1. Introduction
The prevalence of lifestyle-related diseases, namely overweight and obesity, type 2 diabetes mellitus (T2DM), cardiovascular conditions and osteoarthritis (OA), is high and still increasing worldwide [
1,
2,
3,
4]. As a result of overlapping risk factor profiles, most subjects are eventually diagnosed with more than one of these conditions or display relevant risk factors for a second (or third, fourth, etc.) disease. Thus, multimorbidity is the rule, not just the exception, in this context.
Multimorbidity is a complex phenomenon, for which, to date, no generally accepted definition exists. While the WHO defines multimorbidity as ‘the co-occurrence of two or more chronic medical conditions in one person’, this definition is not very useful in clinical practice, where usually a narrower definition, specifically focusing on lifestyle-related diseases, is more appropriate. While typical disease combinations and patterns can be defined, for example, T2DM in combination with obesity, it is important to note that a ‘typical’ multimorbid patient does not exist, which has to be taken into account when developing and designing therapeutic strategies. In addition, associated factors, namely psychosocial characteristics (see below) or medication—multimorbidity is often accompanied with polypharmacy—have to be taken into account (for review, see [
5]).
The high prevalence of lifestyle-related diseases, usually in the context of multimorbidity, has led to the development of a new field of medicine, the so-called ‘lifestyle medicine’. It analyzes the complex interplay of different characteristics of an unhealthy lifestyle and their contribution to disease development. In addition, based on this knowledge, it develops strategies aiming at attenuating lifestyle-associated risk factors. These can act on a preventive or therapeutic level. The most important risk factors associated with an unhealthy lifestyle are tobacco smoking, overweight/obesity, a high blood pressure, an unhealthy diet and a sedentary lifestyle. Most patients with chronic lifestyle-related diseases present with several of these risk factors; thus, programs aiming at helping these patients to adopt a healthier lifestyle should be multi-faceted, including elements to enhance physical activity as well as nutritional counselling. In addition, psychosocial factors, such as volition and motivation, are very important. Consequently, lifestyle intervention programs should also contain coaching sessions that help patients overcome typical barriers and obstacles that might hamper the adoption of a healthier lifestyle and—even more importantly—their adherence to it (for review, see [
6]).
Nevertheless, despite the fact that lifestyle intervention programs based on these elements, i.e., the promotion of physical activity as well as nutritional and psychosocial counselling, are known to be highly efficient to prevent, treat and stabilize lifestyle-related diseases (for review, see [
6]), so far, exercise responses in subjects with multimorbidity have not been well characterized, and it is unclear how training programs for this cohort of patients should be designed, monitored and regulated [
7].
Exercise biomarkers, i.e., biological factors that respond to physical activity and sports and can be assessed in bodily fluids such as blood or urine, are promising candidates for training supervision and management. In the context of subjects with lifestyle-related diseases, metabolism-associated markers in particular have important potential. Adipokines such as leptin, adiponectin and resistin are released from adipose tissue and are involved in metabolic control. All of these markers have been shown to respond to exercise interventions in patients with either (pre)diabetes and/or overweight/obesity (for reviews, see [
8,
9]).
‘MultiPill-Exercise’ is a lifestyle intervention program designed to increase exercise participation and improve activity behavior in subjects with multimorbidity. The program consists of a set of exercise-based modules, as well as associated elements such as psychosocial counselling or nutritional support, and has previously been described in detail [
10].
Briefly, the program consisted of two 12 week periods, the first of which was designed as a more supervised phase, including regular sessions at our outpatient clinic. Here, patients underwent a specific training program, consisting of different elements, where all patients were subjected to individually shaped sessions of endurance, strength and functional training, in which training intensity was continuously adapted with increasing fitness. The program also included so-called ‘movement teasers’, in which patients could choose between a variety of different activities, such as Thai Chi/Yoga, Aqua Fitness or dancing. This first 12 week period was followed by a more self-directed period of the same duration, during which subjects were advised to maintain regular physical activity while training at local gyms or recreational fitness centers. In addition, patients were also advised to keep a training log. The program also contained classroom sessions, delivering both theoretical and practical knowledge on how to achieve a healthy lifestyle. These lectures addressed topics such as ‘principles of exercise and training’, ‘active everyday lifestyle’ and ‘nutrition and health’, as well as psychosocial factors such as personal motives and goals, motivation, volition and barriers. Furthermore, patients were offered individual counselling sessions to address the topics most relevant to them in more depth, as well as additional disease-specific offerings such as relaxation classes, workshops teaching strengthening exercises for specific muscles or T2DM-oriented nutritional counselling.
The data described here are the results of a pilot study on n = 39 subjects that was carried out in 2019/2020 [
11]. Based thereon, a prospective, randomized, controlled trial on n = 320 subjects was initiated in April 2022 [
11].
To assess the potential relevance of exercise-responsive biomarkers in this cohort, we tested three adipokines (leptin, adiponectin and resistin). The primary goals of our exploratory study were to assess adipokine patterns in this heterogeneous patient subgroup throughout the intervention to evaluate their potential to monitor and predict individual training responses, and to establish specific hypotheses for further testing in the future.
2. Subjects, Materials and Methods
Subjects and training intervention. The design of our pilot study ‘MultiPill-Exercise’ has previously been described [
12]. Briefly, n = 39 subjects (men: n = 12; women: n = 27; mean age 55.2 ± 10.3 years; mean BMI 31.1 ± 3.0 kg/m
2) who presented with at least two of four conditions (obesity, T2DM, cardiovascular disease and OA or a risk thereof) were enrolled in the study. Subjects were recruited in two waves, starting in August of 2019 (n = 20) and in January of 2020 (n = 19). They were exposed to a six-month health intervention program which included endurance and resistance physical activity (PA), as well as psychosocial and nutritional counselling. At baseline (T0), as well as after three (T1) and six (T2) months of the intervention, extensive diagnostics, including spiroergometry and calipometry (three-point method [
13,
14]), as well as blood and urine sampling, were performed. Urine was taken to assess a specific OA marker, i.e., CTX-II (C-terminal cross-linked telopeptide of type II collagen); however, due to the low number of OA patients in our sample, a statistical analysis of these data was not possible, similar to data for another OA marker, COMP (cartilage oligomeric protein), that we assessed in the circulation. Due to COVID-19-associated restrictions, T1 diagnostics had to be cancelled for subjects in wave #2. In addition, as specified in [
11], the intervention itself had to be considerably adapted and modified for this group to comply with COVID-19 contact restrictions then effective at our institution. For some subjects, no spiroergometry data were available at T1 or T2, or they dropped out of the entire study (for reasons, see [
11]). In addition, for technical reasons, some or all biomarkers were not determined for certain subjects included in wave #2. For details, see
Table 1. The study was conducted in accordance with the Declaration of Helsinki, approved by the Ethics Committee of the Medical Clinic Tübingen (298/2019BO2, 05-04-2019) and registered at the German clinical trial register (DRKS00016702). For a flow diagram of study progression, please refer to [
11].
Determination of adipokine concentrations. Adipokines (leptin, adiponectin and resistin) were determined using specific ELISAs (leptin: E07 ELISA/Mediagnost, Reutlingen, Germany; adiponectin: E09 ELISA/Mediagnost, Reutlingen, Germany; resistin: E 50 ELISA/Mediagnost, Reutlingen, Germany). All factors were determined from patients’ serum. At baseline (T0), n = 39 samples of waves #1 and #2 were analyzed for adiponectin and resistin and n = 38 for leptin (no data available for MP1952 for technical reasons). After three months (T1) and after six months (T6), n = 20 and n = 17 samples, respectively, of the first wave were analyzed for all markers, with n = 3 subjects (MP1902, MP1912 and MP1913) having been lost to follow-up at T2. In addition, for technical reasons, no biomarkers were assessed for subjects of wave #2 at T2. For leptin analyses, sera of MP1932, MP1946 and MP1949 had to be diluted two-fold, in contrast to all other samples which were employed in the assays as undiluted fluids. With the exception of the leptin reading for subject MP1953, which corresponded to a single read, all analyses were run in duplicates and the respective means were taken for further analysis. Finally, for subjects MP1906 and MP1913, no spiroergometry data were available at T1, and for subjects MP1901 and MP1919 at T2, since subjects discontinued cycling for reasons other than peripheral exhaustion. For details, see
Table 1.
Statistical analysis. Quantitative results were reported as means ± standard deviation. Comparisons of biomarker concentrations between patient subgroups and within-group comparisons (i.e., over time) were carried out using unpaired or paired t-tests, respectively. Simple linear regression and multiple linear regression analyses were performed to analyze the data through generalized least squares. Additionally, Akaike information criterion (AIC) was used to compare models through the maximum likelihood estimate of each model, with lower levels indicating better fits of the respective model. Shapiro–Wilk tests were performed on each variable to test its normality, and in case it was significant (p < 0.05), a log transformation was applied to the data. Spearman’s correlation coefficients were used to determine the association between two variables. Due to the exploratory character of our study, no correction for multiple testing was introduced. Statistical analyses were carried out using SPSS, Version 26.0 (IBM Corporation, Armonk, New York, NY, USA).
4. Discussion
Adipokine leptin was identified in 1994 as the gene product of the
ob gene, which is defect in obese
ob/ob mice. Via modulation of the production of specific neuropeptides, it regulates the activity of the ‘hunger’ and ‘satiety’ centers in the hypothalamus, thereby repressing appetite and consequently food intake. Thus, initially, strategies aiming at increasing leptin levels were considered as a new therapeutic approach in the treatment of obesity. However, it was soon discovered that individuals with obesity show increased, not decreased, levels when compared to lean subjects, despite the fact that leptin deficiency leads to obesity in
ob/ob mice. The reason for this is that people with obesity have often developed resistance to the actions of leptin, a complex phenomenon involving, among others, effects on leptin transport, the density of leptin receptors on cell surfaces and leptin receptor downstream signaling. Novel therapeutic approaches aim at combining leptin administration with that of a so-called leptin sensitizer, which can overpower leptin resistance (for a review, see [
15]). In addition, as demonstrated in our study, leptin might be a suitable predictive biomarker in the context of exercise-centered lifestyle intervention programs for subjects with obesity.
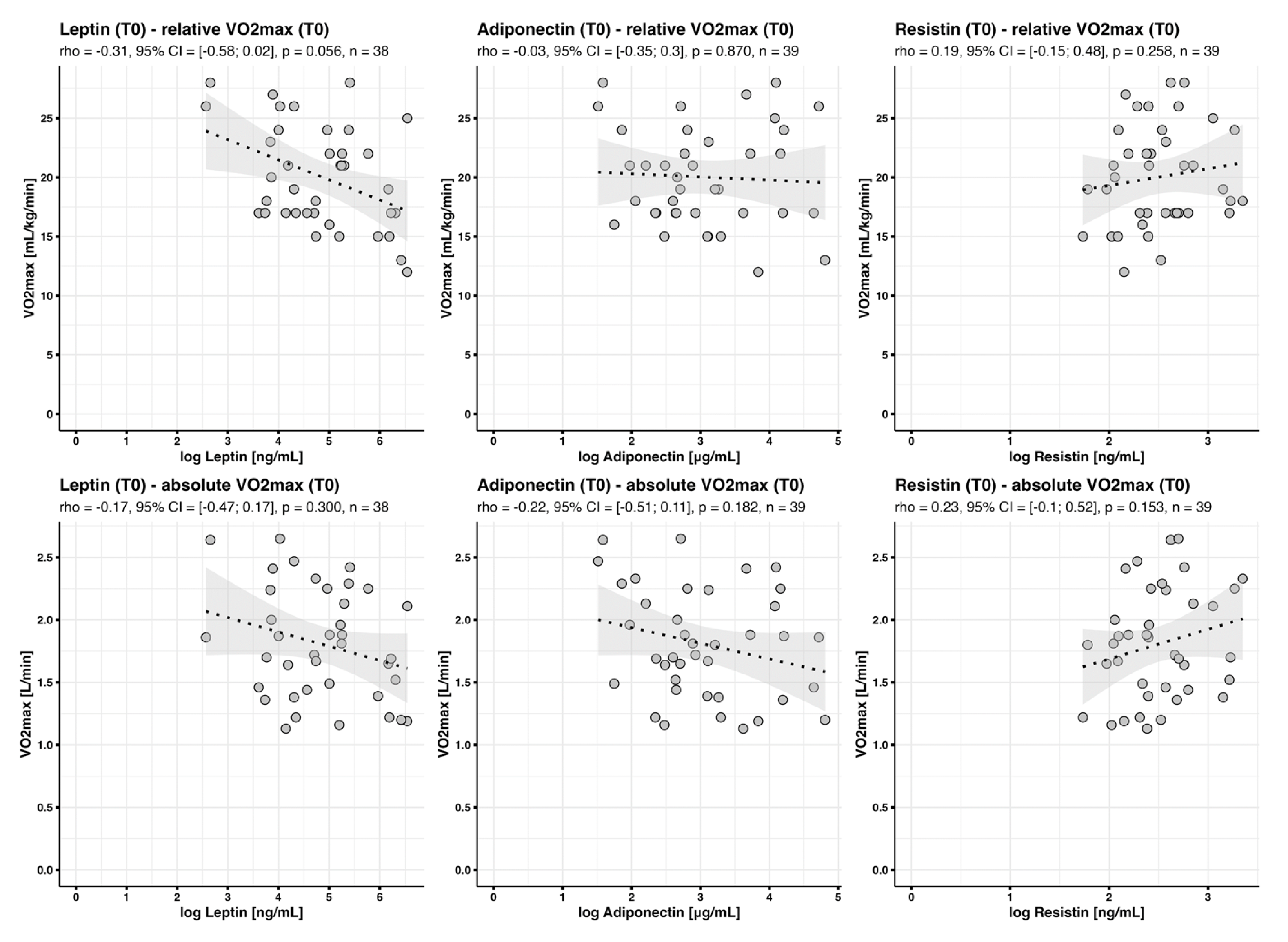
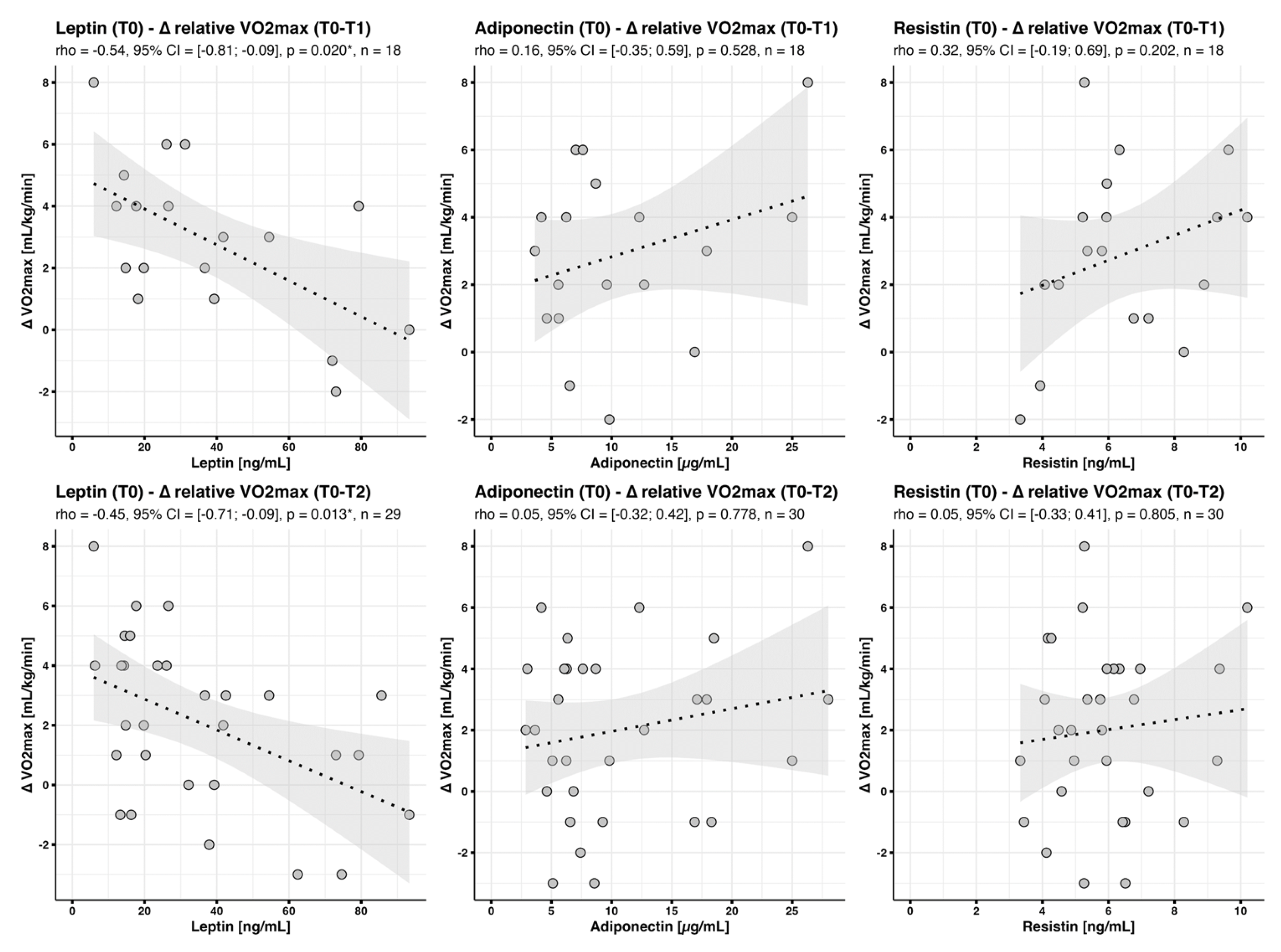
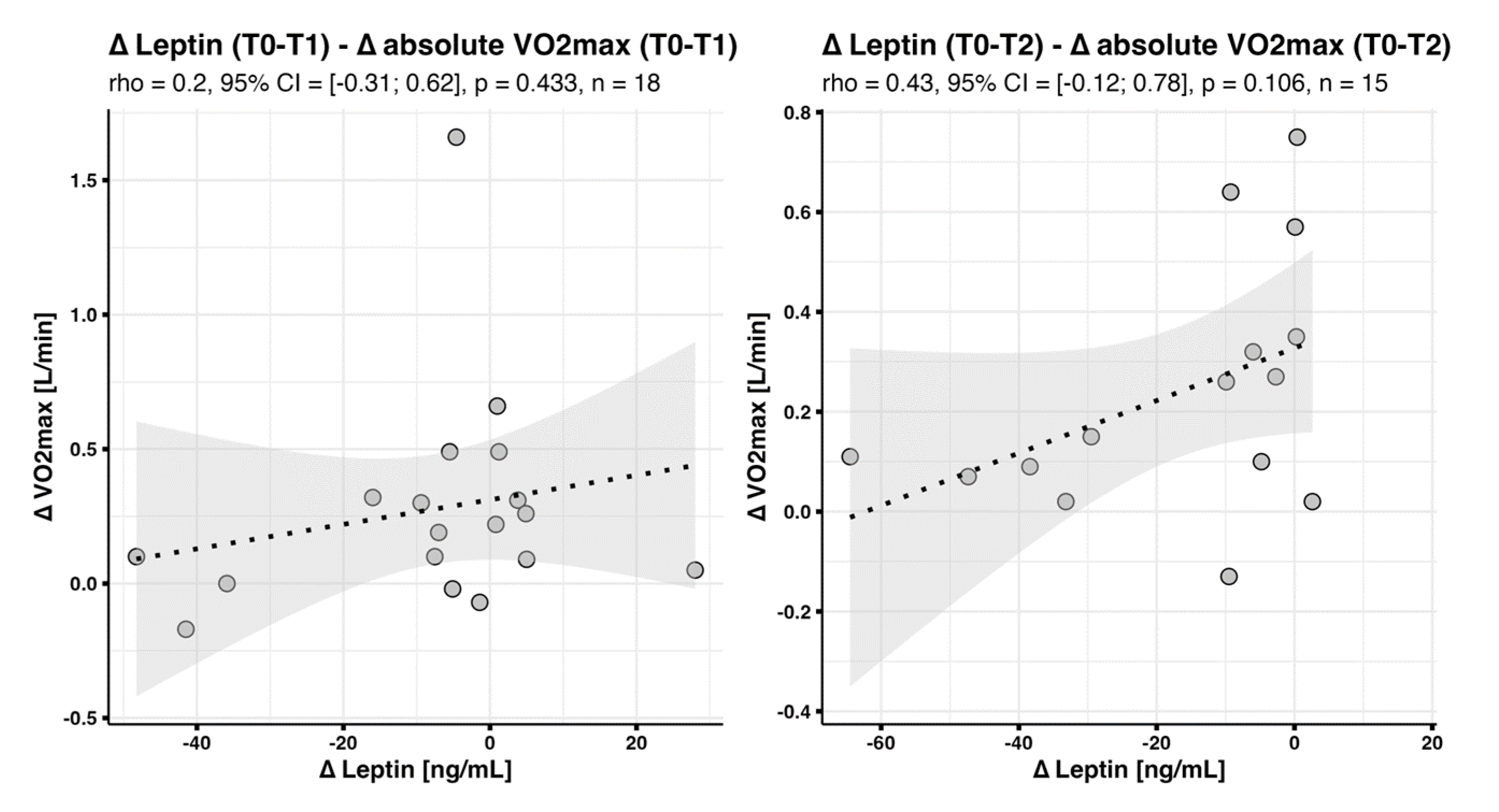
In the context of clinical practice, our data indicate that leptin might be a suitable surrogate biomarker to manage, monitor and evaluate exercise-based lifestyle interventions for subjects with multimorbidity, whereas adiponectin and resistin might be less appropriate. Particularly in subjects at risk for obesity or T2DM, adiponectin and resistin concentrations did not change significantly throughout the intervention. In contrast, as expected, leptin concentrations were elevated in subjects with overweight and obesity, and, specifically in the latter, declined during the intervention. A qualitative individualized analysis suggested that, predominantly in subjects with very high leptin readings at baseline, concentrations of this adipokine strongly declined by T1 and (even more) T2. Moreover, we observed a strong association between baseline leptin levels and changes in cardiorespiratory fitness (
), indicating that people with higher leptin concentrations benefitted less from the intervention in terms of increasing their aerobic capacity. This effect might in part be due to the fact that
and BMI, as well as BMI and leptin concentrations, are strong confounders, as has been described in a broad variety of other previous studies (for reviews, see [
16,
17,
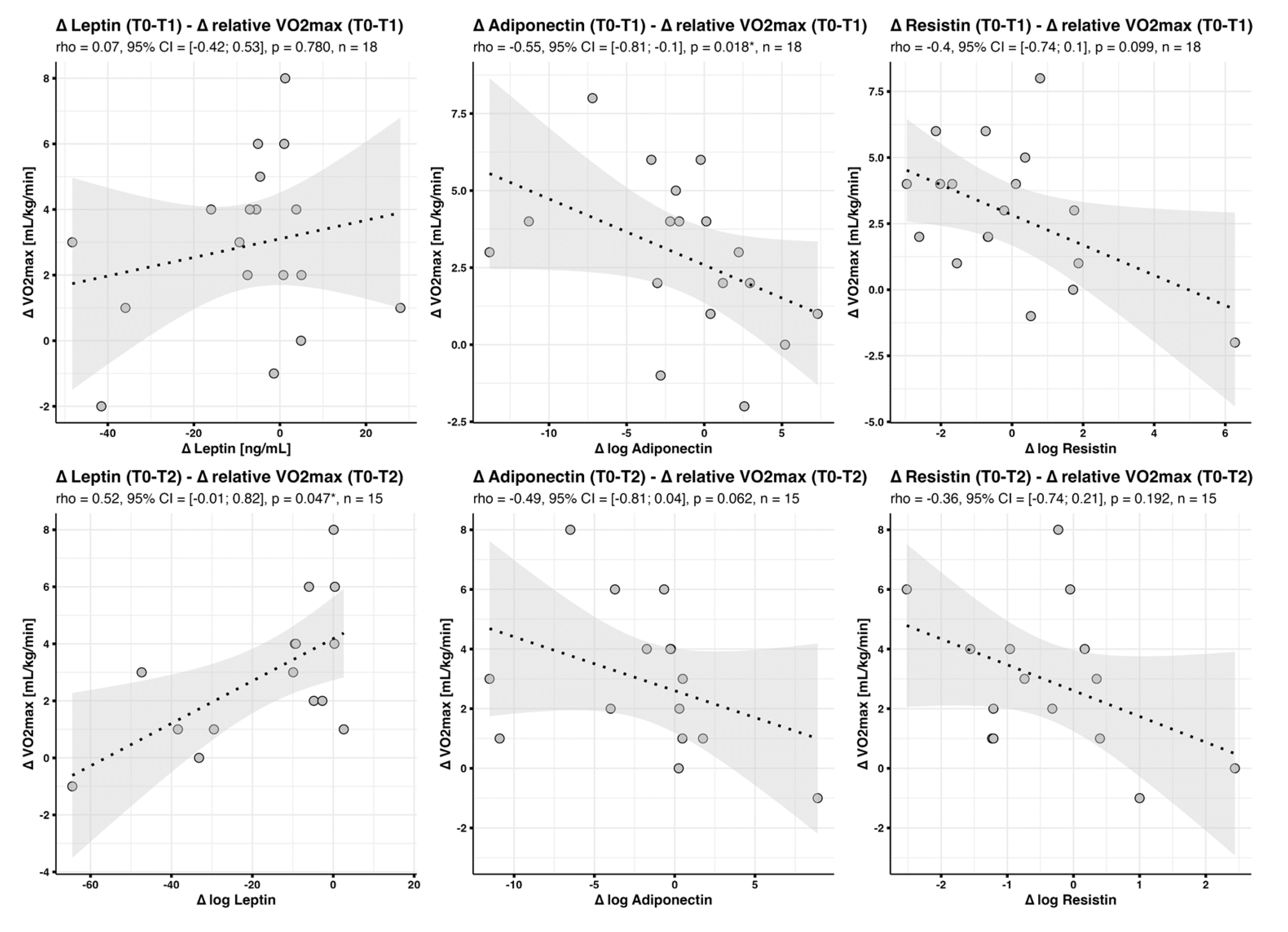
18]). Consistently, in our study population, there was a positive correlation between changes in leptin levels and changes in BMI during the intervention, illustrating that weight loss was immediately associated with decreasing leptin levels. In contrast, there was no negative correlation between intervention-induced changes in
and changes in leptin levels, indicating that the respective effects might be more long term. In general, the observed associations between BMI and training effects might be explained by the facts that (1) our intervention was not controlled for exercise duration and intensity, so that it is well possible that people with a lower BMI might have trained more efficiently and (2) we assessed relative
, so that gains in absolute
might have been underestimated in subjects with a high BMI. The latter hypothesis is supported by the finding that the negative correlations between baseline BMI or leptin levels and changes in absolute
were much weaker when compared to correlations with changes in relative
, and mostly non-significant.
With regard to training practice, the fact that baseline leptin levels, explaining 35% (AIC 82.54)/22% (AIC 138.85) of changes in relative
between T0 and T1 or T0 and T2, were a better predictor of training effects than baseline BMI, explaining 22% (AIC 85.42)/25% (AIC 142.63), respectively, is noteworthy, suggesting that leptin concentrations might be superior to BMI in predicting individual training success, probably due to the fact that they more closely reflect body fat. Not only are adipokines mainly produced in adipose tissue (for review, see [
19]), but they also reflect its distribution. Specifically, subcutaneous adipocytes secrete higher levels of leptin than those of the visceral type (for review, see [
20]). It is possible that, for issues related to mobility, for people with more subcutaneous fat, exercising efficiently might be harder when compared to individuals with a higher proportion of visceral fat, thus leading to lower gains in fitness. In addition, there might be gender- and age-related effects, since fat distribution is different in men and women and also dependent on age [
20], which might be correlated with different training efficiencies in different patient subgroups. In addition, several studies suggest that, independently of fat distribution, there might be gender-specific differences in regard to leptin regulation (for a review, see [
15]). Unfortunately, due to the low number of male subjects in our sample, it was not possible to assess gender-specific differences with regard to correlations between leptin concentrations and training response with sufficient statistical reliability. However, interestingly, a preliminary analysis suggests that a correlation between baseline leptin and training response might be particularly strong in women (
Supplementary Figure S7). This will be analyzed in subsequent studies in more detail.
Moreover, all known methods to assess body fat are either inexact and time consuming, such as skinfold calipometry used in our study, or require very expensive and complex equipment (for a review, see [
21]), warranting the need for novel strategies. It is very likely that leptin might be an even better predictor of training adaptation in subject cohorts with a higher degree of variability with regard to body composition. Consequently, in the future, it might be very promising to study the potential of leptin concentration as a biomarker for individualized training control in more detail, particularly in different patient subgroups. Furthermore, when analyzing larger cohorts, it will also be possible to include patients with higher degrees of multimorbidity, including a broader spectrum of chronic diseases, namely psychiatric conditions such as depression or cancer.
Thus, in the future and specifically in subjects with complex diagnoses and high degrees of multimorbidity, assessing leptin levels prior to starting medical training interventions might be a simple, quick and cost-effective way to predict individual responses to sports programs. Based on this assumption, further studies aimed at designing effective training programs for such potential ‘low responders’ might be carried out. It is likely that for a training regimen to be effective in such subjects, it will have to be more restrictive and closely controlled when compared to regimens for patients predisposed to respond well to exercise.
Taken together, our data suggest that—in addition to BMI—leptin concentrations might be a predictive marker for the effects of an exercise-based lifestyle intervention program on the cardiorespiratory fitness in subjects with multimorbidity. Against this background, it might be an effective strategy to enroll high-BMI and/or high-leptin subjects particularly in highly supervised, intensity-controlled exercise regimens.
Limitations of our study: Our study was a pilot, hypothesis-generating study with only n = 39 subjects. In addition, due to COVID-19-associated contact restrictions, there were no T1 data for subjects recruited in wave #1, thus further decreasing numbers. In addition, our study did not contain a control group. Consequently, data will have to be verified in larger and more heterogeneous cohorts. To this end, a larger clinical trial, the MultiPill-Exercise main study, a randomized controlled trial, was initiated in April 2022.



 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}