
The Efficacy and Safety of Rebamipide Ophthalmic Suspension (OPC-12759) in Patients with Dry Eye Disease: A Systematic Review of Randomized Controlled Trials

 ,
,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
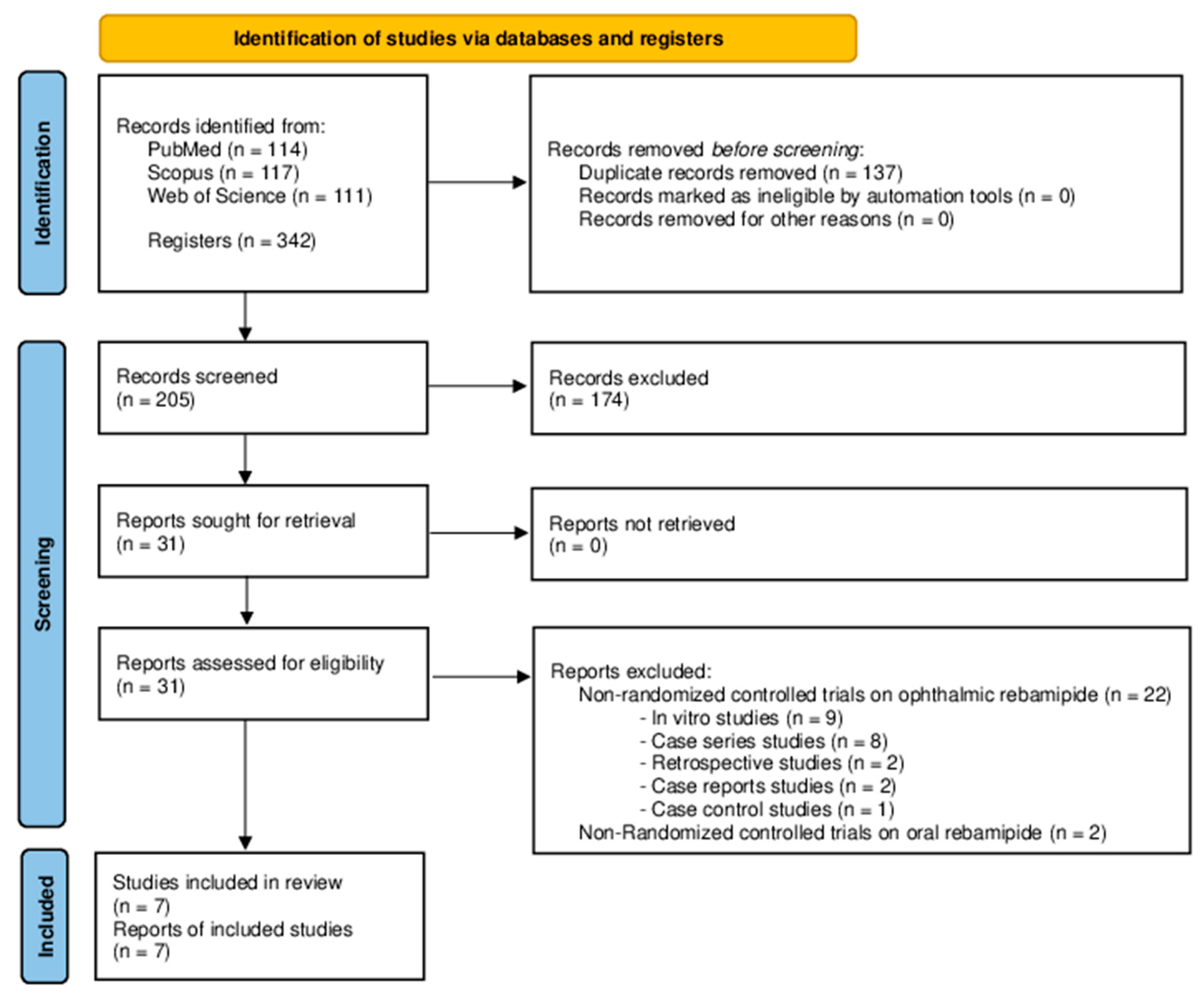
2.1. Data Sources and Search Strategy
2.2. Study Selection
2.3. Quality Assessment and Data Extraction
3. Results
3.1. Study Characterisitcs
3.2. Outcomes

{kind=link}
{kind=link}
{kind=link}
| Author (Date) | Design | F/U 1 | Patients | Age 2 | Sex (F/M) | Eyes | Inclusion Criteria | Intervention | Control | Posology 3 (TG/CG) | CoI |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Kinoshita et al. [21] 2012 | MT DM | 1 | 308 | 55.2 [20 to 86] | 269/39 | 308 | DED | REB (1%) REB (2%) | Placebo | 4/4 | Yes |
| Kinoshita et al. [20] 2013 | MT SM | 1 | 188 | 56.6 ± 17.4 | 163/25 | 188 | DED | REB (2%) | AT (SH 0.1%) | 4/6 | Yes |
| Igarashi et al. [36] 2015 | MN | 1 | 25 | 34.1 ± 10.8 | 22/3 | 50 | DED refractive surgery | REB (2%) | AT (NR%) | 4/4 | No |
| Kato et al. [38] 2017 | MT SM | 1 | 33 | 71.1 ± 6.8 | 23/10 | 33 | DED cataract surgery | REB (2%) Diclofenac (0.1%) | Diclofenac (0.1%) | 4/3 | Yes |
| Kobashi et al. [37] 2017 | MN | 1 | 40 | 70.4 ± 15.8 | 19/21 | 40 | DED PK | REB (2%) | DQS (3%) | 4/4 | No |
| Shimazaki et al. [33] 2017 | MT UM | 1 | 67 | 39.9 ± 9.6 | 47/20 | 67 | DED | REB (2%) | DQS (3%) | 4/6 | Yes |
| Jain et al. [22] 2023 | MN | 3 | 80 | NR [18 to 75] | 47/33 | 160 | DED | REB (2%) | AT (CMC 0.5%) | 4/4 | No |
| Author (Date) | Rebamipide Group | Control Group | Inter-Group Differences 2 | F/A | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| DEQS (0–100) | TBUT, s | ST, mm | tCFS | DEQS (0–100) | TBUT, s | ST, mm | tCFS | DEQS (0–100) | TBUT, s | ST, mm | tCFS | |||
| Kinoshita et al. [21] 2012 | Baseline | NR | 2.8 ± 0.2 | 2.5 ± 0.3 | 7 ± 0.2 | NR | 2.9 ± 0.2 | 2.4 ± 0.2 | 6.9 ± 0.2 | - | 0.5 * | 0.5 | −1.8 * | F |
| Last visit | NR | 3.5 ± 0.3 | 3.5 ± 0.2 | 3.4 ± 0.1 | NR | 3.1 ± 0.3 | 2.9 ± 0.3 | 5.1 ± 0.2 | ||||||
| Difference 1 | - | 0.7 * | 1 | −3.6 * | - | 0.2 | 0.5 | −1.8 | ||||||
| Kinoshita et al. [20] 2013 | Baseline | NR | 2.7 ± 0.1 | 2.5 ± 0.2 | 7 ± 0.2 | NR | 2.5 ± 0.1 | 2.3 ± 0.2 | 7 ± 0.2 | - | 0.2 | −0.5 | −0.8 * | F |
| Last visit | NR | 3.5 ± 0.1 | 3 ± 0.2 | 3.3 ± 0.3 | NR | 3.1 ± 0.1 | 3.3 ± 0.3 | 4.1 ± 0.8 | ||||||
| Difference 1 | - | 0.8 | 0.5 | −3.7 * | - | 0.6 | 1 | −2.9 | ||||||
| Igarashi et al. [36] 2015 | Baseline | NR | 2.2 ± 0.7 | 11.4 ± 9 | 4.3 ± 1 | NR | 2.7 ± 0.8 | 13.7 ± 11.9 | 4.1 ± 1.3 | - | 2.2 | 1 | −2.1 | F |
| Last visit | NR | 4.5 ± 1.7 | 14.9 ± 7.4 | 1.9 ± 1 | NR | 2.8 ± 0.8 | 16.2 ± 11.7 | 3.6 ± 1.2 | ||||||
| Difference 1 | - | 2.3 * | 3.5 * | −2.4 * | - | 0.1 | 2.5 | −0.5 | ||||||
| Kato et al. [38] 2017 | Baseline | NR | 6.9 ± 2.2 | NR | NR | NR | 7.4 ± 2.7 | NR | NR | - | 0.5 | - | - | F |
| Last visit | NR | 4.2 ± 3.1 | NR | NR | NR | 4.2 ± 2.9 | NR | NR | ||||||
| Difference 1 | - | −2.7 * | - | - | - | −3.2 * | - | - | ||||||
| Kobashi et al. [37] 2017 | Baseline | 28.8 ± 22 | 3.3 ± 1.4 | NR | 5.1 ± 3 | 23.3 ± 21 | 3.9 ± 1.5 | NR | 4.5 ± 3 | −6.4 | 0.6 | - | −1 | F |
| Last visit | 17.3 ± 19 | 5.9 ± 1.5 | NR | 1.7 ± 1.6 | 18.2 ± 20 | 5.9 ± 1.6 | NR | 2.1 ± 2 | ||||||
| Difference 1 | −11.5 | 2.6 * | - | −3.4 * | −5.1 | 2 * | - | −2.4 * | ||||||
| Shimazaki et al. [33] 2017 | Baseline | 48.6 ± 18 | 3.2 ± 0.8 | 15.2 ± 10.7 | 1.6 ± 1 | 44.7 ± 20 | 3.4 ± 1 | 13.7 ± 9.5 | 1.2 ± 0.7 | −0.6 | 0.5 | - | −0.2 | F |
| Last visit | 24.8 ± 19 | 4.2 ± 0.8 | NR | 0.8 ± 0.4 | 21.5 ± 17 | 3.9 ± 0.9 | NR | 0.6 ± 0.6 | ||||||
| Difference 1 | −23.8 * | 1 * | - | −0.8 * | −23.2 * | 0.5 | - | −0.6 | ||||||
| Jain et al. [22] 2023 | Baseline | NR | NR | NR | NR | NR | NR | NR | NR | - | - | - | - | F |
| Last visit | NR | NR | NR | NR | NR | NR | NR | NR | ||||||
| Difference 1 | - | - | - | - | - | - | - | - | ||||||
| Author (Date) | Rebamipide Group | Control Group | Inter-Group Differences 1 | |
|---|---|---|---|---|
| Kinoshita et al. [21] 2012 | Ocular AEs, % | 5.9 | 8.7 | −2.8 |
| Non-ocular AEs, % | 20 | 8.7 | 11.3 | |
| Kinoshita et al. [20] 2013 | Ocular Aes, % | 7.5 | 9.4 | −1.9 |
| Non-ocular AEs, % | 16.1 | 2.1 | 14 | |
| Igarashi et al. [36] 2015 | Ocular AEs, % | NR | NR | - |
| Non-ocular AEs, % | NR | NR | - | |
| Kato et al. [38] 2017 | Ocular AEs, % | NR | NR | - |
| Non-ocular AEs, % | NR | NR | - | |
| Kobashi et al. [37] 2017 | Ocular AEs, % | NR | NR | - |
| Non-ocular AEs, % | NR | NR | - | |
| Shimazaki et al. [33] 2017 | Ocular AEs, % | NR | NR | - |
| Non-ocular AEs, % | NR | NR | - | |
| Jain et al. [22] 2023 | Ocular AEs, % | NR | NR | - |
| Non-ocular AEs, % | 10 | NR | - |
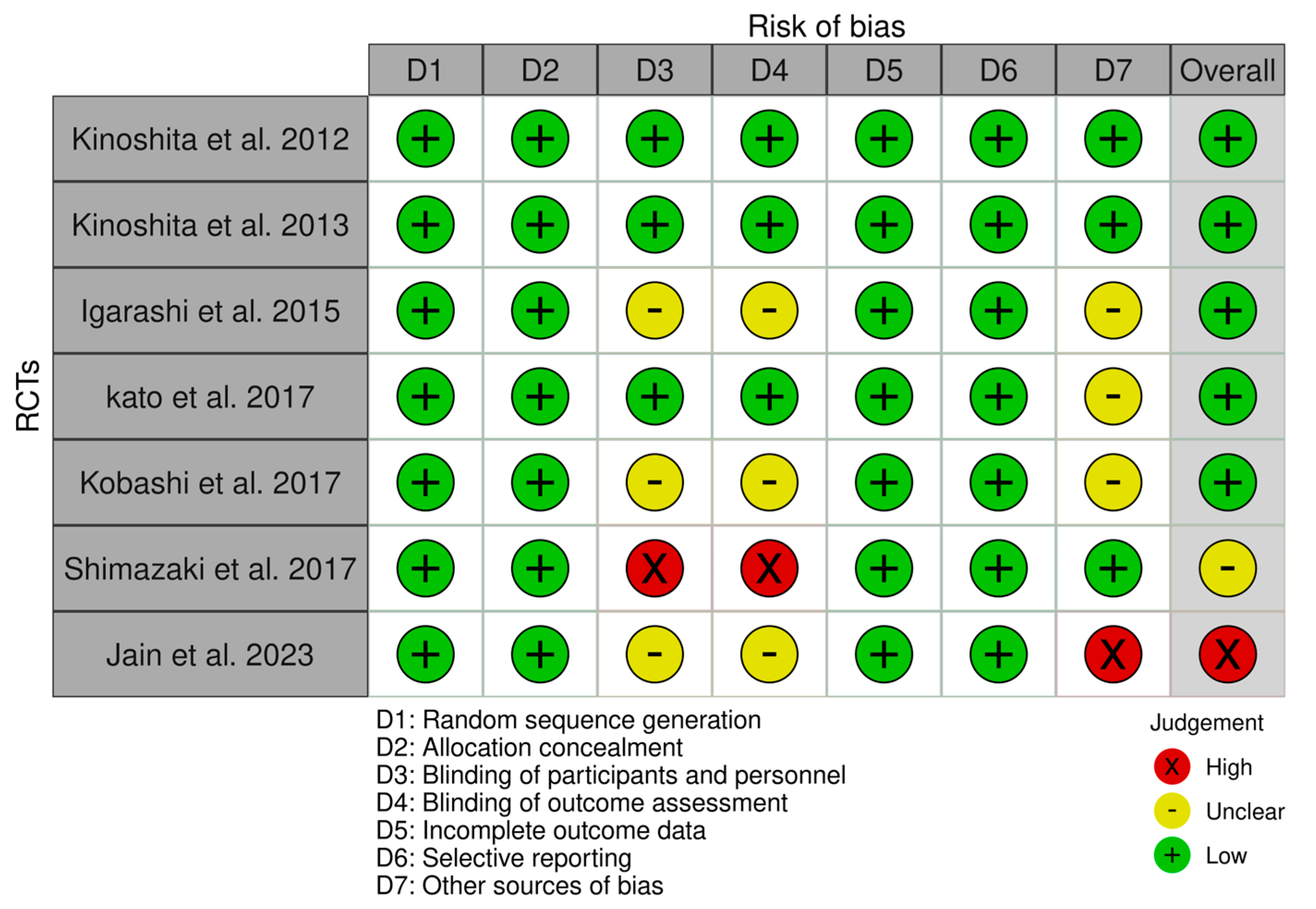
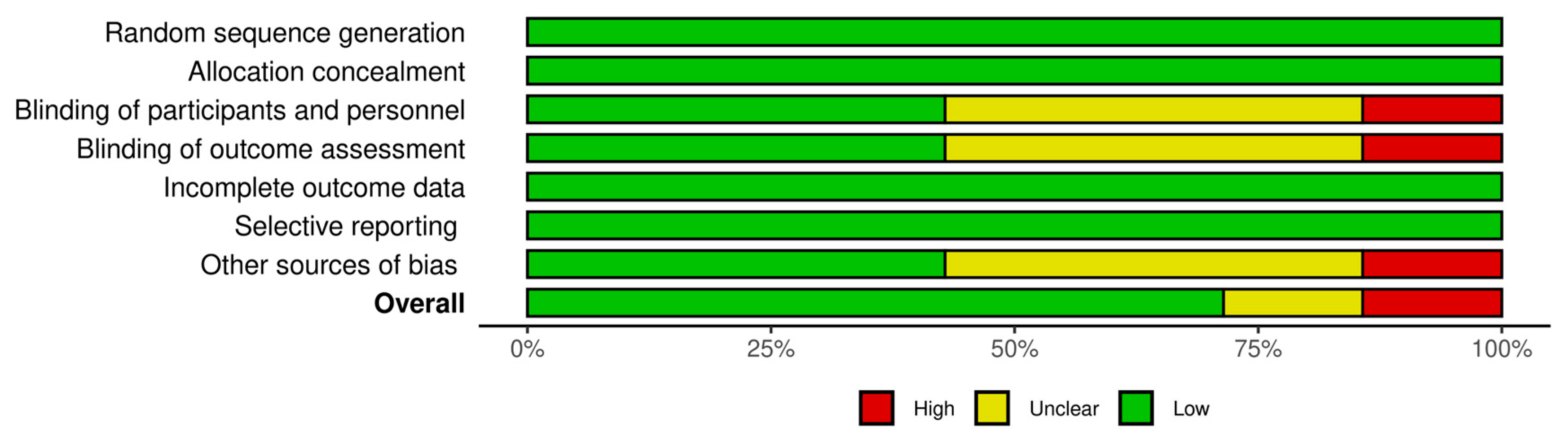
3.3. Risk of Bias
4. Discussion
4.1. REB Ophthalmic Suspension Efficacy
4.2. REB Ophthalmic Suspension Safety
4.3. REB Ophthalmic Suspension vs. DQS Ophthalmic Solution
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Craig, J.P.; Nichols, K.K.; Akpek, E.K.; Caffery, B.; Dua, H.S.; Joo, C.K.; Liu, Z.; Nelson, J.D.; Nichols, J.J.; Tsubota, K.; et al. TFOS DEWS II Definition and Classification Report. Ocul. Surf. 2017, 15, 276–283. [Google Scholar] [CrossRef]
- Stapleton, F.; Alves, M.; Bunya, V.Y.; Jalbert, I.; Lekhanont, K.; Malet, F.; Na, K.S.; Schaumberg, D.; Uchino, M.; Vehof, J.; et al. TFOS DEWS II Epidemiology Report. Ocul. Surf. 2017, 15, 334–365. [Google Scholar] [CrossRef] [PubMed]
- Stern, M.E.; Gao, J.; Siemasko, K.F.; Beuerman, R.W.; Pflugfelder, S.C. The Role of the Lacrimal Functional Unit in the Pathophysiology of Dry Eye. Exp. Eye Res. 2004, 78, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Bron, A.J.; de Paiva, C.S.; Chauhan, S.K.; Bonini, S.; Gabison, E.E.; Jain, S.; Knop, E.; Markoulli, M.; Ogawa, Y.; Perez, V.; et al. TFOS DEWS II Pathophysiology Report. Ocul. Surf. 2017, 15, 438–510. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.; Downie, L.E.; Korb, D.; Benitez-del-Castillo, J.M.; Dana, R.; Deng, S.X.; Dong, P.N.; Geerling, G.; Hida, R.Y.; Liu, Y.; et al. TFOS DEWS II Management and Therapy Report. Ocul. Surf. 2017, 15, 575–628. [Google Scholar] [CrossRef] [PubMed]
- Kashima, T.; Itakura, H.; Akiyama, H.; Kishi, S. Rebamipide Ophthalmic Suspension for the Treatment of Dry Eye Syndrome: A Critical Appraisal. Clin. Ophthalmol. 2014, 8, 1003–1010. [Google Scholar] [CrossRef]
- Jaafar, M.H.; Safi, S.Z.; Tan, M.P.; Rampal, S.; Mahadeva, S. Efficacy of Rebamipide in Organic and Functional Dyspepsia: A Systematic Review and Meta-Analysis. Dig. Dis. Sci. 2018, 63, 1250–1260. [Google Scholar] [CrossRef]
- He, Q.; Liu, M.; Rong, Z.; Liang, H.; Xu, X.; Sun, S.; Lei, Y.; Li, P.; Meng, H.; Zheng, R.; et al. Rebamipide Attenuates Alcohol-Induced Gastric Epithelial Cell Injury by Inhibiting Endoplasmic Reticulum Stress and Activating Autophagy-Related Proteins. Eur. J. Pharmacol. 2022, 922, 17489. [Google Scholar] [CrossRef]
- Uchino, Y. The Ocular Surface Glycocalyx and Its Alteration in Dry Eye Disease: A Review. Investig. Ophthalmol. Vis. Sci. 2018, 59, DES157–DES162. [Google Scholar] [CrossRef]
- Zhao, H.; Jumblatt, J.E.; Wood, T.O.; Jumblatt, M.M. Quantification of MUC5AC Protein in Human Tears. Cornea 2001, 20, 873–877. [Google Scholar] [CrossRef]
- Ablamowicz, A.F.; Nichols, J.J. Ocular Surface Membrane-Associated Mucins. Ocul. Surf. 2016, 14, 331–341. [Google Scholar] [CrossRef] [PubMed]
- Gipson, I.K.; Argüeso, P. Role of Mucins in the Function of the Corneal and Conjunctival Epithelia. Int. Rev. Cytol. 2003, 231, 1–49. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Carrasco, R.; Argüeso, P.; Fini, M.E. Membrane-Associated Mucins of the Human Ocular Surface in Health and Disease. Ocul. Surf. 2021, 21, 313–330. [Google Scholar] [CrossRef]
- Itoh, S.; Itoh, K.; Shinohara, H. Regulation of Human Corneal Epithelial Mucins by Rebamipide. Curr. Eye Res. 2014, 39, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Takeji, Y.; Urashima, H.; Aoki, A.; Shinohara, H. Rebamipide Increases the Mucin-like Glycoprotein Production in Corneal Epithelial Cells. J. Ocul. Pharmacol. Ther. 2012, 28, 259–263. [Google Scholar] [CrossRef] [PubMed]
- Kase, S.; Shinohara, T.; Kase, M.; Ishida, S. Effect of Topical Rebamipide on Goblet Cells in the Lid Wiper of Human Conjunctiva. Exp. Ther. Med. 2017, 13, 3516–3522. [Google Scholar] [CrossRef]
- Fukuda, K.; Ishida, W.; Tanaka, H.; Harada, Y.; Fukushima, A. Inhibition by Rebamipide of Cytokine-Induced or Lipopolysaccharide-Induced Chemokine Synthesis in Human Corneal Fibroblasts. Br. J. Ophthalmol. 2014, 98, 1751–1755. [Google Scholar] [CrossRef]
- Tanaka, H.; Fukuda, K.; Ishida, W.; Harada, Y.; Sumi, T.; Fukushima, A. Rebamipide Increases Barrier Function and Attenuates TNFα-Induced Barrier Disruption and Cytokine Expression in Human Corneal Epithelial Cells. Br. J. Ophthalmol. 2013, 97, 912–916. [Google Scholar] [CrossRef]
- Sotozono, C.; Ueta, M.; Kinoshita, S. Japan: Diagnosis and Management of Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis With Severe Ocular Complications. Front. Med. 2021, 8, 657327. [Google Scholar] [CrossRef]
- Kinoshita, S.; Oshiden, K.; Awamura, S.; Suzuki, H.; Nakamichi, N.; Yokoi, N. A Randomized, Multicenter Phase 3 Study Comparing 2% Rebamipide (OPC-12759) with 0.1% Sodium Hyaluronate in the Treatment of Dry Eye. Ophthalmology 2013, 120, 1158–1165. [Google Scholar] [CrossRef]
- Kinoshita, S.; Awamura, S.; Oshiden, K.; Nakamichi, N.; Suzuki, H.; Yokoi, N. Rebamipide (OPC-12759) in the Treatment of Dry Eye: A Randomized, Double-Masked, Multicenter, Placebo-Controlled Phase II Study. Ophthalmology 2012, 119, 2471–2478. [Google Scholar] [CrossRef] [PubMed]
- Jain, K.; Jaju, M.; Yadav, D. Efficacy and Safety of Topical 2% Rebamipide Ophthalmic Suspension in Dry Eye Disease at Tertiary Care Centre. Indian J. Ophthalmol. 2023, 71, 1598–1602. [Google Scholar] [CrossRef] [PubMed]
- Simsek, C.; Dogru, M.; Shinzawa, M.; Den, S.; Kojima, T.; Iseda, H.; Suzuki, M.; Shibasaki, Y.; Yoshida, N.; Shimazaki, J. The Efficacy of 2% Topical Rebamipide on Conjunctival Squamous Metaplasia and Goblet Cell Density in Dry Eye Disease. J. Ocul. Pharmacol. Ther. 2019, 35, 350–358. [Google Scholar] [CrossRef] [PubMed]
- Sakane, Y.; Yamaguchi, M.; Shiraishi, A. Retrospective Observational Study on Rebamipide Ophthalmic Suspension on Quality of Life of Dry Eye Disease Patients. J. Ophthalmol. 2019, 2019, 8145731. [Google Scholar] [CrossRef]
- Igarashi, T.; Kobayashi, M.; Yaguchi, C.; Fujimoto, C.; Suzuki, H.; Takahashi, H. Efficacy of Rebamipide Instillation for Contact Lens Discomfort With Dry Eye. Eye Contact Lens 2018, 44 (Suppl. 2), S137–S142. [Google Scholar] [CrossRef]
- Teshigawara, T.; Meguro, A.; Mizuki, N. The Effect of Rebamipide on Refractive Accuracy of Cataract Surgery in Patients with Dry Eye. Ophthalmol. Ther. 2022, 11, 603–611. [Google Scholar] [CrossRef]
- Teshigawara, T.; Meguro, A.; Mizuki, N. Impact of Perioperative Dry Eye Treatment with Rebamipide Versus Artificial Tears on Visual Outcomes After Cataract Surgery in Japanese Population. Ophthalmol. Ther. 2022, 11, 1479–1491. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 Explanation and Elaboration: Updated Guidance and Exemplars for Reporting Systematic Reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- DistillerSR. Version 2.35. DistillerSR Inc. 2022. Available online: https://www.distillersr.com/ (accessed on 30 July 2023).
- Wolffsohn, J.S.; Arita, R.; Chalmers, R.; Djalilian, A.; Dogru, M.; Dumbleton, K.; Gupta, P.K.; Karpecki, P.; Lazreg, S.; Pult, H.; et al. TFOS DEWS II Diagnostic Methodology Report. Ocul. Surf. 2017, 15, 539–574. [Google Scholar] [CrossRef]
- Sall, K.; Foulks, G.N.; Pucker, A.D.; Ice, K.L.; Zink, R.C.; Magrath, G. Validation of a Modified National Eye Institute Grading Scale for Corneal Fluorescein Staining. Clin. Ophthalmol. 2023, 17, 757–767. [Google Scholar] [CrossRef] [PubMed]
- Shimazaki, J.; Seika, D.; Saga, M.; Fukagawa, K.; Sakata, M.; Iwasaki, M.; Okano, T. A Prospective, Randomized Trial of Two Mucin Secretogogues for the Treatment of Dry Eye Syndrome in Office Workers. Sci. Rep. 2017, 7, 15210. [Google Scholar] [CrossRef] [PubMed]
- Campbell, M.; McKenzie, J.E.; Sowden, A.; Katikireddi, S.V.; Brennan, S.E.; Ellis, S.; Hartmann-Boyce, J.; Ryan, R.; Shepperd, S.; Thomas, J.; et al. Synthesis without Meta-Analysis (SWiM) in Systematic Reviews: Reporting Guideline. BMJ 2020, 368, l6890. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Igarashi, A.; Kamiya, K.; Kobashi, H.; Shimizu, K. Effect of Rebamipide Ophthalmic Suspension on Intraocular Light Scattering for Dry Eye After Corneal Refractive Surgery. Cornea 2015, 34, 895–900. [Google Scholar] [CrossRef] [PubMed]
- Kobashi, H.; Kamiya, K.; Shimizu, K. Randomized Comparison Between Rebamipide Ophthalmic Suspension and Diquafosol Ophthalmic Solution for Dry Eye After Penetrating Keratoplasty. J. Ocul. Pharmacol. Ther. 2017, 33, 13–18. [Google Scholar] [CrossRef]
- Kato, K.; Miyake, K.; Kondo, N.; Asano, S.; Takeda, J.; Takahashi, A.; Takashima, Y.; Kondo, M. Conjunctival Goblet Cell Density Following Cataract Surgery With Diclofenac Versus Diclofenac and Rebamipide: A Randomized Trial. Am. J. Ophthalmol. 2017, 181, 26–36. [Google Scholar] [CrossRef] [PubMed]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-Bias VISualization (Robvis): An R Package and Shiny Web App for Visualizing Risk-of-Bias Assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Baudouin, C.; Aragona, P.; Messmer, E.M.; Tomlinson, A.; Calonge, M.; Boboridis, K.G.; Akova, Y.A.; Geerling, G.; Labetoulle, M.; Rolando, M. Role of Hyperosmolarity in the Pathogenesis and Management of Dry Eye Disease: Proceedings of the OCEAN Group Meeting. Ocul. Surf. 2013, 11, 246–258. [Google Scholar] [CrossRef]
- Pflugfelder, S.C.; de Paiva, C.S. The Pathophysiology of Dry Eye Disease: What We Know and Future Directions for Research. Ophthalmology 2017, 124, S4–S13. [Google Scholar] [CrossRef]
- Mencucci, R.; Favuzza, E.; Decandia, G.; Cennamo, M.; Giansanti, F. Hyaluronic Acid/Trehalose Ophthalmic Solution in Reducing Post-Cataract Surgery Dry Eye Signs and Symptoms: A Prospective, Interventional, Randomized, Open-Label Study. J. Clin. Med. 2021, 10, 4699. [Google Scholar] [CrossRef] [PubMed]
- Labetoulle, M.; Benitez-Del-castillo, J.M.; Barabino, S.; Vanrell, R.H.; Daull, P.; Garrigue, J.S.; Rolando, M. Artificial Tears: Biological Role of Their Ingredients in the Management of Dry Eye Disease. Int. J. Mol. Sci. 2022, 23, 2434. [Google Scholar] [CrossRef] [PubMed]
- Prabhasawat, P.; Tesavibul, N.; Mahawong, W. A Randomized Double-Masked Study of 0.05% Cyclosporine Ophthalmic Emulsion in the Treatment of Meibomian Gland Dysfunction. Cornea 2012, 31, 1386–1393. [Google Scholar] [CrossRef] [PubMed]
- Tuan, H.I.; Chi, S.C.; Kang, Y.N. An Updated Systematic Review With Meta-Analysis Of Randomized Trials On Topical Cyclosporin A For Dry-Eye Disease. Drug Des. Devel Ther. 2020, 14, 265. [Google Scholar] [CrossRef]
- Shin, J.; Rho, C.R.; Hyon, J.Y.; Chung, T.Y.; Yoon, K.C.; Joo, C.K. A Randomized, Placebo-Controlled Phase II Clinical Trial of 0.01% or 0.02% Cyclosporin A with 3% Trehalose in Patients with Dry Eye Disease. J. Ocul. Pharmacol. Ther. 2021, 37, 4–11. [Google Scholar] [CrossRef]
- Pan, Q.; Angelina, A.; Marrone, M.; Stark, W.J.; Akpek, E.K. Autologous Serum Eye Drops for Dry Eye. Cochrane Database Syst. Rev. 2017, 2, CD009327. [Google Scholar] [CrossRef]
- Rodríguez Calvo-de-Mora, M.; Domínguez-Ruiz, C.; Barrero-Sojo, F.; Rodríguez-Moreno, G.; Antúnez Rodríguez, C.; Ponce Verdugo, L.; Hernández Lamas, M.D.C.; Hernández‐Guijarro, L.; Villalvilla Castillo, J.; Fernández‐Baca Casares, I.; et al. Autologous versus Allogeneic versus Umbilical Cord Sera for the Treatment of Severe Dry Eye Disease: A Double-Blind Randomized Clinical Trial. Acta Ophthalmol. 2022, 100, e396–e408. [Google Scholar] [CrossRef]
- Ozdemir, S.; Yeo, S.W.J.; Lee, J.J.; Bhaskar, A.; Finkelstein, E.; Tong, L. Patient Medication Preferences for Managing Dry Eye Disease: The Importance of Medication Side Effects. Patient 2022, 15, 679–690. [Google Scholar] [CrossRef]
- Uchino, M.; Yokoi, N.; Shimazaki, J.; Hori, Y.; Tsubota, K. Adherence to Eye Drops Usage in Dry Eye Patients and Reasons for Non-Compliance: A Web-Based Survey. J. Clin. Med. 2022, 11, 367. [Google Scholar] [CrossRef]
- Messmer, E.; Chan, C.; Asbell, P.; Johnson, G.; Sloesen, B.; Cook, N. Comparing the Needs and Preferences of Patients with Moderate and Severe Dry Eye Symptoms across Four Countries. BMJ Open Ophthalmol. 2019, 4, e000360. [Google Scholar] [CrossRef]
- Sakane, Y.; Yamaguchi, M.; Yokoi, N.; Uchino, M.; Dogru, M.; Oishi, T.; Ohashi, Y.; Ohashi, Y. Development and Validation of the Dry Eye-Related Quality-of-Life Score Questionnaire. JAMA Ophthalmol. 2013, 131, 1331–1338. [Google Scholar] [CrossRef] [PubMed]
- Tananuvat, N.; Tansanguan, S.; Wongpakaran, N.; Wongpakaran, T. Reliability, Validity, and Responsiveness of the Thai Version of the Dry Eye-Related Quality-of-Life Score Questionnaire. PLoS ONE 2022, 17, e0271228. [Google Scholar] [CrossRef] [PubMed]
- Shimmura, S.; Ono, M.; Shinozaki, K.; Toda, I.; Takamura, E.; Mashima, Y.; Tsubota, K. Sodium Hyaluronate Eyedrops in the Treatment of Dry Eyes. Br. J. Ophthalmol. 1995, 79, 1007–1011. [Google Scholar] [CrossRef] [PubMed]
- Sall, K.; Stevenson, O.D.; Mundorf, T.K.; Reis, B.L. Two Multicenter Randomized Studies of the Efficacy and Safety of Cyclosporine Ophthalmic Emulsion in Moderate to Severe Dry Eye Disease. Ophthalmology 2000, 107, 631–639. [Google Scholar] [CrossRef] [PubMed]
- Kahook, M.Y.; Noecker, R.J. Comparison of Corneal and Conjunctival Changes after Dosing of Travoprost Preserved with SofZia, Latanoprost with 0.02% Benzalkonium Chloride, and Preservative-Free Artificial Tears. Cornea 2008, 27, 339–343. [Google Scholar] [CrossRef]
- Kahook, M.Y.; Noecker, R. Quantitative Analysis of Conjunctival Goblet Cells after Chronic Application of Topical Drops. Adv. Ther. 2008, 25, 743–751. [Google Scholar] [CrossRef]
- Liang, H.; Brignole-Baudouin, F.; Riancho, L.; Baudouin, C. Reduced in Vivo Ocular Surface Toxicity with Polyquad-Preserved Travoprost versus Benzalkonium-Preserved Travoprost or Latanoprost Ophthalmic Solutions. Ophthalmic Res. 2012, 48, 89–101. [Google Scholar] [CrossRef]
- Straub, M.; Bron, A.M.; Muselier-Mathieu, A.; Creuzot-Garcher, C. Long-Term Outcome after Topical Ciclosporin in Severe Dry Eye Disease with a 10-Year Follow-Up. Br. J. Ophthalmol. 2016, 100, 1547–1550. [Google Scholar] [CrossRef]
- Sheppard, J.D.; Torkildsen, G.L.; Lonsdale, J.D.; D’Ambrosio, F.A.; McLaurin, E.B.; Eiferman, R.A.; Kennedy, K.S.; Semba, C.P. Lifitegrast Ophthalmic Solution 5.0% for Treatment of Dry Eye Disease: Results of the OPUS-1 Phase 3 Study. Ophthalmology 2014, 121, 475–483. [Google Scholar] [CrossRef]
- Tauber, J.; Karpecki, P.; Latkany, R.; Luchs, J.; Martel, J.; Sall, K.; Raychaudhuri, A.; Smith, V.; Semba, C.P. Lifitegrast Ophthalmic Solution 5.0% versus Placebo for Treatment of Dry Eye Disease: Results of the Randomized Phase III OPUS-2 Study. Ophthalmology 2015, 122, 2423–2431. [Google Scholar] [CrossRef]
- Holland, E.J.; Luchs, J.; Karpecki, P.M.; Nichols, K.K.; Jackson, M.A.; Sall, K.; Tauber, J.; Roy, M.; Raychaudhuri, A.; Shojaei, A. Lifitegrast for the Treatment of Dry Eye Disease: Results of a Phase III, Randomized, Double-Masked, Placebo-Controlled Trial (OPUS-3). Ophthalmology 2017, 124, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Frampton, J.E. Varenicline Solution Nasal Spray: A Review in Dry Eye Disease. Drugs 2022, 82, 1481–1488. [Google Scholar] [CrossRef] [PubMed]
- Wirta, D.; Torkildsen, G.L.; Boehmer, B.; Hollander, D.A.; Bendert, E.; Zeng, L.; Ackermann, M.; Nau, J. ONSET-1 Phase 2b Randomized Trial to Evaluate the Safety and Efficacy of OC-01 (Varenicline Solution) Nasal Spray on Signs and Symptoms of Dry Eye Disease. Cornea 2022, 41, 1207–1216. [Google Scholar] [CrossRef] [PubMed]
- Quiroz-Mercado, H.; Hernandez-Quintela, E.; Chiu, K.H.; Henry, E.; Nau, J.A. A Phase II Randomized Trial to Evaluate the Long-Term (12-Week) Efficacy and Safety of OC-01 (Varenicline Solution) Nasal Spray for Dry Eye Disease: The MYSTIC Study. Ocul. Surf. 2022, 24, 15–21. [Google Scholar] [CrossRef]
- Wirta, D.; Vollmer, P.; Paauw, J.; Chiu, K.-H.H.; Henry, E.; Striffler, K.; Nau, J.; Rubin, J.; Reilly, C.; Bergstrom, L.; et al. Efficacy and Safety of OC-01 (Varenicline Solution) Nasal Spray on Signs and Symptoms of Dry Eye Disease The ONSET-2 Phase 3 Randomized Trial. Ophthalmology 2022, 129, 379–387. [Google Scholar] [CrossRef]
- Jang, D.J.; Lee, J.H.; Kim, D.H.; Kim, J.W.; Koo, T.S.; Cho, K.H. The Development of Super-Saturated Rebamipide Eye Drops for Enhanced Solubility, Stability, Patient Compliance, and Bioavailability. Pharmaceutics 2023, 15, 950. [Google Scholar] [CrossRef]
- Wu, D.; Chen, W.Q.; Li, R.; Wang, Y. Efficacy and Safety of Topical Diquafosol Ophthalmic Solution for Treatment of Dry Eye: A Systematic Review of Randomized Clinical Trials. Cornea 2015, 34, 644–650. [Google Scholar] [CrossRef]
- Lee, H.J.; Yang, S.; Cheon, E.J.; Shin, S.; Byun, Y.S.; Kim, H.S.; Chung, S.H. Diquafosol Ophthalmic Solution Enhances Mucin Expression via ERK Activation in Human Conjunctival Epithelial Cells with Hyperosmotic Stress. Mol. Vis. 2022, 28, 114. [Google Scholar]
- Tauber, J.; Davitt, W.F.; Bokosky, J.E.; Nichols, K.K.; Yerxa, B.R.; Schaberg, A.E.; LaVange, L.M.; Mills-Wilson, M.C.; Kellerman, D.J. Double-Masked, Placebo-Controlled Safety and Efficacy Trial of Diquafosol Tetrasodium (INS365) Ophthalmic Solution for the Treatment of Dry Eye. Cornea 2004, 23, 784–792. [Google Scholar] [CrossRef]
- Matsumoto, Y.; Ohashi, Y.; Watanabe, H.; Tsubota, K. Efficacy and Safety of Diquafosol Ophthalmic Solution in Patients with Dry Eye Syndrome: A Japanese Phase 2 Clinical Trial. Ophthalmology 2012, 119, 1954–1960. [Google Scholar] [CrossRef]
- Park, D.H.; Chung, J.K.; Seo, D.R.; Lee, S.J. Clinical Effects and Safety of 3% Diquafosol Ophthalmic Solution for Patients With Dry Eye After Cataract Surgery: A Randomized Controlled Trial. Am. J. Ophthalmol. 2016, 163, 122–131.e2. [Google Scholar] [CrossRef] [PubMed]
- Ogami, T.; Asano, H.; Hiraoka, T.; Yamada, Y.; Oshika, T. The Effect of Diquafosol Ophthalmic Solution on Clinical Parameters and Visual Function in Soft Contact Lens-Related Dry Eye. Adv. Ther. 2021, 38, 5534–5547. [Google Scholar] [CrossRef] [PubMed]
- Cui, L.; Li, Y.; Lee, H.S.; Yang, J.M.; Choi, W.; Yoon, K.C. Effect of Diquafosol Tetrasodium 3% on the Conjunctival Surface and Clinical Findings after Cataract Surgery in Patients with Dry Eye. Int. Ophthalmol. 2018, 38, 2021–2030. [Google Scholar] [CrossRef] [PubMed]
- Arita, R.; Suehiro, J.; Haraguchi, T.; Maeda, S.; Maeda, K.; Tokoro, H.; Amano, S. Topical Diquafosol for Patients with Obstructive Meibomian Gland Dysfunction. Br. J. Ophthalmol. 2013, 97, 725–729. [Google Scholar] [CrossRef] [PubMed]
- Amano, S.; Inoue, K. Effect of Topical 3% Diquafosol Sodium on Eyes with Dry Eye Disease and Meibomian Gland Dysfunction. Clin. Ophthalmol. 2017, 11, 1677–1682. [Google Scholar] [CrossRef] [PubMed]
- Ohguchi, T.; Kojima, T.; Ibrahim, O.M.; Nagata, T.; Shimizu, T.; Shirasawa, T.; Kawakita, T.; Satake, Y.; Tsubota, K.; Shimazaki, J.; et al. The Effects of 2% Rebamipide Ophthalmic Solution on the Tear Functions and Ocular Surface of the Superoxide Dismutase-1 (Sod1) Knockout Mice. Investig. Ophthalmol. Vis. Sci. 2013, 54, 7793–7802. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Zhang, H.; Qin, G.; Wu, Y.; Song, Y.; Yang, L.; Yu, S.; He, X.; Moore, J.E.; Moutari, S.; et al. Impact of Diquafosol Ophthalmic Solution on Tear Film and Dry Eye Symptom in Type 2 Diabetic Dry Eye: A Pilot Study. J. Ocul. Pharmacol. Ther. 2022, 38, 133–140. [Google Scholar] [CrossRef]
- Hayashi, Y.; Toshida, H.; Matsuzaki, Y.; Matsui, A.; Ohta, T. Persistent Corneal Epithelial Defect Responding to Rebamipide Ophthalmic Solution in a Patient with Diabetes. Int. Med. Case Rep. J. 2016, 9, 113–116. [Google Scholar] [CrossRef]
- Barrientos, R.T.; Godín, F.; Rocha-De-Lossada, C.; Soifer, M.; Sánchez-González, J.M.; Moreno-Toral, E.; González, A.L.; Zein, M.; Larco, P.; Mercado, C.; et al. Ophthalmological Approach for the Diagnosis of Dry Eye Disease in Patients with Sjögren’s Syndrome. Life 2022, 12, 1899. [Google Scholar] [CrossRef]
- Ballesteros-Sánchez, A.; Gargallo-Martínez, B.; Gutiérrez-Ortega, R.; Sánchez-González, J.-M. Intra-Observer Repeatability Assessment of the S390L Firefly WDR Slit Lamp in Patients with Dry Eye Disease: Objective, Automated and Non-Invasive Measures. Eye Contact Lens 2023, 49, 283–291. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ballesteros-Sánchez, A.; Sánchez-González, M.C.; De-Hita-Cantalejo, C.; Gutiérrez-Sánchez, E.; Rocha-de-Lossada, C.; Sánchez-González, J.-M. The Efficacy and Safety of Rebamipide Ophthalmic Suspension (OPC-12759) in Patients with Dry Eye Disease: A Systematic Review of Randomized Controlled Trials. J. Clin. Med. 2023, 12, 7155. https://doi.org/10.3390/jcm12227155
Ballesteros-Sánchez A, Sánchez-González MC, De-Hita-Cantalejo C, Gutiérrez-Sánchez E, Rocha-de-Lossada C, Sánchez-González J-M. The Efficacy and Safety of Rebamipide Ophthalmic Suspension (OPC-12759) in Patients with Dry Eye Disease: A Systematic Review of Randomized Controlled Trials. Journal of Clinical Medicine. 2023; 12(22):7155. https://doi.org/10.3390/jcm12227155
Chicago/Turabian StyleBallesteros-Sánchez, Antonio, María Carmen Sánchez-González, Concepción De-Hita-Cantalejo, Estanislao Gutiérrez-Sánchez, Carlos Rocha-de-Lossada, and José-María Sánchez-González. 2023. "The Efficacy and Safety of Rebamipide Ophthalmic Suspension (OPC-12759) in Patients with Dry Eye Disease: A Systematic Review of Randomized Controlled Trials" Journal of Clinical Medicine 12, no. 22: 7155. https://doi.org/10.3390/jcm12227155
APA StyleBallesteros-Sánchez, A., Sánchez-González, M. C., De-Hita-Cantalejo, C., Gutiérrez-Sánchez, E., Rocha-de-Lossada, C., & Sánchez-González, J. -M. (2023). The Efficacy and Safety of Rebamipide Ophthalmic Suspension (OPC-12759) in Patients with Dry Eye Disease: A Systematic Review of Randomized Controlled Trials. Journal of Clinical Medicine, 12(22), 7155. https://doi.org/10.3390/jcm12227155