

Incidence and Outcomes of Valve-in-Valve Transcatheter Aortic Valve Implantation in Failed Bioprosthetic Valves

 ,
,  , ,
, ,
Abstract
:Highlights
- Transcatheter aortic valve replacement (TAVR) has become the standard of care beside sur-gical valve replacement (SAVR) in the majority of patients with aortic stenosis (AS) among all risk categories and is the preferred treatment of choice in older patients.
- Bioprosthetic valve failure is an ongoing issue necessitating reoperations or valve-in-valve interventions.
- As redo-SAVR is related to elevated peri-procedural risks and mortality, valve-in-valve in-terventions are expected to increase in the future.
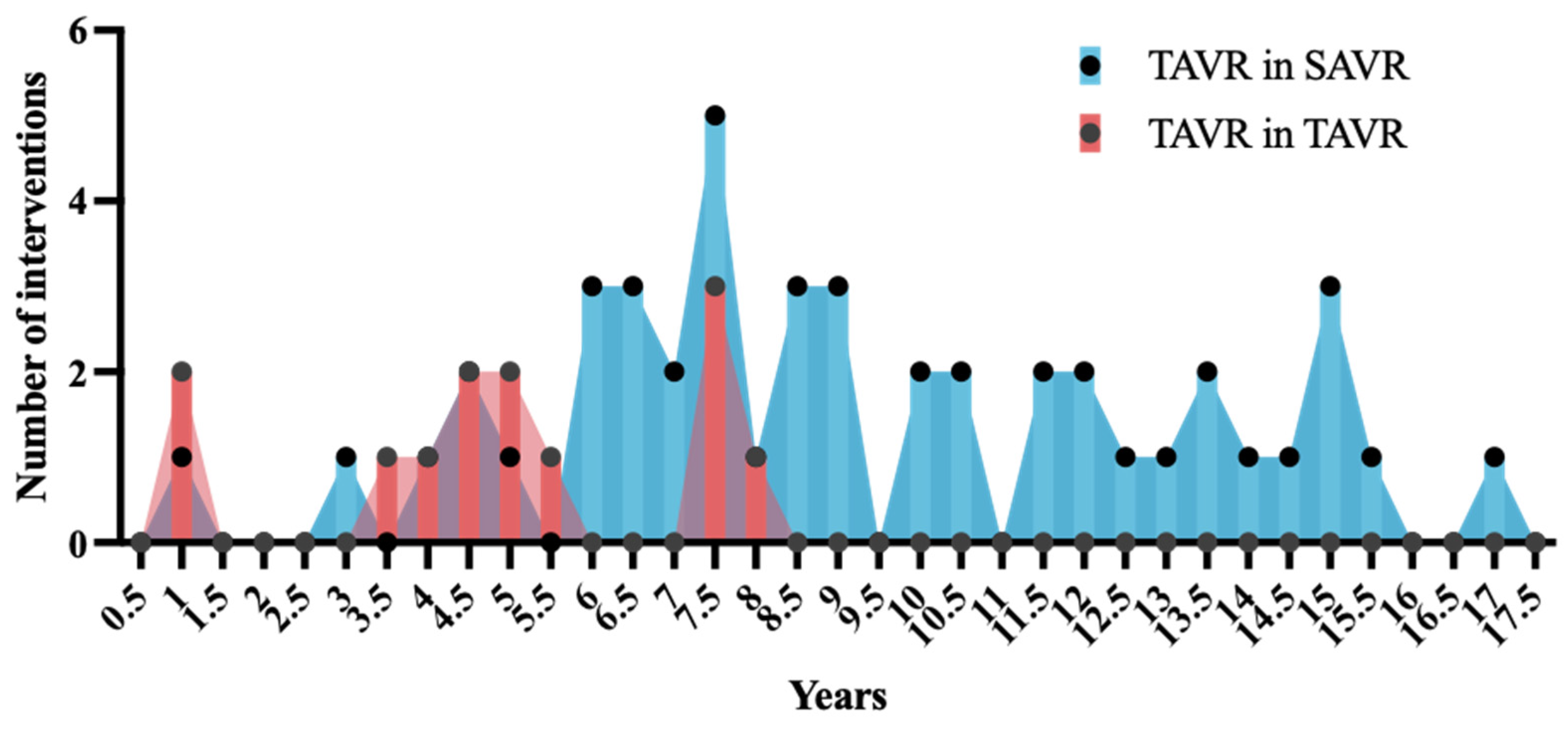
- Over the last decade, a steep increase in valve-in-valve procedures was observed, resulting in an incidence of 4% among TAVR procedures.
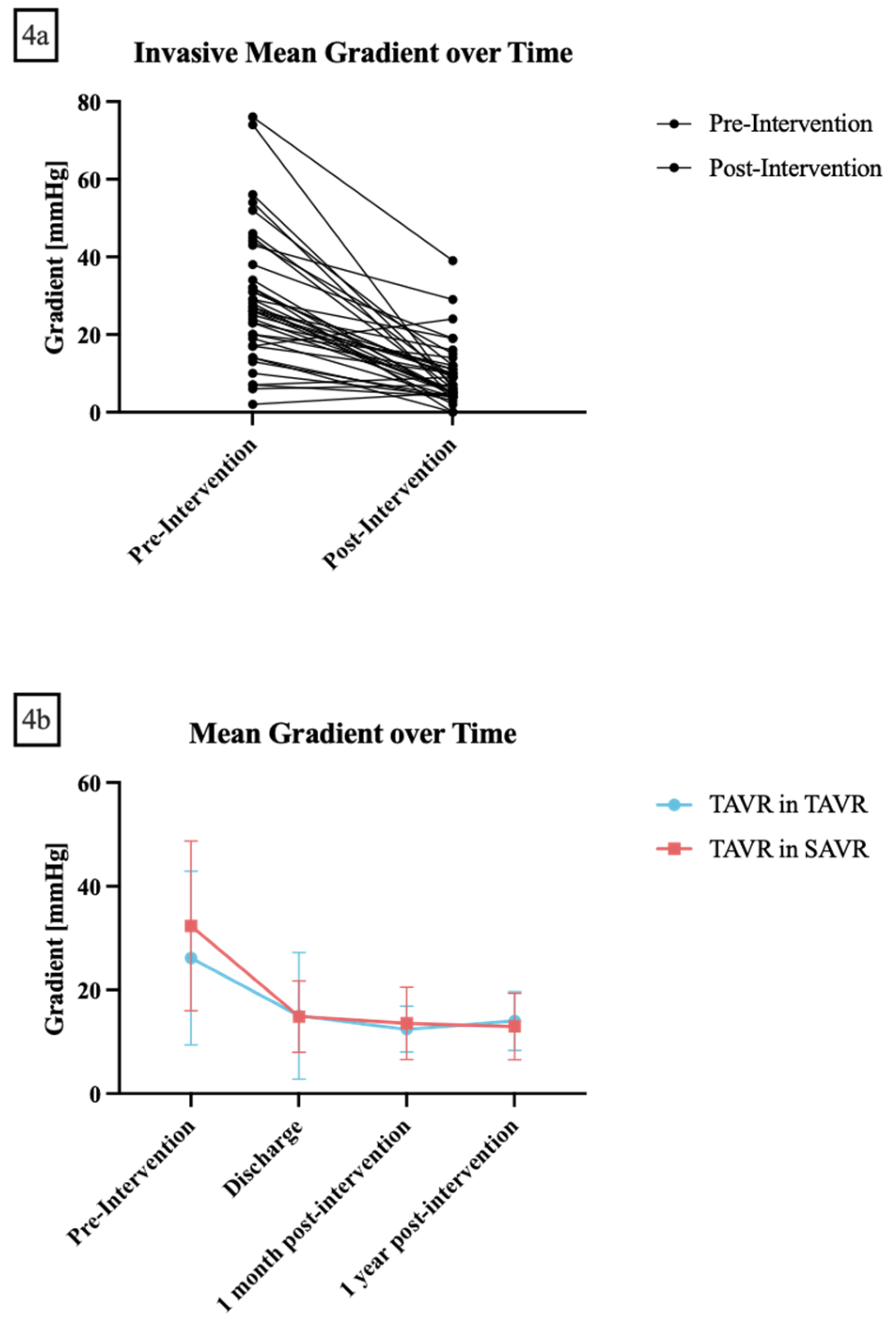
- Valve-in-valve interventions are feasible and showed lasting improvements in mean aortic valve gradients.
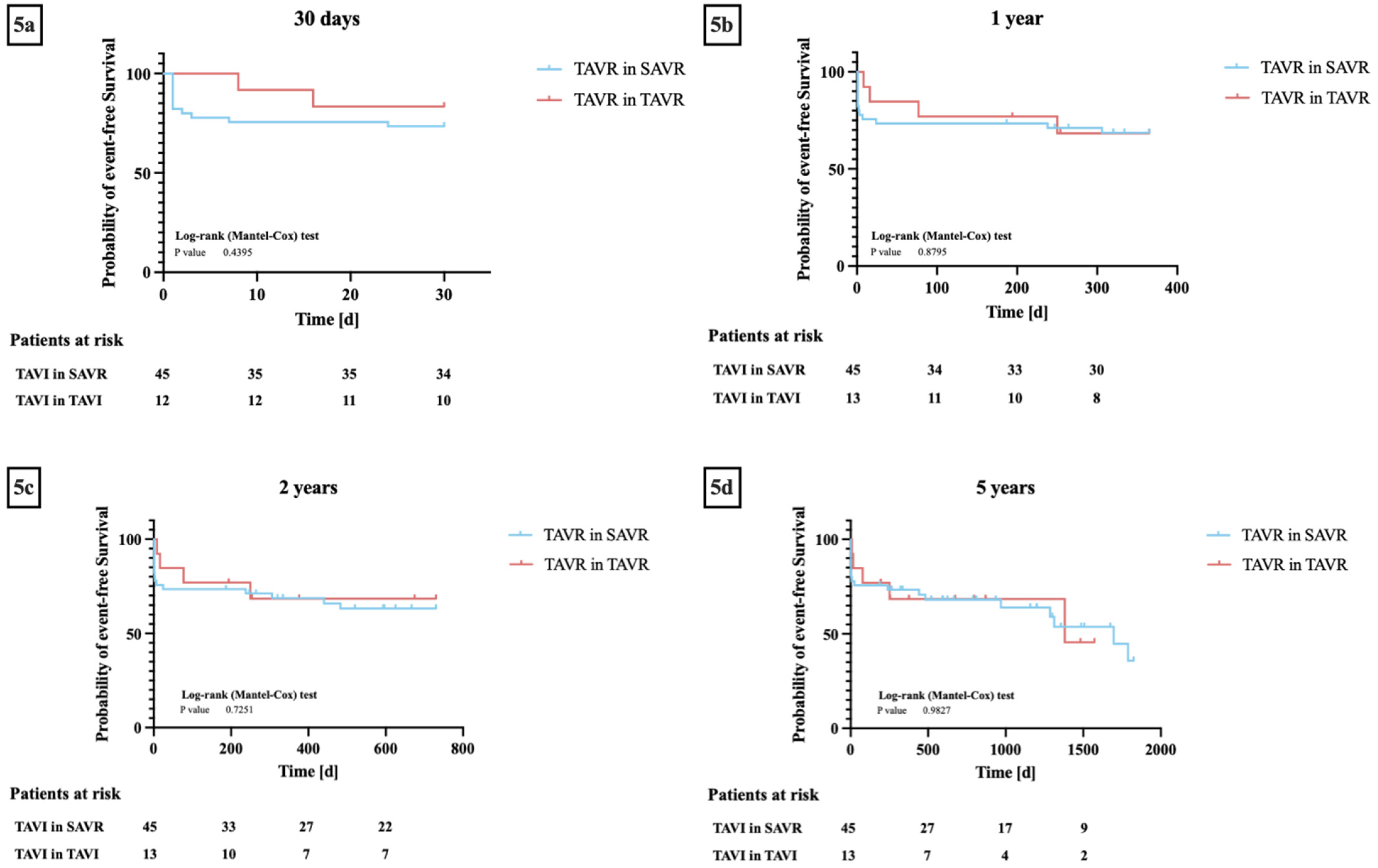
- No differences in technical and device successes or event-free survival between TAVR-in-SAVR and TAVR-in-TAVR could be observed.
Abstract
1. Introduction
2. Methods
2.1. Study Design and Patient Cohort
2.2. Data Collection and Clinical Endpoints
2.3. Statistical Analysis
3. Results
3.1. Patient Cohort and Baseline Characteristics
3.2. Incidence and Trends of Valve-in-Valve Procedures
3.3. Procedural Characteristics
3.4. Procedural Outcomes
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AS | aortic stenosis |
| CT | computed tomography |
| ECG | electrocardiogram |
| eGFR | estimated glomerular filtration rate |
| EuroSCORE | European System for Cardiac Operative Risk Evaluation |
| LVEF | left ventricular ejection fraction |
| SAVR | surgical aortic valve replacement |
| TAVR | transcatheter aortic valve replacement |
| TiSAVR | TAVR in SAVR |
| TiTAVR | TAVR in TAVR |
| TTE | transthoracic echocardiography |
| VARC | Valve Academic Research Consortium |
References
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P.; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 143, e72–e227. [Google Scholar] [CrossRef]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef] [PubMed]
- Kundi, H.; Strom, J.B.; Valsdottir, L.R.; Elmariah, S.; Popma, J.J.; Shen, C.; Yeh, R.W. Trends in Isolated Surgical Aortic Valve Replacement According to Hospital-Based Transcatheter Aortic Valve Replacement Volumes. JACC Cardiovasc. Interv. 2018, 11, 2148–2156. [Google Scholar] [CrossRef]
- Sharma, T.; Krishnan, A.M.; Lahoud, R.; Polomsky, M.; Dauerman, H.L. National Trends in TAVR and SAVR for Patients With Severe Isolated Aortic Stenosis. J. Am. Coll. Cardiol. 2022, 80, 2054–2056. [Google Scholar] [CrossRef] [PubMed]
- UK TAVI Trial Investigators; Toff, W.D.; Hildick-Smith, D.; Kovac, J.; Mullen, M.J.; Wendler, O.; Mansouri, A.; Rombach, I.; Abrams, K.R.; Conroy, S.P.; et al. Effect of Transcatheter Aortic Valve Implantation vs Surgical Aortic Valve Replacement on All-Cause Mortality in Patients with Aortic Stenosis: A Randomized Clinical Trial. JAMA 2022, 327, 1875–1887. [Google Scholar] [CrossRef]
- Bapat, V.N.; Zaid, S.; Fukuhara, S.; Saha, S.; Vitanova, K.; Kiefer, P.; Squiers, J.J.; Voisine, P.; Pirelli, L.; von Ballmoos, M.W.; et al. Surgical Explantation After TAVR Failure: Mid-Term Outcomes From the EXPLANT-TAVR International Registry. JACC Cardiovasc. Interv. 2021, 14, 1978–1991. [Google Scholar] [CrossRef]
- Tang, G.H.L.; Zaid, S.; Kleiman, N.S.; Goel, S.S.; Fukuhara, S.; Marin-Cuartas, M.; Kiefer, P.; Abdel-Wahab, M.; De Backer, O.; Søndergaard, L.; et al. Explant vs Redo-TAVR After Transcatheter Valve Failure: Mid-Term Outcomes From the EXPLANTORREDO-TAVR International Registry. JACC Cardiovasc. Interv. 2023, 16, 927–941. [Google Scholar] [CrossRef]
- Al-Abcha, A.; Saleh, Y.; Boumegouas, M.; Prasad, R.; Herzallah, K.; Baloch, Z.Q.; Abdelkarim, O.; Rayamajhi, S.; Abela, G.S. Meta-Analysis of Valve-in-Valve Transcatheter Aortic Valve Implantation Versus Redo-surgical Aortic Valve Replacement in Failed Bioprosthetic Aortic Valve. Am. J. Cardiol. 2021, 146, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Spaziano, M.; Mylotte, D.; Thériault-Lauzier, P.; De Backer, O.; Søndergaard, L.; Bosmans, J.; Debry, N.; Modine, T.; Barbanti, M.; Tamburino, C.; et al. Transcatheter aortic valve implantation versus redo surgery for failing surgical aortic bioprostheses: A multicentre propensity score analysis. EuroIntervention 2017, 13, 1149–1156. [Google Scholar] [CrossRef] [PubMed]
- Gatta, F.; Haqzad, Y.; Gradinariu, G.; Malvindi, P.G.; Khalid, Z.; Suelo-Calanao, R.L.; Moawad, N.; Bashir, A.; Rogers, L.J.; Lloyd, C.; et al. Redo aortic valve replacement vs valve-in-valve trans-catheter aortic valve implantation: A UK propensity-matched analysis. Monaldi Arch. Chest Dis. 2023. [Google Scholar] [CrossRef] [PubMed]
- Pilgrim, T.; Franzone, A.; Stortecky, S.; Nietlispach, F.; Haynes, A.G.; Tueller, D.; Toggweiler, S.; Muller, O.; Ferrari, E.; Noble, S.; et al. Predicting Mortality After Transcatheter Aortic Valve Replacement: External Validation of the Transcatheter Valve Therapy Registry Model. Circ. Cardiovasc. Interv. 2017, 10, e005481. [Google Scholar] [CrossRef]
- Stortecky, S.; Heg, D.; Tueller, D.; Pilgrim, T.; Muller, O.; Noble, S.; Jeger, R.; Toggweiler, S.; Ferrari, E.; Taramasso, M.; et al. Infective Endocarditis After Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2020, 75, 3020–3030. [Google Scholar] [CrossRef]
- Attinger-Toller, A.; Ferrari, E.; Tueller, D.; Templin, C.; Muller, O.; Nietlispach, F.; Toggweiler, S.; Noble, S.; Roffi, M.; Jeger, R.; et al. Age-Related Outcomes After Transcatheter Aortic Valve Replacement: Insights From the SwissTAVI Registry. JACC Cardiovasc. Interv. 2021, 14, 952–960. [Google Scholar] [CrossRef]
- VARC-3 WRITING COMMITTEE; Généreux, P.; Piazza, N.; Alu, M.C.; Nazif, T.; Hahn, R.T.; Pibarot, P.; Bax, J.J.; Leipsic, J.A.; Blanke, P.; et al. Valve Academic Research Consortium 3: Updated endpoint definitions for aortic valve clinical research. Eur. Heart J. 2021, 42, 1825–1857. [Google Scholar] [CrossRef] [PubMed]
- Nalluri, N.; Atti, V.; Munir, A.B.; Karam, B.; Patel, N.J.; Kumar, V.; Vemula, P.; Edla, S.; Asti, D.; Paturu, A.; et al. Valve in valve transcatheter aortic valve implantation (ViV-TAVI) versus redo-Surgical aortic valve replacement (redo-SAVR): A systematic review and meta-analysis. J. Interv. Cardiol. 2018, 31, 661–671. [Google Scholar] [CrossRef] [PubMed]
- Raschpichler, M.C.; Woitek, F.; Chakravarty, T.; Flint, N.; Yoon, S.-H.; Mangner, N.; Patel, C.G.; Singh, C.; Kashif, M.; Kiefer, P.; et al. Valve-in-Valve for Degenerated Transcatheter Aortic Valve Replacement Versus Valve-in-Valve for Degenerated Surgical Aortic Bioprostheses: A 3-Center Comparison of Hemodynamic and 1-Year Outcome. J. Am. Heart Assoc. 2020, 9, e013973. [Google Scholar] [CrossRef]
- Fukuhara, S.; Brescia, A.A.; Shiomi, S.; Rosati, C.M.; Yang, B.; Kim, K.M.; Deeb, G.M. Surgical explantation of transcatheter aortic bioprostheses: Results and clinical implications. J. Thorac. Cardiovasc. Surg. 2021, 162, 539–547.e1. [Google Scholar] [CrossRef] [PubMed]
- Webb, J.G.; Blanke, P.; Meier, D.; Sathananthan, J.; Lauck, S.; Chatfield, A.G.; Jelisejevas, J.; Wood, D.A.; Akodad, M. TAVI in 2022: Remaining issues and future direction. Arch. Cardiovasc. Dis. 2022, 115, 235–242. [Google Scholar] [CrossRef]
- Landes, U.; Webb, J.G.; De Backer, O.; Sondergaard, L.; Abdel-Wahab, M.; Crusius, L.; Kim, W.-K.; Hamm, C.; Buzzatti, N.; Montorfano, M.; et al. Repeat Transcatheter Aortic Valve Replacement for Transcatheter Prosthesis Dysfunction. J. Am. Coll. Cardiol. 2020, 75, 1882–1893. [Google Scholar] [CrossRef]
- Landes, U.; Sathananthan, J.; Witberg, G.; De Backer, O.; Sondergaard, L.; Abdel-Wahab, M.; Holzhey, D.; Kim, W.-K.; Hamm, C.; Buzzatti, N.; et al. Transcatheter Replacement of Transcatheter Versus Surgically Implanted Aortic Valve Bioprostheses. J. Am. Coll. Cardiol. 2021, 77, 1–14. [Google Scholar] [CrossRef]
- Makkar, R.R.; Kapadia, S.; Chakravarty, T.; Cubeddu, R.; Mahoney, P.; Yadav, P.; Iyer, P.; Kaneko, Y.; Kodali, S.; Mack, M.; et al. Outcomes of Repeat TAVR with Balloon-Expandable SAPIEN 3/Ultra Valves. tctMD. Available online: https://www.tctmd.com/slide/outcomes-repeat-tavr-balloon-expandable-sapien-3ultra-valves (accessed on 15 May 2023).
- Tarantini, G.; Delgado, V.; de Backer, O.; Sathananthan, J.; Treede, H.; Saia, F.; Blackman, D.; Parma, R. Redo-Transcatheter Aortic Valve Implantation Using the SAPIEN 3/Ultra Transcatheter Heart Valves-Expert Consensus on Procedural Planning and Techniques. Am. J. Cardiol. 2023, 192, 228–244. [Google Scholar] [CrossRef] [PubMed]
- Sá, M.P.B.O.; Van den Eynde, J.; Simonato, M.; Cavalcanti, L.R.P.; Doulamis, I.P.; Weixler, V.; Kampaktsis, P.N.; Gallo, M.; Laforgia, P.L.; Zhigalov, K.; et al. Valve-in-Valve Transcatheter Aortic Valve Replacement Versus Redo Surgical Aortic Valve Replacement: An Updated Meta-Analysis. JACC Cardiovasc. Interv. 2021, 14, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Thandra, A.; Abusnina, W.; Jhand, A.; Shaikh, K.; Bansal, R.; Pajjuru, V.S.; Al-Abdouh, A.; Kanmanthareddy, A.; Alla, V.M. Valve-in-valve transcatheter aortic valve replacement versus redo surgical valve replacement for degenerated bioprosthetic aortic valve: An updated meta-analysis comparing midterm outcomes. Catheter. Cardiovasc. Interv. 2021, 97, 1481–1488. [Google Scholar] [CrossRef] [PubMed]
- Dvir, D.; Leipsic, J.; Blanke, P.; Ribeiro, H.B.; Kornowski, R.; Pichard, A.; Rodés-Cabau, J.; Wood, D.A.; Stub, D.; Ben-Dor, I.; et al. Coronary obstruction in transcatheter aortic valve-in-valve implantation: Preprocedural evaluation, device selection, protection, and treatment. Circ. Cardiovasc. Interv. 2015, 8, e002079. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, E.; Stortecky, S.; Heg, D.; Muller, O.; Nietlispach, F.; Tueller, D.; Toggweiler, S.; Noble, S.; Maisano, F.; Roffi, M.; et al. The hospital results and 1-year outcomes of transcatheter aortic valve-in-valve procedures and transcatheter aortic valve implantations in the native valves: The results from the Swiss-TAVI Registry. Eur. J. Cardiothorac. Surg. 2019, 56, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Raschpichler, M.; de Waha, S.; Holzhey, D.; Schwarzer, G.; Flint, N.; Kaewkes, D.; Bräuchle, P.T.; Dvir, D.; Makkar, R.; Ailawadi, G.; et al. Valve-in-Valve Transcatheter Aortic Valve Replacement Versus Redo Surgical Aortic Valve Replacement for Failed Surgical Aortic Bioprostheses: A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2022, 11, e7965. [Google Scholar] [CrossRef]
- Calabrò, P.; Gragnano, F.; Niccoli, G.; Marcucci, R.; Zimarino, M.; Spaccarotella, C.; Renda, G.; Patti, G.; Andò, G.; Moscarella, E.; et al. Antithrombotic Therapy in Patients Undergoing Transcatheter Interventions for Structural Heart Disease. Circulation 2021, 144, 1323–1343. [Google Scholar] [CrossRef]
- Webb, J.G.; Mack, M.J.; White, J.M.; Dvir, D.; Blanke, P.; Herrmann, H.C.; Leipsic, J.; Kodali, S.K.; Makkar, R.; Miller, D.C.; et al. Transcatheter Aortic Valve Implantation Within Degenerated Aortic Surgical Bioprostheses: PARTNER 2 Valve-in-Valve Registry. J. Am. Coll. Cardiol. 2017, 69, 2253–2262. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Basic Characteristics | Patients (N = 58) |
| Female, n (%) | 26 (45%) |
| Age, years | 79 ± 9.4 |
| Body mass index, kg/m2 | 26.8 ± 5.5 |
| LVEF, % | 51.0 ± 13.8 |
| EuroSCORE, % | 8.7 ± 8.5 |
| Preconditions | Patients (N = 58) |
| Diabetes, n (%) | 21 (36%) |
| Dyslipidemia, n (%) | 35 (60%) |
| Hypertension, n (%) | 47 (81%) |
| Coronary artery disease, n (%) | 38 (66%) |
| Myocardial infarction, n (%) | 14 (24%) |
| eGFR (CKD-EPI), mL/min | 50.1 ± 24.1 |
| Hemoglobin, g/L | 121.0 ± 22.0 |
| Previous Interventions, n (%) | Patients (N = 58) |
| Any heart surgery | 50 (86%) |
| Surgical aortic valve replacement | 46 (79%) |
| Coronary artery bypass grafting | 19 (33%) |
| Transcatheter aortic valve replacement | 13 (22%) |
| Prior pacemaker | 11 (19%) |
| Percutaneous coronary intervention | 22 (38%) |
| ECG Characteristics, n (%) | Patients (N = 58) |
| No changes | 23 (40%) |
| Right or left bundle branch block | 10 (17%) |
| Any AV block | 6 (10%) |
| Atrial fibrillation | 18 (31%) |
| Paced rhythm | 4 (7%) |
| Echocardiography Parameters | Patients (N = 46) |
| LVEF, % | 51.0 ± 13.8 |
| Aortic valve mean gradient, mmHg | 31.0 ± 16.5 |
| Aortic valve peak gradient, mmHg | 50.8 ± 24.6 |
| Aortic valve area, cm2 | 0.95 ± 0.46 |
| Reason for ViV-TAVI, n (%) | Patients (N = 58) |
| Prosthetic regurgitation | |
| ≤Mild | 0 (0%) |
| >Mild | 17 (29%) |
| Prosthetic stenosis | 28 (48%) |
| Combined regurgitation and stenosis | 10 (17%) |
| Old device Type, n (%) | Patients (N = 58) |
| SAVR | 45 (78%) |
| TAVI | 13 (22%) |
| Device size | |
| ≤25 mm | 39 (67%) |
| >25 mm | 19 (33%) |
| New Device Type, n (%) | Patients (N = 58) |
| Balloon-expandable | 23 (40%) |
| Self-expanding | 35 (60%) |
| Mechanically expanding | 0 (0%) |
| Device size | |
| ≤25 mm | 33 (57%) |
| >25 mm | 25 (43%) |
| Procedural Measurements | Patients (N = 46) |
| Invasive gradients (mmHg) | |
| Preprocedural mean | 27.2 ± 17.2 |
| Preprocedural peak | 35.7 ± 26.1 |
| Postprocedural mean | 9.5 ± 7.6 |
| Postprocedural peak | 10.7 ± 10.0 |
| Time between valve interventions (years) | 8.6 ± 3.9 |
| Post-Procedural Echo Gradients (mmHg) | Patients |
| 1 month post-procedural, n | 13.3 ± 6.4, 37 |
| 1 year post-procedural, n | 13.2 ± 6.3, 21 |
| Complications, n (%) | Patients (N = 58) |
|---|---|
| No complications | 39 (67%) |
| Death | |
| Procedural death | 1 (2%) |
| Procedural reanimation | 4 (7%) |
| In-hospital death | 2 (4%) |
| Coronary occlusion | 0 (0%) |
| Stroke | 0 (0%) |
| Transient ischemic attack | 1 (2%) |
| Permanent pace maker | 4 (7%) |
| Myocardial infarction | 0 (0%) |
| Vascular complication | |
| Major complication (stent or surgery) | 3(5%) |
| Minor complication (compression, ballooning, blood transfusion) | 5(9%) |
| Valve embolization | 2 (4%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stolte, T.; Boeddinghaus, J.; Allegra, G.; Leibundgut, G.; Reuthebuch, O.; Kaiser, C.; Müller, C.; Nestelberger, T. Incidence and Outcomes of Valve-in-Valve Transcatheter Aortic Valve Implantation in Failed Bioprosthetic Valves. J. Clin. Med. 2023, 12, 5868. https://doi.org/10.3390/jcm12185868
Stolte T, Boeddinghaus J, Allegra G, Leibundgut G, Reuthebuch O, Kaiser C, Müller C, Nestelberger T. Incidence and Outcomes of Valve-in-Valve Transcatheter Aortic Valve Implantation in Failed Bioprosthetic Valves. Journal of Clinical Medicine. 2023; 12(18):5868. https://doi.org/10.3390/jcm12185868
Chicago/Turabian StyleStolte, Thorald, Jasper Boeddinghaus, Giampiero Allegra, Gregor Leibundgut, Oliver Reuthebuch, Christoph Kaiser, Christian Müller, and Thomas Nestelberger. 2023. "Incidence and Outcomes of Valve-in-Valve Transcatheter Aortic Valve Implantation in Failed Bioprosthetic Valves" Journal of Clinical Medicine 12, no. 18: 5868. https://doi.org/10.3390/jcm12185868
APA StyleStolte, T., Boeddinghaus, J., Allegra, G., Leibundgut, G., Reuthebuch, O., Kaiser, C., Müller, C., & Nestelberger, T. (2023). Incidence and Outcomes of Valve-in-Valve Transcatheter Aortic Valve Implantation in Failed Bioprosthetic Valves. Journal of Clinical Medicine, 12(18), 5868. https://doi.org/10.3390/jcm12185868