
Effects of Olympic Combat Sports on Cardiorespiratory Fitness in Non-Athlete Population: A Systematic Review of Randomized Controlled Trials

 ,
,  ,
,  , , ,
, , , 
Abstract
:1. Introduction
2. Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Information and Database Search Process
2.4. Studies Selection and Data Collection Process
2.5. Methodological Quality Assessment
2.6. Data Synthesis
2.7. Risk of Bias in Individual Studies
2.8. Summary Measures for Meta-Analysis
2.9. Certainty of Evidence
3. Results
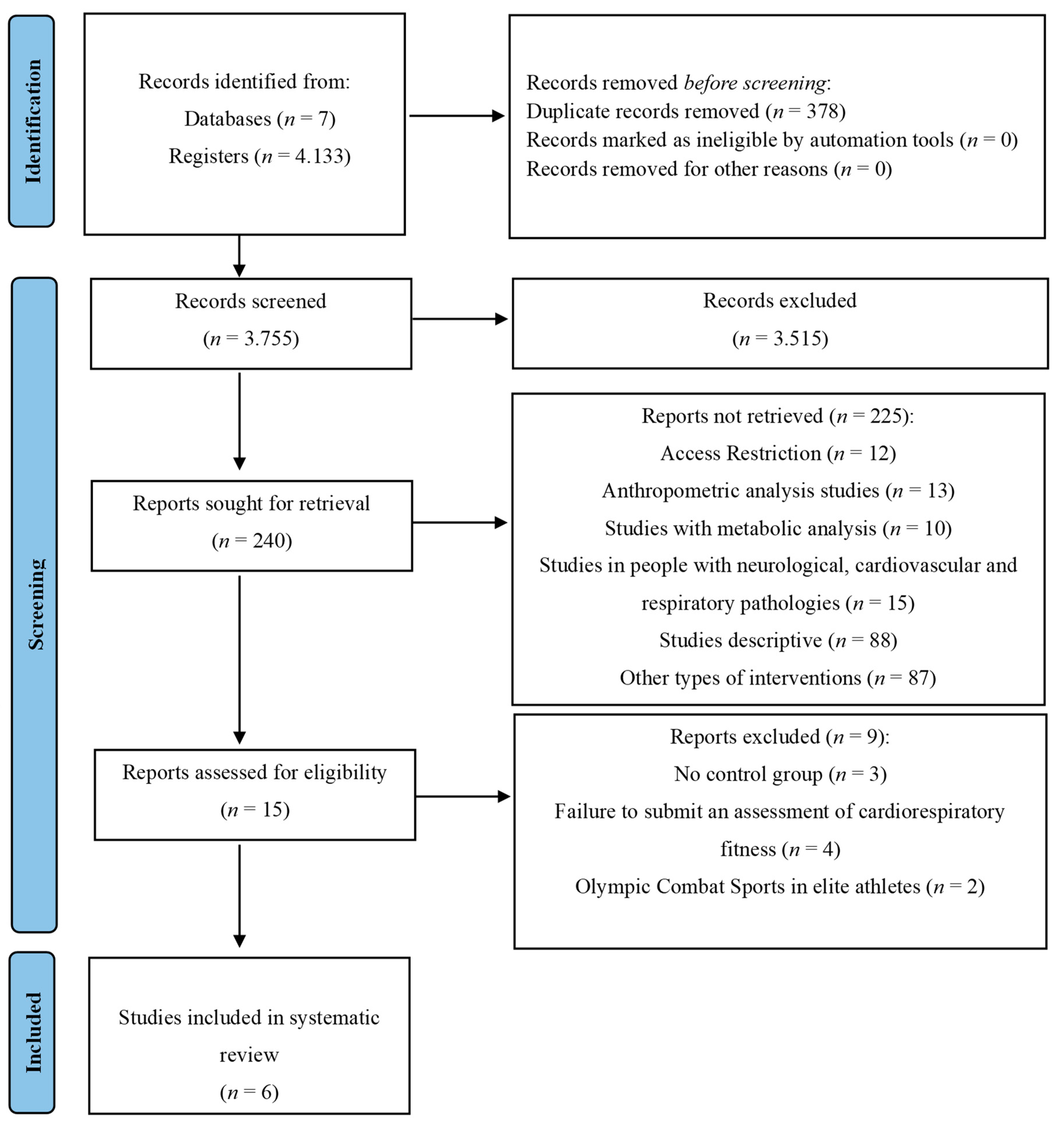
3.1. Study Selection
3.2. Methodological Quality
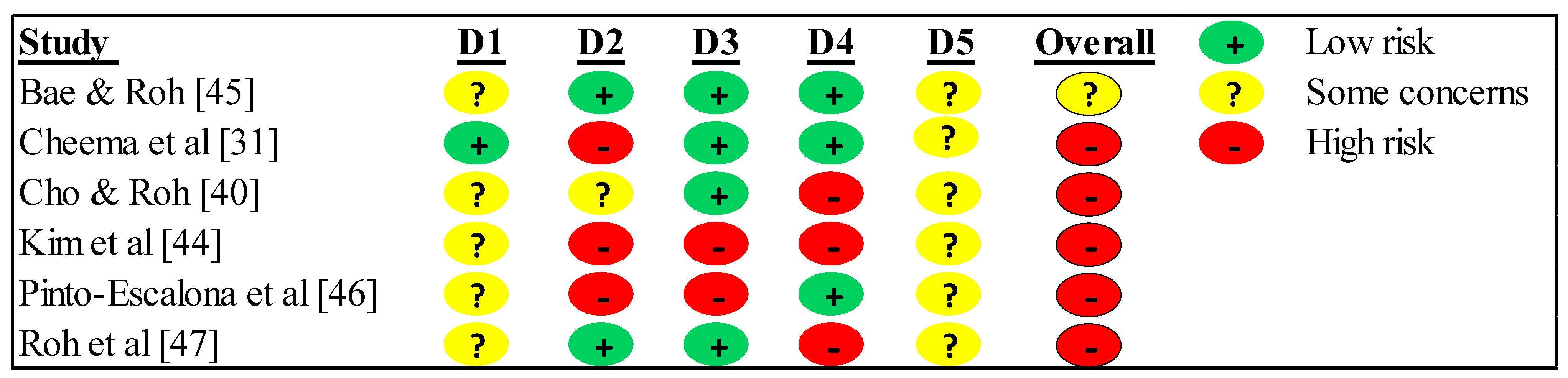
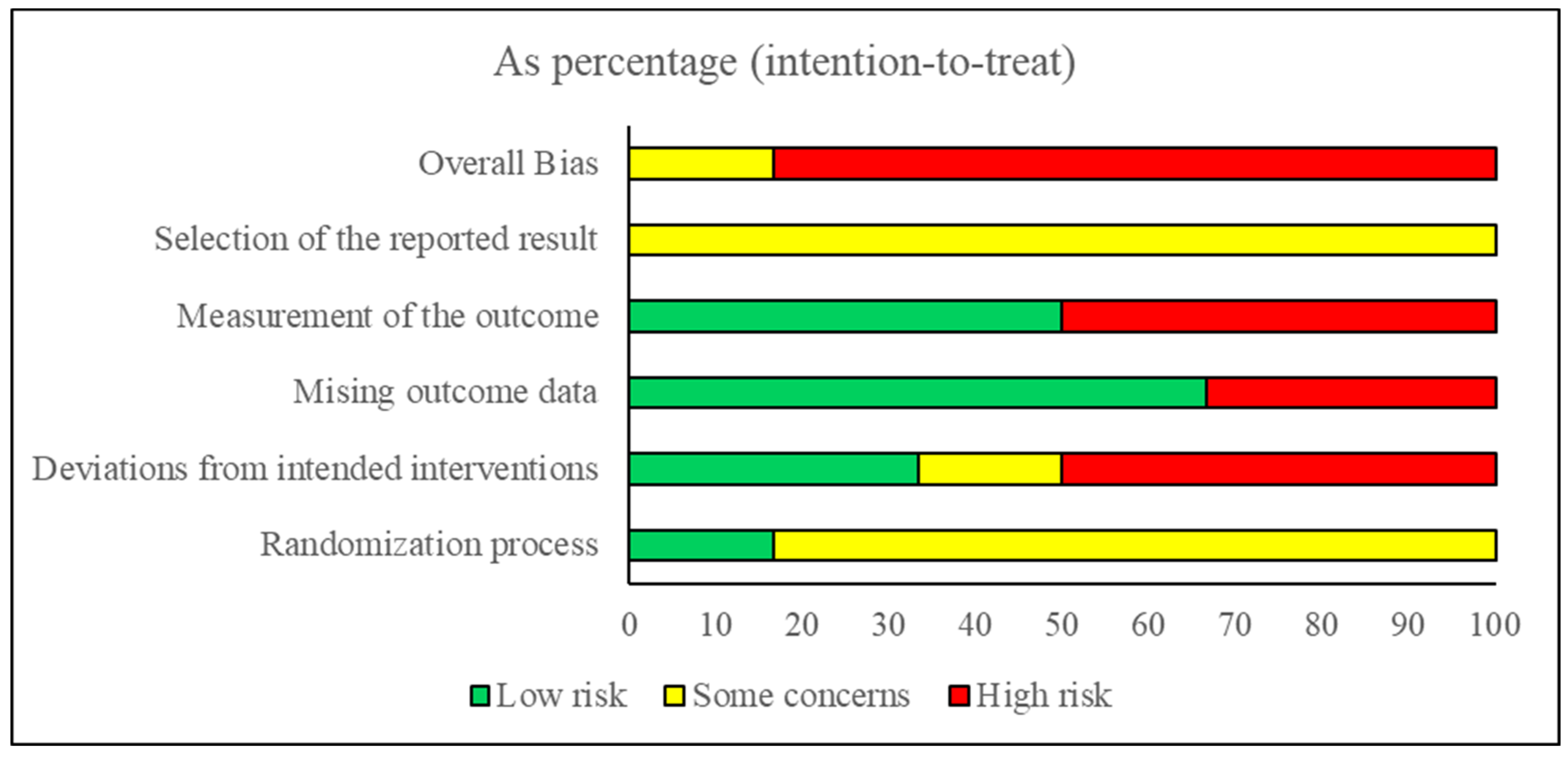
3.3. Risk of Bias within Studies
3.4. Studies Characteristics
3.5. Sample Characteristics
3.6. Dosing and Conducted Interventions
3.7. Data Collection Instruments of Cardiorespiratory Fitness (CRF)
3.7.1. Direct Method
3.7.2. Indirect Method
3.8. Outcome of Cardiorespiratory Fitness (CRF)
3.8.1. Direct Method
3.8.2. Indirect Method
3.9. Certainty of Evidence
3.10. Adverse Events and Adherence
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Raghuveer, G.; Hartz, J.; Lubans, D.R.; Takken, T.; Wiltz, J.L.; Mietus-Snyder, M.; Perak, A.M.; Baker-Smith, C.; Pietris, N.; Edwards, N.M. Cardiorespiratory Fitness in Youth: An Important Marker of Health: A Scientific Statement from the American Heart Association. Circulation 2020, 142, e101–e118. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour. Available online: https://apps.who.int/iris/bitstream/handle/10665/337001/9789240014886-eng.pdf (accessed on 8 June 2023).
- Xiang, L.; Deng, K.; Mei, Q.; Gao, Z.; Yang, T.; Wang, A.; Fernandez, J.; Gu, Y. Population and Age-Based Cardiorespiratory Fitness Level Investigation and Automatic Prediction. Front. Cardiovasc. Med. 2021, 8, 758589. [Google Scholar] [CrossRef]
- Franklin, B.A.; Eijsvogels, T.M.H.; Pandey, A.; Quindry, J.; Toth, P.P. Physical activity, cardiorespiratory fitness, and cardiovascular health: A clinical practice statement of the ASPC Part I: Bioenergetics, contemporary physical activity recommendations, benefits, risks, extreme exercise regimens, potential maladaptations. Am. J. Prev. Cardiol. 2022, 12, 100424. [Google Scholar] [CrossRef] [PubMed]
- Letnes, J.M.; Nes, B.M.; Wisløff, U. Age-related decline in peak oxygen uptake: Cross-sectional vs. longitudinal findings. A review. Int. J. Cardiol. Cardiovasc. Risk Prev. 2023, 16, 200171. [Google Scholar] [CrossRef]
- Tahira, S. The Association between Sports Participation and Physical Fitness. Int. J. Sport Stud. Health 2022, 4, e127001. [Google Scholar] [CrossRef]
- Malm, C.; Jakobsson, J.; Isaksson, A. Physical Activity and Sports-Real Health Benefits: A Review with Insight into the Public Health of Sweden. Sports 2019, 7, 127. [Google Scholar] [CrossRef]
- Anderson, E.; Durstine, J.L. Physical activity, exercise, and chronic diseases: A brief review. Sports Med. Health Sci. 2019, 1, 3–10. [Google Scholar] [CrossRef]
- Arija, V.; Villalobos, F.; Pedret, R.; Vinuesa, A.; Timón, M.; Basora, T.; Aguas, D.; Basora, J.; Domínguez, E.; Jovani, D.; et al. Effectiveness of a physical activity program on cardiovascular disease risk in adult primary health-care users: The “Pas-a-Pas” community intervention trial. BMC Public Health 2017, 17, 576. [Google Scholar] [CrossRef]
- Aune, D.; Norat, T.; Leitzmann, M.; Tonstad, S.; Vatten, L.J. Physical activity and the risk of type 2 diabetes: A systematic review and dose-response meta-analysis. Eur. J. Epidemiol. 2015, 30, 529–542. [Google Scholar] [CrossRef]
- McTiernan, A.; Friedenreich, C.M.; Katzmarzyk, P.T.; Powell, K.E.; Macko, R.; Buchner, D.; Pescatello, L.S.; Bloodgood, B.; Tennant, B.; Vaux-Bjerke, A.; et al. Physical Activity in Cancer Prevention and Survival: A Systematic Review. Med. Sci. Sports Exerc. 2019, 51, 1252–1261. [Google Scholar] [CrossRef] [PubMed]
- Pescatello, L.S.; Buchner, D.M.; Jakicic, J.M.; Powell, K.E.; Kraus, W.E.; Bloodgood, B.; Campbell, W.W.; Dietz, S.; Dipietro, L.; George, S.M.; et al. Physical Activity to Prevent and Treat Hypertension: A Systematic Review. Med. Sci. Sports Exerc. 2019, 51, 1314–1323. [Google Scholar] [CrossRef] [PubMed]
- Yuksel, H.S.; Şahin, F.N.; Maksimovic, N.; Drid, P.; Bianco, A. School-Based Intervention Programs for Preventing Obesity and Promoting Physical Activity and Fitness: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 347. [Google Scholar] [CrossRef] [PubMed]
- Pearce, M.; Garcia, L.; Abbas, A.; Strain, T.; Schuch, F.B.; Golubic, R.; Kelly, P.; Khan, S.; Utukuri, M.; Laird, Y.; et al. Association Between Physical Activity and Risk of Depression: A Systematic Review and Meta-analysis. JAMA Psychiatry 2022, 79, 550–559. [Google Scholar] [CrossRef]
- Pinheiro, M.B.; Oliveira, J.; Bauman, A.; Fairhall, N.; Kwok, W.; Sherrington, C. Evidence on physical activity and osteoporosis prevention for people aged 65+ years: A systematic review to inform the WHO guidelines on physical activity and sedentary behaviour. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 150. [Google Scholar] [CrossRef]
- Miko, H.C.; Zillmann, N.; Ring-Dimitriou, S.; Dorner, T.E.; Titze, S.; Bauer, R. Effects of Physical Activity on Health. Gesundheitswesen 2020, 82, S184–S195. [Google Scholar] [CrossRef]
- Stamenković, A.; Manić, M.; Roklicer, R.; Trivić, T.; Malović, P.; Drid, P. Effects of Participating in Martial Arts in Children: A Systematic Review. Children 2022, 9, 1203. [Google Scholar] [CrossRef]
- Lambert, C.; Ritzmann, R.; Lambert, S.; Lachmann, D.; Malliaropoulos, N.G.; Gesslein, M.; Peters, N.; Shafizadeh, S. Prevalence of sport injuries in Olympic combat sports: A cross-sectional study examining one Olympic period. J. Sports Med. Phys. Fit. 2022, 62, 1496–1504. [Google Scholar] [CrossRef] [PubMed]
- Ng-Knight, T.; Gilligan-Lee, K.A.; Massonnié, J.; Gaspard, H.; Gooch, D.; Querstret, D.; Johnstone, N. Does Taekwondo improve children’s self-regulation? If so, how? A randomized field experiment. Dev. Psychol. 2022, 58, 522–534. [Google Scholar] [CrossRef]
- Kadri, A.; Slimani, M.; Bragazzi, N.L.; Tod, D.; Azaiez, F. Effect of Taekwondo Practice on Cognitive Function in Adolescents with Attention Deficit Hyperactivity Disorder. Int. J. Environ. Res. Public Health 2019, 16, 204. [Google Scholar] [CrossRef]
- Li, D.E.; Chiang, J.L.; Loh, Z.H.M.; Zainuldin, R. Taekwondo Poomsae practise in slow motion and the balance of healthy older adults: A Pre-Experimental Study. Physiother. Res. Int. J. Res. Clin. Phys. Ther. 2023, 28, e2027. [Google Scholar] [CrossRef] [PubMed]
- Valdés-Badilla, P.; Herrera-Valenzuela, T.; Ramirez-Campillo, R.; Aedo-Muñoz, E.; Báez-San Martín, E.; Ojeda-Aravena, A.; Branco, B.H.M. Effects of Olympic Combat Sports on Older Adults’ Health Status: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 7381. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.Z.; Zhou, M.; Weng, J.H. Eight Trigrams Boxing Combined with Wenyang Huoxue Recipe Improves Cardiopulmonary Motor Function and the Quality of Life of Patients with Coronary Heart Disease. Int. J. Gen. Med. 2021, 14, 7557–7566. [Google Scholar] [CrossRef] [PubMed]
- Vasconcelos, B.B.; Protzen, G.V.; Galliano, L.M.; Kirk, C.; Del Vecchio, F.B. Effects of High-Intensity Interval Training in Combat Sports: A Systematic Review with Meta-Analysis. J. Strength Cond. Res. 2020, 34, 888–900. [Google Scholar] [CrossRef]
- Barley, O.R.; Chapman, D.W.; Guppy, S.N.; Abbiss, C.R. Considerations When Assessing Endurance in Combat Sport Athletes. Front. Physiol. 2019, 10, 205. [Google Scholar] [CrossRef]
- Schwartz, J.; Takito, M.; Fabrício, b.; Del Vecchio, F.; Antonietti, L.; Bullet, E.; Franchini, E. Health-related physical fitness in martial arts and combat sports practitioners. Sport Sci. Health 2015, 11, 171–180. [Google Scholar] [CrossRef]
- Valdés-Badilla, P.; Ramirez-Campillo, R.; Herrera-Valenzuela, T.; Branco, B.H.M.; Guzmán-Muñoz, E.; Mendez-Rebolledo, G.; Concha-Cisternas, Y.; Hernandez-Martínez, J. Effectiveness of Olympic Combat Sports on Balance, Fall Risk or Falls in Older Adults: A Systematic Review. Biology 2022, 11, 74. [Google Scholar] [CrossRef]
- Linhares, D.; Brandão Pinto de Castro, J.; Borba-Pinheiro, C.; Linhares, B.; Santos, L.; Marcos-Pardo, P.; Vale, R. Effect of combat sports on physical fitness and activities of daily living of older adults: A systematic review and meta-analysis of randomized controlled trials. J. Gerontol. Geriatr. 2023, 71, 115–126. [Google Scholar] [CrossRef]
- Combs, S.A.; Diehl, M.D.; Chrzastowski, C.; Didrick, N.; McCoin, B.; Mox, N.; Staples, W.H.; Wayman, J. Community-based group exercise for persons with Parkinson disease: A randomized controlled trial. NeuroRehabilitation 2013, 32, 117–124. [Google Scholar] [CrossRef]
- Brasil, I.; Monteiro, W.; Lima, T.; Seabra, A.; Farinatti, P. Effects of judo training upon body composition, autonomic function, and cardiorespiratory fitness in overweight or obese children aged 8- to 13 years. J. Sports Sci. 2020, 38, 2508–2516. [Google Scholar] [CrossRef] [PubMed]
- Cheema, B.S.; Davies, T.B.; Stewart, M.; Papalia, S.; Atlantis, E. The feasibility and effectiveness of high-intensity boxing training versus moderate-intensity brisk walking in adults with abdominal obesity: A pilot study. BMC Sports Sci. Med. Rehabil. 2015, 7, 3. [Google Scholar] [CrossRef] [PubMed]
- Roh, H.T.; Cho, S.Y.; So, W.Y. Effects of Regular Taekwondo Intervention on Oxidative Stress Biomarkers and Myokines in Overweight and Obese Adolescents. Int. J. Environ. Res. Public Health 2020, 17, 2505. [Google Scholar] [CrossRef]
- Page, M.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Smart, N.A.; Waldron, M.; Ismail, H.; Giallauria, F.; Vigorito, C.; Cornelissen, V.; Dieberg, G. Validation of a new tool for the assessment of study quality and reporting in exercise training studies: TESTEX. Int. J. Evid.-Based Healthc. 2015, 13, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Verhagen, A.P.; de Vet, H.C.; de Bie, R.A.; Kessels, A.G.; Boers, M.; Bouter, L.M.; Knipschild, P.G. The Delphi list: A criteria list for quality assessment of randomized clinical trials for conducting systematic reviews developed by Delphi consensus. J. Clin. Epidemiol. 1998, 51, 1235–1241. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0.; The Cochrane Collaboration: Chichester, UK, 2011. [Google Scholar]
- Davey, J.; Turner, R.M.; Clarke, M.J.; Higgins, J.P.T. Characteristics of meta-analyses and their component studies in the Cochrane Database of Systematic Reviews: A cross-sectional, descriptive analysis. BMC Med. Res. Methodol. 2011, 11, 160. [Google Scholar] [CrossRef]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H.; et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- Cho, S.Y.; Roh, H.T. Taekwondo Enhances Cognitive Function as a Result of Increased Neurotrophic Growth Factors in Elderly Women. Int. J. Environ. Res. Public Health 2019, 16, 962. [Google Scholar] [CrossRef]
- Kim, Y.H.; Jeong, M.K.; Park, H.; Park, S.K. Effects of Regular Taekwondo Intervention on Health-Related Physical Fitness, Cardiovascular Disease Risk Factors and Epicardial Adipose Tissue in Elderly Women with Hypertension. Int. J. Environ. Res. Public Health 2021, 18, 2935. [Google Scholar] [CrossRef]
- Lee, S.; Hong, G.; Park, S. The effect of taekwondo training on physical fitness and the allergic response factor of hypersensitive obese children. ARCH BUDO 2018, 14, 113–121. [Google Scholar]
- Mohammed, M.H.; Choi, H.J. Can eight weeks of judo and taekwondo physical education improve the health-related fitness of male university students? Phys. Educ. Stud. 2020, 24, 109–114. Available online: https://sportedu.org.ua/index.php/PES/article/view/1058 (accessed on 8 June 2023). [CrossRef]
- Kim, H.; Stebbins, C.L.; Chai, J.H.; Song, J.K. Taekwondo training and fitness in female adolescents. J. Sports Sci. 2011, 29, 133–138. [Google Scholar] [CrossRef]
- Bae, J.Y.; Roh, H.T. Regular Taekwondo Training Affects Mood State and Sociality but Not Cognitive Function among International Students in South Korea. Healthcare 2021, 9, 820. [Google Scholar] [CrossRef] [PubMed]
- Pinto-Escalona, T.; Gobbi, E.; Valenzuela, P.L.; Bennett, S.J.; Aschieri, P.; Martin-Loeches, M.; Paoli, A.; Martinez-de-Quel, O. Effects of a school-based karate intervention on academic achievement, psychosocial functioning, and physical fitness: A multi-country cluster randomized controlled trial. J. Sport Health Sci. 2021. [Google Scholar] [CrossRef]
- Roh, H.T.; Cho, S.Y.; So, W.Y. Taekwondo Training Improves Mood and Sociability in Children from Multicultural Families in South Korea: A Randomized Controlled Pilot Study. Int. J. Environ. Res. Public Health 2018, 15, 757. [Google Scholar] [CrossRef]
- Kaya, I. Investigating the Effects of Maximal Strength Training on Wrestlers’ Physical, Physiological and Selected Motor Skills. The Anthropologist 2015, 20, 592–598. [Google Scholar] [CrossRef]
- Kamandulis, S.; Bruzas, V.; Mockus, P.; Stasiulis, A.; Snieckus, A.; Venckunas, T. Sport-Specific Repeated Sprint Training Improves Punching Ability and Upper-Body Aerobic Power in Experienced Amateur Boxers. J. Strength Cond. Res. 2018, 32, 1214–1221. [Google Scholar] [CrossRef]
- Ojeda-Aravena, A.; Herrera-Valenzuela, T.; Valdés-Badilla, P.; Cancino-López, J.; Zapata-Bastias, J.; García-García, J.M. Effects of 4 Weeks of a Technique-Specific Protocol with High-Intensity Intervals on General and Specific Physical Fitness in Taekwondo Athletes: An Inter-Individual Analysis. Int. J. Environ. Res. Public Health 2021, 18, 3643. [Google Scholar] [CrossRef]
- Herrera-Valenzuela, T.; Carter, J.; Leiva, E.; Valdés-Badilla, P.; Ojeda-Aravena, A.; Franchini, E. Effect of a Short HIIT Program with Specific Techniques on Physical Condition and Activity during Simulated Combat in National-Level Boxers. Sustainability 2021, 13, 8746. [Google Scholar] [CrossRef]
- Hernández, C. Estimación del consumo máximo de oxígeno mediante pruebas de ejercicio maximales y submaximales. Mov. Científico 2012, 6, 19. [Google Scholar] [CrossRef]
- Haas, F.; Sweeney, G.; Pierre, A.; Plusch, T.; Whiteson, J. Validation of a 2 Minute Step Test for Assessing Functional Improvement. Open J. Ther. Rehabil. 2017, 5, 71–81. [Google Scholar] [CrossRef]
- Meys, R.; Janssen, S.; Franssen, F.; Vaes, A.; Stoffels, A.; Hees, H.V.; Borst, B.V.D.; Klijn, P.; Burtin, C.; Hul, A.V.T.; et al. Reliability, construct validity and determinants of 6-minute walk distance in patients with asthma. J. Eur. Respir. J. 2021, 58, PA313. [Google Scholar] [CrossRef]
- Nusdwinuringtyas, N.; Triangto, K.; Alwi, I.; Yunus, F. The Validity and Reliability of Six Minute Walk Test in a 15 Meter Track. Indones. J. Phys. Med. Rehabil. 2022, 10, 57–66. [Google Scholar] [CrossRef]
- Lanza, C.; Zagatto Edo, P.; Silva, J.C.; Selman, J.P.; Imperatori, T.B.; Zanatta, D.J.; de Carvalho, L.N.; Reimberg, M.M.; Dal Corso, S. Reference Equation for the Incremental Shuttle Walk Test in Children and Adolescents. J. Pediatr. 2015, 167, 1057–1061. [Google Scholar] [CrossRef] [PubMed]
- Tomlinson, O.W.; Markham, L.; Wollerton, R.L.; Knight, B.A.; Duckworth, A.; Gibbons, M.A.; Scotton, C.J.; Williams, C.A. Validity and repeatability of cardiopulmonary exercise testing in interstitial lung disease. BMC Pulm. Med. 2022, 22, 485. [Google Scholar] [CrossRef] [PubMed]
- Heine, M.; van den Akker, L.E.; Verschuren, O.; Visser-Meily, A.; Kwakkel, G. Reliability and responsiveness of cardiopulmonary exercise testing in fatigued persons with multiple sclerosis and low to mild disability. PLoS ONE 2015, 10, e0122260. [Google Scholar] [CrossRef]
- Kaviani, S.; Schoeller, D.A.; Ravussin, E.; Melanson, E.L.; Henes, S.T.; Dugas, L.R.; Dechert, R.E.; Mitri, G.; Schoffelen, P.F.M.; Gubbels, P.; et al. Determining the Accuracy and Reliability of Indirect Calorimeters Utilizing the Methanol Combustion Technique. Nutr. Clin. Pract. 2018, 33, 206–216. [Google Scholar] [CrossRef] [PubMed]
- Purcell, S.; Johnson-Stoklossa, C.; Tibaes, J.R.B.; Frankish, A.; Elliott, S.; Raj, P.; Prado, C. Accuracy and reliability of a portable indirect calorimeter compared to whole-body indirect calorimetry for measuring resting energy expenditure. Clin. Nutr. ESPEN 2020, 39, 67–73. [Google Scholar] [CrossRef]
- Hamlin, M.J.; Draper, N.; Blackwell, G.; Shearman, J.P.; Kimber, N.E. Determination of maximal oxygen uptake using the bruce or a novel athlete-led protocol in a mixed population. J. Hum. Kinet. 2012, 31, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Quintino, L.F.; Aguiar, L.T.; de Brito, S.A.F.; Pereira, A.S.; Teixeira-Salmela, L.F.; de Morais Faria, C.D.C. Reliability and validity of the incremental shuttle walking test in individuals after stroke. Top. Stroke Rehabil. 2021, 28, 331–339. [Google Scholar] [CrossRef]
- Eike, G.S.H.; Aadland, E.; Blom, E.E.; Riiser, A. Validation of a Modified Submaximal Balke Protocol to Assess Cardiorespiratory Fitness in Individuals at High Risk of or With Chronic Health Conditions—A Pilot Study. Front. Sports Act. Living 2021, 3, 642538. [Google Scholar] [CrossRef]
- Honore, P.M.; Redant, S.; Preseau, T.; Kaefer, K.; Barreto Gutierrez, L.; Anane, S.; Attou, R.; Gallerani, A.; De Bels, D. Indirect calorimetry is the gold standard to assess REE in ICU patients: Some limitations to consider. Crit. Care 2021, 25, 406. [Google Scholar] [CrossRef] [PubMed]
- Ross, R.M.; Murthy, J.N.; Wollak, I.D.; Jackson, A.S. The six minute walk test accurately estimates mean peak oxygen uptake. BMC Pulm. Med. 2010, 10, 31. [Google Scholar] [CrossRef] [PubMed]
- Franchini, E.; Cormack, S.; Takito, M.Y. Effects of High-Intensity Interval Training on Olympic Combat Sports Athletes’ Performance and Physiological Adaptation: A Systematic Review. J. Strength Cond. Res. 2019, 33, 242–252. [Google Scholar] [CrossRef] [PubMed]
- Nam, S.S.; Lim, K. Effects of Taekwondo training on physical fitness factors in Korean elementary students: A systematic review and meta-analysis. J. Exerc. Nutr. Biochem. 2019, 23, 36–47. [Google Scholar] [CrossRef]
- Degens, H.; Stasiulis, A.; Skurvydas, A.; Statkeviciene, B.; Venckunas, T. Physiological comparison between non-athletes, endurance, power and team athletes. Eur. J. Appl. Physiol. 2019, 119, 1377–1386. [Google Scholar] [CrossRef]
- Tabben, M.; Chaouachi, A.; Hadi, M.; Aloui, A.; Habacha, H.; Tourny, C.; Franchini, E. Physical and physiological characteristics of high-level combat sport athletes. J. Combat. Sports Martial Arts 2014, 5, 1–5. [Google Scholar] [CrossRef]
- Ojeda-Aravena, A.; Herrera-Valenzuela, T.; Valdés-Badilla, P.; Báez-San Martín, E.; Thapa, R.K.; Ramirez-Campillo, R. A Systematic Review with Meta-Analysis on the Effects of Plyometric-Jump Training on the Physical Fitness of Combat Sport Athletes. Sports 2023, 11, 33. [Google Scholar] [CrossRef]
- Peset Mancebo, M.F.; Ferrer Sapena, A.; Villamón Herrera, M.; González Moreno, L.M.; Toca Herrera, J.-L.; Aleixandre Benavent, R. Scientific literature analysis of Judo in Web of Science. Arch. Budo 2013, 9, 81–91. [Google Scholar] [CrossRef]
- Pérez Gutiérrez, M.; Valdés-Badilla, P.; Gutiérrez-García, C.; Herrera-Valenzuela, T. Taekwondo scientific production published on the web of science (1988-2016): Collaboration and topics. Movimento 2017, 23, 1325–1340. [Google Scholar] [CrossRef]
- Silva, A.; Quaresma, A. Motivation and martial arts and combat sports participation: A study protocol. Revista de Artes Marciales Asiáticas 2019, 14, 34. [Google Scholar] [CrossRef]
- Morales, J.; Fukuda, D.H.; Curto, C.; Iteya, M.; Kubota, H.; Pierantozzi, E.; La Monica, M. Progression of combat sport activities for youth athletes. Strength Cond. J. 2020, 42, 78–89. [Google Scholar] [CrossRef]
- Domaradzki, J.; Kochan-Jacheć, K.; Trojanowska, I.; Koźlenia, D. Kickboxers and crossfitters vertebral column curvatures in sagittal plane: Crossfit practice influence in kickboxers body posture. J. Bodyw. Mov. Ther. 2021, 25, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Kong, X.; Ma, J. Effects of combat sports on cerebellar function in adolescents: A resting-state fMRI study. Br. J. Radiol. 2022, 95, 20210826. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Population | Functionally independent individuals with only one cardiometabolic risk factor (i.e., diabetes mellitus, hypertension, dyslipidemia, overweight or obesity, among others) and/or established cardiovascular or pulmonary disease. | People with sequels of cardiovascular disease of neuromuscular type (i.e., the sequel of cerebrovascular accident). Elite athletes or sportsmen. |
| Intervention | Interventions with OCS (boxing, fencing, judo, karate, taekwondo, wrestling) for four weeks or more. | Physical activity interventions not involving OCS. |
| Comparator | Interventions with a control group with or without supervised physical activity. | Lack of baseline and/or follow-up data. Absence of control group. |
| Outcome | At least one assessment (pre- and post-intervention) of CRF by the direct method (VO2max on a treadmill, ergospirometry, among others) or indirect method (6-min walk test, 2-min walk test, Chester step test, shuttle walking test, among others). | Do not present a CRF assessment. |
| Study design | Experimental design studies (randomized controlled trial) with pre- and post-assessment. | Non-randomized controlled trial, cross-sectional, retrospective, and prospective studies. |
| Study | Eligibility Criteria Specified | Randomly Allocated Participants | Allocation Concealed | Groups Similar at Baseline | Assessors Blinded | Outcome Measures Assessed >85% of Participants * | Intention to Treat Analysis | Reporting of between Group Statistical Comparisons | Point Measures and Measures of Variability Reported ** | Activity Monitoring in Control Group | Relative Exercise Intensity Reviewed | Exercise Volume and Energy Expended | Overall TESTEX # |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cho and Roh [40] | Yes | Yes | Yes | Yes | Unclear | Yes (2) | Yes | Yes | Yes (1) | No | Yes | Yes | 11/15 |
| Cheema, et al. [31] | Yes | Yes | Yes | Yes | Yes | Yes (2) | Yes | Yes | Yes (2) | Yes | Yes | Yes | 14/15 |
| Kim, et al. [44] | Yes | Yes | No | Yes | No | Yes (1) | Yes | Yes | Yes (2) | No | Yes | Yes | 10/15 |
| Bae and Roh [45] | Yes | Yes | Unclear | Yes | Unclear | Yes (1) | Yes | Yes | Yes (2) | Yes | Yes | Yes | 11/15 |
| Roh, Cho, and So [47] | Yes | Yes | Unclear | Yes | No | Yes (1) | No | Yes | Yes (2) | No | Yes | Yes | 9/15 |
| Pinto-Escalona, et al. [46] | Yes | Yes | Yes | Unclear | Unclear | Yes (3) | Unclear | Yes | Yes (2) | Yes | Unclear | Yes | 11/15 |
| Study | Country | Study Design | Sample’s Initial Health | Groups | Mean Age (Year) | Type of Intervention and Control Group | Training Volume | Training Intensity | Direct Method Data Collection | Indirect Data Collection Method | Main Outcomes | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (n) | Weeks | Frequency (Weekly) | Time Per Session (min) | ||||||||||
| Cho and Roh [40] | South Korea | RCT | Older people apparently healthy | EG: 19 CG: 18 | EG: 68.89 ± 4.16 CG: 69.00 ± 4.41 | EG: Taekwondo CG: usual activities | 16 | 5 | 60 | 50–80% HRmax | NR | 2MWT | EG vs. CG ↑ 2MWT in favor of EG |
| Cheema et al. [31] | Australia | RCT | Adults apparently healthy | EG: 6 CG: 6 | EG: 43 ± 19 CG: 36 ± 15 | EG: Boxing CG: Walking | 12 | 4 | 50 | EG: 86–89% HRmax CG: 64–77% HRmax | Indirect calorimetry using a standard ramp protocol on a laboratory treadmill | NR | EG vs. CG ↑ VO2max in favor of EG |
| Kim et al. [44] | United States of America | RCT | High school females apparently healthy | EG: 21 CG: 10 | EG: 15.7 ± 0.4 CG: 15.9 ± 0.6 | EG: Taekwondo CG: usual activities | 12 | 2 | 50 | 61% HRmax | Ergometric tape test Bruce. | 20-m shuttle run test | EG vs. CG ↔ VO2max EG vs. CG ↑ 20-m shuttle run test in favor of EG |
| Bae and Roh [45] | South Korea | RCT | University students apparently healthy | EG: 12 CG: 12 | EG: 22.42 ± 4.40 CG: 23.25 ± 4.31 | EG: Taekwondo CG: Physical activity and recreational sports | 16 | 1 | 60 | 50–80% HRmax | CP test spirometry (Ebbeling protocol) | NR | EG vs. CG ↔ VO2max |
| Pinto-Escalona et al. [46] | Multicenter (Spain, Portugal, France, Poland and Germany) | RCT | Schoolchildren apparently healthy | EG: 388 CG: 333 | EG: 7.4 ± 0.5 CG: 7.4 ± 0.4 | EG: Karate CG: Physical education classes | 36 | 2 | 120 | NR | NR | 20-m shuttle run test | EG vs. CG ↑ 20-m shuttle run test in favor of EG |
| Roh, Cho, and So [47] | South Korea | RCT | Schoolchildren apparently healthy | EG: 15 CG: 15 | EG: 11.53 ± 0.64 CG: 11.40 ± 0.63 | EG: Taekwondo CG: Physical education classes | 16 | 1 | 60 | 50–80% HRmax | CP test with spirometry (protocol of Nemeth) | NR | EG vs. CG ↔ VO2max |
| Outcome | Study Design | Risk of Bias in Individual Studies | Risk of Publication Bias | Inconsistency | Indirectness | Imprecision | Certainty of Evidence | Recommendation |
|---|---|---|---|---|---|---|---|---|
| Direct method | 4 RCT and 97 participants | Moderate to high 1 | High 3 | Moderate 4 | Moderate 5 | Moderate to high 6 | Moderate to low 8 | The available evidence did not allow definitive recommendations on using OCS to improve CRF in the non-athlete population. |
| Indirect method | 2 RCT and 758 participants | High 2 | High 3 | Moderate 4 | Moderate 5 | High 7 | Low 9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muñoz-Vásquez, C.; Hernandez-Martinez, J.; Ramos-Espinoza, F.; Herrera-Valenzuela, T.; Magnani Branco, B.H.; Guzman-Muñoz, E.; Floriano Landim, S.; Mondaca-Urrutia, J.; Valdés-Badilla, P. Effects of Olympic Combat Sports on Cardiorespiratory Fitness in Non-Athlete Population: A Systematic Review of Randomized Controlled Trials. J. Clin. Med. 2023, 12, 7223. https://doi.org/10.3390/jcm12237223
Muñoz-Vásquez C, Hernandez-Martinez J, Ramos-Espinoza F, Herrera-Valenzuela T, Magnani Branco BH, Guzman-Muñoz E, Floriano Landim S, Mondaca-Urrutia J, Valdés-Badilla P. Effects of Olympic Combat Sports on Cardiorespiratory Fitness in Non-Athlete Population: A Systematic Review of Randomized Controlled Trials. Journal of Clinical Medicine. 2023; 12(23):7223. https://doi.org/10.3390/jcm12237223
Chicago/Turabian StyleMuñoz-Vásquez, Cristopher, Jordan Hernandez-Martinez, Francisco Ramos-Espinoza, Tomas Herrera-Valenzuela, Braulio Henrique Magnani Branco, Eduardo Guzman-Muñoz, Sibila Floriano Landim, Jessica Mondaca-Urrutia, and Pablo Valdés-Badilla. 2023. "Effects of Olympic Combat Sports on Cardiorespiratory Fitness in Non-Athlete Population: A Systematic Review of Randomized Controlled Trials" Journal of Clinical Medicine 12, no. 23: 7223. https://doi.org/10.3390/jcm12237223
APA StyleMuñoz-Vásquez, C., Hernandez-Martinez, J., Ramos-Espinoza, F., Herrera-Valenzuela, T., Magnani Branco, B. H., Guzman-Muñoz, E., Floriano Landim, S., Mondaca-Urrutia, J., & Valdés-Badilla, P. (2023). Effects of Olympic Combat Sports on Cardiorespiratory Fitness in Non-Athlete Population: A Systematic Review of Randomized Controlled Trials. Journal of Clinical Medicine, 12(23), 7223. https://doi.org/10.3390/jcm12237223