
Micronutrients in Pregnancy after Bariatric Surgery: A Narrative Review

 , ,
, ,
Abstract
:1. Introduction
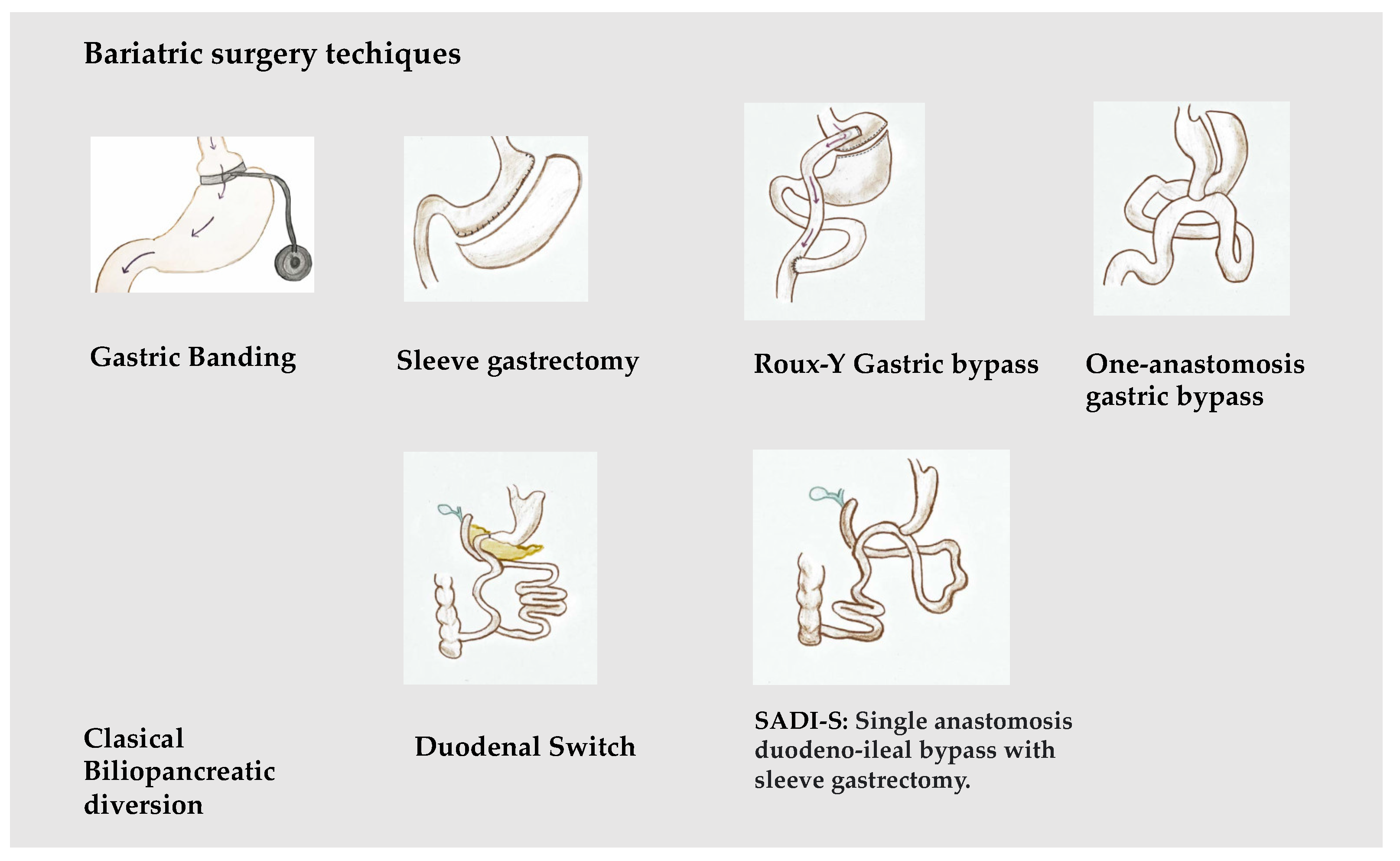
2. Bariatric Surgery and Pregnancy
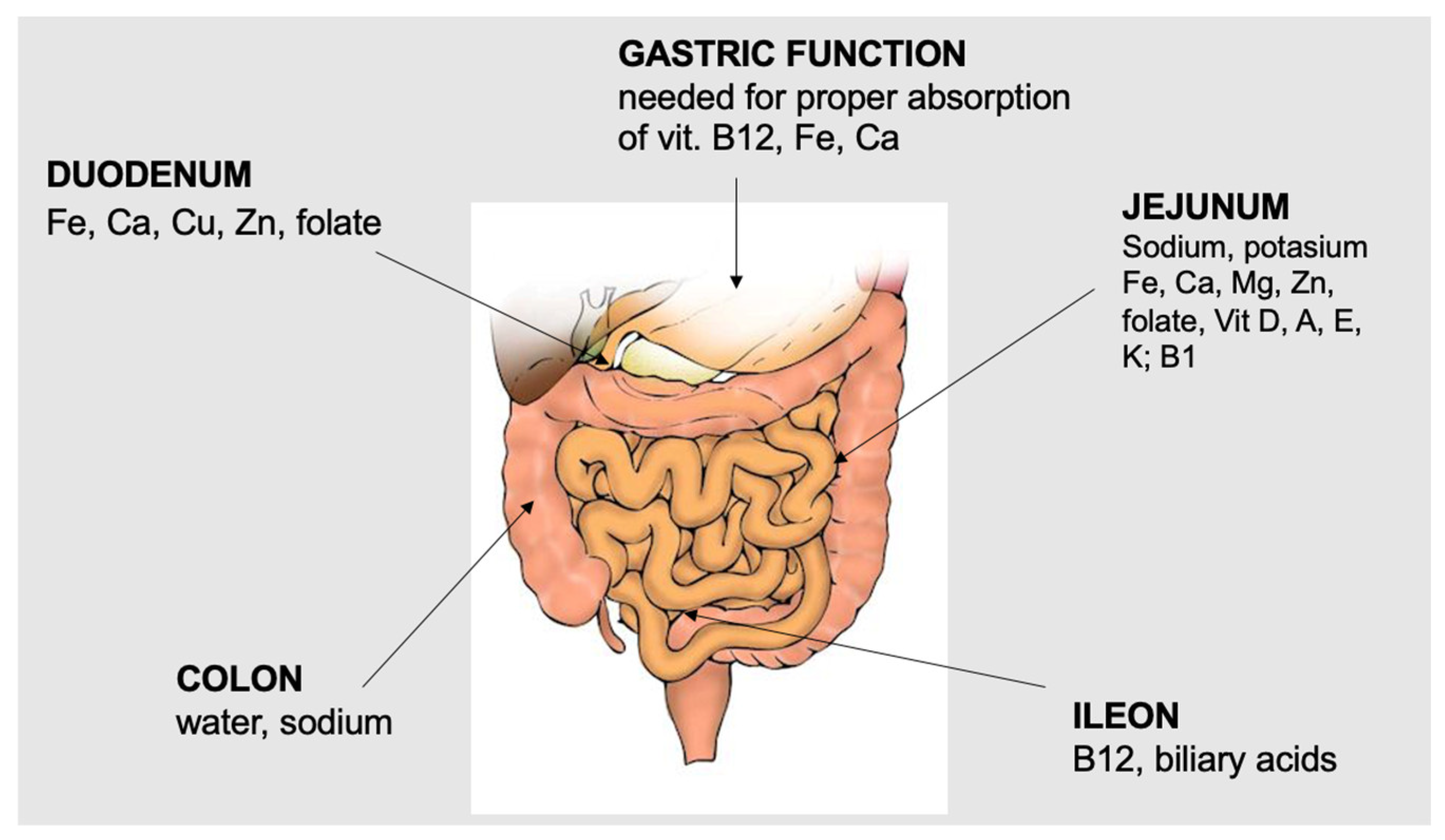
3. Micronutrients, Pregnancy, and Bariatric Surgery
3.1. Folate
3.2. Vitamin B12
3.3. Thiamine
3.4. Calcium and Vitamin D
3.5. Vitamin A
3.6. Vitamin E
3.7. Vitamin K
3.8. Iron
3.9. Magnesium
3.10. Zinc
3.11. Copper
3.12. Selenium
3.13. Iodine
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Mechanick, J.I.; Hurley, D.L.; Garvey, W.T. Adiposity-Based Chronic Disease as a new Diagnostic Term: The American Association of Clinical Endocrinologists and American College of Endocrinology Position Statement. Endocr. Pract. 2016, 23, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Garvey, W.T.; Mechanick, J.I.; Brett, E.M.; Garber, A.J.; Hurley, D.L.; Jastreboff, A.M.; Nadolsky, K.; Pessah-Pollack, R.; Plodkowski, R.; Reviewers of the AACE/ACE Obesity Clinical Practice Guidelines. American association of clinical endocrinologists and american college of endocrinology comprehensive clinical practice guidelines for medical care of patients with obesity—Executive Summary. Endocr. Pract. 2016, 22, 1–203. [Google Scholar] [CrossRef]
- Rittenberg, V.; Seshadri, S.; Sunkara, S.K.; Sobaleva, S.; Oteng-Ntim, E.; El-Toukhy, T. Effect of body mass index on IVF treatment outcome: An updated systematic review and meta-analysis. Reprod. Biomed. Online 2011, 23, 421–439. [Google Scholar] [CrossRef] [PubMed]
- Bellver, J.; Busso, C.; Pellicer, A.; Remohí, J.; Simón, C. Obesity and assisted reproductive technology outcomes. Reprod. Biomed. Online 2006, 12, 562–568. [Google Scholar] [CrossRef] [PubMed]
- Yu, Z.; Han, S.; Zhu, J.; Sun, X.; Ji, C.; Guo, X. Pre-Pregnancy Body Mass Index in Relation to Infant Birth Weight and Offspring Overweight/Obesity: A Systematic Review and Meta-Analysis. PLoS ONE 2013, 8, e61627. [Google Scholar] [CrossRef] [PubMed]
- Marchi, J.; Berg, M.; Dencker, A.; Olander, E.K.; Begley, C. Risks associated with obesity in pregnancy, for the mother and baby: A systematic review of reviews. Obes. Rev. 2015, 16, 621–638. [Google Scholar] [CrossRef]
- Goldstein, R.F.; Abell, S.K.; Ranasinha, S.; Misso, M.; Boyle, J.A.; Black, M.H.; Li, N.; Hu, G.; Corrado, F.; Rode, L.; et al. Association of Gestational Weight Gain with Maternal and Infant Outcomes: A Systematic Review and Meta-analysis. JAMA 2017, 317, 2207–2225. [Google Scholar] [CrossRef]
- Santos, S.; Voerman, E.; Amiano, P.; Barros, H.; Beilin, L.; Bergström, A.; Charles, M.; Chatzi, L.; Chevrier, C.; Chrousos, G.; et al. Impact of maternal body mass index and gestational weight gain on pregnancy complications: An individual participant data meta-analysis of European, North American, and Australian cohorts. BJOG 2019, 126, 984–995. [Google Scholar] [CrossRef]
- Martin, A.; Krishna, I.; Ellis, J.; Paccione, R.; Badell, M. Super obesity in pregnancy: Difficulties in clinical management. J. Perinatol. 2014, 34, 495–502. [Google Scholar] [CrossRef]
- Crane, J.M.; Murphy, P.; Burrage, L.; Hutchens, D. Maternal and Perinatal Outcomes of Extreme Obesity in Pregnancy. J. Obstet. Gynaecol. Can. 2013, 35, 606–611. [Google Scholar] [CrossRef]
- Arterburn, D.E.; Courcoulas, A.P. Bariatric surgery for obesity and metabolic conditions in adults. BMJ 2014, 349, g3961. [Google Scholar] [CrossRef] [PubMed]
- Angrisani, L.; Santonicola, A.; Iovino, P.; Ramos, A.; Shikora, S.; Kow, L. Bariatric Surgery Survey 2018: Similarities and Disparities Among the 5 IFSO Chapters. Obes. Surg. 2021, 31, 1937–1948. [Google Scholar] [CrossRef]
- Batterham, R.L.; Cummings, D.E. Mechanisms of Diabetes Improvement Following Bariatric/Metabolic Surgery. Diabetes Care 2016, 39, 893–901. [Google Scholar] [CrossRef] [PubMed]
- Hutch, C.R.; Sandoval, D.A. Physiological and molecular responses to bariatric surgery: Markers or mechanisms underlying T2DM resolution? Ann. N. Y. Acad. Sci. 2017, 1391, 5–19. [Google Scholar] [CrossRef]
- Davies, N.K.; O’Sullivan, J.M.; Plank, L.D.; Murphy, R. Altered gut microbiome after bariatric surgery and its association with metabolic benefits: A systematic review. Surg. Obes. Relat. Dis. 2019, 15, 656–665. [Google Scholar] [CrossRef]
- Penney, N.C.; Kinross, J.; Newton, R.C.; Purkayastha, S. The role of bile acids in reducing the metabolic complications of obesity after bariatric surgery: A systematic review. Int. J. Obes. 2015, 39, 1565–1574. [Google Scholar] [CrossRef]
- Vítek, L.; Haluzík, M. The role of bile acids in metabolic regulation. J. Endocrinol. 2016, 228, R85–R96. [Google Scholar] [CrossRef]
- Syn, N.L.; E Cummings, D.; Wang, L.Z.; Lin, D.J.; Zhao, J.J.; Loh, M.; Koh, Z.J.; Chew, C.A.; Loo, Y.E.; Tai, B.C.; et al. Association of metabolic–bariatric surgery with long-term survival in adults with and without diabetes: A one-stage meta-analysis of matched cohort and prospective controlled studies with 174 772 participants. Lancet 2021, 397, 1830–1841. [Google Scholar] [CrossRef]
- Wiggins, T.; Guidozzi, N.; Welbourn, R.; Ahmed, A.R.; Markar, S.R. Association of bariatric surgery with all-cause mortality and incidence of obesity-related disease at a population level: A systematic review and meta-analysis. PLOS Med. 2020, 17, e1003206. [Google Scholar] [CrossRef]
- Amaya García, M.J.; Vilchez López, F.J.; Campos Martín, C.; Sánchez Vera, P.; Pereira Cunill, J.L. Micronutrientes en Cirugía Bariátrica. Nutr. Hosp. 2012, 27, 349–361. [Google Scholar] [CrossRef]
- Parrott, J.; Frank, L.; Rabena, R.; Craggs-Dino, L.; Isom, K.A.; Greiman, L. American Society for Metabolic and Bariatric Surgery Integrated Health Nutritional Guidelines for the Surgical Weight Loss Patient 2016 Update: Micronutrients. Surg. Obes. Relat. Dis. 2019, 13, 727–741. [Google Scholar] [CrossRef] [PubMed]
- Jensterle, M.; Rizzo, M.; Janez, A. Glucagon-Like Peptide 1 and Taste Perception: From Molecular Mechanisms to Potential Clinical Implications. Int. J. Mol. Sci. 2021, 22, 902. [Google Scholar] [CrossRef] [PubMed]
- Mechanick, J.I.; Apovian, C.; Brethauer, S.; Garvey, W.T.; Joffe, A.M.; Kim, J.; Kushner, R.F.; Lindquist, R.; Pessah-Pollack, R.; Seger, J.; et al. Clinical practice guidelines for the perioperative nutrition, metabolic, and nonsurgical support of patients undergoing bariatric procedures—2019 update: Cosponsored by American Association of Clinical Endocrinologists/American College of Endocrinology, The Obesity Society, American Society for Metabolic & Bariatric Surgery, Obesity Medicine Association, and American Society of Anesthesiologists. Surg. Obes. Relat. Dis. 2020, 16, 175–247. [Google Scholar] [CrossRef] [PubMed]
- O’Kane, M.; Parretti, H.M.; Pinkney, J.; Welbourn, R.; Hughes, C.A.; Mok, J.; Walker, N.; Thomas, D.; Devin, J.; Coulman, K.D.; et al. British Obesity and Metabolic Surgery Society Guidelines on perioperative and postoperative biochemical monitoring and micronutrient replacement for patients undergoing bariatric surgery—2020 update. Obes. Rev. 2020, 21, e13087. [Google Scholar] [CrossRef]
- Galazis, N.; Docheva, N.; Simillis, C.; Nicolaides, K.H. Maternal and neonatal outcomes in women undergoing bariatric surgery: A systematic review and meta-analysis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 181, 45–53. [Google Scholar] [CrossRef]
- Yi, X.Y.; Li, Q.F.; Zhang, J.; Wang, Z.H. A meta-analysis of maternal and fetal outcomes of pregnancy after bariatric surgery. Int. J. Gynaecol. Obstet. 2015, 130, 3–9. [Google Scholar] [CrossRef]
- Kwong, W.; Tomlinson, G.; Feig, D.S. Maternal and neonatal outcomes after bariatric surgery; a systematic review and meta-analysis: Do the benefits outweigh the risks? Am. J. Obstet. Gynecol. 2018, 218, 573–580. [Google Scholar] [CrossRef]
- Badreldin, N.; Kuller, J.; Rhee, E.; Brown, L.; Laifer, S. Pregnancy Management After Bariatric Surgery. Obstet. Gynecol. Surv. 2016, 71, 361–368. [Google Scholar] [CrossRef]
- Harreiter, J.; Schindler, K.; Bancher-Todesca, D.; Göbl, C.; Langer, F.; Prager, G.; Gessl, A.; Leutner, M.; Ludvik, B.; Luger, A.; et al. Management of Pregnant Women after Bariatric Surgery. J. Obes. 2018, 2018, 4587064. [Google Scholar] [CrossRef]
- González, I.; Lecube, A.; Rubio, M.; García-Luna, P.P. Pregnancy after bariatric surgery: Improving outcomes for mother and child. Int. J. Women’s Health 2016, 8, 721–729. [Google Scholar] [CrossRef]
- Shawe, J.; Ceulemans, D.; Akhter, Z.; Neff, K.; Hart, K.; Heslehurst, N.; Štotl, I.; Agrawal, S.; Steegers-Theunissen, R.; Taheri, S.; et al. Pregnancy after bariatric surgery: Consensus recommendations for periconception, antenatal and postnatal care. Obes. Rev. 2019, 20, 1507–1522. [Google Scholar] [CrossRef] [PubMed]
- Alamri, S.H.; Abdeen, G.N. Maternal Nutritional Status and Pregnancy Outcomes Post-bariatric Surgery. Obes. Surg. 2022, 32, 1325–1340. [Google Scholar] [CrossRef] [PubMed]
- Huang, B.; Yo, J.H.; Gandhi, S.; Maxwell, C. Micronutrient screening, monitoring, and supplementation in pregnancy after bariatric surgery. Obstet. Med. 2022, 15, 151–159. [Google Scholar] [CrossRef]
- Guthrie, T.M.; Dix, C.F.; Truby, H.; Kumar, S.; de Jersey, S.J. A Systematic Review Investigating Maternal Nutrition During Pregnancy After Bariatric Surgery. Obes. Surg. 2023, 33, 1857–1865. [Google Scholar] [CrossRef] [PubMed]
- Akhter, Z.; Rankin, J.; Ceulemans, D.; Ngongalah, L.; Ackroyd, R.; Devlieger, R.; Vieiram, R.; Heslehurst, N. Investigating the association between pregnancy following bariatric surgery and adverse perinatal outcomes: A systematic review and meta-analysis. PLoS Med. 2018, 125, e1002866. [Google Scholar]
- Cooper, N.; Fiennes, A.; Hashemi, M.; Adamo, M.; El-Kalaawy, M. Pregnancy in first 12 months after bariatric surgery. Surg. Obes. Relat. Dis. 2010, 6, 234. [Google Scholar] [CrossRef]
- Johansson, K.; Cnattingius, S.; Näslund, I.; Roos, N.; Lagerros, Y.T.; Granath, F.; Stephansson, O.; Neovius, M. Outcomes of Pregnancy after Bariatric Surgery. N. Engl. J. Med. 2015, 372, 814–824. [Google Scholar] [CrossRef] [PubMed]
- Heusschen, L.; Krabbendam, I.; van der Velde, J.M.; Deden, L.N.; Aarts, E.O.; Merién, A.E.R.; Emous, M.; Bleumink, G.S.; Lutgers, H.L.; Hazebroek, E.J. A Matter of Timing—Pregnancy After Bariatric Surgery. Obes. Surg. 2021, 31, 2072–2079. [Google Scholar] [CrossRef] [PubMed]
- Harrison, R.K.; Berkelhammer, C.; Suarez, V.; Kay, H.H. Managing Malnourishment in Pregnancy after Bariatric Surgery. J. Obstet. Gynaecol. Can. 2018, 40, 211–214. [Google Scholar] [CrossRef]
- Karmon, A.; Sheiner, E. Pregnancy after bariatric surgery: A comprehensive review. Arch. Gynecol. Obstet. 2008, 277, 381–388. [Google Scholar] [CrossRef]
- Beiglböck, H.; Mörth, E.; Reichardt, B.; Stamm, T.; Itariu, B.; Harreiter, J.; Eichelter, J.; Prager, G.; Kautzky-Willer, A.; Wolf, P.; et al. The Timing of Pregnancies After Bariatric Surgery has No Impact on Children’s Health—A Nationwide Population-based Registry Analysis. Obes. Surg. 2023, 33, 149–155. [Google Scholar] [CrossRef]
- Mensink, G.B.M.; Fletcher, R.; Gurinović, M.; Huybrechts, I.; Lafay, L.; Serra-Majem, L.; Szponar, L.; Tetens, I.; Verkaik-Kloosterman, J.; Baka, A.; et al. Mapping low intake of micronutrients across Europe. Br. J. Nutr. 2013, 110, 755–773. [Google Scholar] [CrossRef]
- Das, J.K.; Salam, R.A.; Kumar, R.; Bhutta, Z.A. Micronutrient fortification of food and its impact on woman and child health: A systematic review. Syst. Rev. 2013, 23, 2–67. [Google Scholar] [CrossRef]
- Maslin, K.; James, A.; Brown, A.; Bogaerts, A.; Shawe, J. What Is Known About the Nutritional Intake of Women during Pregnancy Following Bariatric Surgery? A Scoping Review. Nutrients 2019, 11, 2116. [Google Scholar] [CrossRef]
- Lecube, A.; de Hollanda, A.; Calañas, A.; Vilarrasa, N.; Rubio, M.A.; Breton, I.; Goday, A.; Vidal, J.; Iglesias, P.; Fernández-Soto, M.L.; et al. Trends in Bariatric Surgery in Spain in the Twenty-First Century: Baseline Results and 1-Month Follow Up of the RICIBA, a National Registry. Obes. Surg. 2015, 26, 1836–1842. [Google Scholar] [CrossRef] [PubMed]
- Alanis, M.C.; Goodnight, W.H.; Hill, E.G.; Robinson, C.J.; Villers, M.S.; Johnson, D.D. Maternal super-obesity (body mass index ≥ 50) and adverse pregnancy outcomes. Acta Obstet. Gynecol. Scand. 2010, 89, 924–930. [Google Scholar] [CrossRef] [PubMed]
- Cogswell, M.E.; Weisberg, P.; Spong, C. Cigarette smoking, alcohol use and adverse pregnancy outcomes: Implications for micronutrient supplementation. J. Nutr. 2003, 133 (Suppl. S1), 1722S–1731S. [Google Scholar] [CrossRef] [PubMed]
- Abbassi-Ghanavati, M.; Greer, L.G.; Cunningham, F.G. Pregnancy and Laboratory Studies. Obstet. Gynecol. 2009, 114, 1326–1331. [Google Scholar] [CrossRef]
- Bailey, L.B.; Stover, P.J.; McNulty, H.; Fenech, M.F.; Gregory, J.F., III.; Mills, J.L.; Pfeiffer, C.M.; Fazili, Z.; Zhang, M.; Ueland, P.M.; et al. Biomarkers of Nutrition for Development—Folate Review. J. Nutr. 2015, 145, 1636S–1680S. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products; Nutrition and Allergies (NDA). Scientific Opinion on Dietary Reference Values for iron. EFSA J. 2015, 13, 4254. [Google Scholar] [CrossRef]
- MRC Vitamin Study Research Group. Prevention of neural tube defects: Results of the Medical Research Council Vitamin Study. Lancet 1991, 338, 131–137. [Google Scholar] [CrossRef]
- Shaw, G.M.; Carmichael, S.L.; Nelson, V.; Selvin, S.; Schaffer, D.M. Occurrence of Low Birthweight and Preterm Delivery among California Infants before and after Compulsory Food Fortification with Folic Acid. Public Health Rep. 2004, 119, 170–173. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, L.; Médico, M. Suplementos en embarazadas: Controversias, evidencias y recomendaciones. Inf. Ter. Sist. Nac. Salud. 2010, 34, 117–128. [Google Scholar]
- Rottenstreich, A.; Elazary, R.; Goldenshluger, A.; Pikarsky, A.J.; Elchalal, U.; Ben-Porat, T. Maternal nutritional status and related pregnancy outcomes following bariatric surgery: A systematic review. Surg. Obes. Relat. Dis. 2019, 15, 324–332. [Google Scholar] [CrossRef]
- Mojtabai, R. Body mass index and serum folate in childbearing age women. Eur. J. Epidemiol. 2004, 19, 1029–1036. [Google Scholar] [CrossRef]
- De-Regil, L.M.; Peña-Rosas, J.P.; Fernández-Gaxiola, A.C.; Rayco-Solon, P. Effects and safety of periconceptional oral folate supplementation for preventing birth defects. Cochrane Database Syst. Rev. 2015, 2015, CD007950. [Google Scholar] [CrossRef]
- Lassi, Z.S.; Salam, R.A.; Haider, B.A.; Bhutta, Z.A. Folic acid supplementation during pregnancy for maternal health and pregnancy outcomes. Cochrane Database Syst. Rev. 2013, 3, CD006896. [Google Scholar] [CrossRef] [PubMed]
- Moussa, H.N.; Nasab, S.H.; A Haidar, Z.; Blackwell, S.C.; Sibai, B.M.; Srikrishnan, A.; Dash, P.; Divieto, C.; Sassi, M.P.; Abdelhafiz, A.H.; et al. Folic acid supplementation: What is new? Fetal, obstetric, long-term benefits and risks. Futur. Sci. OA 2016, 2, FSO116. [Google Scholar] [CrossRef] [PubMed]
- E Brolin, R.; Gorman, R.C.; Milgrim, L.M.; A Kenler, H. Multivitamin prophylaxis in prevention of post-gastric bypass vitamin and mineral deficiencies. Int. J. Obes. 1991, 15, 661–667. [Google Scholar]
- MacLean, L.D. Nutrition following intestinal bypass and gastric operations for morbid obesity. Can. J. Surg. 1984, 27, 134–135. [Google Scholar]
- Gasteyger, C.; Suter, M.; Calmes, J.M.; Gaillard, R.C.; Giusti, V. Changes in Body Composition, Metabolic Profile and Nutritional Status 24 Months after Gastric Banding. Obes. Surg. 2006, 16, 243–250. [Google Scholar] [CrossRef]
- Aasheim, E.T.; Björkman, S.; Søvik, T.T.; Engström, M.; E Hanvold, S.; Mala, T.; Olbers, T.; Bøhmer, T. Vitamin status after bariatric surgery: A randomized study of gastric bypass and duodenal switch. Am. J. Clin. Nutr. 2009, 90, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Skroubis, G.; Sakellaropoulos, G.; Pouggouras, K.; Mead, N.; Nikiforidis, G.; Kalfarentzos, F. Comparison of Nutritional Deficiencies after Rouxen-Y Gastric Bypass and after Biliopancreatic Diversion with Roux-en-Y Gastric Bypass. Obes. Surg. 2002, 12, 551–558. [Google Scholar] [CrossRef]
- Weng, T.-C.; Chang, C.-H.; Dong, Y.-H.; Chang, Y.-C.; Chuang, L.-M. Anaemia and related nutrient deficiencies after Roux-en-Y gastric bypass surgery: A systematic review and meta-analysis. BMJ Open 2015, 5, e006964. [Google Scholar] [CrossRef] [PubMed]
- Moliterno, J.A.; DiLuna, M.L.; Sood, S.; Roberts, K.E.; Duncan, C.C. Gastric bypass: A risk factor for neural tube defects? J. Neurosurg. Pediatr. 2008, 1, 406–409. [Google Scholar] [CrossRef]
- Pelizzo, G.; Calcaterra, V.; Fusillo, M.; Nakib, G.; Ierullo, A.M.; Alfei, A.; Spinillo, A.; Stronati, M.; Cena, H. Malnutrition in pregnancy following bariatric surgery: Three clinical cases of fetal neural defects. Nutr. J. 2014, 13, 59. [Google Scholar] [CrossRef]
- Devlieger, R.; Guelinckx, I.; Jans, G.; Voets, W.; Vanholsbeke, C.; Vansant, G. Micronutrient Levels and Supplement Intake in Pregnancy after Bariatric Surgery: A Prospective Cohort Study. PLoS ONE 2014, 9, e114192. [Google Scholar] [CrossRef] [PubMed]
- Bebber, F.E.; Rizzolli, J.; Casagrande, D.S.; Rodrigues, M.T.; Padoin, A.V.; Mottin, C.C.; Repetto, G. Pregnancy after Bariatric Surgery: 39 Pregnancies Follow-up in a Multidisciplinary Team. Obes. Surg. 2011, 21, 1546–1551. [Google Scholar] [CrossRef]
- González, I.; Rubio, M.A.; Cordido, F.; Bretón, I.; Morales, M.J.; Vilarrasa, N.; Monereo, S.; Lecube, A.; Caixàs, A.; Vinagre, I.; et al. Maternal and Perinatal Outcomes After Bariatric Surgery: A Spanish Multicenter Study. Obes. Surg. 2014, 25, 436–442. [Google Scholar] [CrossRef]
- O’leary, F.; Samman, S. Vitamin B12 in Health and Disease. Nutrients 2010, 2, 299–316. [Google Scholar] [CrossRef]
- Finkelstein, J.L.; Layden, A.J.; Stover, P.J. Vitamin B-12 and Perinatal Health. Adv. Nutr. Int. Rev. J. 2015, 6, 552–563. [Google Scholar] [CrossRef]
- Rogne, T.; Tielemans, M.J.; Chong, M.F.-F.; Yajnik, C.S.; Krishnaveni, G.V.; Poston, L.; Jaddoe, V.W.V.; Steegers, E.A.P.; Joshi, S.; Chong, Y.-S.; et al. Associations of Maternal Vitamin B12 Concentration in Pregnancy with the Risks of Preterm Birth and Low Birth Weight: A Systematic Review and Meta-Analysis of Individual Participant Data. Am. J. Epidemiol. 2017, 185, 212–223. [Google Scholar] [CrossRef]
- Majumder, S.; Soriano, J.; Cruz, A.L.; Dasanu, C.A. Vitamin B12 deficiency in patients undergoing bariatric surgery: Preventive strategies and key recommendations. Surg. Obes. Relat. Dis. 2013, 9, 1013–1019. [Google Scholar] [CrossRef] [PubMed]
- Smelt, H.J.M.; Pouwels, S.; Smulders, J.F. Different Supplementation Regimes to Treat Perioperative Vitamin B12 Deficiencies in Bariatric Surgery: A Systematic Review. Obes. Surg. 2017, 27, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Mechanick, J.; Youdim, A.; Jones, D.; Timothy Garvey, W.; Hurley, D.L.; Mc Mahon, M. AACE/TOS/ASMBS Bariatric Surgery Clinical Practice Guidelines. Endocr. Pract. 2013, 19, 1–36. [Google Scholar]
- Busetto, L.; Dicker, D.; Azran, C.; Batterham, R.L.; Farpour-Lambert, N.; Fried, M.; Hjelmesæth, J.; Kinzl, J.; Leitner, D.R.; Makaronidis, J.M.; et al. Obesity Management Task Force of the European Association for the Study of Obesity Released “Practical Recommendations for the Post-Bariatric Surgery Medical Management”. Obes. Surg. 2018, 28, 2117–2121. [Google Scholar] [CrossRef] [PubMed]
- Grange, D.K.; Finlay, J.L. Nutritional Vitamin B12 Deficiency in a Breastfed Infant Following Maternal Gastric Bypass. Pediatr. Hematol. Oncol. 1994, 11, 311–318. [Google Scholar] [CrossRef]
- Wardinsky, T.D.; Montes, R.G.; Friederich, R.L.; Broadhurst, R.B.; Sinnhuber, V.; Bartholomew, D. Vitamin B12 Deficiency Associated With Low Breast-Milk Vitamin B12 Concentration in an Infant Following Maternal Gastric Bypass Surgery. Arch. Pediatr. Adolesc. Med. 1995, 149, 1281–1284. [Google Scholar] [CrossRef]
- Celiker, M.Y.; Chawla, A. Congenital B12 deficiency following maternal gastric bypass. J. Perinatol. 2009, 29, 640–642. [Google Scholar] [CrossRef]
- Gascoin, G.; Gerard, M.; Sallé, A.; Becouarn, G.; Rouleau, S.; Sentilhes, L.; Coutant, R. Risk of low birth weight and micronutrient deficiencies in neonates from mothers after gastric bypass: A case control study. Surg. Obes. Relat. Dis. 2017, 13, 1384–1391. [Google Scholar] [CrossRef]
- Mead, N.C.; Sakkatos, P.; Sakellaropoulos, G.C.; Adonakis, G.L.; Alexandrides, T.K.; Kalfarentzos, F. Pregnancy outcomes and nutritional indices after 3 types of bariatric surgery performed at a single institution. Surg. Obes. Relat. Dis. 2014, 10, 1166–1173. [Google Scholar] [CrossRef]
- Sriram, K.; Manzanares, W.; Joseph, K. Thiamine in Nutrition Therapy. Nutr. Clin. Pract. 2012, 27, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Ashraf, V.; Prijesh, J.; Praveenkumar, R.; Saifudheen, K. Wernicke’s encephalopathy due to hyperemesis gravidarum: Clinical and magnetic resonance imaging characteristics. J. Postgrad. Med. 2016, 62, 260–263. [Google Scholar] [CrossRef]
- Frank, L.L. Thiamin in Clinical Practice. J. Parenter. Enter. Nutr. 2015, 39, 503–520. [Google Scholar] [CrossRef]
- Kareem, O.; Nisar, S.; Tanvir, M.; Muzaffer, U.; Bader, G.N. Thiamine deficiency in pregnancy and lactation: Implications and present perspectives. Front. Nutr. 2023, 10, 1080611. [Google Scholar] [CrossRef]
- Di Gangi, S.; Gizzo, S.; Patrelli, T.S.; Saccardi, C.; D’antona, D.; Nardelli, G.B. Wernicke’s encephalopathy complicating hyperemesis gravidarum: From the background to the present. J. Matern. Neonatal Med. 2012, 25, 1499–1504. [Google Scholar] [CrossRef] [PubMed]
- Finglas, P.M. Dietary Reference intakes for thiamin, riboflavin, niacin, vitamin B6, folate, vitamin B12, pantothenic acid, biotin and choline. Trends Food Sci. Technol. 2000, 11, 296–297. [Google Scholar] [CrossRef]
- Jans, G.; Matthys, C.; Bogaerts, A.; Lannoo, M.; Verhaeghe, J.; Van der Schueren, B.; Devlieger, R. Maternal Micronutrient Deficiencies and Related Adverse Neonatal Outcomes after Bariatric Surgery: A Systematic Review. Adv. Nutr. Int. Rev. J. 2015, 6, 420–429. [Google Scholar] [CrossRef]
- Kröll, D.; Laimer, M.; Borbély, Y.M.; Laederach, K.; Candinas, D.; Nett, P.C. Wernicke Encephalopathy: A Future Problem Even After Sleeve Gastrectomy? A Systematic Literature Review. Obes. Surg. 2016, 26, 205–212. [Google Scholar] [CrossRef]
- Ngene, N.C.; Moodley, J. Clinical awareness for health care professionals: Fatal encephalopathy complicating persistent vomiting in pregnancy. S. Afr. Med. J. 2016, 106, 792–794. [Google Scholar] [CrossRef]
- Bahardoust, M.; Eghbali, F.; Shahmiri, S.S.; Alijanpour, A.; Yarigholi, F.; Valizadeh, R.; Madankan, A.; Pouraskari, A.B.; Ashtarinezhad, B.; Farokhi, H.; et al. B1 Vitamin Deficiency After Bariatric Surgery, Prevalence, and Symptoms: A Systematic Review and Meta-analysis. Obes. Surg. 2022, 32, 3104–3112. [Google Scholar] [CrossRef] [PubMed]
- Saab, R.O.; El Khoury, M.I.; Jabbour, R.A. Wernicke encephalopathy after Roux-en-Y gastric bypass and hyperemesis gravidarum. Surg. Obes. Relat. Dis. 2013, 9, e105–e107. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, Treatment, and Prevention of Vitamin D Deficiency: An Endocrine Society Clinical Practice Guideline. Med. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Wagner, C.L.; Hollis, B.W. The Implications of Vitamin D Status During Pregnancy on Mother and her Developing Child. Front. Endocrinol. 2018, 9, 500. [Google Scholar] [CrossRef]
- Bodnar, L.M.; Catov, J.M.; Simhan, H.N.; Holick, M.F.; Powers, R.W.; Roberts, J.M. Maternal Vitamin D Deficiency Increases the Risk of Preeclampsia. J. Clin. Endocrinol. Metab. 2007, 92, 3517–3522. [Google Scholar] [CrossRef]
- Wei, S.-Q.; Qi, H.-P.; Luo, Z.-C.; Fraser, W.D. Maternal vitamin D status and adverse pregnancy outcomes: A systematic review and meta-analysis. J. Matern.-Fetal Neonatal Med. 2013, 26, 889–899. [Google Scholar] [CrossRef] [PubMed]
- Hu, K.-L.; Zhang, C.-X.; Chen, P.; Zhang, D.; Hunt, S. Vitamin D Levels in Early and Middle Pregnancy and Preeclampsia, a Systematic Review and Meta-Analysis. Nutrients 2022, 14, 999. [Google Scholar] [CrossRef] [PubMed]
- Perez-Ferre, N.; Torrejon, M.J.; Fuentes, M.; Fernandez, M.D.; Ramos, A.; Bordiu, E.; del Valle, L.; Rubio, M.A.; Bedia, A.R.; Montañez, C.; et al. Association of Low Serum 25-Hydroxyvitamin D Levels in Pregnancy with Glucosehomeostasis and Obstetric And Newborn Outcomes. Endocr. Pract. 2012, 18, 676–684. [Google Scholar] [CrossRef] [PubMed]
- Switzer, N.J.; Marcil, G.; Prasad, S.; Debru, E.; Church, N.; Mitchell, P.; Billington, E.O.; Gill, R.S. Long-term hypovitaminosis D and secondary hyperparathyroidism outcomes of the Roux-en-Y gastric bypass: A systematic review. Obes. Rev. 2017, 65, 560–566. [Google Scholar] [CrossRef]
- Chakhtoura, M.T.; Nakhoul, N.; Akl, E.A.; Mantzoros, C.S.; El Hajj Fuleihan, G.A. Guidelines on vitamin D replacement in bariatric surgery: Identification and systematic appraisal. Metabolism 2016, 65, 586–597. [Google Scholar] [CrossRef] [PubMed]
- Medeiros, M.; Matos, A.C.; Pereira, S.E.; Saboya, C.; Ramalho, A. Vitamin D and its relation with ionic calcium, parathyroid hormone, maternal and neonatal characteristics in pregnancy after roux-en-Y gastric bypass. Arch. Gynecol. Obstet. 2016, 293, 539–547. [Google Scholar] [CrossRef]
- Cruz, S.; de Matos, A.C.; da Cruz, S.P.; Pereira, S.; Saboya, C.; Ramalho, A. Maternal Anthropometry and Its Relationship with the Nutritional Status of Vitamin D, Calcium, and Parathyroid Hormone in Pregnant Women after Roux-en-Y Gastric Bypass. Obes. Surg. 2018, 28, 3116–3124. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Prevalence of Vitamin A Deficiency in Populations at Risk 1995–2005: WHO Global Database on Vitamin A Deficiency; WHO Iris: Geneva, Switzerland, 2009; p. 55. Available online: https://apps.who.int/iris/handle/10665/44110 (accessed on 15 August 2023).
- Snoek, K.; van de Woestijne, N.; Willemsen, S.; Klaassen, R.; Galjaard, S.; Laven, J.; Steegers-Theunissen, R.; Schoenmakers, S. The Impact of Preconception Gastric Bypass Surgery on Maternal Micronutrient Status before and during Pregnancy: A Retrospective Cohort Study in the Netherlands between 2009 and 2019. Nutrients 2022, 14, 736. [Google Scholar] [CrossRef] [PubMed]
- OMS. Concentraciones en suero de retinol para establecer la prevalencia de la carencia de vitamina A a escala poblacional. In Sistema de Información Nutricional Sobre Vitaminas y Minerales; Organización Mundial de la Salud: Geneva, Switzerland, 2011. [Google Scholar]
- Rubio, M.A.; Cuesta, M.; Pelaz, L.; Pérez, C.; Torrejón, M.J.; Cabrerizo, L.; Matía, P.; Pérez-Ferre, N.; Sánchez-Pernaute, A.; Torres, A. Fat-soluble vitamin deficiencies after bariatric surgery could be misleading if they are not appropriately adjusted. Nutr. Hosp. 2014, 30, 118–123. [Google Scholar] [CrossRef]
- Rayman, M.P.; Bode, P.; Redman, C.W.G. Low selenium status is associated with the occurrence of the pregnancy disease preeclampsia in women from the United Kingdom. Am. J. Obstet. Gynecol. 2003, 189, 1343–1349. [Google Scholar] [CrossRef]
- Oliveira, J.M.; Michelazzo, F.B.; Stefanello, J.; Rondó, P.H. Influence of iron on vitamin A nutritional status. Nutr. Rev. 2008, 66, 141–147. [Google Scholar] [CrossRef]
- WHO. Guideline: Vitamin A Supplementation in Pregnant Women; World Health Organization: Geneva, Switzerland, 2011; pp. 1–30. [Google Scholar]
- McCauley, M.E.; van den Broek, N.; Dou, L.; Othman, M. Vitamin A supplementation during pregnancy for maternal and newborn outcomes. Cochrane Database Syst. Rev. 2015, 10, CD008666. [Google Scholar] [CrossRef]
- EFSA NDA Panel. Scientific Opinion on Dietary Reference Values for biotin. EFSA J. 2015, 12, 3580. [Google Scholar] [CrossRef]
- Slater, G.H.; Ren, C.J.; Siegel, N.; Williams, T.; Barr, D.; Wolfe, B.; Dolan, K.; A Fielding, G. Serum fat-soluble vitamin deficiency andabnormal calcium metabolism after malabsorptivebariatric surgery. J. Gastrointest. Surg. 2004, 8, 48–55. [Google Scholar] [CrossRef]
- Eckert, M.J.; Perry, J.T.; Sohn, V.Y.; Boden, J.; Martin, M.J.; Rush, R.M.; Steele, S.R. Incidence of low vitamin A levels and ocular symptoms after Roux-en-Y gastric bypass. Surg. Obes. Relat. Dis. 2010, 6, 653–657. [Google Scholar] [CrossRef]
- Pereira, S.; Saboya, C.; Chaves, G.; Ramalho, A. Class III Obesity and its Relationship with the Nutritional Status of Vitamin A in Pre- and Postoperative Gastric Bypass. Obes. Surg. 2009, 19, 738–744. [Google Scholar] [CrossRef] [PubMed]
- Vales Montero, M.; Chavarría Cano, B.; Martínez Ginés, M.L.; Díaz Otero, F.; Velázquez Pérez, J.M.; Cuerda Compes, M.C.; Bretón Lesmes, I. Deficiencia clínica de vitamina A tras bypass gástrico: Descripción de un caso clínico y revisión de la literatura. Nutr. Hosp. 2016, 33, 404. [Google Scholar] [CrossRef]
- Ocón, J.; Cabrejas, C.; Altemir, J.; Moros, M. Phrynoderma. J. Parenter. Enter. Nutr. 2012, 36, 361–364. [Google Scholar] [CrossRef]
- Fok, J.S.; Li, J.Y.Z.; Yong, T.Y. Visual deterioration caused by vitamin A deficiency in patients after bariatric surgery. Eat. Weight. Disord.—Stud. Anorexia, Bulim. Obes. 2012, 17, e144–e146. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Leví, A.M.; Pérez-Ferre, N.; Sánchez-Pernaute, A.; García, A.J.T.; Herrera, M.A.R. Torres Garcia, and M. a Rubio Herrera, “Severe vitamin A deficiency after malabsortive bariatric surgery. Nutr. Hosp. 2013, 28, 1337–1340. [Google Scholar] [CrossRef] [PubMed]
- Stroh, C.; Weiher, C.; Hohmann, U.; Meyer, F.; Lippert, H.; Manger, T. Vitamin A Deficiency (VAD) After a Duodenal Switch Procedure: A Case Report. Obes. Surg. 2009, 20, 397–400. [Google Scholar] [CrossRef]
- Chagas, C.B.; Saunders, C.; Pereira, S.; Silva, J.; Saboya, C.; Ramalho, A. Vitamin A Deficiency in Pregnancy: Perspectives after Bariatric Surgery. Obes. Surg. 2012, 23, 249–254. [Google Scholar] [CrossRef]
- Huerta, S.; Rogers, L.M.; Li, Z.; Heber, D.; Liu, C.; Livingston, E.H. Vitamin A deficiency in a newborn resulting from maternal hypovitaminosis A after biliopancreatic diversion for the treatment of morbid obesity. Am. J. Clin. Nutr. 2002, 76, 426–429. [Google Scholar] [CrossRef]
- Smets, K.J.; Barlow, T.; Vanhaesebrouck, P. Maternal vitamin A deficiency and neonatal microphthalmia: Complications of biliopancreatic diversion? Eur. J. Pediatr. 2006, 165, 502–504. [Google Scholar] [CrossRef]
- Breton, J.O.; Sallan, L. Maternal and neonatal complications in a pregnant woman with biliopancreatic diversion. [Spanish] TT—Complicaciones maternas y neonatales en una mujer gestante con derivacion biliopancreatica. Nutr. Hosp. Organo Of. Soc. Esp. Nutr. Parenter. Y Enter. 2010, 25, 120–122. [Google Scholar]
- Mackie, F.L.; Cooper, N.S.; Whitticase, L.J.; Smith, A.; Martin, W.L.; Cooper, S.C. Vitamin A and micronutrient deficiencies post-bariatric surgery: Aetiology, complications and management in a complex multiparous pregnancy. Eur. J. Clin. Nutr. 2018, 72, 1176–1179. [Google Scholar] [CrossRef] [PubMed]
- Cruz, S.; Matos, A.; Da Cruz, S.P.; Pereira, S.; Saboya, C.; Ramalho, A. Relationship between the Nutritional Status of Vitamin A per Trimester of Pregnancy with Maternal Anthropometry and Anemia after Roux-en-Y Gastric Bypass. Nutrients 2017, 9, 989. [Google Scholar] [CrossRef] [PubMed]
- Hazart, J.; Le Guennec, D.; Accoceberry, M.; Lemery, D.; Mulliez, A.; Farigon, N.; Lahaye, C.; Miolanne-Debouit, M.; Boirie, Y. Maternal Nutritional Deficiencies and Small-for-Gestational-Age Neonates at Birth of Women Who Have Undergone Bariatric Surgery. J. Pregnancy 2017, 2017, 4168541. [Google Scholar] [CrossRef] [PubMed]
- Niki, E.; Traber, M.G. A History of Vitamin E. Ann. Nutr. Metab. 2012, 61, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Traber, M.G. Vitamin E Inadequacy in Humans: Causes and Consequences. Adv. Nutr. Int. Rev. J. 2014, 5, 503–514. [Google Scholar] [CrossRef]
- Institute of Medicine; Food and Nutrition Board; Panel on Dietary Antioxidants and Related Compounds; Subcommittee on Upper Reference Levels of Nutrients; Subcommittee on Interpretation and Uses of Dietary Reference Intakes; Standing Committee on the Scientific Evaluation of Dietary Reference Intakes. Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium, and Carotenoids; National Academies Press (US): Washington, DC, USA, 2000. [Google Scholar] [CrossRef]
- Chen, K.; Zhang, X.; Wei, X.-P.; Qu, P.; Liu, Y.-X.; Li, T.-Y. Antioxidant vitamin status during pregnancy in relation to cognitive development in the first two years of life. Early Hum. Dev. 2009, 85, 421–427. [Google Scholar] [CrossRef]
- Koscik, R.L.; Lai, H.J.; Laxova, A.; Zaremba, K.M.; Kosorok, M.R.; Douglas, J.A.; Rock, M.J.; Splaingard, M.L.; Farrell, P.M. Preventing early, prolonged vitamin E deficiency: An opportunity for better cognitive outcomes via early diagnosis through neonatal screening. J. Pediatr. 2005, 147, S51–S56. [Google Scholar] [CrossRef]
- Hovdenak, N.; Haram, K. Influence of mineral and vitamin supplements on pregnancy outcome. Eur. J. Obstet. Gynecol. Reprod. Biol. 2012, 164, 127–132. [Google Scholar] [CrossRef]
- Sitrin, M.D.; Lieberman, F.; Jensen, W.E.; Noronha, A.; Milburn, C.; Addington, W. Vitamin E Deficiency and Neurologic Disease in Adults with Cystic Fibrosis. Ann. Intern. Med. 1987, 107, 51–54. [Google Scholar] [CrossRef]
- Wilson, R.D.; Audibert, F.; Brock, J.-A.; Carroll, J.; Cartier, L.; Gagnon, A.; Johnson, J.-A.; Langlois, S.; Murphy-Kaulbeck, L.; Okun, N.; et al. Pre-conception Folic Acid and Multivitamin Supplementation for the Primary and Secondary Prevention of Neural Tube Defects and Other Folic Acid-Sensitive Congenital Anomalies. J. Obstet. Gynaecol. Can. 2015, 37, 534–549. [Google Scholar] [CrossRef] [PubMed]
- Bastos Maia, S.; Rolland Souza, A.S.; Costa Caminha, M.d.F.; Lins da Silva, S.; Callou Cruz, R.d.S.B.L.; Carvalho dos Santos, C.; Batista Filho, M. Vitamin A and Pregnancy: A Narrative Review. Nutrients 2019, 11, 681. [Google Scholar] [CrossRef]
- Harshman, S.G.; Saltzman, E.; Booth, S.L. Vitamin K. Curr. Opin. Clin. Nutr. Metab. Care 2014, 17, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Pearson, D.A. Bone Health and Osteoporosis: The Role of Vitamin K and Potential Antagonism by Anticoagulants. Nutr. Clin. Pract. 2007, 22, 517–544. [Google Scholar] [CrossRef]
- Shahrook, S.; Ota, E.; Hanada, N.; Sawada, K.; Mori, R. Vitamin K supplementation during pregnancy for improving outcomes: A systematic review and meta-analysis. Sci. Rep. 2018, 8, 11459. [Google Scholar] [CrossRef] [PubMed]
- Homan, J.; Ruinemans-Koerts, J.; Aarts, E.; Janssen, I.M.; Berends, F.J.; de Boer, H. Management of vitamin K deficiency after biliopancreatic diversion with or without duodenal switch. Surg. Obes. Relat. Dis. 2016, 12, 338–344. [Google Scholar] [CrossRef]
- Van Mieghem, T.; Van Schoubroeck, D.; Depiere, M.; Debeer, A.; Hanssens, M. Fetal Cerebral Hemorrhage Caused by Vitamin K Deficiency After Complicated Bariatric Surgery. Obstet. Gynecol. 2008, 112, 434–436. [Google Scholar] [CrossRef] [PubMed]
- Bersani, I.; De Carolis, M.P.; Salvi, S.; Zecca, E.; Romagnoli, C.; De Carolis, S. Maternal–neonatal vitamin K deficiency secondary to maternal biliopancreatic diversion. Blood Coagul. Fibrinolysis 2011, 22, 334–336. [Google Scholar] [CrossRef]
- Jans, G.; Guelinckx, I.; Voets, W.; Galjaard, S.; Van Haard, P.M.; Vansant, G.M.; Devlieger, R. Vitamin K1 monitoring in pregnancies after bariatric surgery: A prospective cohort study. Surg. Obes. Relat. Dis. 2014, 10, 885–890. [Google Scholar] [CrossRef]
- Aron-Wisnewsky, J.; O Verger, E.; Bounaix, C.; Dao, M.C.; Oppert, J.-M.; Bouillot, J.-L.; Chevallier, J.-M.; Clément, K. Nutritional and Protein Deficiencies in the Short Term following Both Gastric Bypass and Gastric Banding. PLoS ONE 2016, 11, e0149588. [Google Scholar] [CrossRef]
- DeLoughery, T.G. Iron Deficiency Anemia. Med. Clin. N. Am. 2017, 101, 319–332. [Google Scholar] [CrossRef]
- Aigner, E.; Feldman, A.; Datz, C. Obesity as an Emerging Risk Factor for Iron Deficiency. Nutrients 2014, 6, 3587–3600. [Google Scholar] [CrossRef]
- Hamamy, H.; Alwan, N.A. Maternal Iron Status in Pregnancy and Long-Term Health Outcomes in the Offspring. J. Pediatr. Genet. 2015, 4, 111–123. [Google Scholar] [CrossRef]
- Spanish Ministry of Health. Grupo de Trabajo de la Guía de Práctica Clínica de Atención en el Embarazo y Puerperio; A Tención en el e Mbarazo y P Uerperio; Spanish Ministry of Health: Madrid, Spain, 2014; p. 397. [Google Scholar]
- Breymann, C. Iron deficiency and anaemia in pregnancy: Modern aspects of diagnosis and therapy. Eur. J. Obstet. Gynecol. Reprod. Biol. 2005, 123, S3–S13. [Google Scholar] [CrossRef]
- World Health Organization. Guideline: Daily Iron and Folic Acid Supplementation in Pregnant Women; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Muñoz, M.; Rosado, E.L. Iron Deficiency and Anaemia in Bariatric Surgical patients: Causes, Diagnosis and Proper Management. Nutr. Hosp. 2009, 24, 640–654. [Google Scholar] [CrossRef] [PubMed]
- Jericó, C.; Bretón, I.; de Gordejuela, A.G.R.; de Oliveira, A.C.; Rubio, M.; Tinahones, F.J.; Vidal, J.; Vilarrasa, N. Diagnóstico y tratamiento del déficit de hierro, con o sin anemia, pre y poscirugía bariátrica. Endocrinol. Y Nutr. 2016, 63, 32–42. [Google Scholar] [CrossRef]
- Steenackers, N.; Van der Schueren, B.; Mertens, A.; Lannoo, M.; Grauwet, T.; Augustijns, P.; Matthys, C. Iron deficiency after bariatric surgery: What is the real problem? Proc. Nutr. Soc. 2018, 77, 445–455. [Google Scholar] [PubMed]
- Nomura, R.M.Y.; Dias, M.C.G.; Igai, A.M.K.; Paiva, L.V.; Zugaib, M. Anemia During Pregnancy after Silastic Ring Roux-en-Y Gastric Bypass: Influence of Time to Conception. Obes. Surg. 2011, 21, 479–484. [Google Scholar] [CrossRef]
- Falcone, V.; Stopp, T.; Feichtinger, M.; Kiss, H.; Eppel, W.; Husslein, P.W.; Prager, G.; Göbl, C.S. Pregnancy after bariatric surgery: A narrative literature review and discussion of impact on pregnancy management and outcome. BMC Pregnancy Childbirth 2018, 18, 507. [Google Scholar] [CrossRef]
- Hezelgrave, N.L.; Oteng-Ntim, E. Pregnancy after Bariatric Surgery: A Review. J. Obes. 2011, 2011, 501939. [Google Scholar] [CrossRef]
- Dalfrà, M.G.; Busetto, L.; Chilelli, N.C.; Lapolla, A. Pregnancy and foetal outcome after bariatric surgery: A review of recent studies. J. Matern. Neonatal Med. 2012, 25, 1537–1543. [Google Scholar] [CrossRef]
- Gröber, U.; Schmidt, J.; Kisters, K. Magnesium in Prevention and Therapy. Nutrients 2015, 7, 8199–8226. [Google Scholar] [CrossRef]
- De Baaij, J.H.F.; Hoenderop, J.G.J.; Bindels, R.J. Magnesium in Man: Implications for Health and Disease. Physiol. Rev. 2015, 95, 1–46. [Google Scholar] [CrossRef] [PubMed]
- Costello, R.B.; Elin, R.J.; Rosanoff, A.; Wallace, T.C.; Guerrero-Romero, F.; Hruby, A.; Lutsey, P.L.; Nielsen, F.H.; Rodriguez-Moran, M.; Song, Y.; et al. Perspective: The Case for an Evidence-Based Reference Interval for Serum Magnesium: The Time Has Come. Adv. Nutr. 2016, 7, 977–993. [Google Scholar] [CrossRef]
- Lager, S.; Powell, T.L. Regulation of Nutrient Transport across the Placenta. J. Pregnancy 2012, 2012, 179827. [Google Scholar] [CrossRef] [PubMed]
- Amaral, L.M.; Wallace, K.; Owens, M.; LaMarca, B. Pathophysiology and Current Clinical Management of Preeclampsia. Curr. Hypertens. Rep. 2017, 19, 61. [Google Scholar] [CrossRef]
- Holcberg, G.; Sapir, O.; Hallak, M.; Alaa, A.; Shorok, H.-Y.; David, Y.; Katz, M.; Huleihel, M. Selective Vasodilator Effect of Magnesium Sulfate in Human Placenta. Am. J. Reprod. Immunol. 2004, 51, 192–197. [Google Scholar] [CrossRef] [PubMed]
- Dhariwal, N.K.; Lynde, G.C. Update in the Management of Patients with Preeclampsia. Anesthesiol. Clin. 2017, 35, 95–106. [Google Scholar] [CrossRef]
- Dalton, L.M.; Fhloinn, D.M.N.; Gaydadzhieva, G.T.; Mazurkiewicz, O.M.; Leeson, H.; Wright, C.P. Magnesium in pregnancy. Nutr. Rev. 2016, 74, 549–557. [Google Scholar] [CrossRef]
- Makrides, M.; Crosby, D.D.; Shepherd, E.; A Crowther, C. Magnesium supplementation in pregnancy. Cochrane Database Syst. Rev. 2014, 2019, CD000937. [Google Scholar] [CrossRef]
- Shepherd, E.; Salam, R.A.; Manhas, D.; Synnes, A.; Middleton, P.; Makrides, M.; Crowther, C.A. Antenatal magnesium sulphate and adverse neonatal outcomes: A systematic review and meta-analysis. PLOS Med. 2019, 16, e1002988. [Google Scholar] [CrossRef]
- Gimenes, J.C.; Nicoletti, C.F.; de Souza Pinhel, M.A.; de Oliveira, B.A.P.; Júnior, W.S.; Marchini, J.S.; Nonino, C.B. Pregnancy After Roux en Y Gastric Bypass: Nutritional and Biochemical Aspects. Obes. Surg. 2017, 27, 1815–1821. [Google Scholar] [CrossRef]
- Trumbo, P.; A Yates, A.; Schlicker, S.; Poos, M. Dietary Reference Intakes. J. Am. Diet. Assoc. 2001, 101, 294–301. [Google Scholar] [CrossRef] [PubMed]
- Prasad, A.S. Discovery of Human Zinc Deficiency: Its Impact on Human Health and Disease. Adv. Nutr. Int. Rev. J. 2013, 4, 176–190. [Google Scholar] [CrossRef] [PubMed]
- Roohani, N.; Hurrell, R.; Kelishadi, R.; Schulin, R. Zinc and its importance for human health: An integrative review. J. Res. Med. Sci. 2013, 18, 144–157. [Google Scholar]
- Wilson, R.L.; Grieger, J.A.; Bianco-Miotto, T.; Roberts, C.T. Association between Maternal Zinc Status, Dietary Zinc Intake and Pregnancy Complications: A Systematic Review. Nutrients 2016, 8, 641. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.B.; Houseman, J.; Seddon, L.; McMullen, E.; Tofflemire, K.; Mills, C.; Corriveau, A.; Weber, J.-P.; LeBlanc, A.; Walker, M.; et al. Maternal and umbilical cord blood levels of mercury, lead, cadmium, and essential trace elements in Arctic Canada. Environ. Res. 2006, 100, 295–318. [Google Scholar] [CrossRef]
- King, J.C. Determinants of maternal zinc status during pregnancy. Am. J. Clin. Nutr. 2000, 71, 1334S–1343S. [Google Scholar] [CrossRef]
- Hanachi, P.; Norrozi, M.; Moosavi, R.M. The Correlation of Prenatal Zinc Concentration and Deficiency with Anthropometric Factors. J. Fam. Reprod. Health 2014, 8, 21–26. [Google Scholar]
- Shen, P.-J.; Gong, B.; Xu, F.-Y.; Luo, Y. Four trace elements in pregnant women and their relationships with adverse pregnancy outcomes. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 4690–4699. [Google Scholar] [PubMed]
- Atazadegan, M.A.; Heidari-Beni, M.; Riahi, R.; Kelishadi, R. Association of selenium, zinc and copper concentrations during pregnancy with birth weight: A systematic review and meta-analysis. J. Trace Elem. Med. Biol. 2022, 69, 126903. [Google Scholar] [CrossRef]
- Rojas, P.; Gosch, M.; Basfi-Fer, K.; Carrasco, F.; Codoceo, J.; Inostroza, J.; Valencia, A.; Adjemian, D.; Rojas, J.; Díaz, E.; et al. Alopecia in women with severe and morbid obesity who undergo bariatric surgery. Nutr. Hosp. 2011, 26, 856–862. [Google Scholar] [CrossRef] [PubMed]
- Chagas, C.; Saunders, C.; Pereira, S.; Silva, J.; Saboya, C.; Ramalho, A. Vitamin A status and its relationship with serum zinc concentrations among pregnant women who have previously undergone Roux-en-Y gastric bypass. Int. J. Gynecol. Obstet. 2016, 133, 94–97. [Google Scholar] [CrossRef]
- Ducarme, G.; Planche, L.; Abet, E.; du Roure, V.D.; Ducet-Boiffard, A. A Prospective Study of Association of Micronutrients Deficiencies during Pregnancy and Neonatal Outcome among Women after Bariatric Surgery. J. Clin. Med. 2021, 10, 204. [Google Scholar] [CrossRef]
- Scheiber, I.F.; Mercer, J.F.; Dringen, R. Metabolism and functions of copper in brain. Prog. Neurobiol. 2014, 116, 33–57. [Google Scholar] [CrossRef]
- Tiffany-Castiglioni, E.; Hong, S.; Qian, Y. Copper handling by astrocytes: Insights into neurodegenerative diseases. Int. J. Dev. Neurosci. 2011, 29, 811–818. [Google Scholar] [CrossRef]
- Altarelli, M.; Ben-Hamouda, N.; Schneider, A.; Berger, M.M. Copper Deficiency: Causes, Manifestations, and Treatment. Nutr. Clin. Pract. 2019, 34, 504–513. [Google Scholar] [CrossRef] [PubMed]
- Uriu-Adams, J.Y.; Scherr, R.E.; Lanoue, L.; Keen, C.L. Influence of copper on early development: Prenatal and postnatal considerations. Biofactors 2010, 36, 136–152. [Google Scholar] [CrossRef]
- Zhang, Z.; Yuan, E.; Liu, J.; Lou, X.; Jia, L.; Li, X.; Zhang, L. Gestational age-specific reference intervals for blood copper, zinc, calcium, magnesium, iron, lead, and cadmium during normal pregnancy. Clin. Biochem. 2013, 46, 777–780. [Google Scholar] [CrossRef] [PubMed]
- Alebic-Juretic, A.; Frkovic, A. Plasma copper concentrations in pathological pregnancies. J. Trace Elem. Med. Biol. 2005, 19, 191–194. [Google Scholar] [CrossRef]
- Keen, C.L.; Uriu-Hare, J.Y.; Hawk, S.N.; Jankowski, M.; Daston, G.P.; Kwik-Uribe, C.L.; Rucker, R.B. Effect of copper deficiency on prenatal development and pregnancy outcome. Am. J. Clin. Nutr. 1998, 67, 1003S–1011S. [Google Scholar] [CrossRef]
- Saltzman, E.; Karl, J.P. Nutrient Deficiencies After Gastric Bypass Surgery. Annu. Rev. Nutr. 2013, 33, 183–203. [Google Scholar] [CrossRef]
- Gletsu-Miller, N.; Broderius, M.; Frediani, J.K.; Zhao, V.M.; Griffith, D.P.; Davis, S.S., Jr.; Sweeney, J.F.; Lin, E.; Prohaska, J.R.; Ziegler, T.R. Incidence and prevalence of copper deficiency following roux-en-y gastric bypass surgery. Int. J. Obes. 2012, 36, 328–335. [Google Scholar] [CrossRef]
- Kumar, P.; Hamza, N.; Madhok, B.; De Alwis, N.; Sharma, M.; Miras, A.D.; Mahawar, K.K. Copper Deficiency after Gastric Bypass for Morbid Obesity: A Systematic Review. Obes. Surg. 2016, 26, 1335–1342. [Google Scholar] [CrossRef]
- Balsa, J.A.; Botella-Carretero, J.I.; Gómez-Martín, J.M.; Peromingo, R.; Arrieta, F.; Santiuste, C.; Zamarrón, I.; Vázquez, C. Copper and Zinc Serum Levels after Derivative Bariatric Surgery: Differences between Roux-en-Y Gastric Bypass and Biliopancreatic Diversion. Obes. Surg. 2011, 21, 744–750. [Google Scholar] [CrossRef]
- Btaiche, I.F.; Yeh, A.Y.; Wu, I.J.; Khalidi, N. Neurologic Dysfunction and Pancytopenia Secondary to Acquired Copper Deficiency Following Duodenal Switch. Nutr. Clin. Pract. 2011, 26, 583–592. [Google Scholar] [CrossRef] [PubMed]
- Griffith, D.P.; Liff, D.A.; Ziegler, T.R.; Esper, G.J.; Winton, E.F. Acquired Copper Deficiency: A Potentially Serious and Preventable Complication Following Gastric Bypass Surgery. Obesity 2009, 17, 827–831. [Google Scholar] [CrossRef]
- Rowin, J.; Lewis, S.L. Copper deficiency myeloneuropathy and pancytopenia secondary to overuse of zinc supplementation. J. Neurol. Neurosurg. Psychiatry 2005, 76, 750–751. [Google Scholar] [CrossRef]
- Pieczyńska, J.; Grajeta, H. The role of selenium in human conception and pregnancy. J. Trace Elem. Med. Biol. 2014, 29, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Combs, J.G.F. Biomarkers of Selenium Status. Nutrients 2015, 7, 2209–2236. [Google Scholar] [CrossRef] [PubMed]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on Dietary Reference Values for selenium. EFSA J. 2014, 12, 3846. [Google Scholar] [CrossRef]
- Xu, M.; Guo, D.; Gu, H.; Zhang, L.; Lv, S. Selenium and Preeclampsia: A Systematic Review and Meta-analysis. Biol. Trace Elem. Res. 2016, 171, 283–292. [Google Scholar] [CrossRef]
- Hamdan, H.Z.; Hamdan, S.Z.; Adam, I. Association of Selenium Levels with Preeclampsia: A Systematic Review and Meta-analysis. Biol. Trace Elem. Res. 2023, 201, 2105–2122. [Google Scholar] [CrossRef] [PubMed]
- Álvarez, S.I.; Castañón, S.G.; Ruata, M.L.C.; Aragüés, E.F.; Terraz, P.B.; Irazabal, Y.G.; González, E.G.; Rodríguez, B.G. Updating of normal levels of copper, zinc and selenium in serum of pregnant women. J. Trace Elem. Med. Biol. 2007, 21, 49–52. [Google Scholar] [CrossRef]
- Bermúdez, L.; García-Vicent, C.; López, J.; Torró, M.I.; Lurbe, E. Assessment of ten trace elements in umbilical cord blood and maternal blood: Association with birth weight. J. Transl. Med. 2015, 13, 291. [Google Scholar] [CrossRef]
- Boldery, R.; Fielding, G.; Rafter, T.; Pascoe, A.L.; Scalia, G.M. Nutritional Deficiency of Selenium Secondary to Weight Loss (Bariatric) Surgery Associated with Life-Threatening Cardiomyopathy. Heart Lung Circ. 2007, 16, 123–126. [Google Scholar] [CrossRef]
- Massoure, P.-L.; Camus, O.; Fourcade, L.; Simon, F. Bilateral leg oedema after bariatric surgery: A selenium-deficient cardiomyopathy. Obes. Res. Clin. Pract. 2017, 11, 622–626. [Google Scholar] [CrossRef]
- Alasfar, F.; Ben-Nakhi, M.; Khoursheed, M.; Kehinde, E.O.; Alsaleh, M. Selenium Is Significantly Depleted Among Morbidly Obese Female Patients Seeking Bariatric Surgery. Obes. Surg. 2011, 21, 1710–1713. [Google Scholar] [CrossRef] [PubMed]
- Freeth, A.; Prajuabpansri, P.; Victory, J.M.; Jenkins, P. Assessment of Selenium in Roux-en-Y Gastric Bypass and Gastric Banding Surgery. Obes. Surg. 2012, 22, 1660–1665. [Google Scholar] [CrossRef]
- Papamargaritis, D.; Aasheim, E.T.; Sampson, B.; le Roux, C.W. Copper, selenium and zinc levels after bariatric surgery in patients recommended to take multivitamin-mineral supplementation. J. Trace Elem. Med. Biol. 2015, 31, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Eltweri, A.M.; Bowrey, D.J.; Sutton, C.D.; Graham, L.; Williams, R.N. An audit to determine if vitamin b12 supplementation is necessary after sleeve gastrectomy. Springerplus 2013, 2, 218. [Google Scholar] [CrossRef] [PubMed]
- Shahmiri, S.S.; Eghbali, F.; Ismaeil, A.; Gholizadeh, B.; Khalooeifard, R.; Valizadeh, R.; Rokhgireh, S.; Kermansaravi, M. Selenium Deficiency After Bariatric Surgery, Incidence and Symptoms: A Systematic Review and Meta-Analysis. Obes. Surg. 2022, 32, 1719–1725. [Google Scholar] [CrossRef]
- Hatch-McChesney, A.; Lieberman, H.R. Iodine and Iodine Deficiency: A Comprehensive Review of a Re-Emerging Issue. Nutrients 2022, 14, 3474. [Google Scholar] [CrossRef] [PubMed]
- Nazeri, P.; Shariat, M.; Azizi, F. Effects of iodine supplementation during pregnancy on pregnant women and their offspring: A systematic review and meta-analysis of trials over the past 3 decades. Eur. J. Endocrinol. 2021, 184, 91–106. [Google Scholar] [CrossRef]
- Michalaki, M.; Volonakis, S.; Mamali, I.; Kalfarentzos, F.; Vagenakis, A.G.; Markou, K.B. Dietary iodine absorption is not influenced by malabsorptive bariatric surgery. Obes Surg. 2014, 24, 1921–1925. [Google Scholar] [CrossRef] [PubMed]
- Lecube, A.; Zafon, C.; Gromaz, A.; Fort, J.M.; Caubet, E.; Baena, J.A.; Tortosa, F. Iodine Deficiency Is Higher in Morbid Obesity in Comparison with Late after Bariatric Surgery and Non-obese Women. Obes. Surg. 2014, 25, 85–89. [Google Scholar] [CrossRef]
- Manousou, S.; Carlsson, L.M.S.; Eggertsen, R.; Hulthén, L.; Jacobson, P.; Landin-Wilhelmsen, K.; Trimpou, P.; Svensson, P.-A.; Nyström, H.F. Iodine Status After Bariatric Surgery—A Prospective 10-Year Report from the Swedish Obese Subjects (SOS) Study. Obes. Surg. 2018, 28, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Cheah, S.; Gao, Y.; Mo, S.; Rigas, G.; Fisher, O.; Chan, D.L.; Chapman, M.G.; Talbot, M.L. Fertility, pregnancy and post partum management after bariatric surgery: A narrative review. Med. J. Aust. 2022, 216, 96–102. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Clinical Consequences of Maternal Obesity and Excess Weight Gain in Pregnancy | |
|---|---|
| Maternal | |
| Pre-conception | Higher risk of type 2 diabetes, high blood pressure, and infertility. |
| Pregnancy | Previous metabolic diseases, gestational diabetes, hypertension, deep vein thrombosis, pulmonary thromboembolism, depression. |
| Delivery | Higher risk of complications, instrumental delivery, caesarean, higher anaesthetic risk. |
| Postpartum | Infection, depression, failure in breastfeeding, weight retention, obesity |
| Newborn and infant | |
| Macrosomia, large-for-gestational-age newborn, prematurity, shoulder dystocia, birth defects, neonatal hypoglycaemia. | |
| Long term | |
| Higher risk of obesity, metabolic complications. Higher vascular risk for both the mother and offspring. | |
| Surgical Technique | Physiopathological Factors | Most Affected Micronutrients |
|---|---|---|
| Gastric banding | Decrease intake Food intolerance (meat, milk) | All micronutrients, especially those with low body stores (thiamine) Iron, zinc, calcium, vit D |
| Sleeve gastrectomy | Decrease intake Food intolerance (meat, milk) Gastrectomy | All micronutrients, especially those with low body stores (thiamine) Iron, zinc, calcium, vit D Vitamin B12, iron, calcium |
| Roux-Y gastric bypass | Decrease intake Food intolerance (meat, milk) Gastrectomy Duodenal/jejunal exclusion | All micronutrients, especially those with low body stores (thiamine) Iron, zinc, calcium, vit D Vitamin B12, iron, calcium Iron, calcium, zinc, copper, liposoluble vitamins |
| Biliopancreatic diversion duodenal switch SADI-S | Decrease intake Food intolerance (meat, milk) Gastrectomy Duodenal/jejunal exclusion Steatorrhea | All micronutrients, especially those with low body stores (thiamine) Iron, zinc, calcium, vit D Vitamin B12, iron, calcium Iron, calcium, zinc, copper, liposoluble vitamins Calcium, liposoluble vitamins |
| Micronutrient | SG/RYGB | BPD and Other Malabsorptive Procedures |
|---|---|---|
| Folate | 400–8008 μg/d 800–1000 μg/d in women of childbearing age | |
| Vitamin B12 | 350–1000 μg/d (oral or sublingual) 1000 μg/month IM-SC) | |
| Thiamine | 12 mg/d Increase to 100–300 mg if low intake, nausea/vomiting | |
| Vitamin D | 3000 UI/d (Vit D > 30 ng/mL) | A higher dose is usually needed |
| Vitamin A | 800–3000 μg/d | 3000 μg/d (10.000 UI) |
| Vitamin E | 15 mg/d | 90 mg/d |
| Vitamin K | 50–120 μg/d | 300 μg/d |
| Iron | SG: male or non-menstruating: 18 mg/d Menstruating female or RYGB/BPD: 45–60 mg/d | |
| Calcium | 1200–1500 mg/d | 1800–2400 mg/d |
| Magnesium | 350 mg/d | 350 mg/d |
| Zinc | SG: 8–11 mg/d RYGB: 8–22 mg/d | 16–22 mg/d |
| Copper | SG: 1 mg/d RYGB 2 mg/d | 2 mg/d |
| Micronutrient | Clinical Consequences of Deficiency for Maternal–Foetal Health |
|---|---|
| Folate | Neural tube defects, miscarriage, abruptio placentae, prematurity |
| Vitamin B12 | Abortion, prematurity, growth retardation, neural tube defects, cognitive impairment |
| Thiamine | Risk of thiamine deficiency in hyperemesis gravidarum |
| Vitamin D | Gestational diabetes, preeclampsia, low birth weight, long-term complications |
| Vitamin A | Foetal malformations, pulmonary dysplasia, anaemia |
| Vitamin E | Preeclampsia, neural tube defects, cognitive impairment, haemolytic disease of the newborn |
| Vitamin K | Periventricular and intraventricular haemorrhage |
| Iron | Increased maternal and foetal morbidity and mortality, miscarriage, decreased weight and foetal development |
| Zinc | Delayed foetal growth and maturation, prematurity |
| Copper | Abortion, prematurity, low weight |
| Selenium | Preeclampsia |
| Iodine | Alteration in the development of central nervous system, mental retardation |
| Micronutrient | Dose | Comment |
|---|---|---|
| Folate | 800–1000 μg | Higher dose in women with obesity (1–5 mg) |
| Vitamin B12 | 1000–2000 μg/1–3 months, i.m. | Can also be administered orally (>350–500 μg/d) |
| Thiamine | 12 mg | Increase to 100–300 mg if low intake, nausea/vomiting |
| Vitamin D | 2000–4000 UI | Vitamin D > 30 ng/mL |
| Vitamin A | 800–1500 μg | A dose below 3000 μg (10.000 UI) is safe in pregnancy; the retinol form of vitamin A should be avoided |
| Vitamin E | 15 mg | Monitoring in malabsorptive techniques |
| Vitamin K | 50–120 μg/d | Higher risk of deficiency in premature newborns |
| Iron | 100–200 mg | Ferritin > 30 mg/L, gradual increase of dose; i.v. iron is not recommended in first term |
| Calcium | 1500–2400 mg | Increase dietary intake; separated from iron supplement |
| Magnesium | 350 mg | Multivitamins usually contain a lower dose |
| Zinc | 12–30 mg | Can decrease copper absorption |
| Copper | 1–2 mg | Separated from zinc supplements |
| Selenium | 50–60 μg | Monitor in malabsorptive techniques |
| Iodine | 200–250 μg | The same dose as that in normal pregnancy |
| Pregnancy in Women with Previous Bariatric Surgery: Summary of Recommendations |
|---|
| Appropriate selection of the bariatric surgical technique. Non-malabsorptive techniques should, in general, be preferred. |
| Appropriate follow-up after bariatric surgery, with the necessary supplementation to prevent and treat possible nutritional deficiencies. |
| Preferably, the onset of pregnancy should be delayed by 12–18 months after bariatric surgery. Pre-conceptional clinical and nutritional assessment is recommended. |
| Follow-up during pregnancy should be carried out by a multidisciplinary team. |
| Close monitoring of the patient if oral tolerance is inadequate or vomiting occurs. It is advisable to increase the thiamine dose to 100–300 mg/day. |
| Monitoring of maternal weight gain and intrauterine growth. Consider oral nutritional supplements and/or pancreatic enzymes. |
| Preventive supplementation with minerals and micronutrients, at the necessary dose, depending on the type of bariatric surgery and clinical and analytical evolution. |
| Iodine recommendations are similar to those for women who have not undergone bariatric surgery. |
| Screening for gestational complications, following specific protocols. In the case of gestational diabetes, it is recommended to avoid oral glucose overload. |
| Monitoring for the occurrence of surgical complications, such as internal hernia, a serious but rare clinical condition that requires a specific diagnostic approach and treatment. |
| Encourage lactation with a close clinical and nutritional follow-up. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bretón, I.; Ballesteros-Pomar, M.D.; Calle-Pascual, A.; Alvarez-Sala, L.A.; Rubio-Herrera, M.A. Micronutrients in Pregnancy after Bariatric Surgery: A Narrative Review. J. Clin. Med. 2023, 12, 5429. https://doi.org/10.3390/jcm12165429
Bretón I, Ballesteros-Pomar MD, Calle-Pascual A, Alvarez-Sala LA, Rubio-Herrera MA. Micronutrients in Pregnancy after Bariatric Surgery: A Narrative Review. Journal of Clinical Medicine. 2023; 12(16):5429. https://doi.org/10.3390/jcm12165429
Chicago/Turabian StyleBretón, Irene, María D. Ballesteros-Pomar, Alfonso Calle-Pascual, Luis Antonio Alvarez-Sala, and Miguel Angel Rubio-Herrera. 2023. "Micronutrients in Pregnancy after Bariatric Surgery: A Narrative Review" Journal of Clinical Medicine 12, no. 16: 5429. https://doi.org/10.3390/jcm12165429
APA StyleBretón, I., Ballesteros-Pomar, M. D., Calle-Pascual, A., Alvarez-Sala, L. A., & Rubio-Herrera, M. A. (2023). Micronutrients in Pregnancy after Bariatric Surgery: A Narrative Review. Journal of Clinical Medicine, 12(16), 5429. https://doi.org/10.3390/jcm12165429