
Influence of Brain Metastasis on Analgesia-Related Outcomes in Patients with Lung and Breast Cancers Treated with Naldemedine: A Propensity Score-Matched Analysis
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
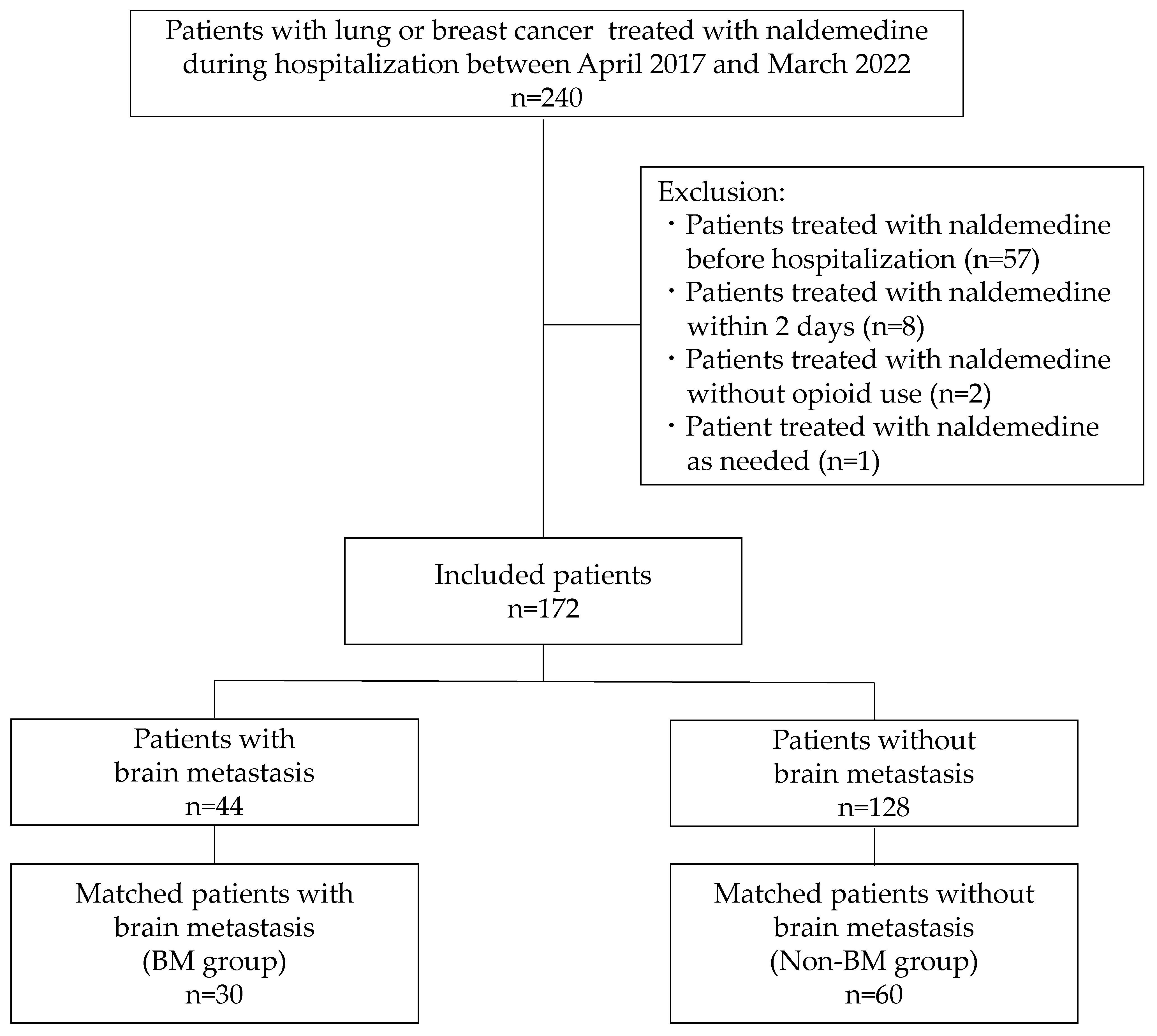
2.1. Study Design and Patient Selection
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
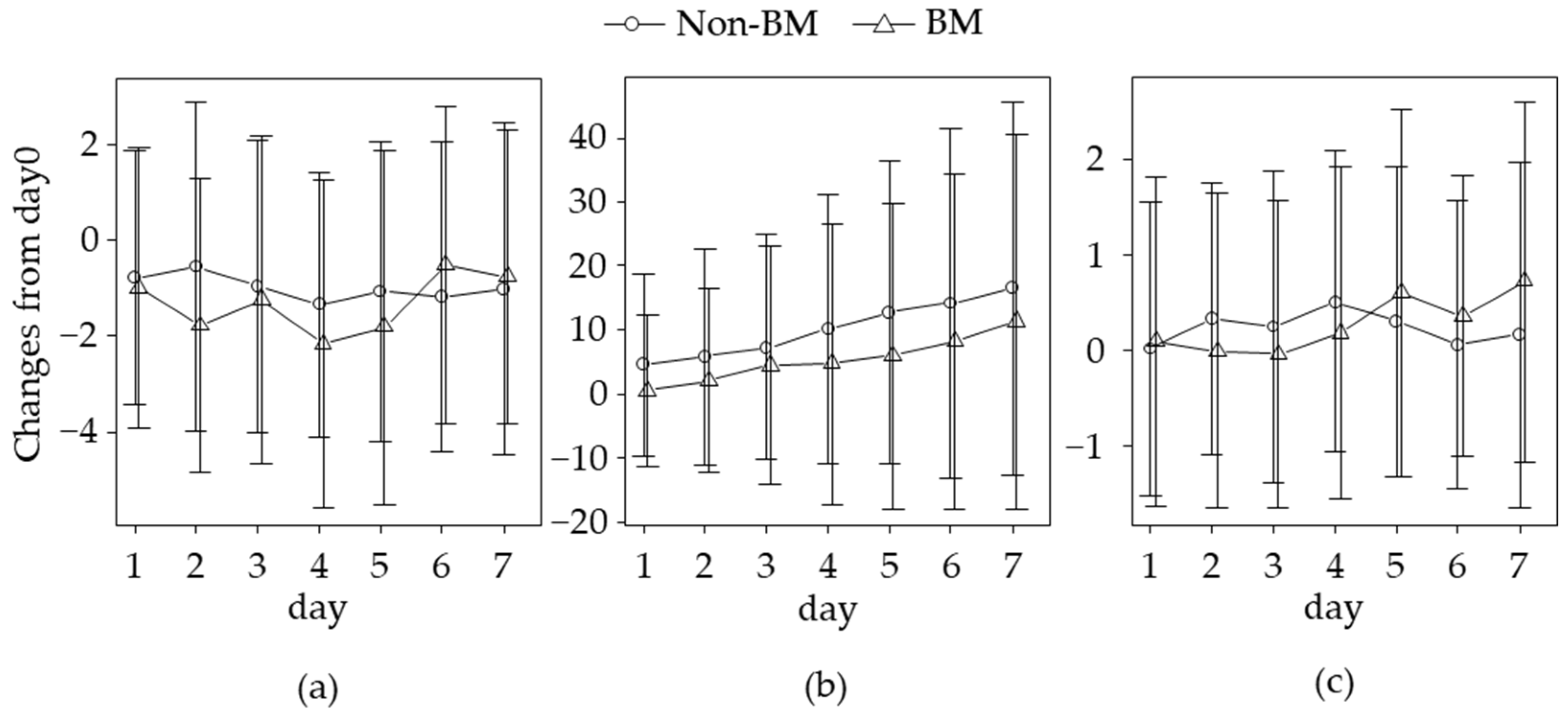
3.2. Changes in Analgesia-Related Outcomes
3.3. Association of BM and Outcome Changes over Time
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BBB | blood–brain barrier |
| BM | brain metastasis |
| CI | confidence interval |
| CNS | central nervous system |
| LS | least square |
| MMEs | morphine milligram equivalents |
| MOR | μ-opioid receptor |
| NRS | numeric rating scale |
| OIC | opioid-induced constipation |
| PAMORA | peripherally acting μ-opioid receptor antagonist |
| PSM | propensity-score matching |
References
- Müller-Lissner, S.; Bassotti, G.; Coffin, B.; Drewes, A.M.; Breivik, H.; Eisenberg, E.; Emmanuel, A.; Laroche, F.; Meissner, W.; Morlion, B. Opioid-Induced Constipation and Bowel Dysfunction: A Clinical Guideline. Pain Med. 2017, 18, 1837–1863. [Google Scholar] [CrossRef]
- Coluzzi, F.; Pappagallo, M. Opioid therapy for chronic noncancer pain: Practice guidelines for initiation and maintenance of therapy. Minerva Anestesiol. 2005, 71, 425–433. [Google Scholar]
- Coluzzi, F.; Scerpa, M.S.; Pergolizzi, J. Naldemedine: A New Option for OIBD. J. Pain Res. 2020, 13, 1209–1222. [Google Scholar] [CrossRef]
- Watari, R.; Matsuda, A.; Ohnishi, S.; Hasegawa, H. Minimal contribution of P-gp on the low brain distribution of naldemedine, a peripherally acting μ-opioid receptor antagonist. Drug Metab. Pharmacokinet. 2019, 34, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Arvanitis, C.D.; Ferraro, G.B.; Jain, R.K. The blood-brain barrier and blood-tumour barrier in brain tumours and metastases. Nat. Rev. Cancer 2020, 20, 26–41. [Google Scholar] [CrossRef] [PubMed]
- Papademetriou, I.T.; Porter, T. Promising approaches to circumvent the blood-brain barrier: Progress, pitfalls and clinical prospects in brain cancer. Ther. Deliv. 2015, 6, 989–1016. [Google Scholar] [CrossRef] [PubMed]
- Warren, K.E. Beyond the Blood:Brain Barrier: The Importance of Central Nervous System (CNS) Pharmacokinetics for the Treatment of CNS Tumors, Including Diffuse Intrinsic Pontine Glioma. Front. Oncol. 2018, 8, 239. [Google Scholar] [CrossRef]
- Kanemasa, T.; Koike, K.; Arai, T.; Ono, H.; Horita, N.; Chiba, H.; Nakamura, A.; Morioka, Y.; Kihara, T.; Hasegawa, M. Pharmacologic effects of naldemedine, a peripherally acting μ-opioid receptor antagonist, in in vitro and in vivo models of opioid-induced constipation. Neurogastroenterol. Motil. 2019, 31, e13563. [Google Scholar] [CrossRef]
- Katakami, N.; Harada, T.; Murata, T.; Shinozaki, K.; Tsutsumi, M.; Yokota, T.; Arai, M.; Tada, Y.; Narabayashi, M.; Boku, N. Randomized Phase III and Extension Studies of Naldemedine in Patients with Opioid-Induced Constipation and Cancer. J. Clin. Oncol. 2017, 35, 3859–3866. [Google Scholar] [CrossRef]
- Hale, M.; Wild, J.; Reddy, J.; Yamada, T.; Arjona Ferreira, J.C. Naldemedine versus placebo for opioid-induced constipation (COMPOSE-1 and COMPOSE-2): Two multicentre, phase 3, double-blind, randomised, parallel-group trials. Lancet Gastroenterol. Hepatol. 2017, 2, 555–564. [Google Scholar] [CrossRef] [PubMed]
- Webster, L.R.; Nalamachu, S.; Morlion, B.; Reddy, J.; Baba, Y.; Yamada, T.; Arjona Ferreira, J.C. Long-term use of naldemedine in the treatment of opioid-induced constipation in patients with chronic noncancer pain: A randomized, double-blind, placebo-controlled phase 3 study. Pain 2018, 159, 987–994. [Google Scholar] [CrossRef] [PubMed]
- Osaka, I.; Ishiki, H.; Yokota, T.; Tada, Y.; Sato, H.; Okamoto, M.; Satomi, E. Safety and efficacy of naldemedine in cancer patients with opioid-induced constipation: A pooled, subgroup analysis of two randomised controlled studies. ESMO Open 2019, 4, e000527. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Feng, Y.; Chen, L.; Yu, J.; Van Ongeval, C.; Bormans, G.; Li, Y.; Ni, Y. Towards updated understanding of brain metastasis. Am. J. Cancer Res. 2022, 12, 4290–4311. [Google Scholar] [PubMed]
- Archie, S.R.; Al Shoyaib, A.; Cucullo, L. Blood-Brain Barrier Dysfunction in CNS Disorders and Putative Therapeutic Targets: An Overview. Pharmaceutics 2021, 13, 1779. [Google Scholar] [CrossRef] [PubMed]
- Streicher, J.M.; Bilsky, E.J. Peripherally Acting μ-Opioid Receptor Antagonists for the Treatment of Opioid-Related Side Effects: Mechanism of Action and Clinical Implications. J. Pharm. Pract. 2018, 31, 658–669. [Google Scholar] [CrossRef] [PubMed]
- Rekatsina, M.; Paladini, A.; Drewes, A.M.; Ayob, F.; Viswanath, O.; Urits, I.; Corli, O.; Pergolizzi, J., Jr.; Varrassi, G. Efficacy and Safety of Peripherally Acting μ-Opioid Receptor Antagonist (PAMORAs) for the Management of Patients with Opioid-Induced Constipation: A Systematic Review. Cureus 2021, 13, e16201. [Google Scholar] [CrossRef] [PubMed]
- Brenner, D.M.; Slatkin, N.E.; Stambler, N.; Israel, R.J.; Coluzzi, P.H. The influence of brain metastases on the central nervous system effects of methylnaltrexone: A post hoc analysis of 3 randomized, double-blind studies. Support. Care Cancer 2021, 29, 5209–5218. [Google Scholar] [CrossRef] [PubMed]
- Upton, D.H.; Ung, C.; George, S.M.; Tsoli, M.; Kavallaris, M.; Ziegler, D.S. Challenges and opportunities to penetrate the blood-brain barrier for brain cancer therapy. Theranostics 2022, 12, 4734–4752. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Before PSM | After PSM | |||||
|---|---|---|---|---|---|---|
| BM n = 44 | Non-BM n = 128 | SMD | BM n = 30 | Non-BM n = 60 | SMD | |
| Age, years | 73.0 (63.0, 80.0) | 68.5 (60.0, 71.3) | 0.396 | 69.0 (62.3, 71.0) | 69.0 (59.0, 74.0) | 0.031 |
| Sex | ||||||
| Male | 29 (65.9) | 79 (61.7) | 0.087 | 20 (66.7) | 37 (61.7) | 0.104 |
| Female | 15 (34.1) | 49 (38.3) | 10 (33.3) | 23 (38.3) | ||
| BMI, kg/m2 | 21.1 (18.0, 22.5) | 20.4 (18.0, 23.2) | 0.065 | 21.6 (18.2, 22.3) | 21.0 (18.7, 23.1) | 0.053 |
| Cancer type | ||||||
| Lung cancer | 38 (86.4) | 104 (81.2) | 0.139 | 25 (83.3) | 49 (81.7) | 0.044 |
| Breast cancer | 6 (13.6) | 24 (18.8) | 5 (16.7) | 11 (18.3) | ||
| Stage | ||||||
| I–II | 2 (4.5) | 17 (13.3) | 0.377 | 2 (6.7) | 5 (8.3) | 0.160 |
| III | 5 (11.4) | 22 (17.2) | 4 (13.3) | 11 (18.3) | ||
| IV | 37 (84.1) | 89 (69.5) | 24 (80.0) | 44 (73.3) | ||
| Recurrent cancer | 7 (15.9) | 38 (29.7) | 0.333 | 6 (20.0) | 13 (21.7) | 0.041 |
| Bone metastasis | 28 (63.6) | 65 (50.8) | 0.262 | 13 (43.3) | 23 (38.3) | 0.102 |
| RT for pain relief | 20 (45.5) | 94 (73.4) | 0.595 | 15 (50.0) | 32 (53.3) | 0.067 |
| Coexisting disease | ||||||
| Hypertension | 15 (34.1) | 49 (38.3) | 0.087 | 11 (36.7) | 23 (38.3) | 0.034 |
| Stroke | 6 (13.6) | 20 (15.6) | 0.056 | 4 (13.3) | 7 (11.7) | 0.050 |
| Schizophrenia | 4 (9.1) | 0 (0.0) | 0.447 | 0 (0.0) | 0 (0.0) | <0.001 |
| Depression | 3 (6.8) | 4 (3.1) | 0.171 | 0 (0.0) | 1 (1.7) | 0.184 |
| Epilepsy | 3 (6.8) | 2 (1.6) | 0.265 | 0 (0.0) | 1 (1.7) | 0.184 |
| Day 0 outcome values | ||||||
| NRS | 4.0 (1.3, 6.0) | 4.0 (1.0, 6.0) | 0.015 | 4.0 (1.0, 6.0) | 4.0 (2.0, 6.0) | 0.053 |
| MMEs | 30.0 (20.0, 45.0) | 22.5 (15.0, 60.0) | 0.106 | 30.0 (18.8, 45.0) | 22.5 (15.0, 50.0) | 0.106 |
| Number of rescues | 1.0 (0.0, 2.0) | 1.0 (0.0, 2.0) | 0.114 | 1.0 (0.0, 2.0) | 1.0 (0.0, 1.0) | 0.140 |
| LS Mean Changes in BM (95% CI) | LS Mean Changes in Non-BM (95% CI) | Difference: BM Minus Non-BM (95% CI) | p-Value | |
|---|---|---|---|---|
| NRS | ||||
| Day 3 | −1.44 (−2.45, −0.43) | −0.81 (−1.48, −0.14) | −0.63 (−1.84, 0.58) | 0.305 |
| Day 7 | −1.29 (−2.42, −0.15) | −0.99 (−1.76, −0.22) | −0.30 (−1.67, 0.11) | 0.666 |
| MMEs | ||||
| Day 3 | 3.78 (−3.30, 10.90) | 8.10 (3.14, 13.10) | −4.32 (−12.97, 4.33) | 0.323 |
| Day 7 | 10.3 (2.81, 17.80) | 15.9 (10.63, 21.10) | −5.57 (−14.71, 3.57) | 0.230 |
| Number of rescues | ||||
| Day 3 | 0.13 (−0.34, 0.61) | 0.26 (−0.08, 0.60) | −0.13 (−0.72, 0.45) | 0.651 |
| Day 7 | 0.52 (−0.03, 1.07) | 0.37 (−0.02, 0.76) | 0.15 (−0.53, 0.82) | 0.668 |
| Coefficient | 95% CI | p-Value | |
|---|---|---|---|
| NRS | |||
| BM (vs. non-BM) | −0.88 | −2.29, 0.54 | 0.229 |
| Days | −0.04 | −0.16, 0.07 | 0.467 |
| Interaction of BM and days | 0.08 | −0.12, 0.29 | 0.435 |
| MMEs | |||
| BM (vs. non-BM) | −3.38 | −12.57, 5.81 | 0.400 |
| Days | 1.94 | 1.40, 2.48 | <0.001 |
| Interaction of BM and ays | −0.31 | −1.26, 0.64 | 0.519 |
| Number of rescues | |||
| BM (vs. non-BM) | −0.34 | −1.03, 0.34 | 0.331 |
| Days | 0.03 | −0.03, 0.09 | 0.382 |
| Interaction of BM and days | 0.07 | −0.04, 0.18 | 0.195 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hanamoto, A.; Koseki, T.; Utsunomiya, A.; Ishihara, T.; Tobe, T.; Kondo, M.; Kijima, Y.; Matsuoka, H.; Mizuno, T.; Hayashi, T.; et al. Influence of Brain Metastasis on Analgesia-Related Outcomes in Patients with Lung and Breast Cancers Treated with Naldemedine: A Propensity Score-Matched Analysis. J. Clin. Med. 2023, 12, 6997. https://doi.org/10.3390/jcm12226997
Hanamoto A, Koseki T, Utsunomiya A, Ishihara T, Tobe T, Kondo M, Kijima Y, Matsuoka H, Mizuno T, Hayashi T, et al. Influence of Brain Metastasis on Analgesia-Related Outcomes in Patients with Lung and Breast Cancers Treated with Naldemedine: A Propensity Score-Matched Analysis. Journal of Clinical Medicine. 2023; 12(22):6997. https://doi.org/10.3390/jcm12226997
Chicago/Turabian StyleHanamoto, Aya, Takenao Koseki, Ayaka Utsunomiya, Takuma Ishihara, Takao Tobe, Masashi Kondo, Yuko Kijima, Hiroshi Matsuoka, Tomohiro Mizuno, Takahiro Hayashi, and et al. 2023. "Influence of Brain Metastasis on Analgesia-Related Outcomes in Patients with Lung and Breast Cancers Treated with Naldemedine: A Propensity Score-Matched Analysis" Journal of Clinical Medicine 12, no. 22: 6997. https://doi.org/10.3390/jcm12226997
APA StyleHanamoto, A., Koseki, T., Utsunomiya, A., Ishihara, T., Tobe, T., Kondo, M., Kijima, Y., Matsuoka, H., Mizuno, T., Hayashi, T., & Yamada, S. (2023). Influence of Brain Metastasis on Analgesia-Related Outcomes in Patients with Lung and Breast Cancers Treated with Naldemedine: A Propensity Score-Matched Analysis. Journal of Clinical Medicine, 12(22), 6997. https://doi.org/10.3390/jcm12226997