
Umbilical Granuloma: Frequency, Associated Factors, 10-Year Treatment Trends, and Effectiveness at a Single Hospital in Japan


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Data Collection
2.2. Ethical Approval
2.3. Collection of Seasonal and Meteorological Data
2.4. Routine Umbilical Care and Treatment Strategies for Umbilical Granuloma
2.4.1. Silver Nitrate Cauterization
2.4.2. Topical Steroid Application
2.4.3. Ethanol Disinfectant
2.4.4. Ligation
2.4.5. Treatment Outcomes
2.5. Statistical Analysis
3. Results
3.1. Samples
3.2. Incidence of Umbilical Granuloma and Associated Factors
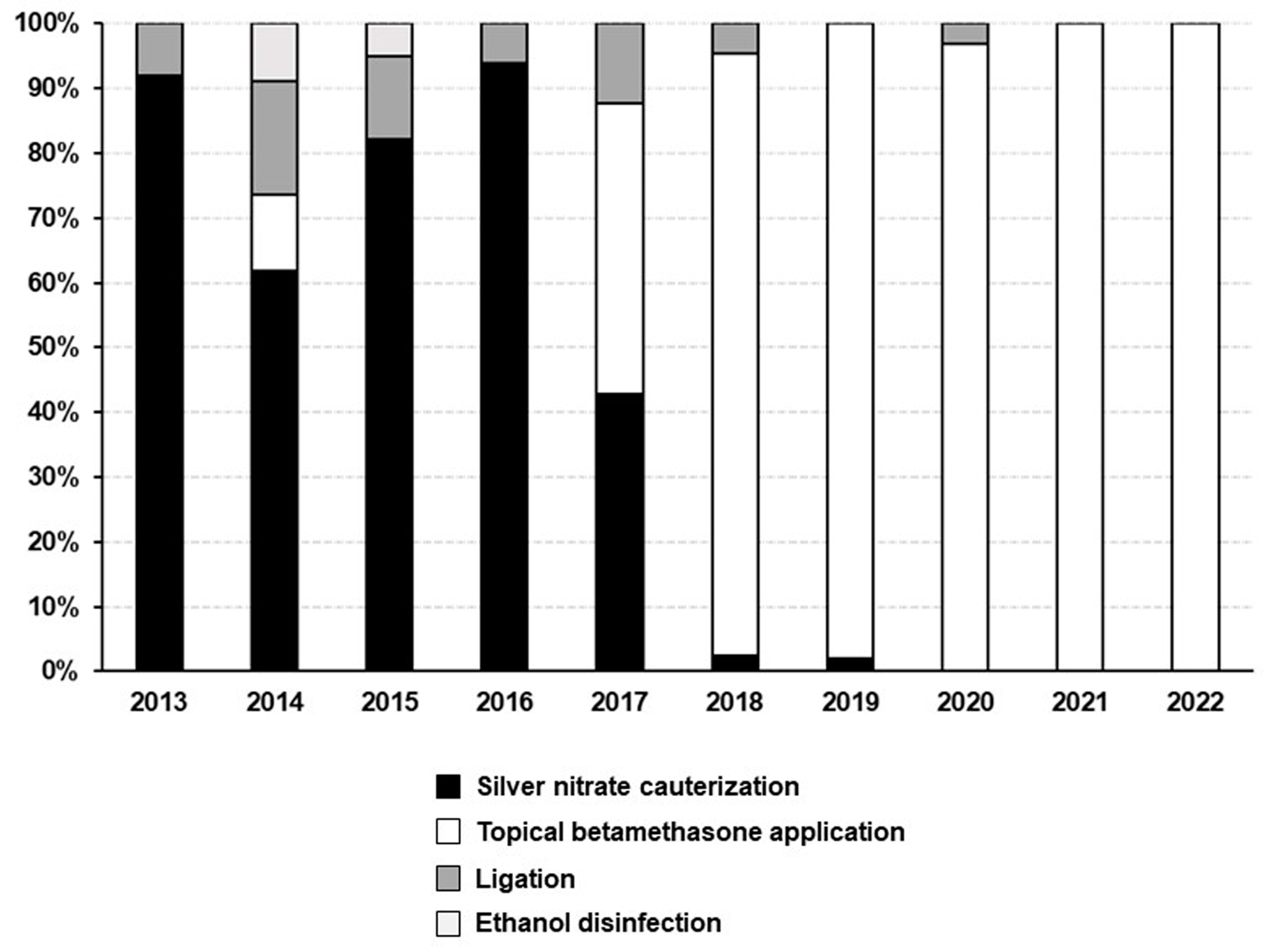
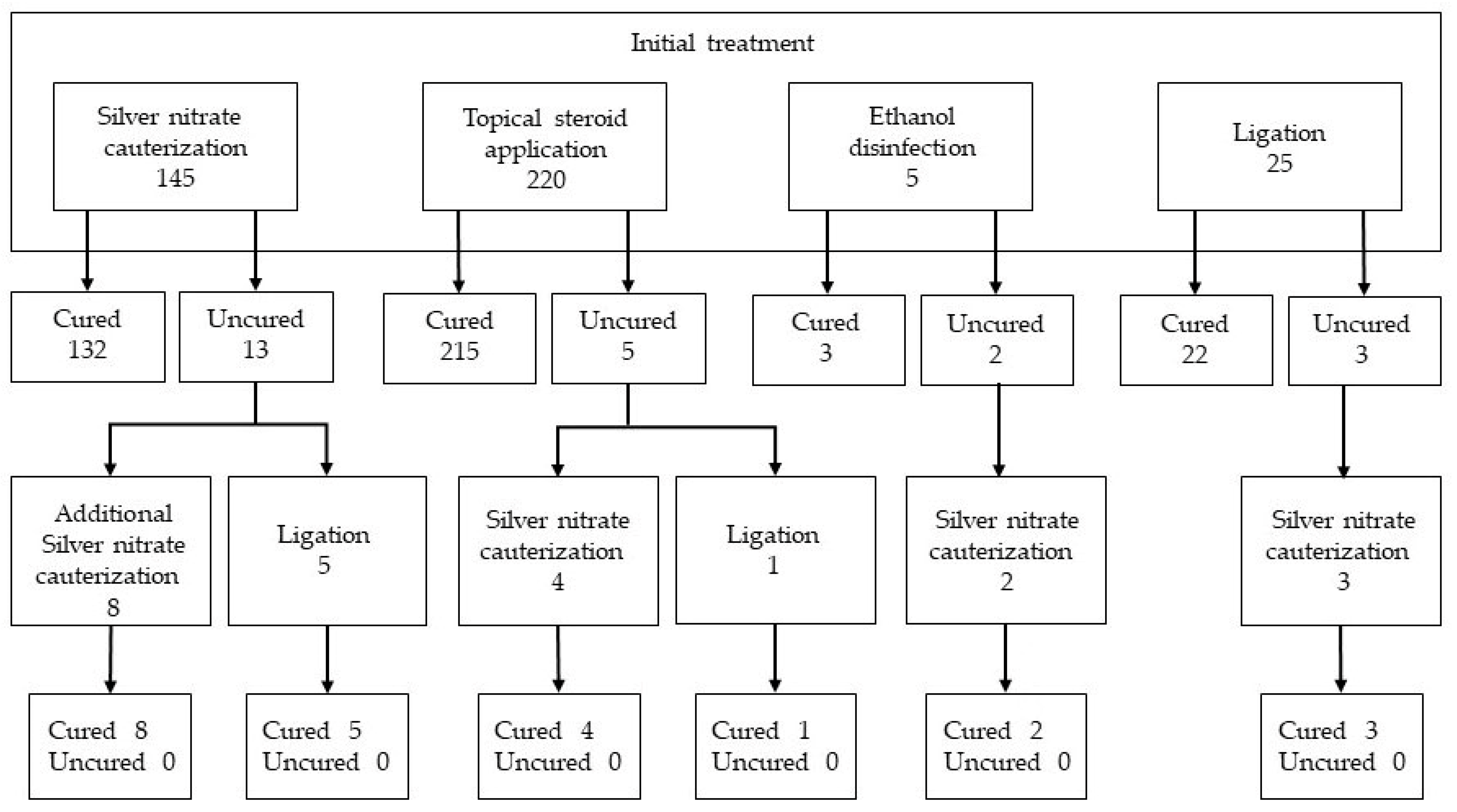
3.3. Umbilical Granuloma Treatment and Its Effectiveness
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nathan, A.T. The umbilicus. In Nelson Textbook of Pediatrics, 21st ed.; Kliegman, R.M., St Geme, J.W., III, Eds.; Elsevier: Philadelphia, PA, USA, 2020; pp. 975–976. [Google Scholar]
- Muniraman, H.; Sardesai, T.; Sardesai, S. Disorders of the umbilical cord. Pediatr. Rev. 2018, 39, 332–341. [Google Scholar] [CrossRef] [PubMed]
- Tülin, Ö.; Muhammet, A. Umbilical granuloma frequency of newborns in Third-line Hospital in Turkey. Afr. Health Sci. 2022, 22, 560–564. [Google Scholar] [CrossRef] [PubMed]
- McCallum, D.I.; Hall, G.F. Umbilical granulomata with particular reference to talc granuloma. Br. J. Dermatol. 1970, 83, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Al Siny, F.I.; Al Mansouri, N.I.; Al Zahrani, F.S. Proximal Clamping of Umbilical Cord and Prevention of Umbilical Granuloma (Preliminary Results). KAU Med. Sci. 2004, 11, 3–7. [Google Scholar]
- Rakotomalala, J.H.; Poenaru, D.; Mayforth, R.D. Disorders of the Umbilicus. In Paediatric Surgery: A Comprehensive Text for Africa; Ameh, E.A., Bickler, S.W., Lakhoo, K., Nwomeh, B.C., Poenaru, D., Eds.; Global HELP Organization: Seattle, WA, USA, 2011; pp. 352–357. [Google Scholar]
- Lotan, G.; Klin, B.; Efrati, Y. Double-ligature: A treatment for pedunculated umbilical granulomas in children. Am. Fam. Physician. 2002, 65, 2067–2068. [Google Scholar]
- Karagüzel, G.; Aldemir, H. Umbilical granuloma: Modern understanding of etiopathogenesis, diagnosis, and management. J. Pediatr. Neonatal. Care 2016, 4, 00136. [Google Scholar] [CrossRef]
- Fahmy, M. Umbilical granuloma (UG). In Umbilicus and Umbilical Cord; Springer International Publishing: Berlin/Heidelberg, Germany, 2018; pp. 133–143. [Google Scholar]
- Japan Meteorological Agency. Weather, Climate & Earthquake Information. Available online: www.jma.go.jp/jma/indexe.html (accessed on 7 June 2023).
- Matsukawa, Y.; Yoshitoshi, E.Y.; Wakasa, T. Clinical features and differential diagnosis of umbilical polyp and umbilical granuloma. J. Jpn Soc. Pediatr. Surg. 2010, 46, 935–940. (In Japanese) [Google Scholar]
- Kim, D.H.; Lee, H.J.; Kim, J.Y.; Jung, H.R. Differential diagnosis of umbilical polyps and granulomas in children: Sonographic and pathologic correlations. Ultrasonography 2021, 40, 248–255. [Google Scholar] [CrossRef]
- Assi, A.N.; Kadem, M.K.; Alrubaee, R.J.; Atshan, F.G. Management of umbilical granuloma. Thi-Qar. Med. J. 2010, 4, 82–87. [Google Scholar]
- Farahani, L.A.; Mohammadzade, A.; Tafazzoli, M.; Esmaeli, H.; Ghazvini, K. Effect of topical application of breast milk and dry cord care on bacterial colonization and umbilical cord separation time in neonates. J. Chin. Clin. Med. 2008, 3, 327–332. [Google Scholar]
- Kapellen, T.M.; Gebauer, C.M.; Brosteanu, O.; Labitzke, B.; Vogtmann, C.; Kiess, W. Higher rate of cord-related adverse events in neonates with dry umbilical cord care compared to chlorhexidine powder. Results of a randomized controlled study to compare efficacy and safety of chlorhexidine powder versus dry care in umbilical cord care of the newborn. Neonatology 2009, 96, 13–18. [Google Scholar] [CrossRef] [PubMed]
- López-Medina, M.D.; López-Araque, A.B.; Linares-Abad, M.; López-Medina, I.M. Umbilical cord separation time, predictors and healing complications in newborns with dry care. PLoS ONE 2020, 15, e0227209. [Google Scholar] [CrossRef] [PubMed]
- Quattrin, R.; Iacobucci, K.; De Tina, A.L.; Gallina, L.; Pittini, C.; Brusaferro, S. 70% alcohol versus dry cord care in the umbilical cord care: A case-control study in Italy. Medicine 2016, 95, e3207. [Google Scholar] [CrossRef]
- Gallina, L.; De Tina, A.L.; Basso, T.; Brusaferro, S.; Quattrin, R. Umbilical cord care after the first day from birth: A case control study in a northeastern Italian hospital. Pediatr. Neonatal. Nurs Open J. 2016, 3, 4–9. [Google Scholar] [CrossRef]
- Fiaz, M.; Bhatti, A.B.; Ahmed, N.; Ahmed, R.R. Comparative study of the therapeutic effects of copper sulphate versus common salt (sodium chloride) in the treatment of infantile umbilical granuloma. J. Med. Sci. Clin. Res. 2017, 5, 31127–31132. [Google Scholar] [CrossRef]
- Pomeranz, A. Anomalies, abnormalities, and care of the umbilicus. Pediatr. Clin. North Am. 2004, 51, 819–827. [Google Scholar] [CrossRef]
- Kim-Fine, S.; Regnault, T.R.H.; Lee, J.S.; Gimbel, S.A.; Greenspoon, J.A.; Fairbairn, J.; Summers, K.; De Vrijer, B. Male gender promotes an increased inflammatory response to lipopolysaccharide in umbilical vein blood. J. Matern. Fetal. Neonatal. Med. 2012, 25, 2470–2474. [Google Scholar] [CrossRef]
- Koch, F.R.; Wagner, C.L.; Jenkins, D.D.; Caplan, M.J.; Perkel, J.K.; Rollins, L.G.; Katikaneni, L.D.; Mulvihill, D.M. Sex differences in cerebral blood flow following chorioamnionitis in healthy term infants. J. Perinatol. 2014, 34, 197–202. [Google Scholar] [CrossRef]
- Carr, B.L.; Copnell, B.; McIntyre, M. Differences in meconium stained amniotic fluid in an Australian population: A retrospective study. Women Birth 2019, 32, e259–e263. [Google Scholar] [CrossRef]
- Shakya, P.; Yadav, M.K.; Poudel, S. Meconium-stained amniotic fluid among term deliveries in a tertiary care centre: A descriptive cross-sectional study. JNMA J. Nepal. Med. Assoc. 2022, 60, 672–675. [Google Scholar] [CrossRef]
- Nagar, H. Umbilical granuloma: A new approach to an old problem. Pediatr. Surg. Int. 2001, 17, 513–514. [Google Scholar] [CrossRef] [PubMed]
- Daniels, J.; Craig, F.; Wajed, R.; Meates, M. Umbilical granulomas: A randomised controlled trial. Arch. Dis. Child Fetal. Neonatal. Ed. 2003, 88, F257. [Google Scholar] [CrossRef] [PubMed]
- Majjiga, V.S.; Kumaresan, P.; Glass, E.J. Silver nitrate burns following umbilical granuloma treatment. Arch. Dis. Child 2005, 90, 674. [Google Scholar] [CrossRef] [PubMed]
- Ho, S.H.; Huang, H.C. Silver nitrate burns following umbilical granuloma treatment. Pediatr. Neonatol. 2023. [Google Scholar] [CrossRef]
- Say, B. Silver nitrate burn after umbilical granuloma treatment: A case report. Skin Dis. Skin Care 2017, 2, 1. [Google Scholar]
- Brødsgaard, A.; Nielsen, T.; Mølgaard, U.; Pryds, O.; Pedersen, P. Treating umbilical granuloma with topical clobetasol propionate cream at home is as effective as treating it with topical silver nitrate in the clinic. Acta Paediatr. 2015, 104, 174–177. [Google Scholar] [CrossRef]
- Ogawa, C.; Sato, Y.; Suzuki, C.; Mano, A.; Tashiro, A.; Niwa, T.; Hamazaki, S.; Tanahashi, Y.; Suzumura, M.; Hayano, S.; et al. Treatment with silver nitrate versus topical steroid treatment for umbilical granuloma: A non- inferiority randomized control trial. PLoS ONE 2018, 13, e0192688. [Google Scholar] [CrossRef]
- Norris, D.A. Mechanisms of action of topical therapies and the rationale for combination therapy. J. Am. Acad. Dermatol. 2005, 53 (Suppl. S1), S17–S25. [Google Scholar] [CrossRef]
- Ali, M.A.; Thrower, S.L.; Hanna, S.J.; Coulman, S.A.; Birchall, J.C.; Wong, F.S.; Dayan, C.M.; Tatovic, D. Topical steroid therapy induces pro-tolerogenic changes in Langerhans cells in human skin. Immunology 2015, 146, 411–422. [Google Scholar] [CrossRef]
- Aydin, M.; Orman, A.; Deveci, U.; Taskin, E. Topical clobetasol propionate may not be safe for treating umbilical granuloma in infants. Acta Paediatr. 2015, 104, e49. [Google Scholar] [CrossRef]
- Dhar, S.; Seth, J.; Parikh, D. Systemic side-effects of topical corticosteroids. Indian J. Dermatol. 2014, 59, 460–464. [Google Scholar] [CrossRef] [PubMed]
- Janssen, P.A.; Selwood, B.L.; Dobson, S.R.; Peacock, D.; Thiessen, P.N. To dye or not to dye: A randomized, clinical trial of a triple dye/alcohol regime versus dry cord care. Pediatrics 2003, 111, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Janyoungsak, P.; Emrat, K.; Chatmapanrangsee, J.; Nuntnarumit, P. Randomised comparative study on the efficacy of 3% versus 30% NaCl solution in the treatment of umbilical granuloma. J. Paediatr. Child Health 2022, 58, 1566–1570. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Umbilical Granuloma | Umbilical Polyp | |
|---|---|---|
| Onset | A few weeks after birth | After umbilical cord separation |
| Color | Dull red or pink | Cherry red |
| Surface characteristics | Unevenness | Smooth |
| Hardness | Soft | Hard |
| Secretions | Serous bloody, sometimes purulent | Serous |
| Pathology | Granulation tissue | Smooth muscle tissue |
| Non-surgical treatment | Effective | Not effective |
| Ultrasonography findings | Hypervascular | Hypovascular |
| Year | Eligible Neonates (No.) | Neonates with Umbilical Granuloma (No.) | Annual Incidence Rate of Umbilical Granuloma (%) |
|---|---|---|---|
| 2013 | 659 | 25 | 3.8 |
| 2014 | 697 | 34 | 4.9 |
| 2015 | 794 | 39 | 4.9 |
| 2016 | 784 | 49 | 6.3 |
| 2017 | 711 | 49 | 6.9 |
| 2018 | 686 | 43 | 6.3 |
| 2019 | 682 | 50 | 7.3 |
| 2020 | 628 | 33 | 5.3 |
| 2021 | 543 | 38 | 7.0 |
| 2022 | 496 | 35 | 7.1 |
| Total | 6680 | 395 | 5.9 |
| Neonates with UG | Neonates without UG | Simple Linear Regression p-Value | Multiple Linear Regression p-Value | |
|---|---|---|---|---|
| n = 395 | n = 6285 | |||
| Gestational age, weeks | 39.43 (38.57–40.28) | 39.14 (38.14–40.0) | <0.001 | <0.001 |
| Birth weight, g | 3066 (2802–3282) | 2984 (2740–3236) | 0.001 | NS |
| Male sex, n (%) | 217 (54.9) | 3132 (49.8) | 0.049 | 0.030 |
| Delivery mode | ||||
| Spontaneous vaginal delivery, n (%) | 270 (68.4) | 4148 (66.0) | 0.334 | NS |
| Vacuum extraction, n (%) | 47 (11.9) | 539 (8.6) | 0.024 | NS |
| Cesarean delivery, n (%) | 75 (19.0) | 1588 (25.3) | 0.005 | NS |
| Meconium-stained amniotic fluid, n (%) | 82 (20.8) | 896 (14.3) | <0.001 | 0.032 |
| Intrauterine infection, n (%) | 1 (0.25) | 25 (0.40) | 0.654 | NS |
| One-minute Apgar score | 8 (8–9) | 8 (8–9) | 0.801 | NS |
| Umbilical arterial blood pH | 7.316 (7.274–7.354) | 7.312 (7.276–7.348) | 0.317 | NS |
| Birth during a warm and humid season *, n (%) | 218 (55.2) | 3329 (53.0) | 0.339 | NS |
| Treatment | p-Value | ||||
|---|---|---|---|---|---|
| Silver Nitrate Cauterization | Betamethasone Valerate Application | Ethanol Disinfection | Ligation | ||
| n = 145 | n = 220 | n = 5 | n = 25 | ||
| Male sex, n (%) | 77 (53.1) | 121 (55.0) | 2 (40.0) | 17 (68.0) | 0.500 |
| Gestational age, weeks | 39.57 | 39.28 | 39.14 | 39.71 | 0.228 |
| (38.57–40.43) | (38.57–40.28) | (38.36–40.42) | (39.14–40.71) | ||
| Birthweight, g | 3036 | 3072 | 3140 | 3068 | 0.861 |
| (2768–3288) | (2833–3293) | (2500–3274) | (2799–3182) | ||
| Delivery mode | |||||
| Spontaneous vaginal delivery, n (%) | 97 (66.9) | 149 (67.7) | 4 (80.0) | 20 (80.0) | 0.560 |
| Vacuum extraction, n (%) | 22 (15.2) | 22 (10.0) | 1 (20.0) | 2 (8.0) | 0.406 |
| Cesarean delivery, n (%) | 26 (17.9) | 46 (20.9) | 0 (0.0) | 3 (12.0) | 0.459 |
| Meconium-stained amniotic fluid, n (%) | 25 (17.2) | 48 (21.8) | 3 (60.0) | 6 (24.0) | 0.108 |
| Intrauterine infection, n (%) | 0 (0) | 1(0.5) | 0(0) | 0 (0) | 0.851 |
| One-minute Apgar score | 8 (8–9) | 8 (8–8) | 9 (8–9) | 8 (8–9) | 0.032 |
| Umbilical arterial blood pH | 7.314 | 7.316 | 7.371 | 7.323 | 0.656 |
| (7.268–7.353) | (7.278–7.353) | (7.128–7.394) | (7.289–7.360) | ||
| Birth during a warm and humid season *, n (%) | 70 (48.3) | 133 (60.5) | 2 (40.0) | 14 (56.0) | 0.126 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iijima, S. Umbilical Granuloma: Frequency, Associated Factors, 10-Year Treatment Trends, and Effectiveness at a Single Hospital in Japan. J. Clin. Med. 2023, 12, 6104. https://doi.org/10.3390/jcm12186104
Iijima S. Umbilical Granuloma: Frequency, Associated Factors, 10-Year Treatment Trends, and Effectiveness at a Single Hospital in Japan. Journal of Clinical Medicine. 2023; 12(18):6104. https://doi.org/10.3390/jcm12186104
Chicago/Turabian StyleIijima, Shigeo. 2023. "Umbilical Granuloma: Frequency, Associated Factors, 10-Year Treatment Trends, and Effectiveness at a Single Hospital in Japan" Journal of Clinical Medicine 12, no. 18: 6104. https://doi.org/10.3390/jcm12186104
APA StyleIijima, S. (2023). Umbilical Granuloma: Frequency, Associated Factors, 10-Year Treatment Trends, and Effectiveness at a Single Hospital in Japan. Journal of Clinical Medicine, 12(18), 6104. https://doi.org/10.3390/jcm12186104