
Trends in Atrial Fibrillation Management—Results from a National Multi-Center Urgent Care Network Registry


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.3. Variables
2.4. Outcomes
2.5. Statistical Analysis
2.6. Trends Analysis
2.7. Subgroup Analyses
3. Results
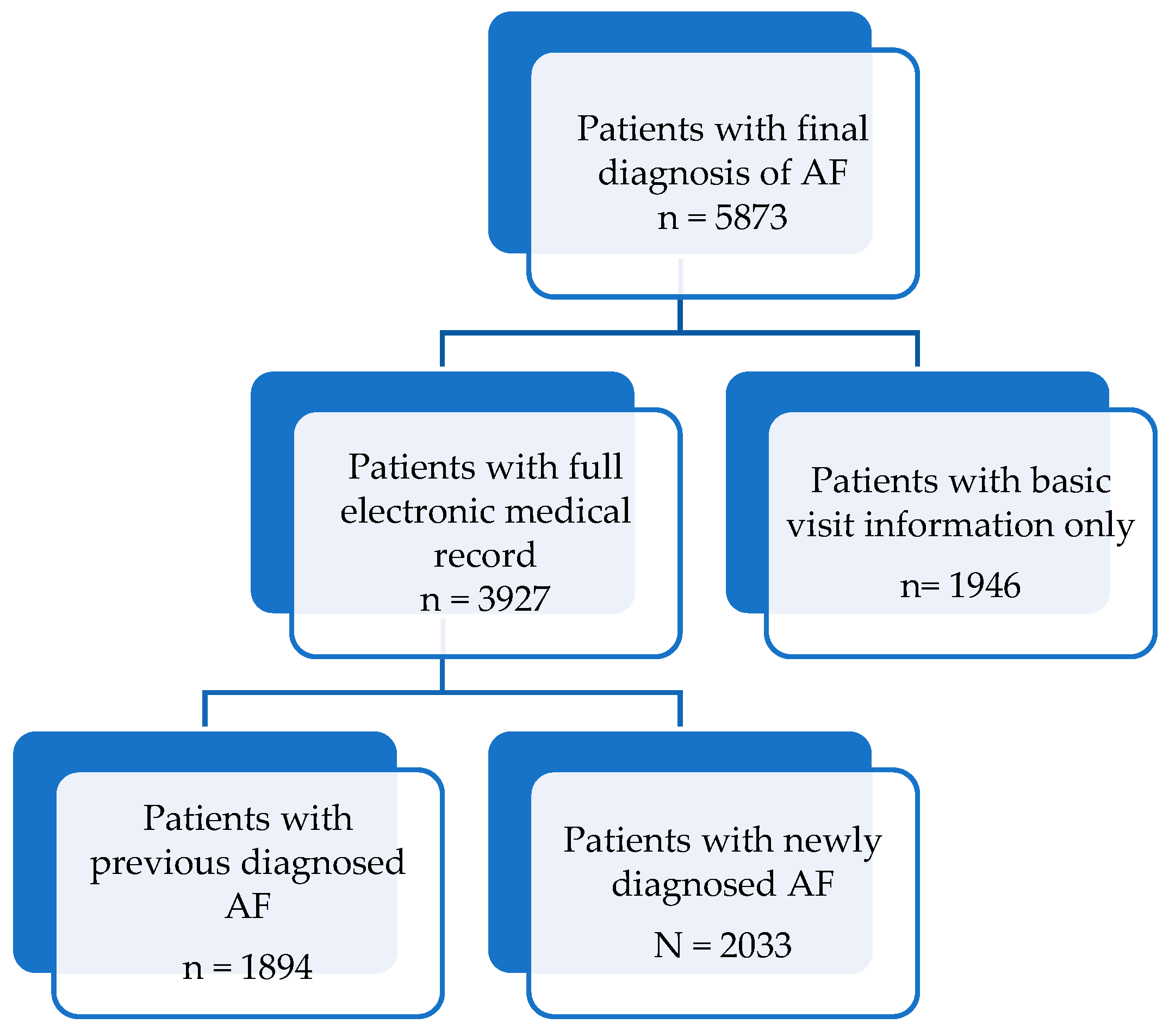
3.1. Subject Characteristics
3.2. Predictors of ED Referral
3.3. Subgroup Analysis of Patients with Newly Diagnosed AF
3.4. Trend Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AC | Anticoagulation |
| ACEI | Angiotensin-converting-enzyme inhibitor |
| ARB | Angiotensin receptor blocker |
| AF | Atrial fibrillation |
| BP | Blood pressure |
| CAD | Coronary artery disease |
| CHF | Congestive heart failure |
| CKD | Chronic kidney disease |
| COPD | Chronic obstructive pulmonary disease |
| CVA | Cerebrovascular accident |
| ECG | Electrocardiography |
| ED | Emergency department |
| EMS | Emergency medical services |
| EMR | Electronic medical record |
| HB | Hemoglobin |
| HMO | Health maintenance organization |
| NOAC | Novel anticoagulant |
| OR | Odds ratio |
| PVD | Peripheral vascular disease |
| SpO2 | Oxygen saturation measured with pulse oximetry |
| TIA | Transient ischemic attack |
| UCC | Urgent care center |
| VKA | Vitamin K antagonist |
Appendix A




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age |
| Male |
| Previously diagnosed AF |
| CHF |
| Hypertension |
| Diabetes mellitus |
| CVA/TIA |
| Vascular disease |
| Medications |
| Aspirin |
| Clopidogrel |
| Anticoagulation medication |
| Antiarrhythmic medication |
| Beta blocker |
| ACEI |
| ARB |
| Symptoms onset (<48 h) |
| Shift of Arrival |
| Morning |
| Evening |
| Night |
| Pulse (BPM) |
| Systolic BP (mmHg) |
| Temperature (°C) |
| SpO2 (%) |
References
- OECD iLibrary. Emergency Care Services: Trends, Drivers and Interventions to Manage the Demand. OECD Health Working Papers. Available online: https://www.oecd-ilibrary.org/social-issues-migration-health/emergency-care-services_5jrts344crns-en (accessed on 30 September 2023).
- Baier, N.; Geissler, A.; Bech, M.; Bernstein, D.; Cowling, T.E.; Jackson, T.; van Manen, J.; Rudkjøbing, A.; Quentin, W. Emergency and Urgent Care Systems in Australia, Denmark, England, France, Germany and the Netherlands–Analyzing Organization, Payment and Reforms. Health Policy 2019, 123, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, D.R. Community-Based Urgent Care in Israel and Worldwide. Isr. J. Health Policy Res. 2013, 2, 38. [Google Scholar] [CrossRef] [PubMed]
- Weinick, R.M.; Burns, R.M.; Mehrotra, A. Many Emergency Department Visits Could Be Managed at Urgent Care Centers and Retail Clinics. Health Aff. 2010, 29, 1630–1636. [Google Scholar] [CrossRef] [PubMed]
- Merritt, B.; Naamon, E.; Morris, S.A. The Influence of an Urgent Care Center on the Frequency of ED Visits in an Urban Hospital Setting. Am. J. Emerg. Med. 2000, 18, 123–125. [Google Scholar] [CrossRef] [PubMed]
- Haklai, Z. Emergency Department Visits—Geographic Characteristics 2009–2011; Health Information Division Ministry of Health: Jerusalem, Israel, 2011. [Google Scholar]
- Rahman, F.; Kwan, G.F.; Benjamin, E.J. Global Epidemiology of Atrial Fibrillation. Nat. Rev. Cardiol. 2014, 11, 639–654. [Google Scholar] [CrossRef]
- Chugh, S.S.; Havmoeller, R.; Narayanan, K.; Singh, D.; Rienstra, M.; Benjamin, E.J.; Gillum, R.F.; Kim, Y.-H.; McAnulty, J.H.; Zheng, Z.-J.; et al. Worldwide Epidemiology of Atrial Fibrillation. Circulation 2014, 129, 837–847. [Google Scholar] [CrossRef]
- January, C.T.; Wann, L.S.; Calkins, H.; Chen, L.Y.; Cigarroa, J.E.; Cleveland, J.C.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; Furie, K.L.; et al. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients with Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart R. Circulation 2019, 140, e125–e151. [Google Scholar] [CrossRef]
- Wong, C.X.; Brooks, A.G.; Leong, D.P.; Roberts-Thomson, K.C.; Sanders, P. The Increasing Burden of Atrial Fibrillation Compared with Heart Failure and Myocardial Infarction: A 15-Year Study of All Hospitalizations in Australia. Arch. Intern. Med. 2012, 172, 739–741. [Google Scholar] [CrossRef]
- Patel, N.J.; Deshmukh, A.; Pant, S.; Singh, V.; Patel, N.; Arora, S.; Shah, N.; Chothani, A.; Savani, G.T.; Mehta, K.; et al. Contemporary Trends of Hospitalization for Atrial Fibrillation in the United States, 2000 through 2010: Implications for Healthcare Planning. Circulation 2014, 129, 2371–2379. [Google Scholar] [CrossRef]
- Lip, G.Y.H. The ABC Pathway: An Integrated Approach to Improve AF Management. Nat. Rev. Cardiol. 2017, 14, 627–628. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Kirchhof, P.; Kühne, M.; Ahlsson, A.; Balsam, P.; Bauersachs, J.; Benussi, S.; Brandes, A.; Braunschweig, F.; et al. 2020 ESC Guidelines for the Diagnosis and Management of Atrial Fibrillation Developed in Collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the Diagnosis and Management of Atrial Fibrillation of the European Society of Cardiology (ESC) Developed with the Special Contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef] [PubMed]
- Coll-Vinent, B.; Martín, A.; Sánchez, J.; Tamargo, J.; Suero, C.; Malagón, F.; Varona, M.; Cancio, M.; Sánchez, S.; Carbajosa, J.; et al. Benefits of Emergency Departments’ Contribution to Stroke Prophylaxis in Atrial Fibrillation: The EMERG-AF Study (Emergency Department Stroke Prophylaxis and Guidelines Implementation in Atrial Fibrillation). Stroke 2017, 48, 1344–1352. [Google Scholar] [CrossRef] [PubMed]
- Martín, A.; Coll-Vinent, B.; Suero, C.; Fernández-Simón, A.; Sánchez, J.; Varona, M.; Cancio, M.; Sánchez, S.; Carbajosa, J.; Malagón, F.; et al. Benefits of Rhythm Control and Rate Control in Recent-Onset Atrial Fibrillation: The HERMES-AF Study. Acad. Emerg. Med. 2019, 26, 1034–1043. [Google Scholar] [CrossRef] [PubMed]
- Scheuermeyer, F.X.; Innes, G.; Pourvali, R.; Dewitt, C.; Grafstein, E.; Heslop, C.; Macphee, J.; Ward, J.; Heilbron, B.; McGrath, L.; et al. Missed Opportunities for Appropriate Anticoagulation among Emergency Department Patients with Uncomplicated Atrial Fibrillation or Flutter. Ann. Emerg. Med. 2013, 62, 557–565.E2. [Google Scholar] [CrossRef]
- Wu, J.; Nadarajah, R.; Nakao, Y.M.; Nakao, K.; Wilkinson, C.; Mamas, M.A.; Camm, A.J.; Gale, C.P. Temporal Trends and Patterns in Atrial Fibrillation Incidence: A Population-Based Study of 3 4 Million Individuals. Lancet Reg. Health Eur. 2022, 17, 100386. [Google Scholar] [CrossRef]
- Freedman, B.; Camm, J.; Calkins, H.; Healey, J.S.; Rosenqvist, M.; Wang, J.; Albert, C.M.; Anderson, C.S.; Antoniou, S.; Benjamin, E.J.; et al. Screening for Atrial Fibrillation: A Report of the AF-SCREEN International Collaboration. Circulation 2017, 135, 1851–1867. [Google Scholar] [CrossRef]
- Noseworthy, P.A.; Kaufman, E.S.; Chen, L.Y.; Chung, M.K.; Elkind, M.S.V.; Joglar, J.A.; Leal, M.A.; McCabe, P.J.; Pokorney, S.D.; Yao, X. Subclinical and Device-Detected Atrial Fibrillation: Pondering the Knowledge Gap: A Scientific Statement from the American Heart Association. Circulation 2019, 140, e944–e963. [Google Scholar] [CrossRef]
- Lee, S.R.; Choi, E.K.; Lee, S.Y.; Lee, E.; Han, K.D.; Cha, M.J.; Kwon, W.Y.; Shin, S.D.; Oh, S.; Lip, G.Y.H. Temporal Trends of Emergency Department Visits of Patients with Atrial Fibrillation: A Nationwide Population-Based Study. J. Clin. Med. 2020, 9, 1485. [Google Scholar] [CrossRef]
- Rozen, G.; Hosseini, S.M.; Kaadan, M.I.; Biton, Y.; Heist, E.K.; Vangel, M.; Mansour, M.C.; Ruskin, J.N. Emergency Department Visits for Atrial Fibrillation in the United States: Trends in Admission Rates and Economic Burden From 2007 to 2014. J. Am. Heart Assoc. 2018, 7, e009024. [Google Scholar] [CrossRef]
- Lip, G.Y.H.; Nieuwlaat, R.; Pisters, R.; Lane, D.A.; Crijns, H.J.G.M.; Andresen, D.; Camm, A.J.; Davies, W.; Capucci, A.; Olsson, B.; et al. Refining Clinical Risk Stratification for Predicting Stroke and Thromboembolism in Atrial Fibrillation Using a Novel Risk Factor-Based Approach: The Euro Heart Survey on Atrial Fibrillation. Chest 2010, 137, 263–272. [Google Scholar] [CrossRef]
- Magnussen, C.; Niiranen, T.J.; Ojeda, F.M.; Gianfagna, F.; Blankenberg, S.; Njølstad, I.; Vartiainen, E.; Sans, S.; Pasterkamp, G.; Hughes, M.; et al. Sex Differences and Similarities in Atrial Fibrillation Epidemiology, Risk Factors, and Mortality in Community Cohorts: Results from the Biomarcare Consortium (Biomarker for Cardiovascular Risk Assessment in Europe). Circulation 2017, 136, 1588–1597. [Google Scholar] [CrossRef] [PubMed]
- Hong, K.L.; Babiolakis, C.; Zile, B.; Bullen, M.; Haseeb, S.; Halperin, F.; Hohl, C.M.; Magee, K.; Sandhu, R.K.; Tian, S.Y.; et al. Canada-Wide Mixed Methods Analysis Evaluating the Reasons for Inappropriate Emergency Department Presentation in Patients with a History of Atrial Fibrillation: The Multicentre AF-ED Trial. BMJ Open 2020, 10, e033482. [Google Scholar] [CrossRef] [PubMed]
- Gehi, A.K.; Deyo, Z.; Mendys, P.; Hatfield, L.; Laux, J.; Walker, T.J.; Chen, S.; O’Bryan, J.; Garner, K.; Sears, S.F.; et al. Novel Care Pathway for Patients Presenting to the Emergency Department with Atrial Fibrillation. Circ. Cardiovasc. Qual. Outcomes 2018, 11, e004129. [Google Scholar] [CrossRef] [PubMed]
- Conti, A.; Canuti, E.; Mariannini, Y.; Viviani, G.; Poggioni, C.; Boni, V.; Pini, R.; Vanni, S.; Padeletti, L.; Gensini, G.F. Clinical Management of Atrial Fibrillation: Early Interventions, Observation, and Structured Follow-up Reduce Hospitalizations. Am. J. Emerg. Med. 2012, 30, 1962–1969. [Google Scholar] [CrossRef] [PubMed]
- Stewart, S.; Ball, J.; Horowitz, J.D.; Marwick, T.H.; Mahadevan, G.; Wong, C.; Abhayaratna, W.P.; Chan, Y.K.; Esterman, A.; Thompson, D.R.; et al. Standard versus Atrial Fibrillation-Specific Management Strategy (SAFETY) to Reduce Recurrent Admission and Prolong Survival: Pragmatic, Multicentre, Randomised Controlled Trial. Lancet 2015, 385, 775–784. [Google Scholar] [CrossRef]
- Carter, L.; Gardner, M.; Magee, K.; Fearon, A.; Morgulis, I.; Doucette, S.; Sapp, J.L.; Gray, C.; Abdelwahab, A.; Parkash, R. An Integrated Management Approach to Atrial Fibrillation. J. Am. Heart Assoc. 2016, 5, e002950. [Google Scholar] [CrossRef]
- Yang, Y.M.; Shao, X.H.; Zhu, J.; Zhang, H.; Liu, Y.; Gao, X.; Yu, L.T.; Liu, L.S.; Zhao, L.; Yu, P.F.; et al. One-Year Outcomes of Emergency Department Patients with Atrial Fibrillation. Angiology 2014, 66, 745–752. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, B.A.; Kim, S.; Fonarow, G.C.; Thomas, L.; Ansell, J.; Kowey, P.R.; Mahaffey, K.W.; Gersh, B.J.; Hylek, E.; Naccarelli, G.; et al. Drivers of Hospitalization for Patients with Atrial Fibrillation: Results from the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF). Am. Heart J. 2014, 167, 735–742.e2. [Google Scholar] [CrossRef]
- Yao, X.; Abraham, N.S.; Caleb Alexander, G.; Crown, W.; Montori, V.M.; Sangaralingham, L.R.; Gersh, B.J.; Shah, N.D.; Noseworthy, P.A. Effect of Adherence to Oral Anticoagulants on Risk of Stroke and Major Bleeding Among Patients with Atrial Fibrillation. J. Am. Heart Assoc. 2016, 5, e003074. [Google Scholar] [CrossRef]
- Romiti, G.F.; Proietti, M.; Bonini, N.; Ding, W.Y.; Boriani, G.; Huisman, M.V.; Lip, G.Y.H. Adherence to the Atrial Fibrillation Better Care (ABC) Pathway and the Risk of Major Outcomes in Patients with Atrial Fibrillation: A Post-Hoc Analysis from the Prospective GLORIA-AF Registry. EClinicalMedicine 2023, 55, 101757. [Google Scholar] [CrossRef]
- Alayo, Q.A.; Oyenuga, A.O.; Adejumo, A.C.; Pottathil, V.; Grewal, D.; Okafor, P.N. The Impact of Night-Time Emergency Department Presentation on Upper Gastrointestinal Hemorrhage Outcomes. J. Clin. Gastroenterol. 2022, 56, 576–583. [Google Scholar] [CrossRef] [PubMed]
- Silbergleit, R.; Kronick, S.L.; Philpott, S.; Lowell, M.J.; Wagner, C. Quality of Emergency Care on the Night Shift. Acad. Emerg. Med. 2006, 13, 325–330. [Google Scholar] [CrossRef] [PubMed]
- Khanna, R.; Wachsberg, K.; Marouni, A.; Feinglass, J.; Williams, M.V.; Wayne, D.B. The Association between Night or Weekend Admission and Hospitalization-Relevant Patient Outcomes. J. Hosp. Med. 2011, 6, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Dong, Z.; Du, X.; Lu, S.; Jiang, C.; Xia, S.; He, L.; Su, X.; Jia, Z.; Long, D.; Sang, C.; et al. Incidence and Predictors of Hospitalization in Patients with Atrial Fibrillation: Results from the Chinese Atrial Fibrillation Registry Study. BMC Cardiovasc. Disord. 2021, 21, 146. [Google Scholar] [CrossRef] [PubMed]
- Barón-Esquivias, G.; Gómez, S.; Brufau, H.; García, L.; Amo, C.; Gutiérrez, J.M.; Wu, L.; Salmerón, F.; Pinilla, S.; López, V. Care Indicators in Patients with Atrial Fibrillation: Assessment of Sex Differences and Management of Clinical Problems. Rev. Española Cardiol. 2016, 69, 384–391. [Google Scholar] [CrossRef]
- Chapa, D.W.; Akintade, B.; Thomas, S.A.; Friedmann, E. Gender Differences in Stroke, Mortality, and Hospitalization among Patients with Atrial Fibrillation: A Systematic Review. Heart Lung J. Acute Crit. Care 2015, 44, 189–198. [Google Scholar] [CrossRef]
- Roten, L.; Rimoldi, S.F.; Schwick, N.; Sakata, T.; Heimgartner, C.; Fuhrer, J.; DelacrÉtaz, E.; Tanner, H. Gender Differences in Patients Referred for Atrial Fibrillation Management to a Tertiary Center. Pacing Clin. Electrophysiol. 2009, 32, 622–626. [Google Scholar] [CrossRef]
- Buhari, H.; Fang, J.; Han, L.; Austin, P.C.; Dorian, P.; Jackevicius, C.A.; Yu, A.Y.X.; Kapral, M.K.; Singh, S.M.; Tu, K.; et al. Stroke Risk in Women with Atrial Fibrillation. Eur. Heart J. 2023, ehad508. [Google Scholar] [CrossRef]
- Kezerle, L.; Tsadok, M.A.; Berliner Senderey, A.; Hoshen, M.; Leventer-Roberts, M.; Reges, O.; Leibowitz, M.; Haim, M. Use of Oral Anticoagulation Therapy in the First 3 Months after the Diagnosis of Atrial Fibrillation in Israel: A Population-Based Study. J. Cardiovasc. Electrophysiol. 2020, 31, 1356–1363. [Google Scholar] [CrossRef]
- Arbel, A.; Abu-Ful, Z.; Preis, M.; Cohen, S.; Saliba, W. Implementation of Oral Anticoagulation Treatment Guidelines in Patients with Newly Diagnosed Atrial Fibrillation. Br. J. Clin. Pharmacol. 2021, 87, 4747–4755. [Google Scholar] [CrossRef]
- Atzema, C.L.; Jackevicius, C.A.; Chong, A.; Dorian, P.; Ivers, N.M.; Parkash, R.; Austin, P.C. Prescribing of Oral Anticoagulants in the Emergency Department and Subsequent Long-Term Use by Older Adults with Atrial Fibrillation. CMAJ 2019, 191, E1345–E1354. [Google Scholar] [CrossRef] [PubMed]
- Kea, B.; Waites, B.T.; Lin, A.; Raitt, M.; Vinson, D.R.; Ari, N.; Welle, L.; Sill, A.; Button, D.; Sun, B.C. Practice Gap in Atrial Fibrillation Oral Anticoagulation Prescribing at Emergency Department Home Discharge. West. J. Emerg. Med. 2020, 21, 924–934. [Google Scholar] [CrossRef] [PubMed]
- Birkmeyer, J.D.; Barnato, A.; Birkmeyer, N.; Bessler, R.; Skinner, J. The Impact of the COVID-19 Pandemic on Hospital Admissions in the United States. Health Aff. 2020, 39, 2010–2017. [Google Scholar] [CrossRef] [PubMed]
- Bodilsen, J.; Nielsen, P.B.; Søgaard, M.; Dalager-Pedersen, M.; Speiser, L.O.Z.; Yndigegn, T.; Nielsen, H.; Larsen, T.B.; Skjøth, F. Hospital Admission and Mortality Rates for Non-COVID Diseases in Denmark during COVID-19 Pandemic: Nationwide Population Based Cohort Study. BMJ 2021, 373, n1135. [Google Scholar] [CrossRef] [PubMed]
- O’Shea, C.J.; Middeldorp, M.E.; Thomas, G.; Harper, C.; Elliott, A.D.; Ray, N.; Campbell, K.; Lau, D.H.; Sanders, P. Atrial Fibrillation Burden during the Coronavirus Disease 2019 Pandemic. EP Europace 2021, 23, 1493–1501. [Google Scholar] [CrossRef]
- Wollborn, J.; Karamnov, S.; Fields, K.G.; Yeh, T.; Muehlschlegel, J.D. COVID-19 Increases the Risk for the Onset of Atrial Fibrillation in Hospitalized Patients. Sci. Rep. 2022, 12, 12014. [Google Scholar] [CrossRef] [PubMed]
- Bassand, J.P.; Accetta, G.; Al Mahmeed, W.; Corbalan, R.; Eikelboom, J.; Fitzmaurice, D.A.; Fox, K.A.A.; Gao, H.; Goldhaber, S.Z.; Goto, S.; et al. Risk Factors for Death, Stroke, and Bleeding in 28,628 Patients from the GARFIELD-AF Registry: Rationale for Comprehensive Management of Atrial Fibrillation. PLoS ONE 2018, 13, e0191592. [Google Scholar] [CrossRef]
- Sagris, D.; Lip, G.Y.H. Atrial Fibrillation, a Contemporary Sign of Multimorbidity and Irregular Social Inequity. Lancet Reg. Health Eur. 2022, 17, 100395. [Google Scholar] [CrossRef]




| Clinical Characteristic * | Overall (N = 3927) | ED (N = 2734) | Home (N = 1193) |
|---|---|---|---|
| Age | 68.74 ± 14.3 | 68.4 ± 14.8 | 69.5 ± 13.1 § |
| Male | 1837 (46.8) | (48.8) | (42.2) § |
| Previously diagnosed AF | 1893 (48.2) | (36.8) | (74.3) § |
| Comorbidities | |||
| CHF | 143 (3.6) | (3.6) | (3.8) |
| Hypertension | 1366 (34.8) | (36.6) | (30.6) § |
| Diabetes mellitus | 557 (14.2) | (15.4) | (11.3) § |
| CVA/TIA | 105 (2.7) | (2.9) | (2.1) |
| Vascular disease ** | 429 (10.9) | (12.7) | (7.0) § |
| CAD | 416 (10.6) | (12.3) | (6.6) § |
| PVD | 19 (0.5) | (0.6) | (0.3) |
| CKD | 66 (1.7) | (2.0) | (1.0) § |
| COPD | 56 (1.4) | (1.7) | (0.8) § |
| Comorbidity Score | |||
| 0 | 3238 (82.4) | (80.3) | (87.3) |
| 1 | 581 (14.8) | (16.5) | (11.0) § |
| Above 2 | 108 (2.8) | (3.2) | (1.8) § |
| Medications | |||
| Aspirin | 290 (7.4) | (7.4) | (7.5) |
| Clopidogrel | 55 (1.4) | (1.3) | (1.7) |
| Anticoagulation medication † | 911 (23.2) | (15.0) | (41.9) § |
| VKA | 222 (5.7) | (3.7) | (10.1) |
| Enoxaparin | 11 (0.3) | (0.2) | (0.5) |
| Apixaban | 387 (9.9) | (6.0) | (18.6) § |
| Dabigatran | 80 (2.0) | (1.4) | (3.4) § |
| Rivaroxaban | 145 (3.7) | (2.5) | (6.4) § |
| Unknown anticoagulation | 74 (1.9) | (1.2) | (3.5) § |
| Antiarrhythmic medication ‡ | 318 (8.1) | (5.0) | (15.3) § |
| Beta blocker | 698 (17.8) | (12.8) | (29.2) § |
| Propafenone | 144 (3.7) | (2.6) | (6.1) § |
| Amiodarone | 92 (2.3) | (1.4) | (4.6) § |
| Flecainide | 68 (1.7) | (0.9) | (3.6) § |
| Digoxin | 18 (0.5) | (0.2) | (1.1) § |
| Sotalol | 18 (0.5) | (0.4) | (0.5) |
| ACEI | 143 (3.6) | (3.3) | (4.4) |
| ARB | 87 (2.2) | (2.0) | (2.7) |
| Symptoms Onset | |||
| <48 h | 1933 (49.2) | (49.5) | (48.5) |
| Shift of Arrival | |||
| Morning | 1392 (35.4) | (33.6) | (39.7) |
| Evening | 1982 (50.5) | (51.3) | (48.5) § |
| Night | 553 (14.1) | (15.1) | (11.7) § |
| Weekend visit | 1262 (32.1) | (32.8) | (30.6) |
| Pulse (BPM) | 103.2 ± 28.0 | 103.6 ± 28.6 | 102.0 ± 26.6 |
| Systolic BP (mmHg) | 134.6 ± 24.4 | 134.4 ± 25.2 | 135.2 ± 22.7 |
| Temperature (°C) | 36.7 ± 0.3 | 36.7 ± 0.4 | 36.7 ± 0.3 § |
| Hb (G/dL) | 12.8 ± 2.2 | 12.8 ± 2.3 | 12.9 ± 2.0 |
| SpO2 (%) | 96.5 ± 3.0 | 96.3 ± 3.3 | 96.8 ± 2.2 § |
| SpO2 < 95% | 567 (14.4) | (15.9) | (11.1) § |
| Variable | OR | 95% CI | p-Value | |
|---|---|---|---|---|
| Age | 0.99 | 0.99–1.00 | 0.024 | |
| Previously diagnosed AF | 0.31 | 0.26–0.37 | <0.001 | |
| SpO2 (%) | 0.94 | 0.91–0.97 | <0.001 | |
| Pulse | 1.00 | 1.00–1.01 | 0.024 | |
| Anticoagulation medication † | 0.56 | 0.46–0.67 | <0.001 | |
| Antiarrhythmic medication ‡ | 0.63 | 0.49–0.82 | <0.001 | |
| Beta blocker | 0.63 | 0.52–0.76 | <0.001 | |
| Vascular disease | 1.87 | 1.43–2.45 | <0.001 | |
| Shift of arrival | Morning | - | - | Reference |
| Evening | 1.31 | 1.11–1.55 | 0.001 | |
| Night | 1.68 | 1.32–2.15 | <0.001 |
| Clinical Characteristic * | Overall (N = 2033) | ED (N = 1726) | Home (N = 307) |
|---|---|---|---|
| Age | 68.65 ± 15.07 | 68.55 ± 15.19 | 69.22 ± 14.39 |
| Male | 1020 (50.2) | (50.5) | (48.5) |
| Comorbidities | |||
| CHF | 57 (2.8) | (2.5) | (4.2) |
| Hypertension | 780 (38.4) | (38.7) | (36.5) |
| Diabetes mellitus | 334 (16.4) | (16.3) | (16.9) |
| CVA/TIA | 59 (2.9) | (3.1) | (2.0) |
| Vascular disease ** | 256 (12.6) | (13.4) | (8.1) § |
| CAD | 249 (12.2) | (13.0) | (8.1) § |
| PVD | 12 (0.6) | (0.7) | (0.0) |
| CKD | 34 (1.7) | (1.7) | (1.3) |
| COPD | 40 (2.0) | (2.1) | (1.3) |
| Comorbidity Score | |||
| 0 | 1643 (80.8) | (80.0) | (85.0) |
| 1 | 333 (16.4) | (17.0) | (13.0) |
| Above 2 | 57 (2.8) | (3.0) | (2.0) |
| Medications | |||
| Aspirin | 149 (7.3) | (7.0) | (9.4) |
| Clopidogrel | 27 (1.3) | (1.2) | (2.0) |
| Anticoagulation medication † | 60 (3.0) | (2.7) | (4.2) |
| VKA | 25 (1.2) | (1.1) | (2.0) |
| Enoxaparin | 5 (0.2) | (0.2) | (0.7) |
| Apixaban | 12 (0.6) | (0.6) | (0.3) |
| Dabigatran | 3 (0.1) | (0.2) | (0) |
| Rivaroxaban | 4 (0.2) | (0.2) | (0.3) |
| Unknown anticoagulation | 11 (0.5) | (0.5) | (1.0) |
| Antiarrhythmic medication ‡ | 8 (0.4) | (0.3) | (1.0) |
| Beta blocker | 149 (7.3) | (6.4) | (12.7) § |
| Propafenone | 5 (0.2) | (0.2) | (0.7) |
| Amiodarone | 1 (0) | (0) | (0) |
| Flecainide | 1 (0) | 1 (0) | 0 (0) |
| Digoxin | 1 (0) | 1 (0) | 0 (0) |
| Sotalol | 0 (0) | (0) | (0) |
| ACEI | 56 (2.8) | (2.3) | (5.2) § |
| ARB | 35 (1.7) | (1.4) | (3.3) § |
| Symptoms Onset | |||
| <48 h | 954 (46.9) | (47.6) | (42.7) |
| Shift of Arrival | |||
| Morning | 736 (36.2) | (35.1) | (42.7) |
| Evening | 1022 (50.3) | (50.7) | (47.9) § |
| Night | 275 (13.5) | (14.3) | (9.4) § |
| Weekend | 669 (32.9) | (33.1) | (31.9) |
| Pulse (BPM) | 102.3 ± 28.5 | 102.4 ± 28.8 | 101.3 ± 27.0 |
| Systolic BP (mmHg) | 134.7 ± 25.4 | 134.4 ± 25.8 | 136.4 ± 23.0 |
| Temperature (°C) | 36.7 ± 0.4 | 36.7 ± 0.4 | 36.7 ± 0.3 |
| Hb (G/dL) | 13.0 ± 2.2 | 12.9 ± 2.2 | 13.1 ± 2.1 |
| SpO2 (%) | 96.3 ± 3.4 | 96.2 ± 3.6 | 96.7 ± 2.3 § |
| SpO2 < 95% | 346 (17.0) | (17.7) | (13.0) § |
| Variable | OR | 95% CI | p-Value | |
|---|---|---|---|---|
| SpO2 (%) | 0.95 | 0.91–0.99 | 0.027 | |
| Beta blocker | 0.52 | 0.34–0.78 | 0.002 | |
| ACEI | 0.45 | 0.24–0.84 | 0.013 | |
| Vascular disease | 1.83 | 1.18–2.84 | 0.007 | |
| Shift of arrival | Morning | - | - | Reference |
| Evening | 1.28 | 0.99–1.67 | 0.065 | |
| Night | 2.01 | 1.29–3.13 | 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lebovitz, S.; Estryk, M.; Zimmerman, D.R.; Pollak, A.; Luria, D.; Amir, O.; Biton, Y. Trends in Atrial Fibrillation Management—Results from a National Multi-Center Urgent Care Network Registry. J. Clin. Med. 2023, 12, 6704. https://doi.org/10.3390/jcm12216704
Lebovitz S, Estryk M, Zimmerman DR, Pollak A, Luria D, Amir O, Biton Y. Trends in Atrial Fibrillation Management—Results from a National Multi-Center Urgent Care Network Registry. Journal of Clinical Medicine. 2023; 12(21):6704. https://doi.org/10.3390/jcm12216704
Chicago/Turabian StyleLebovitz, Shalom, Menachem Estryk, Deena R. Zimmerman, Arthur Pollak, David Luria, Offer Amir, and Yitschak Biton. 2023. "Trends in Atrial Fibrillation Management—Results from a National Multi-Center Urgent Care Network Registry" Journal of Clinical Medicine 12, no. 21: 6704. https://doi.org/10.3390/jcm12216704
APA StyleLebovitz, S., Estryk, M., Zimmerman, D. R., Pollak, A., Luria, D., Amir, O., & Biton, Y. (2023). Trends in Atrial Fibrillation Management—Results from a National Multi-Center Urgent Care Network Registry. Journal of Clinical Medicine, 12(21), 6704. https://doi.org/10.3390/jcm12216704