
Microscopic Colitis: Pathogenesis and Diagnosis




Abstract
:Simple Summary
Abstract

{kind=link}
{kind=link}
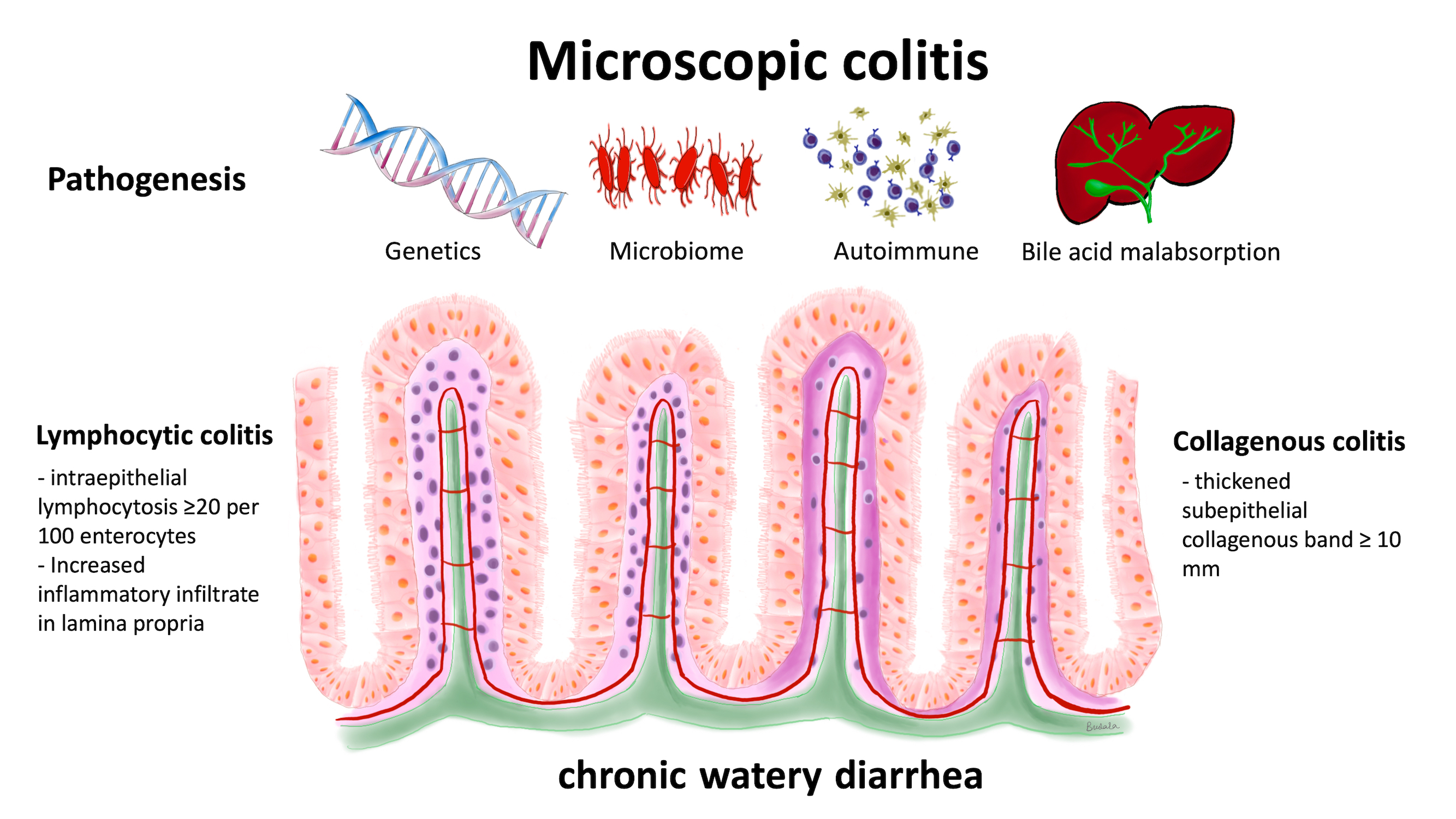
1. Microscopic Colitis
2. Pathogenesis of Microscopic Colitis
2.1. Genetic Predisposition
2.2. Gut Microbiome
2.3. Autoimmune-Related Colonic Injury
2.4. Bile Acid Malabsorption
3. Microscopic Colitis and the Differential Diagnosis of Chronic Diarrhea
4. Standard Diagnosis: Colonoscopy
5. Histological Diagnosis of Microscopic Colitis
6. Laboratory Biomarkers
6.1. Complete Blood Counts (CBC) and Electrolytes
6.2. Erythrocyte Sedimentation Rate (ESR) and C-Reactive Protein (CRP)
6.3. Other Serology Markers
7. Fecal Biomarkers
7.1. Fecal Neutrophils
7.2. Fecal Calprotectin
7.3. Fecal Lactoferrin
7.4. Fecal Myeloperoxidase
7.5. Fecal Eosinophils
7.6. Fecal Mast Cells
8. Management
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Miehlke, S.; Guagnozzi, D.; Zabana, Y.; Tontini, G.E.; Kanstrup Fiehn, A.M.; Wildt, S.; Bohr, J.; Bonderup, O.; Bouma, G.; D’Amato, M.; et al. European guidelines on microscopic colitis: United European Gastroenterology and European Microscopic Colitis Group statements and recommendations. United Eur. Gastroenterol. J. 2021, 9, 13–37. [Google Scholar] [CrossRef] [PubMed]
- Miehlke, S.; Verhaegh, B.; Tontini, G.E.; Madisch, A.; Langner, C.; Münch, A. Microscopic colitis: Pathophysiology and clinical management. Lancet Gastroenterol. Hepatol. 2019, 4, 305–314. [Google Scholar] [CrossRef]
- Lindström, C.G. ‘Collagenous colitis’ with watery diarrhoea—A new entity? Pathol. Eur. 1976, 11, 87–89. [Google Scholar]
- Lazenby, A.J.; Yardley, J.H.; Giardiello, F.M.; Jessurun, J.; Bayless, T.M. Lymphocytic (“microscopic”) colitis: A comparative histopathologic study with particular reference to collagenous colitis. Hum. Pathol. 1989, 20, 18–28. [Google Scholar] [CrossRef] [PubMed]
- Ingle, S.B.; Adgaonkar, B.D.; Ingle, C.R. Microscopic colitis: Common cause of unexplained nonbloody diarrhea. World J. Gastrointest. Pathophysiol. 2014, 5, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Fiehn, A.-M.K.; Miehlke, S.; Aust, D.; Vieth, M.; Bonderup, O.; Fernández-Bañares, F.; Mihaly, E.; Kupcinskas, J.; Madisch, A.; Munck, L.K.; et al. Distribution of histopathological features along the colon in microscopic colitis. Int. J. Color. Dis. 2021, 36, 151–159. [Google Scholar] [CrossRef]
- Nielsen, O.H.; Fernandez-Banares, F.; Sato, T.; Pardi, D.S. Microscopic colitis: Etiopathology, diagnosis, and rational management. eLife 2022, 11, e79397. [Google Scholar] [CrossRef]
- Tanaka, M.; Mazzoleni, G.; Riddell, R.H. Distribution of collagenous colitis: Utility of flexible sigmoidoscopy. Gut 1992, 33, 65. [Google Scholar] [CrossRef] [Green Version]
- Zabana, Y.; Tontini, G.; Hultgren-Hörnquist, E.; Skonieczna-Żydecka, K.; Latella, G.; Østvik, A.E.; Marlicz, W.; D’Amato, M.; Arias, A.; Mielhke, S.; et al. Pathogenesis of Microscopic Colitis: A Systematic Review. J. Crohns Colitis 2022, 16, 143–161. [Google Scholar] [CrossRef]
- Ianiro, G.; Cammarota, G.; Valerio, L.; Annicchiarico, B.E.; Milani, A.; Siciliano, M.; Gasbarrini, A. Microscopic colitis. World J. Gastroenterol. 2012, 18, 6206–6215. [Google Scholar] [CrossRef]
- Nielsen, D.L.; Juhl, C.B.; Chen, I.M.; Kellermann, L.; Nielsen, O.H. Immune checkpoint Inhibitor–Induced diarrhea and Colitis: Incidence and Management. A systematic review and Meta-analysis. Cancer Treat. Rev. 2022, 109, 102440. [Google Scholar] [CrossRef] [PubMed]
- Westerlind, H.; Mellander, M.R.; Bresso, F.; Munch, A.; Bonfiglio, F.; Assadi, G.; Rafter, J.; Hubenthal, M.; Lieb, W.; Kallberg, H.; et al. Dense genotyping of immune-related loci identifies HLA variants associated with increased risk of collagenous colitis. Gut 2017, 66, 421–428. [Google Scholar] [CrossRef]
- Westerlind, H.; Bonfiglio, F.; Mellander, M.R.; Hubenthal, M.; Brynedal, B.; Bjork, J.; Torkvist, L.; Padyukov, L.; Ohlsson, B.; Lofberg, R.; et al. HLA Associations Distinguish Collagenous From Lymphocytic Colitis. Am. J. Gastroenterol. 2016, 111, 1211–1213. [Google Scholar] [CrossRef]
- Green, H.D.; Beaumont, R.N.; Thomas, A.; Hamilton, B.; Wood, A.R.; Sharp, S.; Jones, S.E.; Tyrrell, J.; Walker, G.; Goodhand, J.; et al. Genome-Wide Association Study of Microscopic Colitis in the UK Biobank Confirms Immune-Related Pathogenesis. J. Crohns Colitis 2019, 13, 1578–1582. [Google Scholar] [CrossRef] [Green Version]
- Stahl, E.; Roda, G.; Dobbyn, A.; Hu, J.; Zhang, Z.; Westerlind, H.; Bonfiglio, F.; Raj, T.; Torres, J.; Chen, A.; et al. Collagenous Colitis Is Associated with HLA Signature and Shares Genetic Risks with Other Immune-Mediated Diseases. Gastroenterology 2020, 159, 549–561.e548. [Google Scholar] [CrossRef] [PubMed]
- Jarnerot, G.; Tysk, C.; Bohr, J.; Eriksson, S. Collagenous colitis and fecal stream diversion. Gastroenterology 1995, 109, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Vesoulis, Z.; Lozanski, G.; Loiudice, T. Synchronous occurrence of collagenous colitis and pseudomembranous colitis. Can. J. Gastroenterol. 2000, 14, 353–358. [Google Scholar] [CrossRef] [Green Version]
- Bohr, J.; Nordfelth, R.; Jarnerot, G.; Tysk, C. Yersinia species in collagenous colitis: A serologic study. Scand. J. Gastroenterol. 2002, 37, 711–714. [Google Scholar] [CrossRef]
- Daferera, N.; Kumawat, A.K.; Hultgren-Hornquist, E.; Ignatova, S.; Strom, M.; Munch, A. Fecal stream diversion and mucosal cytokine levels in collagenous colitis: A case report. World J. Gastroenterol. 2015, 21, 6065–6071. [Google Scholar] [CrossRef]
- Rindom Krogsgaard, L.; Kristian Munck, L.; Bytzer, P.; Wildt, S. An altered composition of the microbiome in microscopic colitis is driven towards the composition in healthy controls by treatment with budesonide. Scand. J. Gastroenterol. 2019, 54, 446–452. [Google Scholar] [CrossRef]
- Morgan, D.M.; Cao, Y.; Miller, K.; McGoldrick, J.; Bellavance, D.; Chin, S.M.; Halvorsen, S.; Maxner, B.; Richter, J.M.; Sassi, S.; et al. Microscopic Colitis Is Characterized by Intestinal Dysbiosis. Clin. Gastroenterol. Hepatol. 2020, 18, 984–986. [Google Scholar] [CrossRef]
- Parker, B.J.; Wearsch, P.A.; Veloo, A.C.M.; Rodriguez-Palacios, A. The Genus Alistipes: Gut Bacteria with Emerging Implications to Inflammation, Cancer, and Mental Health. Front. Immunol. 2020, 11, 906. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.; Blakley, I.C.; Fodor, A.A.; Keku, T.O.; Woosley, J.T.; Peery, A.F.; Sandler, R.S. Microbial Associations with Microscopic Colitis. Clin. Transl. Gastroenterol. 2022, 13, e00528. [Google Scholar] [CrossRef] [PubMed]
- Hertz, S.; Durack, J.; Kirk, K.F.; Nielsen, H.L.; Lin, D.L.; Fadrosh, D.; Lynch, K.; Piceno, Y.; Thorlacius-Ussing, O.; Nielsen, H.; et al. Microscopic Colitis Patients Possess a Perturbed and Inflammatory Gut Microbiota. Dig. Dis. Sci. 2022, 67, 2433–2443. [Google Scholar] [CrossRef]
- Gustafsson, R.J.; Ohlsson, B.; Benoni, C.; Jeppsson, B.; Olsson, C. Mucosa-associated bacteria in two middle-aged women diagnosed with collagenous colitis. World. J. Gastroenterol. 2012, 18, 1628–1634. [Google Scholar] [CrossRef]
- Wang, M.; Ahrne, S.; Jeppsson, B.; Molin, G. Comparison of bacterial diversity along the human intestinal tract by direct cloning and sequencing of 16S rRNA genes. FEMS Microbiol. Ecol. 2005, 54, 219–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayashi, H.; Sakamoto, M.; Benno, Y. Phylogenetic analysis of the human gut microbiota using 16S rDNA clone libraries and strictly anaerobic culture-based methods. Microbiol. Immunol. 2002, 46, 535–548. [Google Scholar] [CrossRef]
- Suau, A.; Bonnet, R.; Sutren, M.; Godon, J.J.; Gibson, G.R.; Collins, M.D.; Dore, J. Direct analysis of genes encoding 16S rRNA from complex communities reveals many novel molecular species within the human gut. Appl. Environ. Microbiol. 1999, 65, 4799–4807. [Google Scholar] [CrossRef] [Green Version]
- Finegold, S.M.; Song, Y.; Liu, C.; Hecht, D.W.; Summanen, P.; Kononen, E.; Allen, S.D. Clostridium clostridioforme: A mixture of three clinically important species. Eur. J. Clin. Microbiol. Infect. Dis. 2005, 24, 319–324. [Google Scholar] [CrossRef]
- Derrien, M.; Vaughan, E.E.; Plugge, C.M.; de Vos, W.M. Akkermansia muciniphila gen. nov., sp. nov., a human intestinal mucin-degrading bacterium. Int. J. Syst. Evol. Microbiol. 2004, 54 Pt 5, 1469–1476. [Google Scholar] [CrossRef] [Green Version]
- Fischer, H.; Holst, E.; Karlsson, F.; Benoni, C.; Toth, E.; Olesen, M.; Lindén, M.; Sjöberg, K. Altered microbiota in microscopic colitis. Gut 2015, 64, 1185–1186. [Google Scholar] [CrossRef] [Green Version]
- Millien, V.; Rosen, D.; Hou, J.; Shah, R. Proinflammatory Sulfur-Reducing Bacteria Are More Abundant in Colonic Biopsies of Patients with Microscopic Colitis Compared to Healthy Controls. Dig. Dis. Sci. 2019, 64, 432–438. [Google Scholar] [CrossRef]
- Wildt, S.; Munck, L.K.; Winther-Jensen, M.; Jess, T.; Nyboe Andersen, N. Autoimmune diseases in microscopic colitis: A Danish nationwide case-control study. Aliment. Pharmacol. Ther. 2021, 54, 1454–1462. [Google Scholar] [CrossRef]
- Fedor, I.; Zold, E.; Barta, Z. Microscopic colitis: Controversies in clinical symptoms and autoimmune comorbidities. Ann. Med. 2021, 53, 1279–1284. [Google Scholar] [CrossRef]
- Göranzon, C.; Kumawat, A.K.; Hultgren-Hörnqvist, E.; Tysk, C.; Eriksson, S.; Bohr, J.; Nyhlin, N. Immunohistochemical characterization of lymphocytes in microscopic colitis. J Crohns Colitis 2013, 7, e434–e442. [Google Scholar] [CrossRef] [Green Version]
- Sandler, R.S.; Hansen, J.J.; Peery, A.F.; Woosley, J.T.; Galanko, J.A.; Keku, T.O. Intraepithelial and Lamina Propria Lymphocytes Do Not Correlate with Symptoms or Exposures in Microscopic Colitis. Clin. Transl. Gastroenterol. 2022, 13, e00467. [Google Scholar] [CrossRef]
- Kuwada, T.; Shiokawa, M.; Kodama, Y.; Ota, S.; Kakiuchi, N.; Nannya, Y.; Yamazaki, H.; Yoshida, H.; Nakamura, T.; Matsumoto, S.; et al. Identification of an Anti–Integrin αvβ6 Autoantibody in Patients with Ulcerative Colitis. Gastroenterology 2021, 160, 2383–2394.e2321. [Google Scholar] [CrossRef]
- Ticho, A.L.; Malhotra, P.; Dudeja, P.K.; Gill, R.K.; Alrefai, W.A. Bile Acid Receptors and Gastrointestinal Functions. Liver Res. 2019, 3, 31–39. [Google Scholar] [CrossRef]
- Pavlidis, P.; Powell, N.; Vincent, R.P.; Ehrlich, D.; Bjarnason, I.; Hayee, B. Systematic review: Bile acids and intestinal inflammation-luminal aggressors or regulators of mucosal defence? Aliment. Pharmacol. Ther. 2015, 42, 802–817. [Google Scholar] [CrossRef]
- Di Vincenzo, F.; Puca, P.; Lopetuso, L.R.; Petito, V.; Masi, L.; Bartocci, B.; Murgiano, M.; De Felice, M.; Petronio, L.; Gasbarrini, A.; et al. Bile Acid-Related Regulation of Mucosal Inflammation and Intestinal Motility: From Pathogenesis to Therapeutic Application in IBD and Microscopic Colitis. Nutrients 2022, 14, 2664. [Google Scholar] [CrossRef]
- Marteau, P.; Lavergne-Slove, A.; Lemann, M.; Bouhnik, Y.; Bertheau, P.; Becheur, H.; Galian, A.; Rambaud, J.C. Primary ileal villous atrophy is often associated with microscopic colitis. Gut 1997, 41, 561–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Germain, E.; Roblin, X.; Colle, P.E.; Barnoud, R.; Faucheron, J.L.; Bonaz, B. Primary ileal villous atrophy associated with microscopic colitis. J. Gastroenterol. Hepatol. 2005, 20, 1800–1801. [Google Scholar] [CrossRef] [PubMed]
- Sapp, H.; Ithamukkala, S.; Brien, T.P.; Ayata, G.; Shaz, B.; Dorfman, D.M.; Wang, H.H.; Antonioli, D.A.; Farraye, F.A.; Odze, R.D. The terminal ileum is affected in patients with lymphocytic or collagenous colitis. Am. J. Surg. Pathol. 2002, 26, 1484–1492. [Google Scholar] [CrossRef]
- Padmanabhan, V.; Callas, P.W.; Li, S.C.; Trainer, T.D. Histopathological features of the terminal ileum in lymphocytic and collagenous colitis: A study of 32 cases and review of literature. Mod. Pathol. 2003, 16, 115–119. [Google Scholar] [CrossRef] [Green Version]
- Ung, K.A.; Gillberg, R.; Kilander, A.; Abrahamsson, H. Role of bile acids and bile acid binding agents in patients with collagenous colitis. Gut 2000, 46, 170–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ung, K.A.; Kilander, A.; Willén, R.; Abrahamsson, H. Role of bile acids in lymphocytic colitis. Hepatogastroenterology 2002, 49, 432–437. [Google Scholar]
- Bohr, J.; Tysk, C.; Eriksson, S.; Abrahamsson, H.; Järnerot, G. Collagenous colitis: A retrospective study of clinical presentation and treatment in 163 patients. Gut 1996, 39, 846–851. [Google Scholar] [CrossRef] [Green Version]
- Northcutt, M.J.; Gentile, N.M.; Goldstein, J.L.; Yen, E.F. Bile Acid Sequestrant Therapy in Microscopic Colitis. J. Clin. Gastroenterol. 2022, 56, 161–165. [Google Scholar] [CrossRef]
- Gurbuz, Y.; Senturk, O.; Muezzinoğlu, B. Postcholecystectomy Microsc. Colitis: Is Bile Acid Malabsorption A Triggering Factor? Am. J. Gastroenterol. 2001, 96, 1655–1656. [Google Scholar] [CrossRef]
- Laing, A.W.; Pardi, D.S.; Loftus, E.V., Jr.; Smyrk, T.C.; Kammer, P.P.; Tremaine, W.J.; Schleck, C.D.; Harmsen, W.S.; Zinsmeister, A.R.; Melton, L.J., 3rd; et al. Microscopic colitis is not associated with cholecystectomy or appendectomy. Inflamm. Bowel Dis. 2006, 12, 708–711. [Google Scholar] [CrossRef]
- Juckett, G.; Trivedi, R. Evaluation of chronic diarrhea. Am. Fam. Physician 2011, 84, 1119–1126. [Google Scholar] [PubMed]
- Dellon, E.S.; Ringel, Y. Treatment of functional diarrhea. Curr. Treat. Options Gastroenterol. 2006, 9, 331–342. [Google Scholar] [CrossRef] [PubMed]
- Burgers, K.; Lindberg, B.; Bevis, Z.J. Chronic Diarrhea in Adults: Evaluation and Differential Diagnosis. Am. Fam. Physician 2020, 101, 472–480. [Google Scholar]
- Smalley, W.; Falck-Ytter, C.; Carrasco-Labra, A.; Wani, S.; Lytvyn, L.; Falck-Ytter, Y. AGA Clinical Practice Guidelines on the Laboratory Evaluation of Functional Diarrhea and Diarrhea-Predominant Irritable Bowel Syndrome in Adults (IBS-D). Gastroenterology 2019, 157, 851–854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arasaradnam, R.P.; Brown, S.; Forbes, A.; Fox, M.R.; Hungin, P.; Kelman, L.; Major, G.; O’Connor, M.; Sanders, D.S.; Sinha, R.; et al. Guidelines for the investigation of chronic diarrhoea in adults: British Society of Gastroenterology, 3rd edition. Gut 2018, 67, 1380–1399. [Google Scholar] [CrossRef] [Green Version]
- Lacy, B.E.; Patel, N.K. Rome Criteria and a Diagnostic Approach to Irritable Bowel Syndrome. J. Clin. Med. 2017, 6, 99. [Google Scholar] [CrossRef] [Green Version]
- Protic, M.; Jojic, N.; Bojic, D.; Milutinovic, S.; Necic, D.; Bojic, B.; Svorcan, P.; Krstic, M.; Popovic, O. Mechanism of diarrhea in microscopic colitis. World J. Gastroenterol. 2005, 11, 5535–5539. [Google Scholar] [CrossRef]
- Tong, J.; Zheng, Q.; Zhang, C.; Lo, R.; Shen, J.; Ran, Z. Incidence, prevalence, and temporal trends of microscopic colitis: A systematic review and meta-analysis. Am. J. Gastroenterol. 2015, 110, 265–276, quiz 277. [Google Scholar] [CrossRef]
- Kane, J.S.; Rotimi, O.; Ford, A.C. Macroscopic findings, incidence and characteristics of microscopic colitis in a large cohort of patients from the United Kingdom. Scand. J. Gastroenterol. 2017, 52, 988–994. [Google Scholar] [CrossRef]
- Sharaf, R.N.; Shergill, A.K.; Odze, R.D.; Krinsky, M.L.; Fukami, N.; Jain, R.; Appalaneni, V.; Anderson, M.A.; Ben-Menachem, T.; Chandrasekhara, V.; et al. Endoscopic mucosal tissue sampling. Gastrointest. Endosc. 2013, 78, 216–224. [Google Scholar] [CrossRef]
- Malik, A.; Nadeem, M.; Javaid, S.; Malik, M.I.; Enofe, I.; Abegunde, A.T. Estimating the optimum number of colon biopsies for diagnosing microscopic colitis: A systematic review. Eur. J. Gastroenterol. Hepatol. 2022, 34, 733–738. [Google Scholar] [CrossRef] [PubMed]
- Chapman, T.P.; Macfaul, G.; Abraham, A. Diagnosing microscopic colitis: Is flexible sigmoidoscopy a reliable alternative to colonoscopy? Clin. Gastroenterol. Hepatol. 2015, 13, 618. [Google Scholar] [CrossRef] [PubMed]
- Virine, B.; Chande, N.; Driman, D.K. Biopsies From Ascending and Descending Colon Are Sufficient for Diagnosis of Microscopic Colitis. Clin. Gastroenterol. Hepatol. 2020, 18, 2003–2009. [Google Scholar] [CrossRef] [PubMed]
- Rutter, C.M.; Johnson, E.; Miglioretti, D.L.; Mandelson, M.T.; Inadomi, J.; Buist, D.S. Adverse events after screening and follow-up colonoscopy. Cancer Causes Control 2012, 23, 289–296. [Google Scholar] [CrossRef] [Green Version]
- Boland, K.; Nguyen, G.C. Microscopic Colitis: A Review of Collagenous and Lymphocytic Colitis. Gastroenterol. Hepatol. 2017, 13, 671–677. [Google Scholar]
- Abboud, R.; Tremaine, W.; Pardi, D. The Association of Serologic Inflammatory Markers with Microscopic Colitis Disease Activity. Am. J. Gastroenterol. 2011, 106, S164–S165. Available online: https://journals.lww.com/ajg/Fulltext/2011/10002/The_Association_of_Serologic_Inflammatory_Markers.420.aspx (accessed on 8 March 2023). [CrossRef]
- Larsson, J.K.; Roth, B.; Ohlsson, B.; Sjöberg, K. Lack of autoantibodies against collagen and related proteins in collagenous colitis. BMC Immunol. 2022, 23, 29. [Google Scholar]
- Holstein, A.; Burmeister, J.; Plaschke, A.; Rosemeier, D.; Widjaja, A.; Egberts, E.H. Autoantibody profiles in microscopic colitis. J. Gastroenterol. Hepatol. 2006, 21, 1016–1020. [Google Scholar] [CrossRef]
- Roth, B.; Gustafsson, R.J.; Ohlsson, B. Auto-antibodies and their association with clinical findings in women diagnosed with microscopic colitis. PLoS ONE 2013, 8, e66088. [Google Scholar] [CrossRef]
- Pisani, L.F.; Tontini, G.E.; Marinoni, B.; Villanacci, V.; Bruni, B.; Vecchi, M.; Pastorelli, L. Biomarkers and microscopic colitis: An unmet need in clinical practice. Front. Med. 2017, 4, 54. [Google Scholar] [CrossRef] [Green Version]
- Kingham, J.G.; Levison, D.A.; Morson, B.C.; Dawson, A.M. Collagenous colitis. Gut 1986, 27, 570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Topel, G.; Cakir, E.; Aydin, I.; Dilek, F.H.; Sari, A.A. Analysis of Clinical and Histopathological Findings in Microscopic Colitis. Türk Patoloji Derg. 2022, 38, 275–283. [Google Scholar] [CrossRef]
- Fournier, B.M.; Parkos, C.A. The role of neutrophils during intestinal inflammation. Mucosal Immunol. 2012, 5, 354–366. [Google Scholar] [CrossRef] [Green Version]
- Maloy, K.J.; Powrie, F. Intestinal homeostasis and its breakdown in inflammatory bowel disease. Nature 2011, 474, 298–306. [Google Scholar] [CrossRef] [PubMed]
- Bjarnason, I. The Use of Fecal Calprotectin in Inflammatory Bowel Disease. Gastroenterol. Hepatol. 2017, 13, 53–56. [Google Scholar]
- Ricciuto, A.; Griffiths, A.M. Clinical value of fecal calprotectin. Crit. Rev. Clin. Lab. Sci. 2019, 56, 307–320. [Google Scholar] [CrossRef]
- Ayling, R.M.; Kok, K. Chapter Six—Fecal Calprotectin. In Advances in Clinical Chemistry; Makowski, G.S., Ed.; Elsevier: Amsterdam, The Netherlands, 2018; Volume 87, pp. 161–190. [Google Scholar]
- Mosli, M.H.; Zou, G.; Garg, S.K.; Feagan, S.G.; MacDonald, J.K.; Chande, N.; Sandborn, W.J.; Feagan, B.G. C-Reactive Protein, Fecal Calprotectin, and Stool Lactoferrin for Detection of Endoscopic Activity in Symptomatic Inflammatory Bowel Disease Patients: A Systematic Review and Meta-Analysis. Am. J. Gastroenterol. 2015, 110, 802–819, quiz 820. [Google Scholar] [CrossRef]
- Batista, L.; Ruiz, L.; Ferrer, C.; Zabana, Y.; Aceituno, M.; Arau, B.; Andújar, X.; Esteve, M.; Fernández-Bañares, F. Usefulness of fecal calprotectin as a biomarker of microscopic colitis in a cohort of patients with chronic watery diarrhoea of functional characteristics. Dig. Liver Dis. 2019, 51, 1646–1651. [Google Scholar] [CrossRef]
- Lyutakov, I.; Nakov, R.; Valkov, H.; Vatcheva-Dobrevska, R.; Vladimirov, B.; Penchev, P. Serum Levels of Fibroblast Growth Factor 19 Correlate with the Severity of Diarrhea and Independently from Intestinal Inflammation in Patients with Inflammatory Bowel Disease or Microscopic Colitis. Turk. J. Gastroenterol. 2021, 32, 374–381. [Google Scholar] [CrossRef]
- von Arnim, U.; Wex, T.; Ganzert, C.; Schulz, C.; Malfertheiner, P. Fecal calprotectin: A marker for clinical differentiation of microscopic colitis and irritable bowel syndrome. Clin. Exp. Gastroenterol. 2016, 9, 97–103. [Google Scholar] [CrossRef] [Green Version]
- Wildt, S.; Nordgaard-Lassen, I.; Bendtsen, F.; Rumessen, J.J. Metabolic and inflammatory faecal markers in collagenous colitis. Eur. J. Gastroenterol. Hepatol. 2007, 19, 567–574. [Google Scholar] [CrossRef] [PubMed]
- Levay, P.F.; Viljoen, M. Lactoferrin: A general review. Haematologica 1995, 80, 252–267. [Google Scholar] [PubMed]
- Buderus, S.; Boone, J.H.; Lentze, M.J. Fecal Lactoferrin: Reliable Biomarker for Intestinal Inflammation in Pediatric IBD. Gastroenterol. Res. Pract. 2015, 2015, 578527. [Google Scholar] [CrossRef]
- Kane, S.V.; Sandborn, W.J.; Rufo, P.A.; Zholudev, A.; Boone, J.; Lyerly, D.; Camilleri, M.; Hanauer, S.B. Fecal lactoferrin is a sensitive and specific marker in identifying intestinal inflammation. Am. J. Gastroenterol. 2003, 98, 1309–1314. [Google Scholar] [CrossRef] [PubMed]
- Fine, K.D.; Ogunji, F.; George, J.; Niehaus, M.D.; Guerrant, R.L. Utility of a rapid fecal latex agglutination test detecting the neutrophil protein, lactoferrin, for diagnosing inflammatory causes of chronic diarrhea. Am. J. Gastroenterol. 1998, 93, 1300–1305. [Google Scholar] [CrossRef] [PubMed]
- Burri, E.; Manz, M.; Rothen, C.; Rossi, L.; Beglinger, C.; Lehmann, F.S. Monoclonal antibody testing for fecal calprotectin is superior to polyclonal testing of fecal calprotectin and lactoferrin to identify organic intestinal disease in patients with abdominal discomfort. Clin. Chim. Acta 2013, 416, 41–47. [Google Scholar] [CrossRef]
- Summerton, C.B.; Longlands, M.G.; Wiener, K.; Shreeve, D.R. Faecal calprotectin: A marker of inflammation throughout the intestinal tract. Eur. J. Gastroenterol. Hepatol. 2002, 14, 841–845. [Google Scholar] [CrossRef]
- Hansberry, D.R.; Shah, K.; Agarwal, P.; Agarwal, N. Fecal Myeloperoxidase as a Biomarker for Inflammatory Bowel Disease. Cureus 2017, 9, e1004. [Google Scholar] [CrossRef] [Green Version]
- Wagner, M.; Sjöberg, K.; Vigren, L.; Olesen, M.; Benoni, C.; Toth, E.; Carlson, M. Elevated fecal levels of eosinophil granule proteins predict collagenous colitis in patients referred to colonoscopy due to chronic non-bloody diarrhea. Scand. J. Gastroenterol. 2016, 51, 835–841. [Google Scholar] [CrossRef]
- Lettesjö, H.; Hansson, T.; Peterson, C.; Ung, K.-A.; Ringström, G.; Abrahamsson, H.; Simrén, M. Detection of inflammatory markers in stools from patients with irritable bowel syndrome and collagenous colitis. Scand. J. Gastroenterol. 2006, 41, 54–59. [Google Scholar] [CrossRef]
- Wechsler, M.E.; Munitz, A.; Ackerman, S.J.; Drake, M.G.; Jackson, D.J.; Wardlaw, A.J.; Dougan, S.K.; Berdnikovs, S.; Schleich, F.; Matucci, A.; et al. Eosinophils in Health and Disease: A State-of-the-Art Review. Mayo Clin. Proc. 2021, 96, 2694–2707. [Google Scholar] [CrossRef] [PubMed]
- Al-Haddad, S.; Riddell, R.H. The role of eosinophils in inflammatory bowel disease. Gut 2005, 54, 1674–1675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rothenberg, M.E.; Mishra, A.; Brandt, E.B.; Hogan, S.P. Gastrointestinal eosinophils. Immunol. Rev. 2001, 179, 139–155. [Google Scholar] [CrossRef] [PubMed]
- Lampinen, M.; Rönnblom, A.; Amin, K.; Kristjansson, G.; Rorsman, F.; Sangfelt, P.; Säfsten, B.; Wagner, M.; Wanders, A.; Winqvist, O.; et al. Eosinophil granulocytes are activated during the remission phase of ulcerative colitis. Gut 2005, 54, 1714–1720. [Google Scholar] [CrossRef] [PubMed]
- Wagner, M.; Lampinen, M.; Sangfelt, P.; Agnarsdottir, M.; Carlson, M. Budesonide treatment of patients with collagenous colitis restores normal eosinophil and T-cell activity in the colon. Inflamm. Bowel Dis. 2010, 16, 1118–1126. [Google Scholar] [CrossRef]
- Sethi, A.; Jain, D.; Roland, B.C.; Kinzel, J.; Gibson, J.; Schrader, R.; Hanson, J.A. Performing colonic mast cell counts in patients with chronic diarrhea of unknown etiology has limited diagnostic use. Arch. Pathol. Lab. Med. 2015, 139, 225–232. [Google Scholar] [CrossRef]
- Doyle, L.A.; Sepehr, G.J.; Hamilton, M.J.; Akin, C.; Castells, M.C.; Hornick, J.L. A clinicopathologic study of 24 cases of systemic mastocytosis involving the gastrointestinal tract and assessment of mucosal mast cell density in irritable bowel syndrome and asymptomatic patients. Am. J. Surg. Pathol. 2014, 38, 832–843. [Google Scholar] [CrossRef] [Green Version]
- Chi, Z.; Xu, J.; Saxena, R. Increased Mast Cell Counts and Degranulation in Microscopic Colitis. Gastroenterol. Res. Pract. 2020, 2020, 9089027. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Songtanin, B.; Chen, J.N.; Nugent, K. Microscopic Colitis: Pathogenesis and Diagnosis. J. Clin. Med. 2023, 12, 4442. https://doi.org/10.3390/jcm12134442
Songtanin B, Chen JN, Nugent K. Microscopic Colitis: Pathogenesis and Diagnosis. Journal of Clinical Medicine. 2023; 12(13):4442. https://doi.org/10.3390/jcm12134442
Chicago/Turabian StyleSongtanin, Busara, Jason N. Chen, and Kenneth Nugent. 2023. "Microscopic Colitis: Pathogenesis and Diagnosis" Journal of Clinical Medicine 12, no. 13: 4442. https://doi.org/10.3390/jcm12134442
APA StyleSongtanin, B., Chen, J. N., & Nugent, K. (2023). Microscopic Colitis: Pathogenesis and Diagnosis. Journal of Clinical Medicine, 12(13), 4442. https://doi.org/10.3390/jcm12134442