
Evaluation of Femoropopliteal In-Stent Restenosis Characteristics Stratified by Stent Design

 , ,
, ,
Abstract
:1. Introduction
2. Methods
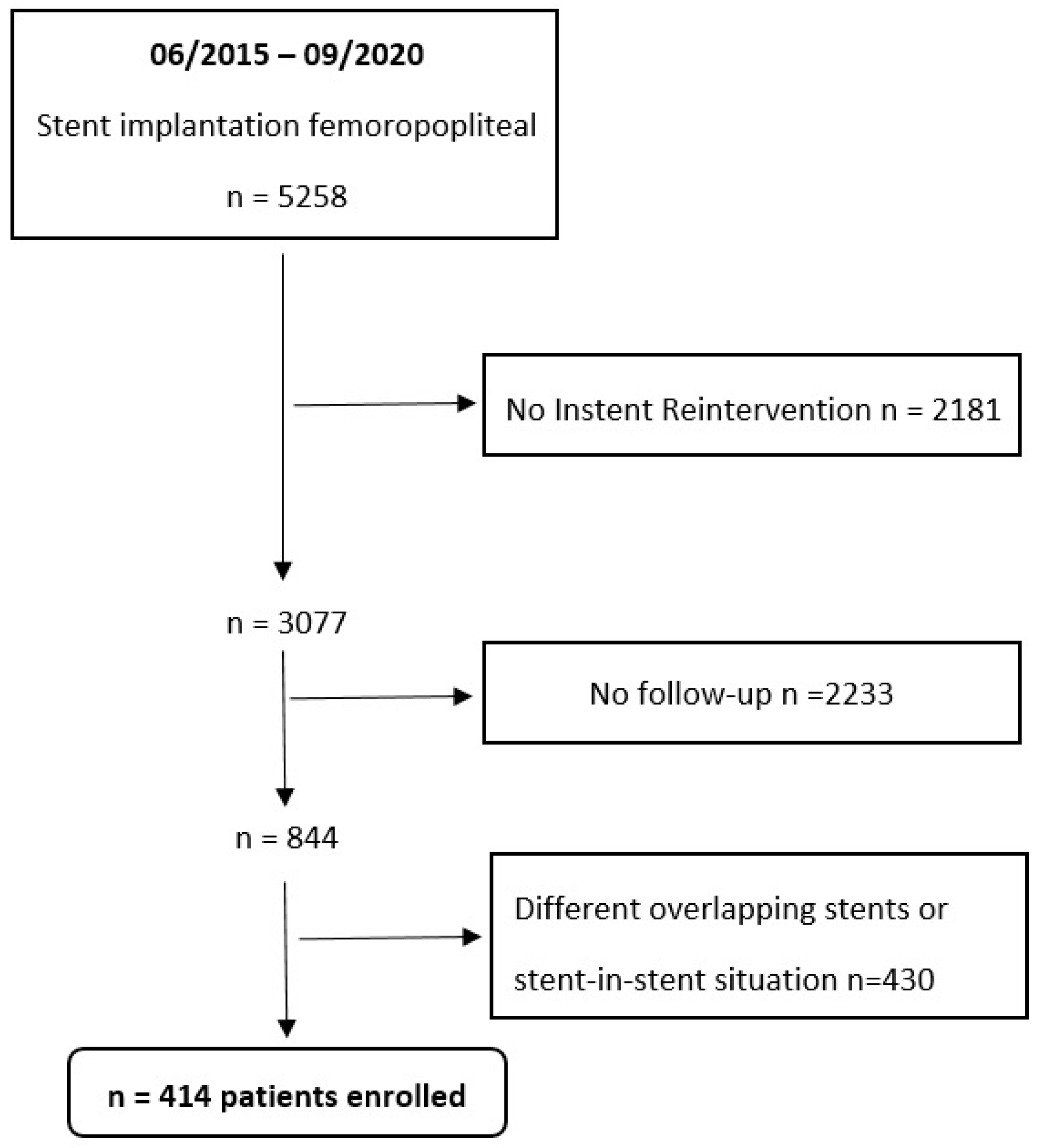
2.1. Patient Population
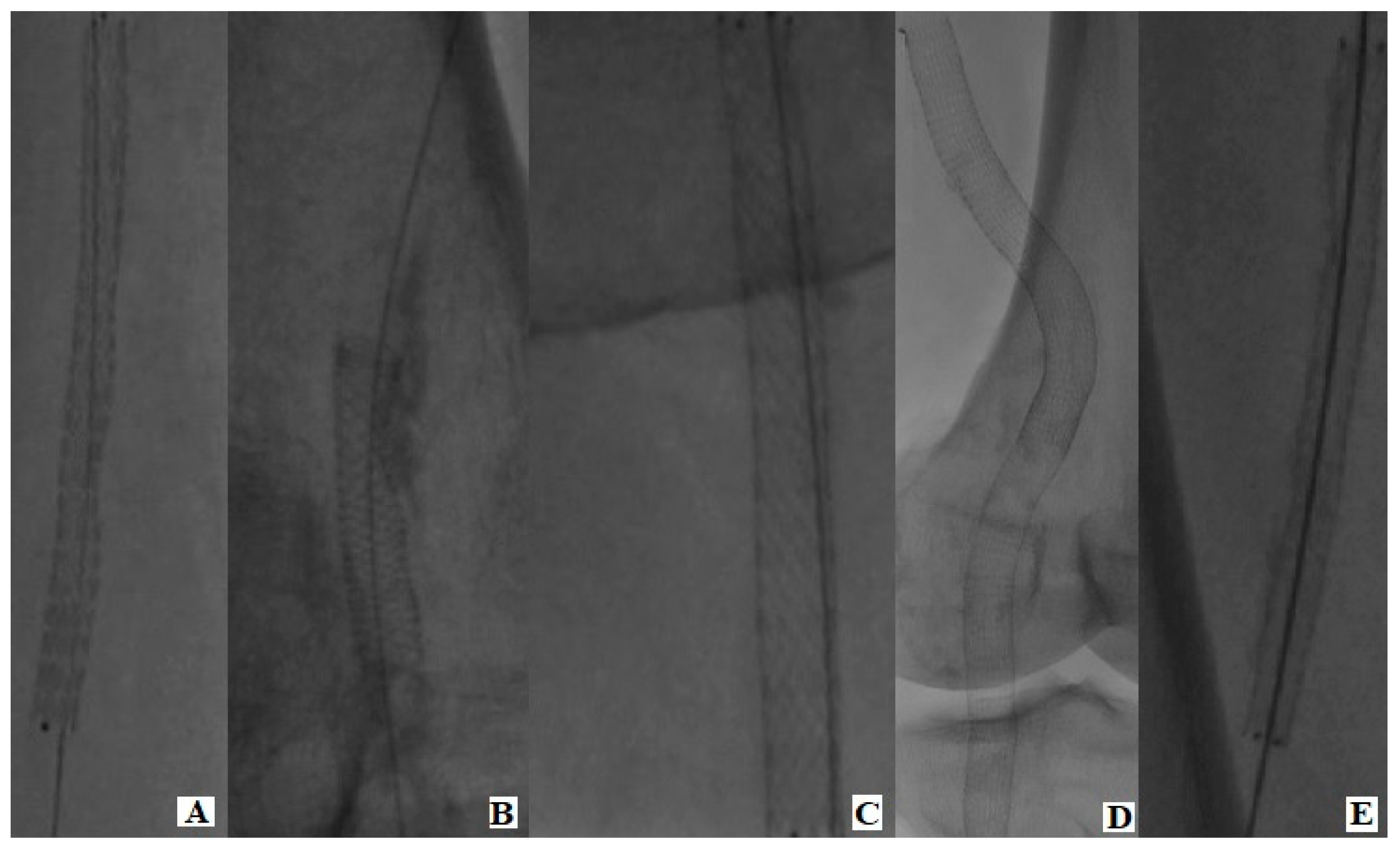
2.2. Included Stent Designs
2.3. Study Endpoints
2.4. Statistical Analysis
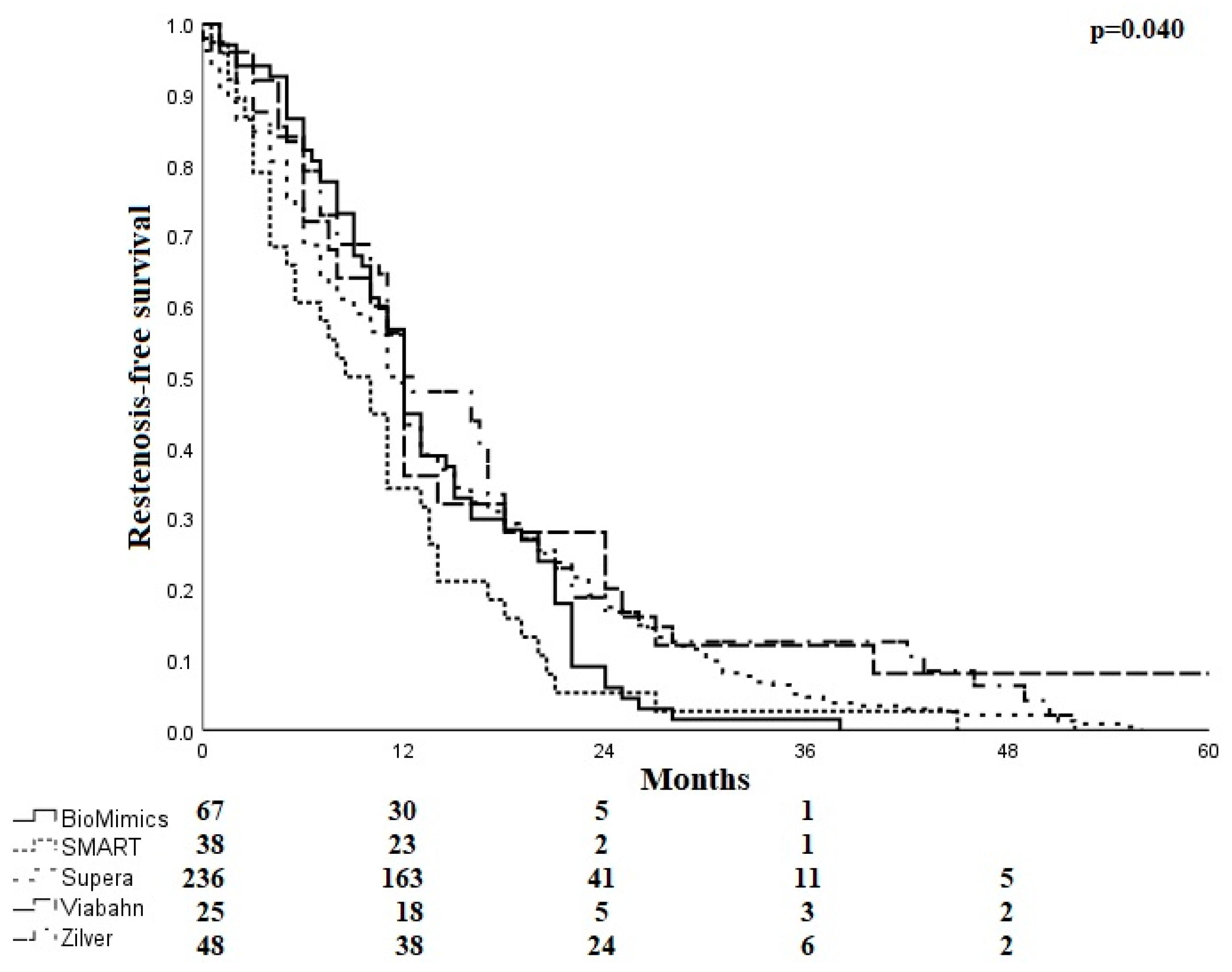
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bennett, M.R.; O’Sullivan, M. Mechanisms of angioplasty and stent restenosis: Implications for design of rational therapy. Pharmacol. Ther. 2001, 91, 149–166. [Google Scholar] [CrossRef] [PubMed]
- Minar, E.; Pokrajac, B.; Maca, T.; Ahmadi, R.; Fellner, C.; Mittlbock, M.; Seitz, W.; Wolfram, R.; Potter, R. Endovascular brachytherapy for prophylaxis of restenosis after femoropopliteal angio-plasty: Results of a prospective randomized study. Circulation 2000, 102, 2694–2699. [Google Scholar] [CrossRef] [PubMed]
- Stonebridge, P.A.; Hoskins, P.R.; Allan, P.L.; Belch, J.F. Spiral laminar flow in vivo. Clin. Sci. 1996, 91, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Berry, J.L.; Santamarina, A.; Moore, J.J.E.; Roychowdhury, S.; Routh, W.D. Experimental and computational flow evaluation of coronary stents. Ann. Biomed. Eng. 2000, 28, 386–398. [Google Scholar] [CrossRef]
- Chen, Z.; Fan, Y.; Deng, X.; Xu, Z. Swirling flow can suppress flow disturbances in endovascular stents: A numerical study. ASAIO J. 2009, 55, 543–549. [Google Scholar] [CrossRef]
- Piorkowski, M. Stentimplantation: Selbstexpandierbare bioaktive Stentsysteme. In Periphere Arterielle Interventionen; Springer: Berlin/Heidelberg, Germany, 2018; pp. 221–225. [Google Scholar]
- Stonebridge, P.A.; Brophy, C.M. Spiral laminar flow in arteries? Lancet 1991, 338, 1360–1361. [Google Scholar] [CrossRef]
- Tosaka, A.; Soga, Y.; Iida, O.; Ishihara, T.; Hirano, K.; Suzuki, K.; Yokoi, H.; Nanto, S.; Nobuyoshi, M. Classification and Clinical Impact of Restenosis After Femoropopliteal Stenting. J. Am. Coll. Cardiol. 2012, 59, 16–23. [Google Scholar] [CrossRef]
- Rutherford, R.B.; Becker, G.J. Standards for evaluating and reporting the results of surgical and percutaneous therapy for peripheral arterial disease. J. Vasc. Interv. Radiol. 1991, 2, 169–174. [Google Scholar] [CrossRef]
- Cheng, C.P.; Choi, G.; Herfkens, R.J.; Taylor, C.A. The effect of aging on deformations of the superficial femoral artery due to hip and knee flexion: Potential clinical implications. J. Vasc. Interv. Radiol. 2010, 21, 195–202. [Google Scholar] [CrossRef]
- Available online: https://www.veryanmed.com/international/products/biomimics-3d-vascular-stent-system/3d-helical-stent-design (accessed on 1 June 2016).
- Armstrong, E.J.; Bishu, K. Supera self-expanding stents for endovascular treatment of femoropopliteal disease: A review of the clinical evidence. Vasc. Health Risk Manag. 2015, 11, 387–395. [Google Scholar] [CrossRef]
- Caro, C.G.; Seneviratne, A.; Heraty, K.B.; Monaco, C.; Burke, M.G.; Krams, R.; Chang, C.C.; Coppola, G.; Gilson, P. Intimal hyperplasia following implantation of helical-centreline and straight-centreline stents in common carotid arteries in healthy pigs: Influence of intraluminal flow †. J. R. Soc. Interface 2013, 10, 20130578. [Google Scholar] [CrossRef]
- Shinke, T.; Robinson, K.; Burke, M.G.; Gilson, P.; Mullins, L.P.; O’Brien, N.; Heraty, K.B.; Taylor, C.; Cheshire, N.J.; Caro, C.G. Novel Helical Stent Design Elicits Swirling Blood, Flow Pattern and Inhibits Neo-intima Formation in Porcine Carotid Arteries. Circulation 2008, 118, S1054. [Google Scholar]
- Zeller, T.; Gaines, P.A.; Ansel, G.M.; Caro, C.G. Helical Centerline Stent Improves Patency: Two-Year Results From the Randomized Mimics Trial. Circ. Cardiovasc. Interv. 2016, 9, e002930. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, E.J.; Singh, S.; Singh, G.D.; Yeo, K.; Ludder, S.; Westin, G.; Anderson, D.; Dawson, D.L.; Pevec, W.C.; Laird, J.R. Angiographic characteristics of femoropopliteal in-stent restenosis: Association with long-term outcomes after endovascular intervention. Catheter. Cardiovasc. Interv. 2013, 82, 1168–1174. [Google Scholar] [CrossRef] [PubMed]
- Ihnat, D.M.; Duong, S.T.; Taylor, Z.C.; Leon, L.R.; Mills, J.L.; Goshima, K.R.; Echeverri, J.A.; Arslan, B. Contemporary outcomes after superficial femoral artery angioplasty and stenting: The influence of TASC classification and runoff score. J. Vasc. Surg. 2008, 47, 967–974. [Google Scholar] [CrossRef]
- Shibuya, T.; Shintani, T.; Edogawa, S.; Satoh, H. A review of surgically treated patients with obstruction after stenting in the femoropopliteal artery region. Ann. Vasc. Dis. 2013, 6, 573–577. [Google Scholar] [CrossRef]
- Iida, O.; Nanto, S.; Uematsu, M.; Ikeoka, K.; Okamoto, S.; Nagata, S. Influence of Stent Fracture on the Long-Term Patency in the Femoro-Popliteal Artery: Experience of 4 Years. JACC Cardiovasc. Interv. 2009, 2, 665–671. [Google Scholar] [CrossRef]
- Diaz, J.A.; Villegas, M.; Tamashiro, G.; Micelli, M.H.; Enterrios, D.; Balestrini, A.; Tamashiro, A. Flexions of the popliteal artery: Dynamic angiography. J. Invasive Cardiol. 2004, 16, 712–715. [Google Scholar]
- Rits, J.; van Herwaarden, J.; Jahrome, A.; Krievins, D.; Moll, F. The incidence of arterial stent fractures with exclusion of coronary, aortic, and non-arterial settings. Eur. J. Vasc. Endovasc. Surg. 2008, 36, 339–345. [Google Scholar] [CrossRef]
- Scheinert, D.; Scheinert, S.; Sax, J.; Piorkowski, C.; Bräunlich, S.; Ulrich, M.; Biamino, G.; Schmidt, A. Prevalence and clinical impact of stent fractures after femoropopliteal stenting. J. Am. Coll. Cardiol. 2005, 45, 312–315. [Google Scholar] [CrossRef]
- Lichtenberg, M.; Zeller, T.; Gaines, P.; Piorkowski, M. BioMimics 3D vascular stent system for femoropopliteal interventions. Vasa 2022, 51, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.-J.; Ko, Y.-G.; Shin, D.-H.; Kim, J.-S.; Kim, B.-K.; Choi, D.; Hong, M.-K.; Jang, Y. Outcomes of Spot Stenting Versus Long Stenting After Intentional Subintimal Approach for Long Chronic Total Occlusions of the Femoropopliteal Artery. JACC Cardiovasc. Interv. 2015, 8, 472–480. [Google Scholar] [CrossRef] [PubMed]
- London, N.; Srinivasan, R.; Naylor, A.; Hartshorne, T.; Ratliff, D.; Bell, P.; Bolia, A. Subintimal angioplasty of femoropopliteal artery occlusions: The long-term results. Eur. J. Vasc. Surg. 1994, 8, 148–155. [Google Scholar] [CrossRef] [PubMed]
- Davies, M.G.; Saad, W.E.; Peden, E.K.; Mohiuddin, I.T.; Naoum, J.J.; Lumsden, A.B. Percutaneous superficial femoral artery interventions for claudication--does runoff matter? Ann. Vasc. Surg. 2008, 22, 790–798. [Google Scholar] [CrossRef]
- Sullivan, T.M.; Zeller, T.; Nakamura, M.; Caro, C.G.; Lichtenberg, M. Swirling Flow and Wall Shear: Evaluating the BioMimics 3D Helical Centerline Stent for the Femoropopliteal Segment. Int. J. Vasc. Med. 2018, 2018, 9795174. [Google Scholar] [CrossRef]
- Sullivan, T.M.; Zeller, T.; Nakamura, M.; Gaines, P.A.; on behalf of the MIMICS-2 Trial Investigators. Treatment of Femoropopliteal Lesions With the BioMimics 3D Vascular Stent System: Two-Year Results From the MIMICS-2 Trial. J. Endovasc. Ther. 2021, 28, 236–245. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| BioMimics | SMART | Supera | Viabahn | Zilver | Total | ||
|---|---|---|---|---|---|---|---|
| n/% | n/% | n/% | n/% | n/% | n/% | p-Value | |
| Total cohort | 67 | 38 | 236 | 25 | 48 | 414 | |
| Male | 33 (49.3) | 18 (47.4) | 151 (64) | 20 (80) | 28 (58.3) | 250 (60.4) | 0.021 |
| Smoker | 27 (40.3) | 15 (39.5) | 64 (27.1) | 13 (52) | 21 (43.8) | 140 (33.8) | 0.015 |
| Former smoker | 13 (19.4) | 13 (34.2) | 79 (33.5) | 8 (32) | 11 (22.9) | 124 (30) | 0.167 |
| Hypertension | 58 (86.6) | 31 (81.6) | 202 (85.6) | 21 (84) | 44 (91.7) | 356 (86) | 0.730 |
| Diabetes mellitus | 27 (40.3) | 12 (31.6) | 86 (36.4) | 9 (36) | 22 (45.8) | 156 (37.7) | 0.673 |
| Hyperlipidemia | 58 (86.6) | 31 (81.6) | 208 (88.1) | 24 (96) | 47 (97.9) | 368 (88.9) | 0.099 |
| Renal insufficency | 18 (26.9) | 8 (21.1) | 64 (27.1) | 5 (20) | 12 (25) | 107 (25.8) | 0.885 |
| Dialysis | 3 (4.5) | 1 (2.6) | 7 (3) | 5 (20) | 1 (2.1) | 12 (2.9) | 0.883 |
| Coronary heart disease | 21 (31.3) | 13 (34.2) | 101 (42.8) | 10 (40) | 24 (50) | 169 (40.8) | 0.265 |
| Cerebral vascular disease | 8 (11.9) | 3 (7.9) | 44 (18.6) | 3 (12) | 8 (16.7) | 66 (15.9) | 0.375 |
| Stroke | 8 (11.9) | 4 (10.5) | 19 (8.1) | 1 (4) | 8 (16.7) | 40 (9.7) | 0.308 |
| BioMimics | SMART | Supera | Viabahn | Zilver | Total | ||
|---|---|---|---|---|---|---|---|
| n/% | n/% | n/% | n/% | n/% | n/% | p-Value | |
| Side | |||||||
| Left | 32 (47.8) | 15 (39.5) | 112 (47.5) | 16 (64) | 19 (39.6) | 194 (46.9) | 0.302 |
| Right | 35 (52.2) | 23 (60.5) | 124 (52.5) | 9 (36) | 29 (60.4) | 220 (53.1) | 0.302 |
| Number of stents | |||||||
| 1 | 54 (80.6) | 175 (74.2) | 10 (40) | 38 (79.2) | 310 (74.9) | <0.001 | |
| 2 | 11 (16.4) | 33 (86.8) | 51 (21.6) | 14 (56) | 8 (16.7) | 89 (21.5) | <0.001 |
| 3 | 2 (3) | 5 (13.2) | 9 (3.8) | 1 (4) | 2 (4.2) | 14 (3.4) | 0.806 |
| 4 | 1 (0.4) | 1 (0.2) | |||||
| Stent localization | |||||||
| 1 | 5 (7.5) | 15 (39.5) | 8 (3.4) | 12 (25) | 40 (9.7) | <0.001 | |
| 1,2 | 7 (10.4) | 3 (7.9) | 6 (2.5) | 1 (4) | 4 (8.3) | 21 (5.1) | 0.063 |
| 1,2,3 | 4 (6) | 1 (2.6) | 13 (5.5) | 9 (36) | 8 (16.7) | 35 (8.5) | <0.001 |
| 1,2,3,4 | 2 (3) | 1 (2.6) | 10 (4.2) | 12 (48) | 1 (2.1) | 26 (6.3) | <0.001 |
| 1,2,4 | 1 (0.4) | 1 (0.2) | 0.944 | ||||
| 1,3 | 1 (0.4) | 1 (2.1) | 2 (0.5) | 0.524 | |||
| 1,3,4 | 1 (0.4) | 1 (0.2) | 0.944 | ||||
| 1,4 | 1 (0.4) | 1 (0.2) | 0.944 | ||||
| 2 | 2 (3) | 3 (7.9) | 16 (6.8) | 5 (10.4) | 26 (6.3) | 0.334 | |
| 2,3 | 5 (7.5) | 1 (2.6) | 17 (7.2) | 3 (6.3) | 26 (6.3) | 0.552 | |
| 2,3,4 | 2 (3) | 14 (5.9) | 3 (12) | 19 (4.6) | 0.071 | ||
| 2,4 | 1 (0.4) | 1 (0.2) | 0.944 | ||||
| 3 | 9 (13.4) | 7 (18.4) | 20 (8.5) | 8 (16.7) | 44 (10.6) | 0.062 | |
| 3,4 | 16 (23.9) | 42 (17.8) | 4 (8.3) | 62 (15) | 0.001 | ||
| 4 | 15 (22.4) | 7 (18.4) | 85 (36) | 2 (4.2) | 109 (26.3) | <0.001 | |
| Mean stent diameter (mm) | 6.2 ± 0.55 | 6.7 ± 1.1 | 5.4 ± 0.51 | 6.0 ± 0.49 | 6.3 ± 0.45 | 5.7 ± 0.77 | <0.001 * |
| Mean stent length (mm) | 117.8 ± 65.7 | 57.4 ± 54.3 | 115.1 ± 83.8 | 311 ± 79.7 | 108.9 ± 97.3 | 121.4 ± 94.8 | <0.001 * |
| Target lesion | |||||||
| Stenosis | 17 (25.4) | 17 (44.7) | 80 (33.9) | 2 (8) | 21 (43.8) | 137 (33.1) | 0.008 |
| Occlusion | 50 (74.6) | 21 (55.3) | 156 (66.1) | 23 (92) | 27 (56.3) | 277 (66.9) | 0.008 |
| n patent BTK vessels | |||||||
| 0 | 2 (5.3) | 6 (2.5) | 1 (2.1) | 9 (2.2) | 0.419 | ||
| 1 | 20 (29.9) | 10 (26.3) | 76 (32.2) | 6 (24) | 18 (37.5) | 130 (31.4) | 0.724 |
| 2 | 29 (43.3) | 15 (39.5) | 101 (42.8) | 7 (28) | 16 (33.3) | 168 (40.6) | 0.495 |
| 3 | 18 (26.9) | 11 (28.9) | 53 (22.5) | 12 (48) | 13 (27.1) | 107 (25.8) | 0.089 |
| 95% CI | ||||||
|---|---|---|---|---|---|---|
| System | Stent Third | n | % | SE (%) | LV | UV |
| BioMimics | 1 | 6 | 9 | 3.5 | 3.8 | 17.5 |
| 1,2 | 2 | 3 | 2.1 | 0.6 | 9.2 | |
| 1,2,3 | 51 | 76.1 | 5.2 | 65 | 85.1 | |
| 1,3 | 3 | 4.5 | 2.5 | 1.3 | 11.5 | |
| 2 | 1 | 1.5 | 1.5 | 0.2 | 6.8 | |
| 2,3 | 3 | 4.5 | 2.5 | 1.3 | 11.5 | |
| 3 | 1 | 1.5 | 1.5 | 0.2 | 6.8 | |
| SMART | 1 | 2 | 5.3 | 3.6 | 1.1 | 15.8 |
| 1,2 | 1 | 2.6 | 2.6 | 0.3 | 11.6 | |
| 1,2,3 | 30 | 78.9 | 6.6 | 64.2 | 89.5 | |
| 1,3 | 1 | 2.6 | 2.6 | 0.3 | 11.6 | |
| 2 | 1 | 2.6 | 2.6 | 0.3 | 11.6 | |
| 2,3 | 2 | 5.3 | 3.6 | 1.1 | 15.8 | |
| 3 | 1 | 2.6 | 2.6 | 0.3 | 11.6 | |
| Supera | 1 | 12 | 5.1 | 1.4 | 2.8 | 8.5 |
| 1,2 | 6 | 2.5 | 1.0 | 1.1 | 5.2 | |
| 1,2,3 | 198 | 83.9 | 2.4 | 78.8 | 88.2 | |
| 1,3 | 4 | 1.7 | 0.8 | 0.6 | 4.0 | |
| 2 | 4 | 1.7 | 0.8 | 0.6 | 4.0 | |
| 2,3 | 6 | 2.5 | 1.0 | 1.1 | 5.2 | |
| 3 | 6 | 2.5 | 1.0 | 1.1 | 5.2 | |
| Viabahn | 1 | 3 | 12 | 6.5 | 3.5 | 28.7 |
| 1,2 | 1 | 4 | 3.9 | 0.4 | 17.2 | |
| 1,2,3 | 20 | 80 | 8.0 | 61.6 | 91.9 | |
| 1,3 | 1 | 4 | 3.9 | 0.4 | 17.2 | |
| 2 | 0 | |||||
| 2,3 | 0 | |||||
| 3 | 0 | |||||
| Zilver | 1 | 3 | 6.3 | 3.5 | 1.8 | 15.7 |
| 1,2 | 2 | 4.2 | 2.9 | 0.9 | 12.7 | |
| 1,2,3 | 37 | 77.1 | 6.1 | 63.8 | 87.2 | |
| 1,3 | 2 | 4.2 | 2.9 | 0.9 | 12.7 | |
| 2 | 1 | 2.1 | 2.1 | 0.2 | 9.3 | |
| 2,3 | 3 | 6.3 | 3.5 | 1.8 | 15.7 | |
| 3 | 0 | |||||
| BioMimics | SMART | Supera | Viabahn | Zilver | Total | p-Value | |
|---|---|---|---|---|---|---|---|
| n/% | n/% | n/% | n/% | n/% | n/% | ||
| Stent localization | Occlusion | ||||||
| Femoral | 18 (56.3) | 21 (70) | 48 (59.3) | 8 (80) | 23 (56.1) | 118 (60.8) | <0.001 |
| Femoropopliteal | 13 (65) | 1 (100) | 54 (77.1) | 11 (73.3) | 3 (60) | 82 (73.9) | <0.001 |
| Popliteal | 12 (80) | 5 (71.4) | 61 (71.8) | 0 | 1 (50) | 79 (72.5) | <0.001 |
| Stent localization | Stenosis | ||||||
| Femoral | 14 (43.9) | 9 (30) | 33 (40.7) | 2 (20) | 18 (43.9) | 76 (39.2) | 0.004 |
| Femoropopliteal | 7 (35) | 16 (22.9) | 4 (26.7) | 2 (40) | 29 (26.1) | 0.012 | |
| Popliteal | 3 (20) | 2 (28.6) | 24 (28.2) | 1 (50) | 30 (27.5) | 0.020 | |
| Stent diameter (mm) | Occlusion | ||||||
| 4 | 0 | 0 | 4 (100) | 0 | 0 | 4(100) | 0.577 |
| 5–5.5 | 5 (100) | 0 | 119 (67.8) | 6 (100) | 0 | 130 (69.6) | <0.001 |
| 6–6.5 | 24 (53.3) | 14 (63.3) | 40 (70.7) | 10 (64.7) | 20 (57.1) | 108 (62.1) | <0.001 |
| 7 | 14 (82.4) | 8 (80) | 0 | 3 (100) | 7 (53.8) | 32 (74.4) | <0.001 |
| 8 | 0 | 2 (66.7) | 0 | 0 | 0 | 2 (66.7) | <0.001 |
| 9 | 0 | 1 (100) | 0 | 0 | 0 | 1 (100) | 0.053 |
| 10 | 0 | 2 (100) | 0 | 0 | 0 | 2 (100) | <0.001 |
| Stent diameter (mm) | Stenosis | ||||||
| 4 | |||||||
| ≥5–6 | 56 (32.2) | 56 (30.4) | <0.001 | ||||
| ≥6–7 | 21 (46.7) | 8 (36.4) | 17 (29.3) | 6 (35.3) | 15 (42.9) | 67 (37.9) | <0.001 |
| 7 | 3 (17.6) | 2 (20) | 6 (46.2) | 11 (25.6) | <0.001 | ||
| 8 | 1 (33.3) | 1 (33.3) | 0.023 | ||||
| Stent lenght (mm) | Occlusion | ||||||
| ≤100 | 19 (52.8) | 24 (68.6) | 93 (68.4) | 0 | 16 (51.6) | 152 (63.9) | <0.001 |
| >100 to ≤200 | 17 (73.9) | 2 (100) | 50 (71.4) | 0 | 5 (55.6) | 74 (70.5) | 0.001 |
| >200 to ≤300 | 6 (85.7) | 1 (100) | 17 (73.9) | 9 (69.2) | 4 (66.7) | 37 (74) | <0.001 |
| >300 to ≤400 | 1 (100) | 0 | 2 (40) | 8 (88.9) | 1 (100) | 12 (75) | <0.001 |
| >400 to ≤500 | 0 | 0 | 1 (50) | 2 (100) | 1 (100) | 4 (80) | 0.008 |
| Stent lenght (mm) | Stenosis | ||||||
| ≤100 | 17 (47.2) | 11 (31.4) | 43 (31.6) | 15 (48.4) | 86 (36.1) | <0.001 | |
| >100 to ≤200 | 6 (26.1) | 20 (28.6) | 1 (100) | 4 (44.4) | 31 (29.5 | 0.347 | |
| >200 to ≤300 | 1 (14.3) | 6 (26.1) | 4 (30.8) | 2 (33.3) | 13 (26) | <0.001 | |
| >300 to ≤400 | 3 (60) | 1 (11.1) | 4 (25) | 0.202 | |||
| >400 to ≤500 | 1 (50) | 1 (20) | 0.931 | ||||
| BTK n | Occlusion | ||||||
| 0 | 0 | 1 (50) | 2 (33.3) | 0 | 1 (100) | 4 (44.4) | 0.571 |
| 1 | 15 (75) | 8 (80) | 57 (75) | 6 (100) | 7 (38.9) | 93 (71.5) | 0.894 |
| 2 | 19 (65.5) | 9 (60) | 62 (61.4) | 6 (85.7) | 12 (75) | 108 (64.3) | 0.793 |
| 3 | 9 (50) | 9 (81.8) | 42 (79.2) | 7 (58.3) | 7 (53.8) | 74 (69.2) | 0.658 |
| BTK n | Stenosis | ||||||
| 0 | 0 | 1 (50) | 4 (66.7) | 0 | 0 | 5 (55.6) | 0.478 |
| 1 | 5 (25) | 2 (20) | 19 (25) | 0 | 11 (61.1) | 37 (28.5) | 0.042 |
| 2 | 10 (34.5) | 6 (40) | 39 (38.6) | 1 (14.3) | 4 (25) | 60 (35.7) | 0.036 |
| 3 | 9 (50) | 2 (18.2) | 11 (20.8) | 5 (41.7) | 6 (46.2) | 33 (30.8) | 0.002 |
| RBC Index Stent Implantation | BioMimics | SMART | Supera | Viabahn | Zilver | Total | p-Value |
|---|---|---|---|---|---|---|---|
| n/% | n/% | n/% | n/% | n/% | n/% | ||
| 0 | 1 (0.4) | 1 (0.2) | |||||
| 1 | 3 (1.3) | 1 (2.1) | 4 (1) | ||||
| 2 | 3 (4.5) | 31 (13.1) | 6 (24) | 6 (12.5) | 46 (11.1) | ||
| 3 | 43 (64.2) | 20 (52.6) | 129 (54.7) | 15 (60) | 29 (60.4) | 236 (57) | |
| 4 | 10 (14.9) | 14 (36.8) | 23 (9.7) | 3 (12) | 5 (10.4) | 55 (13.3) | |
| 5 | 10 814.9) | 4 (10.5) | 47 (19.9) | 1 (4) | 7 (14.7) | 69 (16.7) | |
| 6 | 1 (1.5) | 2 (0.8) | 3 (0.7) | ||||
| MV | 3.45 | 3.58 | 3.35 | 2.96 | 3.23 | 3.35 | 0.099 |
| RBC in-stent reintervention | |||||||
| 0 | 1 (0.4) | 1 (4) | 2 (0.5) | ||||
| 1 | 2 (3) | 7 (3) | 3 (12) | 1 (2.1) | 13 (3.1) | ||
| 2 | 2 (3) | 2 (5.3) | 25 (10.6) | 4 (16) | 4 (8.3) | 37 (8.9) | |
| 3 | 34 (50.7) | 16 (42.1) | 101 (42.8) | 14 (56) | 22 (45.8) | 187 (45.2) | |
| 4 | 14 (20.9) | 15 (39.5) | 55 (23.3) | 2 (8) | 10 (20.8) | 96 (23.2) | |
| 5 | 15 (22.4) | 5 (13.2) | 42 (17.8) | 1 (4) | 11 (22.9) | 74 (17.9) | |
| 6 | 5 (2.1) | 5 (1.2) | |||||
| MV | 3.57 | 3.61 | 3.47 | 2.64 | 3.54 | 3.46 | 0.002 |
| Univariable Analysis | Multivariable Analysis | |||||
|---|---|---|---|---|---|---|
| OR 8 | 95% CI 9 | p-Value | Adj. 10 OR | 95% CI | Adj. p-Value | |
| Smoking status 1 | ||||||
| Current smoker | 1.787 | 1.082; 2.982 | 0.024 | 1.831 | 1.05; 3.229 | 0.034 |
| Former smoker | 1.083 | 0.661; 1.781 | 0.752 | 1.339 | 0.779; 2.318 | 0.294 |
| Comorbidities 2 | ||||||
| Diabetes mellitus | 0.825 | 0.542; 1.26 | 0.372 | |||
| Renal disease | 0.588 | 0.378; 0.917 | 0.019 | 0.663 | 0.407; 1.083 | 0.099 |
| Intervention details | ||||||
| Pre-interventional occlusion 3 | 5.103 | 3.28; 8.018 | 0.000 | 4.788 | 3.043; 7.609 | 0.000 |
| Popliteal Intervention 4 | 1.758 | 1.163; 2.668 | 0.008 | 1.761 | 1.116; 2.792 | 0.015 |
| Final vessel diameter | 1.012 | 0.775; 1.333 | 0.930 | |||
| Total length of stent | 1.002 | 1; 1.004 | 0.087 | |||
| Stentlocation 5 | ||||||
| Superficial femoral artery mid | 0.778 | 0.285; 2.12 | 0.621 | |||
| Superficial femoral artery distal | 0.667 | 0.278; 1.579 | 0.359 | |||
| Popliteal artery | 1.756 | 0.814; 3.746 | 0.146 | |||
| Multisegmental | 1.697 | 0.827; 3.417 | 0.142 | |||
| Number of patent below the knee arteries 6 | ||||||
| 1 | 3.142 | 0.79; 13.311 | 0.101 | |||
| 2 | 2.250 | 0.575; 9.391 | 0.240 | |||
| 3 | 2.803 | 0.699; 11.965 | 0.142 | |||
| Type of stent 7 | ||||||
| Supera | 0.910 | 0.413; 1.888 | 0.806 | |||
| Viabahn | 1.290 | 0.414; 4.306 | 0.666 | |||
| BioMimics | 0.730 | 0.301; 1.703 | 0.473 | |||
| Zilver | 0.524 | 0.207; 1.277 | 0.161 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Noory, E.; Böhme, T.; Salm, J.; Beschorner, U.; Endress, L.; Bollenbacher, R.; Westermann, D.; Zeller, T. Evaluation of Femoropopliteal In-Stent Restenosis Characteristics Stratified by Stent Design. J. Clin. Med. 2023, 12, 7225. https://doi.org/10.3390/jcm12237225
Noory E, Böhme T, Salm J, Beschorner U, Endress L, Bollenbacher R, Westermann D, Zeller T. Evaluation of Femoropopliteal In-Stent Restenosis Characteristics Stratified by Stent Design. Journal of Clinical Medicine. 2023; 12(23):7225. https://doi.org/10.3390/jcm12237225
Chicago/Turabian StyleNoory, Elias, Tanja Böhme, Jonas Salm, Ulrich Beschorner, Larissa Endress, Roaa Bollenbacher, Dirk Westermann, and Thomas Zeller. 2023. "Evaluation of Femoropopliteal In-Stent Restenosis Characteristics Stratified by Stent Design" Journal of Clinical Medicine 12, no. 23: 7225. https://doi.org/10.3390/jcm12237225
APA StyleNoory, E., Böhme, T., Salm, J., Beschorner, U., Endress, L., Bollenbacher, R., Westermann, D., & Zeller, T. (2023). Evaluation of Femoropopliteal In-Stent Restenosis Characteristics Stratified by Stent Design. Journal of Clinical Medicine, 12(23), 7225. https://doi.org/10.3390/jcm12237225