
Relationship between Middle Cerebral Artery Pulsatility Index and Delayed Neurocognitive Recovery in Patients undergoing Robot-Assisted Laparoscopic Prostatectomy


 ,
, 
 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Anesthesia Protocol
2.2. Data Collection and Measurements
- (1)
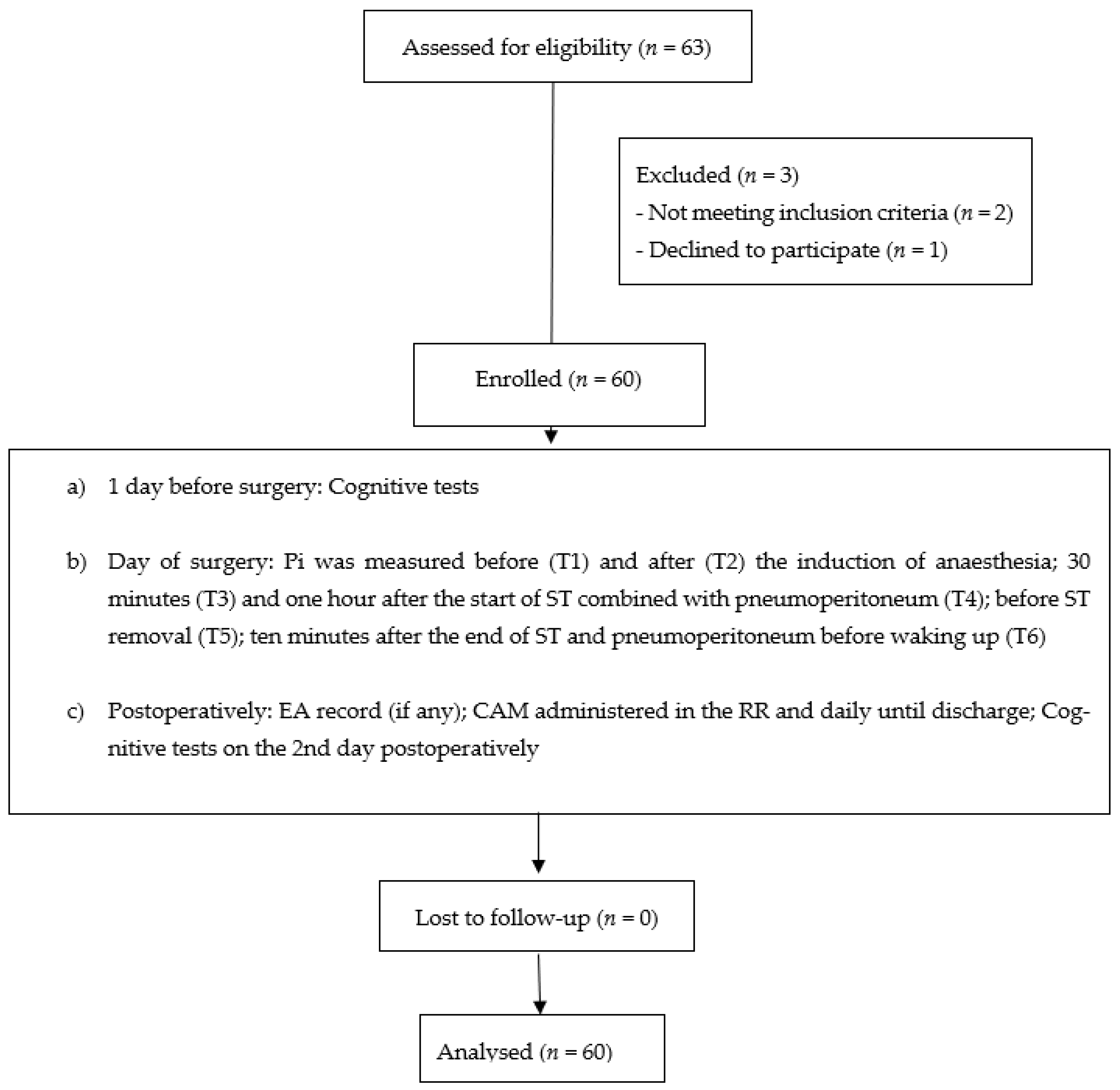
- For the diagnosis of dNCR, the following tests were performed on the day before surgery and on the 2nd day postoperatively: the Rey Auditory Verbal Learning Test (RAVLT), the Raven’s Progressive Matrices test, the trail-making test (part A and part B), the Clock drawing test, a phonemic and semantic verbal fluency test, and the Rey–Osterrieth complex figure test (ROCF). dNCR (dichotomous variable) was diagnosed in the individual patient when there was a postoperative decrement of ≥1 standard deviation (SD) (of the whole group at baseline) in a single test and no improvement (score ≥ 1 SD) in the other tests [7]. An improvement in a test score—between the first and the second assessment—smaller than 1 SD of the whole group at baseline was interpreted as a consequence of the practice effect [8].
- (2)
- The onset of POD was assessed by the Confusion Assessment Method (CAM). CAM was administered in the RR and daily until discharge [9].
- (3)
- (4)
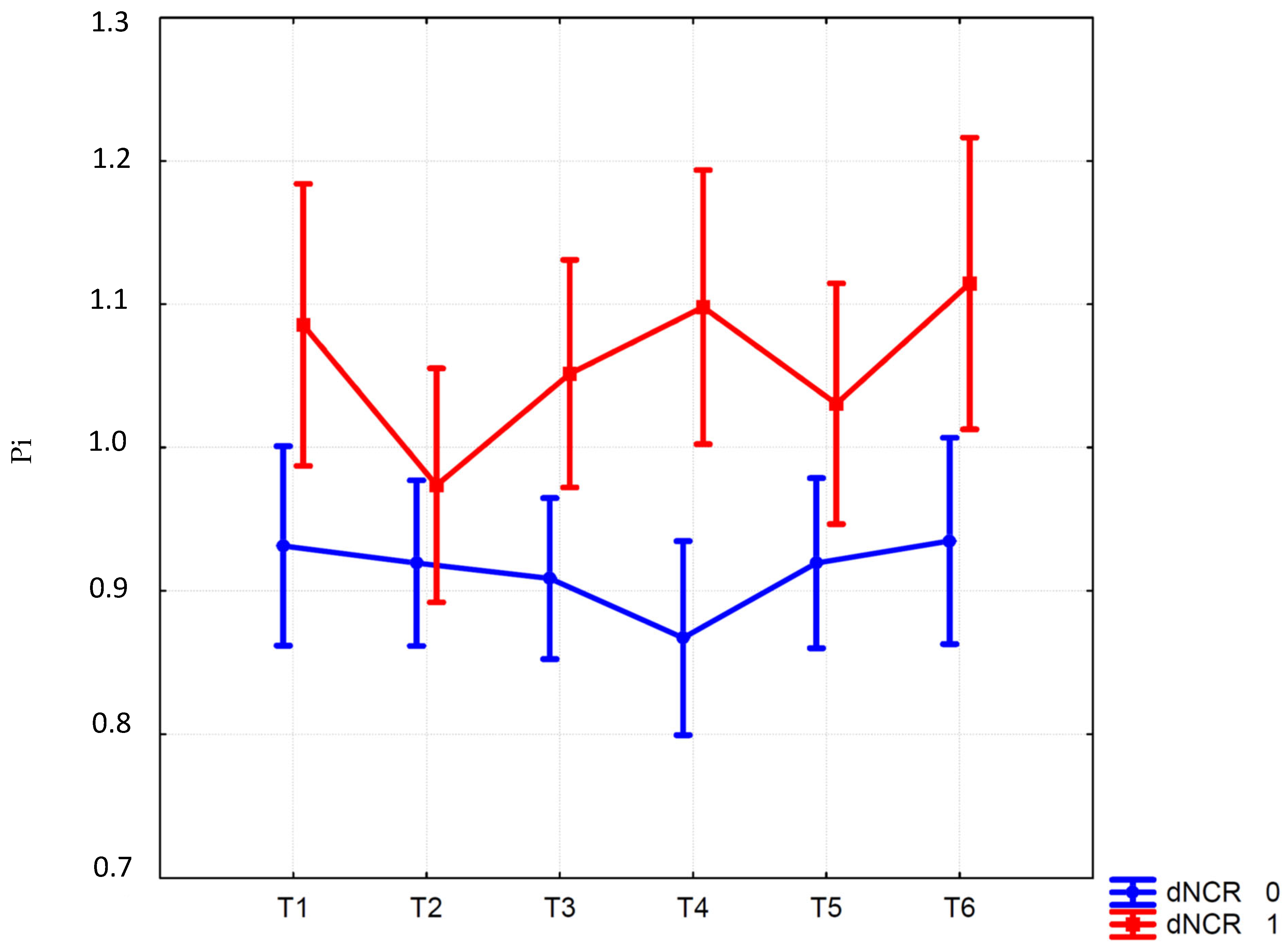
- During surgery, mean blood pressure, heart rate, BIS, carbon dioxide end-tidal, and pneumoperitoneum-pressure values were recorded (when applicable): before (T1) and after (T2) the induction of anesthesia; thirty minutes (T3) and one hour after the start of ST combined with pneumoperitoneum (T4); before ST removal (T5); ten minutes after the end of ST and pneumoperitoneum before waking up (T6). ST, a position used routinely during RALP, involves lowering (by 45 degrees) the top of the operating table from the head side and maintaining this position for almost the entire duration of the surgery. Pneumoperitoneum pressure was applied immediately before ST application and maintained at values < 12 mmHg.
- (5)
- Pain was assessed using NRS ranging from 0 with no pain to 10 with the worst pain ever felt at the following times: at the patient’s arrival in the recovery room, and after 1, 2, 8, 12, 24 and 48 h.
- (6)
- The 36-Item Short Form Health Survey (SF-36) was assessed on the day before surgery and on the 2nd day postoperatively [13].
2.3. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Robba, C.; Cardim, D.; Donnelly, J.; Bertuccio, A.; Bacigaluppi, S.; Bragazzi, N.; Cabella, B.; Liu, X.; Matta, B.; Lattuada, M.; et al. Effects of pneumoperitoneum and Trendelenburg position on intracranial pressure assessed using different non-invasive methods. Br. J. Anaesth. 2016, 117, 783–791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, K.; Wang, L.; Wang, Q.; Liu, X.; Lu, Y.; Li, Y.; Wong, G.T.C. Effects of pneumoperitoneum and steep Trendelenburg position on cerebral hemodynamics during robotic-assisted laparoscopic radical prostatectomy: A randomized controlled study. Medicine 2019, 98, e15794. [Google Scholar] [CrossRef] [PubMed]
- Bellner, J.; Romner, B.; Reinstrup, P.; Kristiansson, K.A.; Ryding, E.; Brandt, L. Transcranial Doppler sonography pulsatility index (PI) reflects intracranial pressure (ICP). Surg. Neurol. 2004, 62, 45–51. [Google Scholar] [CrossRef]
- Gosling, R.G.; King, D.H. Arterial assessment by Doppler-shift ultrasound. Proc. R. Soc. Med. 1974, 67, 447–449. [Google Scholar]
- Budohoski, K.P.; Schmidt, B.; Smielewski, P.; Kasprowicz, M.; Plontke, R.; Pickard, J.D.; Klingelhöfer, J.; Czosnyka, M. Non-invasively estimated ICP pulse amplitude strongly correlates with outcome after TBI. Acta Neurochir. 2012, 114, 121–125. [Google Scholar] [CrossRef]
- Russo, A.; Romanò, B.; Papanice, D.; Cataldo, A.; Gandi, C.; Vaccarella, L.; Totaro, A.; Sacco, E.; Bassi, P.; Aceto, P.; et al. InTrathecal mORphine, traNsversus Abdominis Plane Block, and tramaDOl Infusion for Catheter-Related Bladder Discomfort in Patients Undergoing Robot-Assisted Laparoscopic Prostatectomy (TORNADO): A Pilot Prospective Controlled Study. J. Clin. Med. 2022, 11, 2136. [Google Scholar] [CrossRef]
- Evered, L.; Silbert, B.; Knopman, D.S.; Scott, D.A.; DeKosky, S.T.; Rasmussen, L.S.; Oh, E.S.; Crosby, G.; Berger, M.; Eckenhoff, R.G. Nomenclature Consensus Working Group. Recommendations for the nomenclature of cognitive change associated with anaesthesia and surgery-2018. Br. J. Anaesth. 2018, 121, 1005–1012. [Google Scholar] [CrossRef] [Green Version]
- Collie, A.; Maruff, P.; Darby, D.G.; McStephen, M. The effects of practice on the cognitive test performance of neurologically normal individuals assessed at brief test-retest intervals. J. Int. Neuropsychol. Soc. 2003, 9, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Aldecoa, C.; Bettelli, G.; Bilotta, F.; Sanders, R.D.; Audisio, R.; Borozdina, A.; Cherubini, A.; Jones, C.; Kehlet, H.; MacLullich, A.; et al. European Society of Anaesthesiology evidence-based and consensus-based guideline on postoperative delirium. Eur. J. Anaesthesiol. 2017, 34, 192–214. [Google Scholar] [CrossRef]
- Spielberger, C.D.; Sydeman, S.J. State-trait anxiety inventory and state-trait anger expression inventory. In The Use of Psychological Testing for Treatment Planning and Outcome Assessment; Maruish, M.E., Ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1994; pp. 292–321. [Google Scholar]
- Beck, A.; Brown, G.; Steer, R. Beck Depression Inventory-II Manual; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- D’Andrea, A.; Conte, M.; Scarafile, R.; Riegler, L.; Cocchia, R.; Pezzullo, E.; Cavallaro, M.; Carbone, A.; Natale, F.; Russo, M.G.; et al. Transcranial Doppler Ultrasound: Physical Principles and Principal Applications in Neurocritical Care Unit. J. Cardiovasc. Echogr. 2016, 26, 28–41. [Google Scholar] [CrossRef] [Green Version]
- Apolone, G.; Mosconi, P. The Italian SF-36 Health Survey: Translation, validation and norming. J. Clin. Epidemiol. 1998, 51, 1025–1036. [Google Scholar] [CrossRef] [PubMed]
- Aceto, P.; Incalzi, R.A.; Bettelli, G.; Carron, M.; Chiumiento, F.; Corcione, A.; Crucitti, A.; Maggi, S.; Montorsi, M.; Pace, M.C.; et al. Perioperative Management of Elderly patients (PriME): Recommendations from an Italian intersociety consensus. Aging Clin. Exp. Res. 2020, 32, 1647–1673. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.-S.; Bai, S.-J.; Lee, J.-R.; Choi, Y.D.; Kim, Y.J.; Choi, S.H. Increase in intracranial pressure during carbon dioxide pneumoperitoneum with steep Trendelenburg positioning proven by ultrasonographic measurement of optic nerve sheath diameter. J. Endourol. 2014, 28, 801–806. [Google Scholar] [CrossRef] [PubMed]
- Kalmar, A.F.; Foubert, L.; Hendrickx, J.F.; Mottrie, A.; Absalom, A.; Mortier, E.P.; Struys, M.M. Influence of steep Trendelenburg position and CO2 pneumoperitoneum on cardiovascular, cerebrovascular, and respiratory homeostasis during robotic prostatectomy. Br. J. Anaesth. 2010, 104, 433–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- La Falce, S.; Novara, G.; Gandaglia, G.; Umari, P.; De Naeyer, G.; D’Hondt, F.; Beresian, J.; Carette, R.; Penicka, M.; Mo, Y.; et al. Low Pressure Robot-assisted Radical Prostatectomy with the AirSeal System at OLV Hospital: Results from a Prospective Study. Clin. Genitourin. Cancer 2017, 15, e1029–e1037. [Google Scholar] [CrossRef]
- Goettel, N.; Burkhart, C.S.; Rossi, A.; Cabella, B.C.; Berres, M.; Monsch, A.U.; Czosnyka, M.; Steiner, L.A. Associations Between Impaired Cerebral Blood Flow Autoregulation, Cerebral Oxygenation, and Biomarkers of Brain Injury and Postoperative Cognitive Dysfunction in Elderly Patients After Major Noncardiac Surgery. Anesth. Analg. 2017, 124, 934–942. [Google Scholar] [CrossRef]
- Aceto, P.; Lai, C.; De Crescenzo, F.; Crea, M.A.; Di Franco, V.; Pellicano, G.R.; Perilli, V.; Lai, S.; Papanice, D.; Sollazzi, L. Cognitive decline after carotid endarterectomy: Systematic review and meta-analysis. Eur. J. Anaesthesiol. 2020, 37, 1066–1074. [Google Scholar] [CrossRef]
- Cheng, C.; Wan, H.; Cong, P.; Huang, X.; Wu, T.; He, M.; Zhang, Q.; Xiong, L.; Tian, L. Targeting neuroinflammation as a preventive and therapeutic approach for perioperative neurocognitive disorders. J. Neuroinflamm. 2022, 19, 297. [Google Scholar] [CrossRef]
- Aceto, P.; Beretta, L.; Cariello, C.; Claroni, C.; Esposito, C.; Forastiere, E.M.; Guarracino, F.; Perucca, R.; Romagnoli, S.; Sollazzi, L.; et al. Joint consensus on anesthesia in urologic and gynecologic robotic surgery: Specific issues in management from a task force of the SIAARTI, SIGO, and SIU. Minerva Anestesiol. 2019, 85, 871–885. [Google Scholar] [CrossRef]
- Aceto, P.; Perilli, V.; Lai, C.; Ciocchetti, P.; Vitale, F.; Sollazzi, L. Postoperative cognitive dysfunction after liver transplantation. Gen. Hosp. Psychiatry 2015, 37, 109–115. [Google Scholar] [CrossRef]
- Chan, M.T.V.; Cheng, B.C.P.; Lee, T.M.C.; Gin, T. BIS-guided anesthesia decreases postoperative delirium and cognitive decline. J. Neurosurg. Anesthesiol. 2013, 25, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Kotekar, N.; Shenkar, A.; Nagaraj, R. Postoperative cognitive dysfunction—Current preventive strategies. Clin. Interv. Aging 2018, 13, 2267–2273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ursino, M.; Giulioni, M.; Lodi, C.A. Relationships among cerebral perfusion pressure, autoregulation, and transcranial Doppler waveform: A modeling study. J. Neurosurg. 1998, 89, 255–266. [Google Scholar] [CrossRef] [PubMed]
- Ripa, M.; Schipa, C.; Kopsacheilis, N.; Nomikarios, M.; Perrotta, G.; De Rosa, C.; Aceto, P.; Sollazzi, L.; De Rosa, P.; Motta, L. The Impact of Steep Trendelenburg Position on Intraocular Pressure. J. Clin. Med. 2022, 11, 2844. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patients without dNCR (n = 40) | Patients with dNCR (n = 20) | t or χ2 (df) | p | |
|---|---|---|---|---|
| Age, years | 69.6 (68.6–70.6) | 70.6 (68.4–72.6) | −1.04 (58) | 0.30 |
| BMI, kg/m2 | 26.2 (25.3–27.2) | 25.7 (24.4–27.0) | 0.72 (58) | 0.47 |
| ASA, II/III | 38/2 | 19/1 | 0.39 (2) | 0.53 |
| CCI | 4.6 (4.3–4.8) | 4.7 (4.3–5.0) | −0.63 (58) | 0.53 |
| MMSE | 25.3 (24.2–26.5) | 26.0 (25.5–26.4) | 1.28 (58) | 0.21 |
| STAI-Y1 | 34.7 (30.8–38.6) | 35.5 (30.2–40.8) | −0.24 (58) | 0.80 |
| STAI-Y2 | 31.3 (29.4–33.2) | 33.1 (29.0–37.3) | −0.93 (58) | 0.35 |
| DBI-II | 7.6 (5.9–9.4) | 8.7 (5.4–12.0) | −0.67 (58) | 0.50 |
| Balanced solution, ml | 620.0 (535.8–704.2) | 605.0 (448.1–761.9) | 0.19 (58) | 0.85 |
| Surgery duration, min | 178.1 (162.7–193.6) | 176.8 (158.0–195.7) | 0.10 (58) | 0.92 |
| Anesthesia duration, min | 207.2 (190.8–223.6) | 208.2 (188.2–228.2) | −0–07 (58) | 0.94 |
| ST duration, min | 145.3 (132.1–158.5) | 150.1 (134.2–165.9) | −0.44 (58) | 0.66 |
| Diuresis, ml | 234.7 (200.7–268.8) | 303.0 (208.7–397.3) | −1.72 (58) | 0.09 |
| I.O. Remifentanil, mcg | 745.5 (621.9–869.1) | 984.7 (708.6–1260.9) | −1.89 (58) | 0.06 |
| P.O. Morphine, Yes/No | 5/35 | 4/16 | 0.15 1) | 0.70 |
| P.O. Tramadol, Yes/No | 13/27 | 6/14 | 0.01 (1) | 0.92 |
| EA, Yes/No | 5/35 | 6/14 | 1.68 (1) | 0.19 |
| POD, Yes/No | 0/40 | 3/17 | 3.55 (1) | 0.03 |
| Hospital stay (days) | 5.1 (4.7–5.5) | 5.7 (4.4–6.9) | −1.06 (58) | 0.29 |
| Patients without dNCR (n = 40) | Patients with dNCR (n = 20) | t (df = 58) | p | |
|---|---|---|---|---|
| RAVLT, stm | 1.3 (0.6–2.1) | 0.1 (−0.8–1.0) | 2.03 | 0.04 |
| RAVLT, ltm | 4.2 (3.2–5.1) | 1.4 (−0.2–3.1) | 3.19 | 0.002 |
| RAVLT, re | 1.5 (0.9–2.2) | −0.4 (−1.3–0.5) | 3.55 | 0.0007 |
| RPMT | −0.01 (−0.8–0.8) | 0.09 (−1.3–1.5) | −0.14 | 0.89 |
| TMT-A | 8.7 (−1.8–19.2) | −4.8 (−20.1–10.3) | 1.51 | 0.14 |
| TMT-B | 3.7 (−13.6–21.0) | −2.6 (−30.3–25.1) | 0.41 | 0.68 |
| CDT | −0.3 (−0.6–0.01) | 0.05 (−0.6–0.7) | −1.12 | 0.27 |
| pVFT | 0.6 (−1.2–2.5) | −0.14 (−3.4–3.1) | 0.46 | 0.65 |
| sVFT | 0.8 (−0.5–2.2) | 0.16 (−1.5–1.9) | 0.63 | 0.53 |
| ROCF, copy | −2.8 (−5.2–−0.4) | −3.5 (−5.5–−1.6) | 0.41 | 0.68 |
| ROCF, recall | 4.6 (3.0–6.3) | 1.2 (−0.9–3.2) | 2.60 | 0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aceto, P.; Russo, A.; Galletta, C.; Schipa, C.; Romanò, B.; Luca, E.; Sacco, E.; Totaro, A.; Lai, C.; Mazza, M.; et al. Relationship between Middle Cerebral Artery Pulsatility Index and Delayed Neurocognitive Recovery in Patients undergoing Robot-Assisted Laparoscopic Prostatectomy. J. Clin. Med. 2023, 12, 1070. https://doi.org/10.3390/jcm12031070
Aceto P, Russo A, Galletta C, Schipa C, Romanò B, Luca E, Sacco E, Totaro A, Lai C, Mazza M, et al. Relationship between Middle Cerebral Artery Pulsatility Index and Delayed Neurocognitive Recovery in Patients undergoing Robot-Assisted Laparoscopic Prostatectomy. Journal of Clinical Medicine. 2023; 12(3):1070. https://doi.org/10.3390/jcm12031070
Chicago/Turabian StyleAceto, Paola, Andrea Russo, Claudia Galletta, Chiara Schipa, Bruno Romanò, Ersilia Luca, Emilio Sacco, Angelo Totaro, Carlo Lai, Marianna Mazza, and et al. 2023. "Relationship between Middle Cerebral Artery Pulsatility Index and Delayed Neurocognitive Recovery in Patients undergoing Robot-Assisted Laparoscopic Prostatectomy" Journal of Clinical Medicine 12, no. 3: 1070. https://doi.org/10.3390/jcm12031070
APA StyleAceto, P., Russo, A., Galletta, C., Schipa, C., Romanò, B., Luca, E., Sacco, E., Totaro, A., Lai, C., Mazza, M., Federico, B., & Sollazzi, L. (2023). Relationship between Middle Cerebral Artery Pulsatility Index and Delayed Neurocognitive Recovery in Patients undergoing Robot-Assisted Laparoscopic Prostatectomy. Journal of Clinical Medicine, 12(3), 1070. https://doi.org/10.3390/jcm12031070