
Post-COVID-19 Symptoms and Heart Disease: Incidence, Prognostic Factors, Outcomes and Vaccination: Results from a Multi-Center International Prospective Registry (HOPE 2)
 , , ,
, , ,  , , , ,
, , , ,  , , , ,
, , , ,  , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Participation Criteria
2.1.1. Data Collection and Variable Definitions
2.1.2. Study Follow-up and Outcomes
2.2. Statistical Analysis
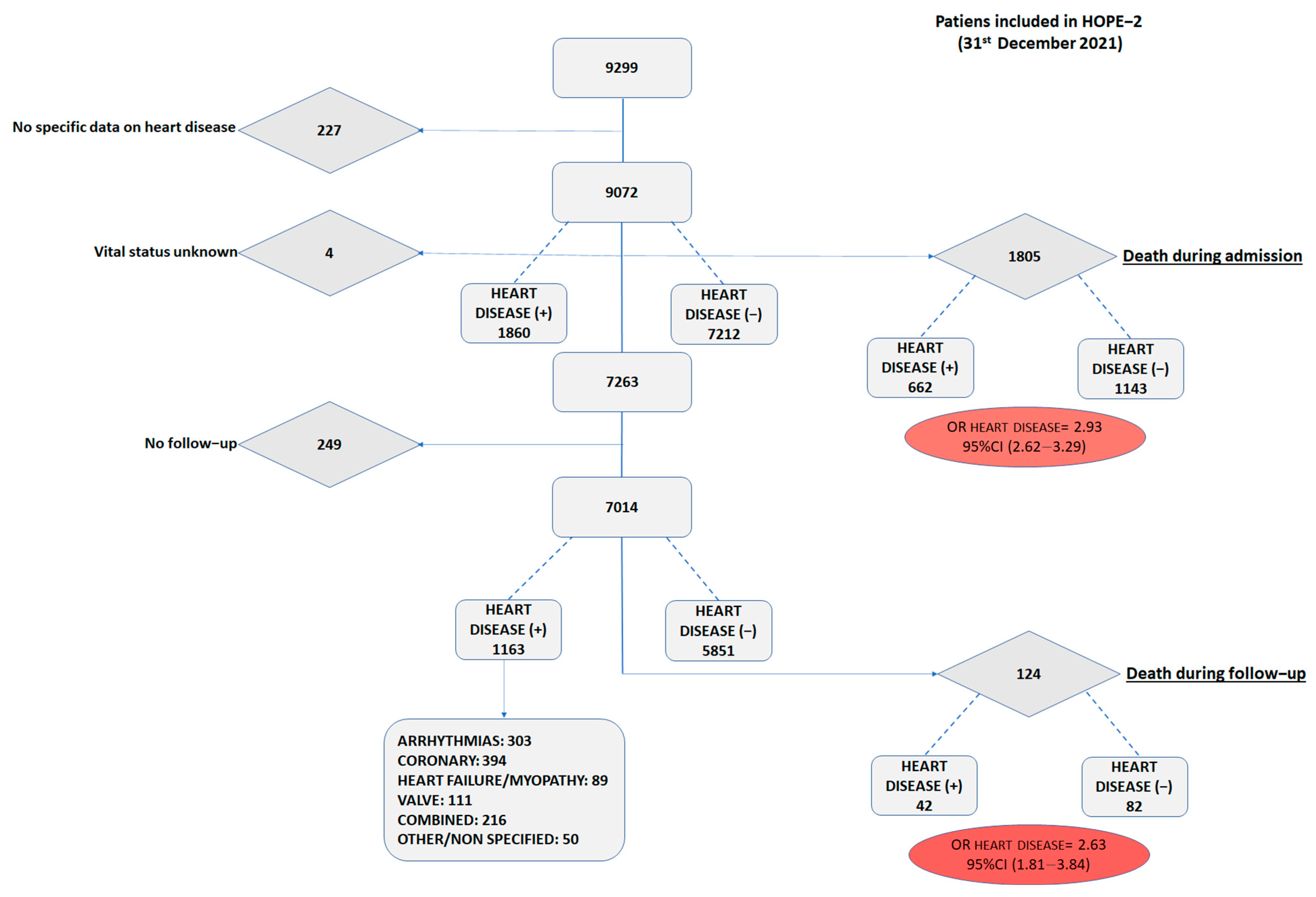
3. Results
3.1. Overall Data and General Info
3.2. Heart Disease (+) vs. Heart Disease (−) Cohorts
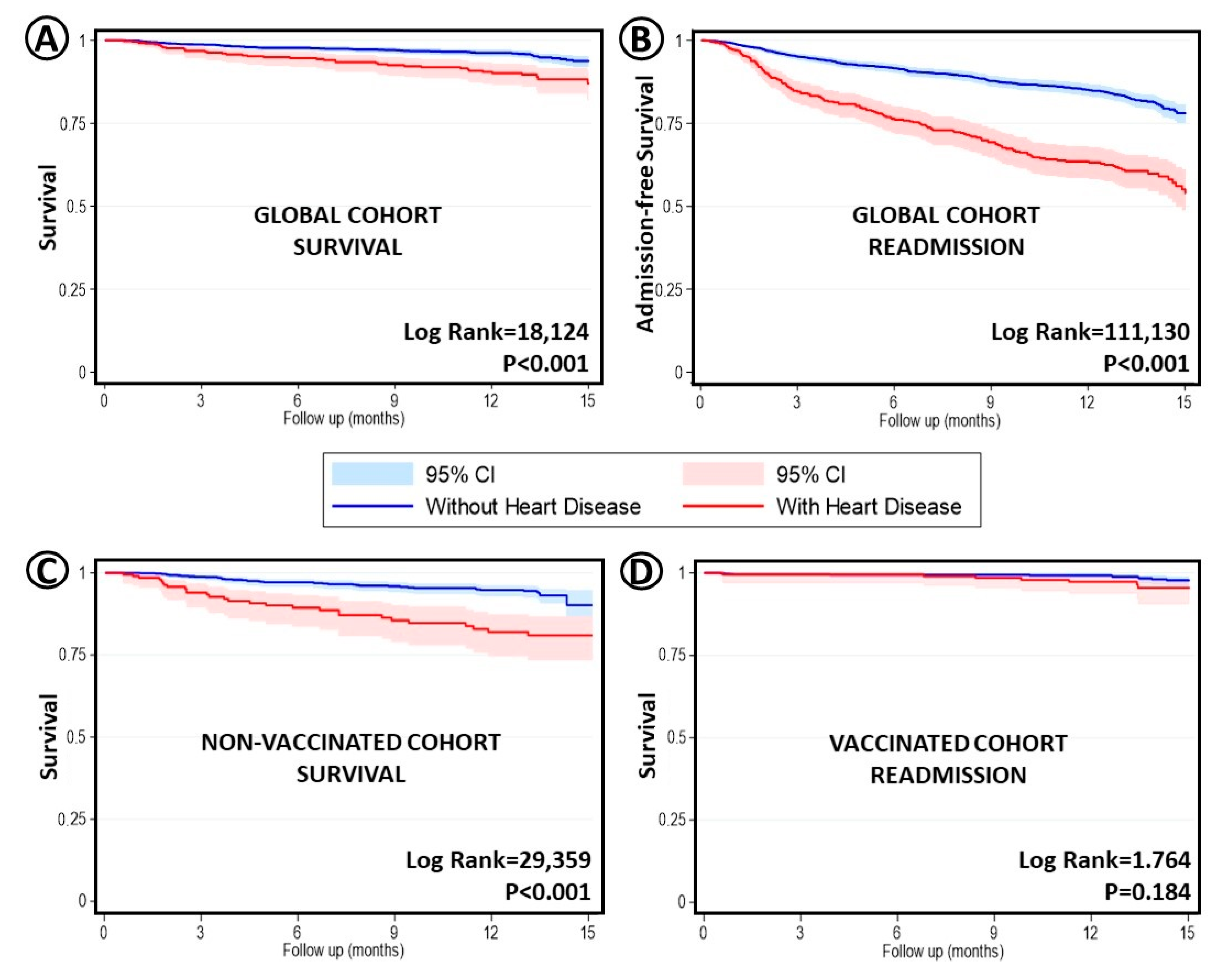
3.3. Heart Disease (+) Patients and Mortality
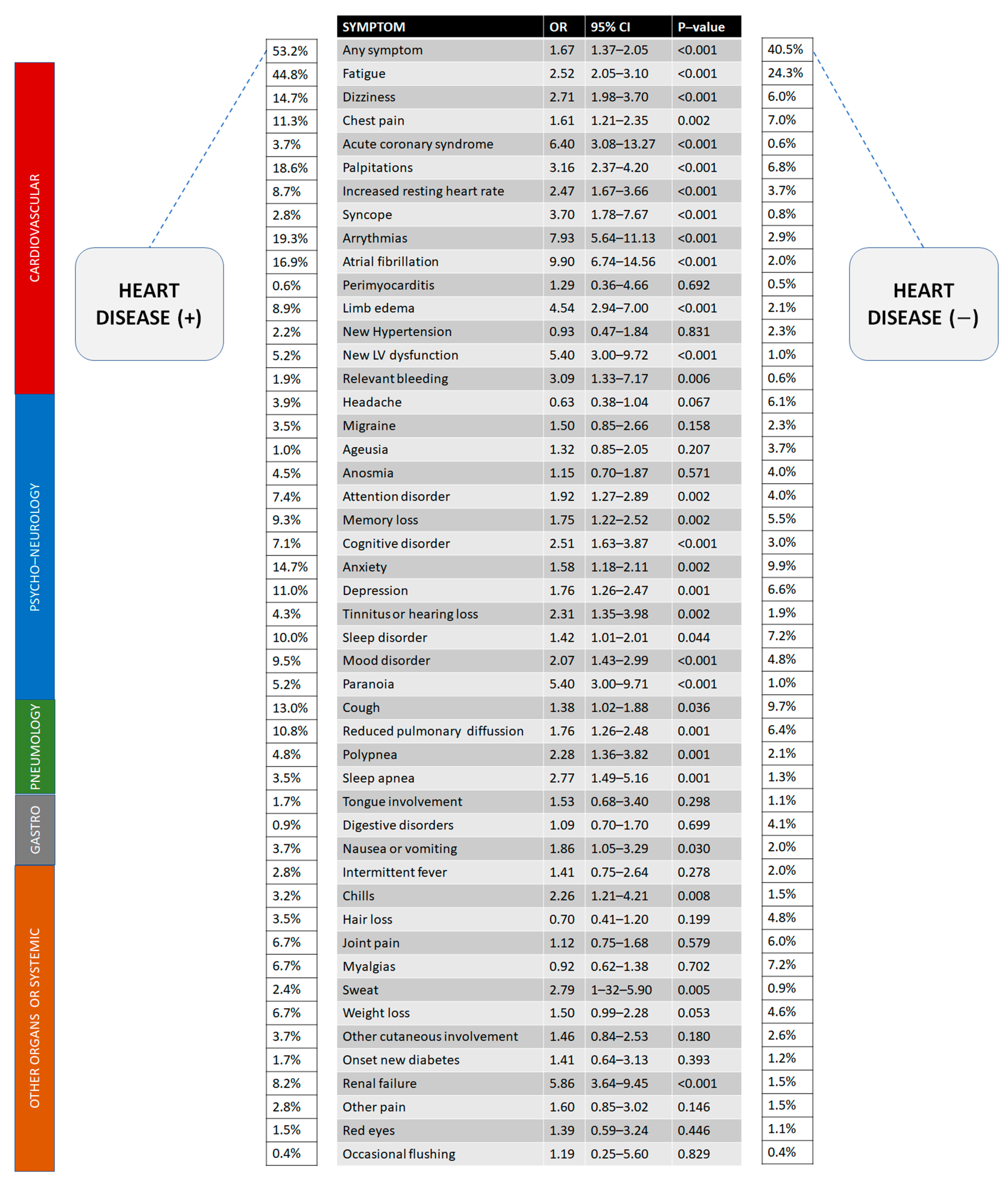
3.4. Symptoms Post-COVID-19 and Vaccination
4. Discussion
Clinical Implications
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Available online: https://covid19.who.int/ (accessed on 26 December 2022).
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 long-term effects of COVID-19: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 16144. [Google Scholar] [CrossRef] [PubMed]
- Jafari-Oori, M.; Moradian, S.T.; Ebadi, A.; Jafari, M.; Dehi, M. Incidence of cardiac complications following COVID-19 infection: An umbrella meta-analysis study. Heart Lung. 2022, 52, 136–145. [Google Scholar] [CrossRef] [PubMed]
- Aden, D.; Zaheer, S.; Kumar, R.; Raj, S.; Khan, T.; Varshney, S. Beyond COVID-19 and SARS-CoV-2, cardiovascular outcomes of “long covid” from a pathological perspective—A look back and road ahead. Pathol. Res. Pract. 2022, 239, 154144. [Google Scholar] [CrossRef] [PubMed]
- Aleksova, A.; Fluca, A.L.; Gagno, G.; Pierri, A.; Padoan, L.; Derin, A.; Moretti, R.; Noveska, E.A.; Azzalini, E.; D’Errico, S.; et al. Long-term effect of SARS-CoV-2 infection on cardiovascular outcomes and all-cause mortality. Life Sci. 2022, 310, 121018. [Google Scholar] [CrossRef] [PubMed]
- Dy, L.F.; Lintao, R.C.V.; Cordero, C.P.; Cabaluna, I.T.G.; Dans, L.F. Prevalence and prognostic associations of cardiac abnormalities among hospitalized patients with COVID-19: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 8449. [Google Scholar] [CrossRef]
- Tian, Y.; Lu, H.; Liu, X.; Zhao, Y.; Zhang, P. Low tricuspid annular plane systolic excursion is associated with a poor outcome in patients with COVID-19: A systematic review and meta-analysis. Medicine 2022, 101, e28971. [Google Scholar] [CrossRef]
- Núñez-Gil, I.J.; Fernández-Ortiz, A.; Maroud Eid, C.; Huang, J.; Romero, R.; Becerra-Muñoz, V.M.; Uribarri, A.; Feltes, G.; Trabatoni, D.; Fernandez-Rozas, I.; et al. Underlying heart diseases and acute COVID-19 outcomes. Cardiol. J. 2021, 28, 202–214. [Google Scholar] [CrossRef] [PubMed]
- Henning, R.J. Cardiovascular complications of COVID-19 severe acute respiratory syndrome. Am. J. Cardiovasc. Dis. 2022, 12, 170–191. [Google Scholar] [PubMed]
- González-Calle, D.; Eiros, R.; Sánchez, P.L. The heart and SARS-CoV-2. Med. Clin. 2022, 159, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Al-Ali, D.; Elshafeey, A.; Mushannen, M.; Kawas, H.; Shafiq, A.; Mhaimeed, N.; Mhaimeed, O.; Mhaimeed, N.; Zeghlache, R.; Salameh, M.; et al. Cardiovascular and haematological events post COVID-19 vaccination: A systematic review. J. Cell. Mol. Med. 2021, 26, 636–653. [Google Scholar] [CrossRef] [PubMed]
- Núñez-Gil, I.J.; Olier, I.; Feltes, G.; Viana-Llamas, M.C.; Maroun-Eid, C.; Romero, R.; Fernández-Rozas, I.; Uribarri, A.; Becerra-Muñoz, V.M.; Alfonso-Rodriguez, E.; et al. HOPE COVID-19 Investigators. Renin-angiotensin system inhibitors effect before and during hospitalization in COVID-19 outcomes: Final analysis of the international HOPE COVID-19 (Health Outcome Predictive Evaluation for COVID-19) registry. Am. Heart J. 2021, 237, 104–115. [Google Scholar] [CrossRef] [PubMed]
- El-Battrawy, I.; Nuñez-Gil, I.J.; Abumayyaleh, M.; Estrada, V.; Manuel Becerra-Muñoz, V.; Uribarri, A.; Fernández-Rozas, I.; Feltes, G.; Arroyo-Espliguero, R.; Trabattoni, D.; et al. COVID-19 and the impact of arterial hypertension-An analysis of the international HOPE COVID-19 Registry (Italy-Spain-Germany). Eur. J. Clin. Investig. 2021, 51, e13582. [Google Scholar] [CrossRef] [PubMed]
- Santoro, F.; Nuñez-Gil, I.J.; Vitale, E.; Viana-Llamas, M.C.; Reche-Martinez, B.; Romero-Pareja, R.; Feltez Guzman, G.; Fernandez Rozas, I.; Uribarri, A.; Becerra-Muñoz, V.M.; et al. Antiplatelet therapy and outcome in COVID-19: The Health Outcome Predictive Evaluation Registry. Heart 2022, 108, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Clemente-Moragón, A.; Martínez-Milla, J.; Oliver, E.; Santos, A.; Flandes, J.; Fernández, I.; Rodríguez-González, L.; Serrano Del Castillo, C.; Ioan, A.M.; López-Álvarez, M.; et al. Metoprolol in Critically Ill Patients with COVID-19. J. Am. Coll. Cardiol. 2021, 78, 1001–1011. [Google Scholar] [CrossRef] [PubMed]
- Gerretsen, P.; Kim, J.; Caravaggio, F.; Quilty, L.; Sanches, M.; Wells, S.; Brown, E.E.; Agic, B.; Pollock, B.G.; Graff-Guerrero, A. Individual determinants of COVID-19 vaccine hesitancy. PLoS ONE 2021, 16, e0258462. [Google Scholar] [CrossRef] [PubMed]
- Salah, H.M.; Mehta, J.L. COVID-19 Vaccine and Myocarditis. Am. J. Cardiol. 2021, 157, 146–148. [Google Scholar] [CrossRef] [PubMed]
- Gundry, S.R. Observational Findings of PULS Cardiac Test Findings for Inflammatory Markers in Patients Receiving mRNA Vaccines. Circulation 2021, 144, A10712. [Google Scholar] [CrossRef]
- Available online: https://www.who.int/publications-detail-redirect/WHO-2019-nCoV-Post_COVID19_condition-Clinical_case_definition2021.1#:~:text=Post%20COVID%2D19%20condition%20occurs,explained%20by%20an%20alterative%20diagnosis (accessed on 8 February 2022).
- Fernández-de-Las-Peñas, C.; Pellicer-Valero, O.J.; Navarro-Pardo, E.; Palacios-Ceña, D.; Florencio, L.L.; Guijarro, C.; Martín-Guerrero, J.D. Symptoms Experienced at the Acute Phase of SARS-CoV-2 Infection as Risk Factor of Long-term Post-COVID Symptoms: The LONG-COVID-EXP-CM Multicenter Study. Int. J. Infect. Dis. 2022, 116, 241–244. [Google Scholar] [CrossRef] [PubMed]
- Charman, S.J.; Velicki, L.; Okwose, N.C.; Harwood, A.; McGregor, G.; Ristic, A.; Banerjee, P.; Seferovic, P.M.; MacGowan, G.A.; Jakovljevic, D.G. Insights into heart failure hospitalizations, management, and services during and beyond COVID-19. ESC Heart Fail. 2021, 8, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Izzo, C.; Visco, V.; Gambardella, J.; Ferruzzi, G.J.; Rispoli, A.; Rusciano, M.R.; Toni, A.L.; Virtuoso, N.; Carrizzo, A.; Di Pietro, P.; et al. Cardiovascular Implications of microRNAs in Coronavirus Disease 2019. J. Pharmacol. Exp. Ther. 2023, 384, 102–108. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics /7014 | Heart Disease (−) /5851 | Heart Disease (+) /1163 | p-Value | Odds Ratio (95% CI) |
|---|---|---|---|---|
| BEFORE ADMISSION | ||||
| Gender, male | 3272 (55.9) | 730 (62.8) | <0.001 | 1.33 (1.17–1.51) |
| Age, mean (SD) | 57.9 (17.0) | 72.7 (13.9) | <0.001 | 4.98 (4.35–5.70) * |
Race
| 73 (1.2) 4389 (75.0) 978 (16.7) 362 (6.2) 49 (0.8) | 26 (2.2) 1005 (86.4) 110 (9.5) 14 (1.2) 8 (0.7) | <0.001 | 0.47(0.39–0.56) ** |
| Health care professional, no | 4989 (85.3) | 1084 (93.2) | <0.001 | 0.42 (0.33–0.54) |
| Hypertension | 2152 (36.8) | 885 (76.1) | <0.001 | 5.47 (4.73–6.32) |
| Dyslipidemia | 1421 (24.3) | 611 (52.5) | <0.001 | 3.45 (3.03–3.93) |
| Diabetes Mellitus | 761 (13.3) | 322 (28.5) | <0.001 | 2.60 (2.24–3.02) |
| Obesity | 960 (16.4) | 264 (22.7) | <0.001 | 1.50 (1.28–1.74) |
| Smoker | 334 (6.3) | 88 (8.3) | 0.018 | 1.34 (1.05–1.72) |
| Renal insufficiency | 165 (2.8) | 124 (10.7) | <0.001 | 4.11 (3.23–5.24) |
| Any lung disease | 770 (16.9) | 323 (35.0) | <0.001 | 2.64 (2.26–3.10) |
| Any cerebrovascular disease | 225 (3.8) | 153 (13.2) | <0.001 | 3.79 (3.05–4.70) |
| Connective disease | 120 (2.1) | 41 (3.5) | 0.002 | 1.74 (1.22–2.50) |
| Liver disease | 153 (2.6) | 58 (5.0) | <0.001 | 1.95 (1.43–2.66) |
| Any cancer | 525 (9.0) | 161 (13.8) | <0.001 | 1.63 (1.35–1.97) |
| Any immunosuppression | 307 (5.2) | 90 (7.7) | 0.001 | 1.51 (1.19–1.93) |
| Any dependency level | 352 (6.3) | 206 (18.2) | <0.001 | 3.32 (2.76–4.00) |
| Home oxygen therapy | 74 (1.3) | 56 (4.8) | <0.001 | 3.94 (2.77–5.62) |
| Oral anticoagulation therapy | 106 (1.8) | 416 (35.8) | <0.001 | 30.18 (24.07–37.85) |
| ACEI/ARB therapy | 1484 (25.4) | 658 (56.6) | <0.001 | 3.83 (3.37–4.37) |
| DURING ADMISSION | ||||
| Hemoglobin at admission (SD) | 13.71 (1.71) | 13.07 (2.07) | <0.001 | - |
| Creatinine at admission (SD) | 0.98 (0.88) | 1.34 (1.21) | <0.001 | - |
| Elevated D dimer, at admission | 2925 (50.1) | 628 (54.1) | 0.013 | 1.17 (1.03–1.33) |
| Elevated procalcitonin, at admission | 630 (10.8) | 181 (15.6) | <0.001 | 1.53 (1.28–1.82) |
| Elevated PCR, at admission | 4563 (78.2) | 993 (85.5) | <0.001 | 1.65 (1.38–1.97) |
| Elevated Troponin, at admission | 284 (4.9) | 186 (16.0) | <0.001 | 3.73 (3.06–4.54) |
Abnormal chest X ray, at admission
| 1055 (20.1) 3313 (63.0) | 230 (22.1) 599 (57.6) | 0.003 | 0.80 (.058–0.94) *** |
| Abnormal blood pressure | 242 (4.6) | 88 (8.5) | <0.001 | 1.92 (1.49–2.47) |
| Heart failure | 107 (1.8) | 166 (14.4) | <0.001 | 8.47 (6.97–11.55) |
| Renal failure | 409 (7.0) | 215 (18.6) | <0.001 | 3.03 (2.53–3.62) |
| Sepsis | 269 (4.6) | 82 (7.1) | <0.001 | 1.58 (1.22–2.04) |
| SIRS | 800 (13.7) | 173 (15.0) | 0.264 | 1.11(0.93–1.32) |
| Relevant bleeding | 83 (1.4) | 49 (4.2) | <0.001 | 3.07 (2.14–4.39) |
| Hemoptysis | 60 (1.0) | 24 (2.1) | 0.003 | 2.04 (1.26–3.29) |
| Embolic event | 99 (1.7) | 28 (2.4) | 0.092 | 1.44 (0.94–2.20) |
| NIMV | 589 (10.1) | 158 (13.7) | <0.001 | 1.41 (1.17–1.70) |
| IMV | 265 (4.6) | 67 (5.8) | 0.067 | 1.30 (0.98–1.70) |
| ECMO or other circulatory support | 21 (0.4) | 9 (0.9) | 0.043 | 2.12 (1.54–2.91) |
| AFTER DISCHARGE | ||||
| Discharge anticoagulation | 1321 (22.7) | 562 (48.8) | <0.001 | 9.44 (7.98–11.17) |
| Abnormal LVEF (<54%) at discharge | 21 (2.4) | 58 (22.5) | <0.001 | 11.90 (7.05–20.46) |
| Elevated D dimer, at discharge | 599 (27.5) | 152 (33.0) | 0.017 | 1.30 (1.05–1.61) |
| Elevated procalcitonin, at discharge | 137 (6.3) | 62 (13.4) | <0.001 | 2.32 (1.69–3.19) |
| Elevated PCR, at discharge | 741 (34.0) | 206 (44.7) | <0.001 | 1.57 (1.28–1.92) |
| Elevated Troponin, at discharge | 48 (2.2) | 33 (7.2) | <0.001 | 3.43 (2.17–5.40) |
| Elevated NTproBNP, at discharge | 50(2.3) | 55 (11.9) | <0.001 | 5.77 (3.88–8.59) |
| Abnormal chest X ray, at discharge | 412 (27.7) | 123 (37.5) | <0.001 | 1.56 (1.22–2.01) |
| Abnormal spirometry, at follow-up | 67 (7.8) | 33 (18.8) | <0.001 | 2.72 (1.73–4.29) |
| Abnormal chest CT scan, at follow-up | 183 (22.9) | 59 (33.7) | 0.003 | 1.71 (1.20–2.47) |
| Readmission during follow-up | 261 (11.8) | 158 (33.5) | <0.001 | 3.77 (3.00–4.75) |
| New COVID-19 episode | 58 (2.6) | 11 (2.3) | 0.722 | 0.89 (0.46–1.71) |
| Any clinical event after discharge | 886 (40.5) | 246 (53.2) | <0.001 | 1.67 (1.37–2.05) |
| Vaccination | 1138 (51.4) | 253 (53.7) | 0.371 | 1.09 (0.90–1.34) |
Vaccine brand
| 157 (2.7) 36 (0.6) 98 (1.7) 831 (14.2) 0 6 (0.1) 10 (0.2) | 20 (1.7) 6 (0.5) 29 (2.5) 192 (16.5) 2 (0.2) 1 (0.1) 3 (0.3) | 0.001 | |
| Death during follow-up | 82 (1.4) | 42 (3.6) | <0.001 | 2.64 (1.81–3.85) |
| Characteristics of Heart Disease Patients /1163 | Alive /1121 | Deceased /42 | p-Value ** | Odds Ratio (95% CI) |
|---|---|---|---|---|
| BEFORE ADMISSION | ||||
| Gender, male | 704 (62.8) | 26 (61.9) | 0.906 | 0.96 (0.51–1.81) |
| Age, mean (SD) | 72.3 (13.8) | 83.4 (9.9) | 0.005 | 4.23 (1.65–10.84) * |
Race
| 26 (2.3) 963 (85.9) 110 (9.8) 14 (1.2) 8 (0.7) | 0 42 (100) 0 0 0 | 0.144 | 0.96 (0.95–0.97) ** |
| Health care professional, no | 1044 (93.1) | 40 (95.2) | 0.934 | 0.68 (0.16–2.59) |
Type of (main) heart disease
| 294 (26.2) 203 (18.1) 384 (34.3) 85 (7.6) 48 (4.3) 107 (9.5) | 9 (21.4) 13 (31.0) 10 (23.8) 4 (9.5) 2 (4.8) 4 (9.5) | 0.360 | - |
| Hypertension | 850 (75.8) | 35 (83.3) | 0.263 | 1.59 (0.70–3.63) |
| Dyslipidemia | 589 (52.5) | 22 (52.4) | 0.984 | 0.99 (0.54–1.84) |
| Diabetes Mellitus | 312 (28.7) | 10 (25.0) | 0.616 | 0.83 (0.40–1.72) |
| Obesity | 255 (22.7) | 9 (21.4) | 0.841 | 0.93 (0.44–1.96) |
| Smoker | 86 (8.4) | 2 (4.9) | 0.419 | 0.56 (0.13–2.35) |
| Renal insufficiency | 114 (10.2) | 10 (23.8) | 0.005 | 2.76 (1.32–5.76) |
| Any lung disease | 305 (34.5) | 18 (48.6) | 0.076 | 1.80 (0.93–3.48) |
| Any cerebrovascular disease | 145 (12.9) | 8 (19.0) | 0.250 | 1.58 (0.72–3.49) |
| Connective disease | 38 (3.4) | 3 (7.1) | 0.195 | 2.20 (0.65–7.41) |
| Liver disease | 55 (4.9) | 3 (7.1) | 0.513 | 1.49 (0.45–4.98) |
| Any cancer | 148 (13.2) | 13 (31.0) | 0.001 | 2.95 (1.50–5.80) |
| Any immunosuppression | 84 (7.5) | 6 (14.3) | 0.106 | 2.06 (0.84–5.02) |
| Any dependency level | 186 (17.1) | 20 (48.8) | <0.001 | 4.62 (2.45–8.69) |
| Home oxygen therapy | 54 (4.8) | 2 (4.8) | 0.987 | 0.99 (0.23–4.20) |
| Oral anticoagulation therapy | 394 (35.1) | 22 (52.4) | 0.022 | 2.03 (1.10–3.76) |
| ACEI/ARB therapy | 638 (56.9) | 20 (47.6) | 0.233 | 0.69 (0.87–1.28) |
| DURING ADMISSION | ||||
| Elevated D dimer, at admission | 601 (53.7) | 27 (64.3) | 0.177 | 1.55 (0.81–2.95) |
| Elevated procalcitonin, at admission | 175 (15.6) | 6 (14.3) | 0.812 | 0.90 (0.37–2.17) |
| Elevated PCR, at admission | 954 (85.3) | 39 (92.9) | 0.169 | 2.25 (0.69–7.36) |
| Elevated Troponin, at admission | 176 (15.7) | 10 (23.8) | 0.161 | 1.67 (0.81–3.47) |
Abnormal chest X ray, at admission
| 218 (21.8) 579 (57.8) | 12 (30.8) 20 (51.3) | 0.414 | 1.17 (0.51–2.69) *** |
| Abnormal blood pressure | 80 (8.0) | 8 (22.9) | 0.002 | 3.43 (1.51–7.80) |
| Heart failure | 155 (13.9) | 11 (26.2) | 0.026 | 2.20 (1.08–4.45) |
| Renal failure | 199 (17.9) | 16(1.4) | 0.001 | 2.82 (1.49–5.36) |
| Sepsis | 75 (6.7) | 7 (16.7) | 0.014 | 2.76 (1.19–6.43) |
| SIRS | 164 (14.7) | 9 (21.4) | 0.234 | 1.58 (0.74–3.36) |
| Relevant bleeding | 45 (4.0) | 4 (9.5) | 0.084 | 2.50 (0.85–7.29) |
| Hemoptysis | 24 (2.2) | 0 | 0.336 | - |
| Embolic event | 27 (2.4) | 1 (2.4) | 0.984 | 0.98 (0.13–7.38) |
| NIMV | 155 (13.9) | 3 (7.1) | 0.209 | 0.47 (0.14–1.56) |
| IMV | 66 (6.0) | 1 (2.4) | 0.332 | 038 (0.05–2.84) |
| ECMO or other circulatory support | 9 (0.9) | 0 | 0.529 | 0.96 (0.94–0.97) |
| AFTER DISCHARGE | ||||
| Discharge anticoagulation | 171 (39.4) | 8 (27.6) | 0.206 | 2.39 (0.65–8.79) |
| Abnormal LVEF (<54%) at discharge | 54(21.8) | 4 (40.0) | 0.176 | 2.39 (0.65–8.79) |
| Elevated D dimer, at discharge | 136 (31.5) | 16 (55.2) | 0.009 | 2.68 (1.25–5.72) |
| Elevated procalcitonin, at discharge | 57 (13.2) | 5 (17.2) | 0.536 | 1.37 (0.50–3.74) |
| Elevated PCR, at discharge | 185 (42.8) | 21 (72.4) | 0.002 | 3.50 (1.52–8.09) |
| Elevated Troponin, at discharge | 29 (6.7) | 4 (13.8) | 0.152 | 2.22 (0.72–6.82) |
| Elevated NTproBNP, at discharge | 47 (10.9) | 8 (27.6) | 0.007 | 3.12 (1.31–7.44) |
| Abnormal chest X ray, at discharge | 115 (36.7) | 8 (53.3) | 0.195 | 1.97 (0.69–5.57) |
| Abnormal spirometry, at follow-up | 33 (19.2) | 0 | 0.331 | - |
| Abnormal chest CT scan, at follow-up | 54 (32.1) | 5 (71.4) | 0.031 | 5.28 (0.99–28.08) |
| Readmission during follow-up | 135 (31.1) | 23 (62.2) | <0.001 | 3.64 (1.82–7.29) |
| New COVID-19 episode | 11 (2.5) | 0 | 0.327 | 0.92 (0.89–0.94) |
| Any clinical event after discharge | 229 (52.9) | 17 (58.6) | 0.549 | 1.62 (0.59–2.71) |
| Vaccination | 245 (56.5) | 8 (21.6) | <0.001 | 0.21 (0.9–0.47) |
Vaccine brand
| 20 (1.8) 6 (0.5) 28 (2.5) 185 (16.5) 2 (0.2) 1 (0.1) 3 (0.3) | 0 0 1 (2.4) 7 (16.7) 0 0 0 | 0.990 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Núñez-Gil, I.J.; Feltes, G.; Viana-Llamas, M.C.; Raposeiras-Roubin, S.; Romero, R.; Alfonso-Rodríguez, E.; Uribarri, A.; Santoro, F.; Becerra-Muñoz, V.; Pepe, M.; et al. Post-COVID-19 Symptoms and Heart Disease: Incidence, Prognostic Factors, Outcomes and Vaccination: Results from a Multi-Center International Prospective Registry (HOPE 2). J. Clin. Med. 2023, 12, 706. https://doi.org/10.3390/jcm12020706
Núñez-Gil IJ, Feltes G, Viana-Llamas MC, Raposeiras-Roubin S, Romero R, Alfonso-Rodríguez E, Uribarri A, Santoro F, Becerra-Muñoz V, Pepe M, et al. Post-COVID-19 Symptoms and Heart Disease: Incidence, Prognostic Factors, Outcomes and Vaccination: Results from a Multi-Center International Prospective Registry (HOPE 2). Journal of Clinical Medicine. 2023; 12(2):706. https://doi.org/10.3390/jcm12020706
Chicago/Turabian StyleNúñez-Gil, Ivan J., Gisela Feltes, María C. Viana-Llamas, Sergio Raposeiras-Roubin, Rodolfo Romero, Emilio Alfonso-Rodríguez, Aitor Uribarri, Francesco Santoro, Víctor Becerra-Muñoz, Martino Pepe, and et al. 2023. "Post-COVID-19 Symptoms and Heart Disease: Incidence, Prognostic Factors, Outcomes and Vaccination: Results from a Multi-Center International Prospective Registry (HOPE 2)" Journal of Clinical Medicine 12, no. 2: 706. https://doi.org/10.3390/jcm12020706
APA StyleNúñez-Gil, I. J., Feltes, G., Viana-Llamas, M. C., Raposeiras-Roubin, S., Romero, R., Alfonso-Rodríguez, E., Uribarri, A., Santoro, F., Becerra-Muñoz, V., Pepe, M., Castro-Mejía, A. F., Signes-Costa, J., Gonzalez, A., Marín, F., Lopez-País, J., Cerrato, E., Vázquez-Cancela, O., Espejo-Paeres, C., López Masjuan, Á., ... Perez-Villacastín, J., on behalf of HOPE-2 Investigators. (2023). Post-COVID-19 Symptoms and Heart Disease: Incidence, Prognostic Factors, Outcomes and Vaccination: Results from a Multi-Center International Prospective Registry (HOPE 2). Journal of Clinical Medicine, 12(2), 706. https://doi.org/10.3390/jcm12020706