
Chromosome Y Haplogroup R Was Associated with the Risk of Premature Myocardial Infarction with ST-Elevation: Data from the CholeSTEMI Registry

 , , ,
, , ,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Control Cohort
2.3. Genetic Testing
2.4. Statistical Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2019, 74, 1376–1414. [Google Scholar] [CrossRef]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, S.; Hawken, S.; Ounpuu, S.; Dans, T.; Avezum, A.; Lanas, F.; McQueen, M.; Budaj, A.; Pais, P.; Varigos, J.; et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-control study. Lancet 2004, 364, 937–952. [Google Scholar] [CrossRef]
- McPherson, R.; Tybjaerg-Hansen, A. Genetics of Coronary Artery Disease. Circ. Res. 2016, 118, 564–578. [Google Scholar] [CrossRef] [PubMed]
- Lorca, R.; Aparicio, A.; Cuesta-Llavona, E.; Pascual, I.; Junco, A.; Hevia, S.; Villazón, F.; Hernandez-Vaquero, D.; Rodríguez Reguero, J.J.; Moris, C.; et al. Familial Hypercholesterolemia in Premature Acute Coronary Syndrome. Insights from CholeSTEMI Registry. J. Clin. Med. 2020, 9, 3489. [Google Scholar] [CrossRef] [PubMed]
- Jobling, M.A.; Tyler-Smith, C. The human Y chromosome: An evolutionary marker comes of age. Nat. Rev. Genet. 2003, 4, 598–612. [Google Scholar] [CrossRef]
- Underhill, P.A.; Shen, P.; Lin, A.A.; Jin, L.; Passarino, G.; Yang, W.H.; Kauffman, E.; Bonné-Tamir, B.; Bertranpetit, J.; Francalacci, P.; et al. Y chromosome sequence variation and the history of human populations. Nat. Genet. 2000, 26, 358–361. [Google Scholar] [CrossRef]
- Underhill, P.A.; Myres, N.M.; Rootsi, S.; Metspalu, M.; Zhivotovsky, L.A.; King, R.J.; Lin, A.A.; Chow, C.-E.T.; Semino, O.; Battaglia, V.; et al. Separating the post-Glacial coancestry of European and Asian Y chromosomes within haplogroup R1a. Eur. J. Hum. Genet. 2010, 18, 479–484. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Parikh, H.; Jia, J.; Myers, T.; Yeager, M.; Jacobs, K.B.; Hutchinson, A.; Burdett, L.; Ghosh, A.; Thun, M.J.; et al. Y chromosome haplogroups and prostate cancer in populations of European and Ashkenazi Jewish ancestry. Hum. Genet. 2012, 131, 1173–1185. [Google Scholar] [CrossRef] [Green Version]
- Charchar, F.J.; Bloomer, L.D.; Barnes, T.A.; Cowley, M.J.; Nelson, C.P.; Wang, Y.; Denniff, M.; Debiec, R.; Christofidou, P.; Nankervis, S.; et al. Inheritance of coronary artery disease in men: An analysis of the role of the Y chromosome. Lancet 2012, 379, 915–922. [Google Scholar] [CrossRef] [Green Version]
- Bloomer, L.D.S.; Nelson, C.P.; Denniff, M.; Christofidou, P.; Debiec, R.; Thompson, J.; Zukowska-Szczechowska, E.; Samani, N.J.; Charchar, F.J.; Tomaszewski, M. Coronary artery disease predisposing haplogroup I of the Y chromosome, aggression and sex steroids—Genetic association analysis. Atherosclerosis 2014, 233, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Lorca, R.; Aparicio, A.; Gómez, J.; Álvarez-Velasco, R.; Pascual, I.; Avanzas, P.; González-Urbistondo, F.; Alen, A.; Vázquez-Coto, D.; González-Fernández, M.; et al. Mitochondrial Heteroplasmy as a Marker for Premature Coronary Artery Disease: Analysis of the Poly-C Tract of the Control Region Sequence. JCM 2023, 12, 2133. [Google Scholar] [CrossRef] [PubMed]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D.; ESC Scientific Document Group. Fourth universal definition of myocardial infarction (2018). Eur. Heart J. 2019, 40, 237–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collet, J.-P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef]
- Williams, R.R.; Hunt, S.C.; Schumacher, M.C.; Hegele, R.A.; Leppert, M.F.; Ludwig, E.H.; Hopkins, P.N. Diagnosing heterozygous familial hypercholesterolemia using new practical criteria validated by molecular genetics. Am. J. Cardiol. 1993, 72, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Defesche, J.C.; Lansberg, P.J.; Umans-Eckenhausen, M.A.W.; Kastelein, J.J.P. Advanced method for the identification of patients with inherited hypercholesterolemia. Semin. Vasc. Med. 2004, 4, 59–65. [Google Scholar] [CrossRef]
- Riobello, C.; Gómez, J.; Gil-Peña, H.; Tranche, S.; Reguero, J.R.; de la Hera, J.M.; Delgado, E.; Calvo, D.; Morís, C.; Santos, F.; et al. KCNQ1 gene variants in the risk for type 2 diabetes and impaired renal function in the Spanish Renastur cohort. Mol. Cell. Endocrinol. 2016, 427, 86–91. [Google Scholar] [CrossRef]
- Vinkhuyzen, A.A.E.; Wray, N.R.; Yang, J.; Goddard, M.E.; Visscher, P.M. Estimation and Partition of Heritability in Human Populations Using Whole-Genome Analysis Methods. Annu. Rev. Genet. 2013, 47, 75–95. [Google Scholar] [CrossRef] [Green Version]
- Zdravkovic, S.; Wienke, A.; Pedersen, N.L.; Marenberg, M.E.; Yashin, A.I.; De Faire, U. Heritability of death from coronary heart disease: A 36-year follow-up of 20,966 Swedish twins. J. Intern. Med. 2002, 252, 247–254. [Google Scholar] [CrossRef]
- Timmers, P.R.H.J.; Wilson, J.F. Limited Effect of Y Chromosome Variation on Coronary Artery Disease and Mortality in UK Biobank-Brief Report. Arterioscler. Thromb. Vasc. Biol. 2022, 42, 1198–1206. [Google Scholar] [CrossRef]
- Eales, J.M.; Maan, A.A.; Xu, X.; Michoel, T.; Hallast, P.; Batini, C.; Zadik, D.; Prestes, P.R.; Molina, E.; Denniff, M.; et al. Human Y Chromosome Exerts Pleiotropic Effects on Susceptibility to Atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 2019, 39, 2386–2401. [Google Scholar] [CrossRef]
- Newby, A.C. Metalloproteinases promote plaque rupture and myocardial infarction: A persuasive concept waiting for clinical translation. Matrix Biol. 2015, 44–46, 157–166. [Google Scholar] [CrossRef]
- Ghattas, A.; Griffiths, H.R.; Devitt, A.; Lip, G.Y.H.; Shantsila, E. Monocytes in Coronary Artery Disease and Atherosclerosis. J. Am. Coll. Cardiol. 2013, 62, 1541–1551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borén, J.; Williams, K.J. The central role of arterial retention of cholesterol-rich apolipoprotein-B-containing lipoproteins in the pathogenesis of atherosclerosis: A triumph of simplicity. Curr. Opin. Lipidol. 2016, 27, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Evans, D.J.W.; Jackman, L.E.; Chamberlain, J.; Crosdale, D.J.; Judge, H.M.; Jetha, K.; Norman, K.E.; Francis, S.E.; Storey, R.F. Platelet P2Y12 Receptor Influences the Vessel Wall Response to Arterial Injury and Thrombosis. Circulation 2009, 119, 116–122. [Google Scholar] [CrossRef] [Green Version]
- Adams, S.M.; Bosch, E.; Balaresque, P.L.; Ballereau, S.J.; Lee, A.C.; Arroyo, E.; López-Parra, A.M.; Aler, M.; Grifo, M.S.G.; Brion, M.; et al. The genetic legacy of religious diversity and intolerance: Paternal lineages of Christians, Jews, and Muslims in the Iberian Peninsula. Am. J. Hum. Genet. 2008, 83, 725–736. [Google Scholar] [CrossRef] [Green Version]
- Bell, K.J.L.; Loy, C.; Cust, A.E.; Teixeira-Pinto, A. Mendelian Randomization in Cardiovascular Research: Establishing Causality When There Are Unmeasured Confounders. Circ. Cardiovasc. Qual. Outcomes 2021, 14, e005623. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| NUCLEOTIDE Y Position | SNP | HAPLOGROUP | ASSAY | EUR | FREQUENCY |
|---|---|---|---|---|---|
| 13407103 | rs2032658 G/A | R | C___2307221_1Y | G (0.58) | 0.0016 |
| 12914512 | rs2032624 C/A | R1 | C___2292796_20 | C (0.58) | 0.0016 |
| 20577481 | rs9786153 T/C | R1B | C__29812961_10 | C (0.53) | <0.0001 |
| 2789135 | rs2534636 C/T | R1A | C__26236081_10 | T (0.05) | 0.0113 |
| 14436668 | rs113623003 G/A | I | C_153784812_10 | A (0.14) | 0.0085 |
| 20587967 | rs13447352 A/C | J | C__33589462_10 | C (0.11) | 0.1168 |
| 19617112 | rs9306841 C/G | E | C__29796914_10 | G (0.03) | 0.0008 |
| 12915617 | rs2032636 G/T | G | C___2292797_20 | T (0.06) | 0.0996 |
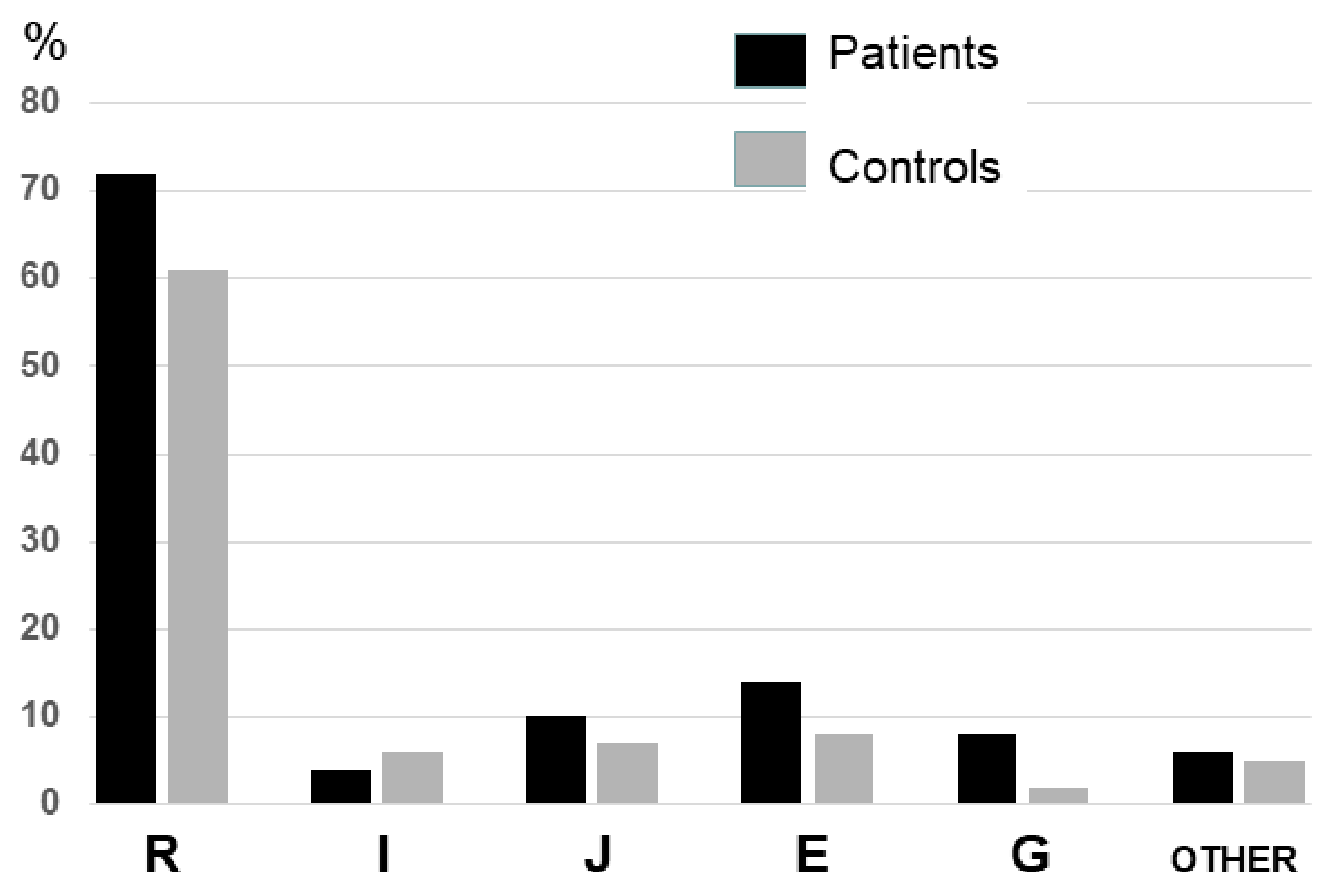
| Haplogroup | Control Cohort N = 200 | Patients Cohort N = 122 | p |
|---|---|---|---|
| R | 122 (0.61) | 88 (0.72) | 0.04 * |
| R1 | 118 (0.59) | 88 (0.72) | 0.02 * |
| R1B | 118 (0.59) | 88 (0.72) | 0.02 * |
| R1A | 4 (0.02) | 0 | 0.12 |
| I | 8 (0.04) | 7 (0.06) | 0.47 |
| J | 20 (0.10) | 8 (0.07) | 0.28 |
| E | 28 (0.14) | 10 (0.08) | 0.12 |
| G | 16 (0.08) | 3 (0.02) | 0.04 * |
| Other | 6 (0.03) | 6 (0.05) | 0.38 |
| 122 Male Patients with Premature STEMI | |
|---|---|
| Mean age at STEMI | 47.11 (±8.99) |
| Cardiovascular risk factors | |
| Previous/current smoker | 95 (86.07%) |
| High blood pressure | 34 (27.87%) |
| Diabetes mellitus | 14 (11.48%) |
| Dyslipidemia | 45 (36.89%) |
| Family history of premature CAD | 30 (24.59%) |
| Y Chromosome Haplogroups | No DM (108) | DM (14) | No HTN (88) | HTN (34) | No DL (77) | DL (45) | Non-Smokers (26) | Smokers (96) | No FH of PCAD (92) | FH of PCAD (30) |
|---|---|---|---|---|---|---|---|---|---|---|
| R | 73.2% | 64.3% | 70.5% | 76.5% | 74% | 68.9% | 76.9% | 70.8% | 71.7% | 73.3% |
| E | 9.3% | - | 10.2% | 2.9% | 7.8% | 8.9% | 11.5% | 7.3% | 9.8% | 3.3% |
| J | 5.6% | 14.3% | 5.7% | 8.8% | 6.5% | 6.7% | 3.9% | 7.3% | 6.5% | 6,7% |
| G | 2.8% | - | 3.4% | - | 3.9% | - | 3.9% | 2.1% | 1.1% | 6.7% * |
| I | 6.5% | - | 6.8% | 2.9% | 5.2% | 6.7% | 3.9% | 6.3% | 6.5% * | 3.3% |
| Other | 2.8% | 21.4% * | 3.4% | 8.8% | 2.6% | 8.9% | 6.3% | 4.4% | 6.7% |
| Mean Values (mg/dL) | R (n = 88) | E (n = 10) | J (n = 8) | G (n = 3) | I (n = 7) | Other (n = 6) |
|---|---|---|---|---|---|---|
| HDL cholesterol | 37.6 | 42.7 | 39 | 34 | 39.57 | 33.33 |
| LDL cholesterol | 114.97 | 120.7 | 111.63 | 110 | 134.7 | 112.17 |
| Triglycerides | 173.30 | 157.2 | 152,88 | 140.67 | 191.86 | 242.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lorca, R.; Aparicio, A.; Salgado, M.; Álvarez-Velasco, R.; Pascual, I.; Gomez, J.; Vazquez-Coto, D.; Garcia-Lago, C.; Velázquez-Cuervo, L.; Cuesta-Llavona, E.; et al. Chromosome Y Haplogroup R Was Associated with the Risk of Premature Myocardial Infarction with ST-Elevation: Data from the CholeSTEMI Registry. J. Clin. Med. 2023, 12, 4812. https://doi.org/10.3390/jcm12144812
Lorca R, Aparicio A, Salgado M, Álvarez-Velasco R, Pascual I, Gomez J, Vazquez-Coto D, Garcia-Lago C, Velázquez-Cuervo L, Cuesta-Llavona E, et al. Chromosome Y Haplogroup R Was Associated with the Risk of Premature Myocardial Infarction with ST-Elevation: Data from the CholeSTEMI Registry. Journal of Clinical Medicine. 2023; 12(14):4812. https://doi.org/10.3390/jcm12144812
Chicago/Turabian StyleLorca, Rebeca, Andrea Aparicio, María Salgado, Rut Álvarez-Velasco, Isaac Pascual, Juan Gomez, Daniel Vazquez-Coto, Claudia Garcia-Lago, Lucinda Velázquez-Cuervo, Elías Cuesta-Llavona, and et al. 2023. "Chromosome Y Haplogroup R Was Associated with the Risk of Premature Myocardial Infarction with ST-Elevation: Data from the CholeSTEMI Registry" Journal of Clinical Medicine 12, no. 14: 4812. https://doi.org/10.3390/jcm12144812
APA StyleLorca, R., Aparicio, A., Salgado, M., Álvarez-Velasco, R., Pascual, I., Gomez, J., Vazquez-Coto, D., Garcia-Lago, C., Velázquez-Cuervo, L., Cuesta-Llavona, E., Avanzas, P., & Coto, E. (2023). Chromosome Y Haplogroup R Was Associated with the Risk of Premature Myocardial Infarction with ST-Elevation: Data from the CholeSTEMI Registry. Journal of Clinical Medicine, 12(14), 4812. https://doi.org/10.3390/jcm12144812