | 29/26 | 78/40 | 0.298 |
| BMI 2 (kg/m2) | 25 (21–29) | 26 (22–29) | 0.266 |
| Bone surgery (n) | 21 (39%) | 64 (40%) | 0.854 |
| Tourniquet duration (min) | 22 (14–38) | 21 (12–33) | 0.742 |
| Preoperative | |||
| Catastrophizing (0–52) | 12 (3–23) | 11 (3–22) | 0.774 |
| Central sensitization (0–36) | 9.0 (6–12) | 8.5 (4–15) | 0.449 |
| Preoperative pain | |||
| Average pain (NRS 0–10) | 2.0 (0–4) | 2.0 (0–5) | 0.403 |
| Maximal pain (NRS 0–10) | 4.5 (1–8) | 5.0 (0–7) | 0.510 |
| Night pain (NRS 0–10) | 0 (0–3) | 0 (0–4.5) | 0.764 |
| DN4 3 value (0–10) | 3.0 (1–4) | 2.0 (1–4) | 0.622 |
| PNB 4 duration | |||
| Total duration (min) | 630 (506–795) | 640 (410–905) | 0.892 |
| Pain when PNB wears off (NRS 5 0–10) | 4.5 (2–8) | 3.3 (1–6) * | 0.030 |
| Incidence of rebound pain (NRS >7/10) (n) | 26 (47%) | 27 (23%) * | 0.002 |
| Control Group (n = 55) | DEXA LD (n = 54) | DEXA HD (n = 64) | p Value | |
|---|---|---|---|---|
| DEXA dose (mg/kg) | ---- | 0.06 (0.05–0.07) | 0.10 (0.10–0.12) | <0.001 |
| PNB duration | ||||
| H1–H2 5 (min) | 400 (309–541) | 292 (195–540) | 332 (223–577) | 0.092 |
| H2–H3 6 (min) | 180 (120–307) | 240 (165–300) | 205 (79–405) | 0.331 |
| Total duration (min) | 630 (506–795) | 583 (445–825) | 661 (402–960) | 0.650 |
| Preoperative pain at day 1 | ||||
| Average pain (NRS 7 0–10) | 25 (1–55) | 2.0 (1–4) | 2.0 (0–5) | 0.408 |
| Maximal pain (NRS 0–10) | 4.0 (2–7) | 6.0 (2–8) | 5.0 (1–8) | 0.564 |
| Pain when PNB wears off (NRS 0–10) | 4.5 (2–8) | 4.0 (1–7) | 3.0 (1–6) | 0.053 |
| Incidence of rebound pain (NRS > 7/10) (n) | 26 (47%) | 14 (26%) * | 13 (20%) * | 0.029 |
| Rebound Pain (n = 27) | No Rebound Pain (n = 91) | p Value | |
|---|---|---|---|
| Age (years) | 45 ± 16 | 51 ± 18 | 0.073 |
| Sex female (n) | 20 (74%) | 48 (53%) | 0.075 |
| BMI 2 (kg/m2) | 28 ± 6 * | 25 ± 5.5 | 0.026 |
| Bone surgery (n) | 17 (65%) * | 31 (34%) | 0.013 |
| Tourniquet duration (min) | 34 ± 26 | 24 ± 17 | 0.121 |
| Preoperative | |||
| Catastrophizing (0–52) | 20 (4–37) * | 9 (2–21) | 0.017 |
| High catastrophizers (n) | 11 (42%) * | 14 (16%) | 0.007 |
| Central sensitization (0–36) | 8.5 (2–17) | 8.5 (4–15) | 0.787 |
| Central sensitization positive (n) | 4 (16%) | 12 (14%) | 0.757 |
| Preoperative pain | |||
| Average pain (NRS 3 0–10) | 4.5 (2–6) * | 2.0 (0–4) | 0.009 |
| Maximal pain (NRS 0–10) | 7.3 (1–9) | 4.5 (0–7) | 0.065 |
| Night pain (NRS 0–10) | 1 (0–6) | 0 (0–3.8) | 0.222 |
| DN4 4 value (0–10) | 3.0 (2–4.5) | 2.0 (1–4) | 0.135 |
| PNB 5 duration | |||
| Total duration (min) | 630 (506–795) | 640 (410–905) | 0.892 |
| Pain when PNB wears off (NRS 3 0–10) | 8.0 (7–8.9) * | 2.0 (1–4) | <0.001 |
| DEXA dose (mg/kg) | 0.08 (0.06–0.10) | 0.09 (0.06–0.10) | 0.650 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Touil, N.; Pavlopoulou, A.; Delande, S.; Geradon, P.; Barbier, O.; Libouton, X.; Lavand’homme, P. Effect of Intravenous Dexamethasone Dose on the Occurrence of Rebound Pain after Axillary Plexus Block in Ambulatory Surgery. J. Clin. Med. 2023, 12, 4310. https://doi.org/10.3390/jcm12134310
Touil N, Pavlopoulou A, Delande S, Geradon P, Barbier O, Libouton X, Lavand’homme P. Effect of Intravenous Dexamethasone Dose on the Occurrence of Rebound Pain after Axillary Plexus Block in Ambulatory Surgery. Journal of Clinical Medicine. 2023; 12(13):4310. https://doi.org/10.3390/jcm12134310
Chicago/Turabian StyleTouil, Nassim, Athanassia Pavlopoulou, Simon Delande, Pierre Geradon, Olivier Barbier, Xavier Libouton, and Patricia Lavand’homme. 2023. "Effect of Intravenous Dexamethasone Dose on the Occurrence of Rebound Pain after Axillary Plexus Block in Ambulatory Surgery" Journal of Clinical Medicine 12, no. 13: 4310. https://doi.org/10.3390/jcm12134310
APA StyleTouil, N., Pavlopoulou, A., Delande, S., Geradon, P., Barbier, O., Libouton, X., & Lavand’homme, P. (2023). Effect of Intravenous Dexamethasone Dose on the Occurrence of Rebound Pain after Axillary Plexus Block in Ambulatory Surgery. Journal of Clinical Medicine, 12(13), 4310. https://doi.org/10.3390/jcm12134310