
Talimogene Laherparepvec (T-VEC): A Review of the Recent Advances in Cancer Therapy

Abstract
:1. Introduction
2. Overview of Oncolytic Virus and T-VEC
3. T-VEC Treatment for Melanoma
3.1. T-VEC Monotherapy for Melanoma and Path to FDA Approval
3.2. T-VEC Combinational Therapy for Melanoma
3.2.1. Rationale for T-VEC Combinational Therapy
3.2.2. Clinical Trials of T-VEC Combinational Therapy for Melanoma
4. T-VEC Treatment in Other Cutaneous Cancer Types
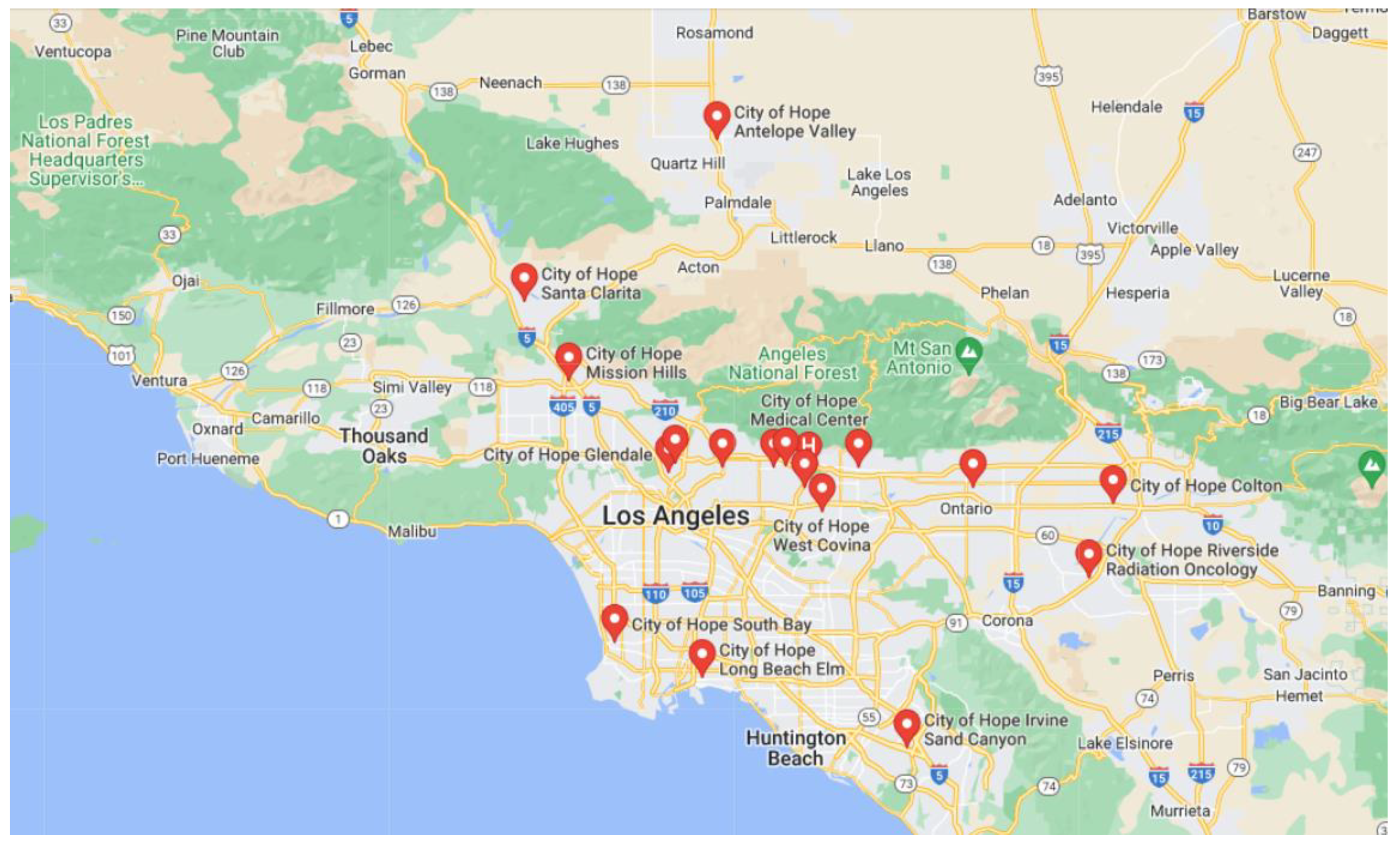
5. T-VEC Treatment Practices in City of Hope
6. Discussion and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kaushik, I.; Ramachandran, S.; Zabel, C.; Gaikwad, S.; Srivastava, S.K. The evolutionary legacy of immune checkpoint inhibitors. Semin. Cancer Biol. 2022, 86 Pt 2, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Naimi, A.; Mohammed, R.N.; Raji, A.; Chupradit, S.; Yumashev, A.V.; Suksatan, W.; Shalaby, M.N.; Thangavelu, L.; Kamrava, S.; Shomali, N.; et al. Tumor immunotherapies by immune checkpoint inhibitors (ICIs); the pros and cons. Cell Commun. Signal. 2022, 20, 44. [Google Scholar] [CrossRef]
- Chaurasiya, S.; Fong, Y.; Warner, S.G. Oncolytic Virotherapy for Cancer: Clinical Experience. Biomedicines 2021, 9, 419. [Google Scholar] [CrossRef] [PubMed]
- Toda, M.; Martuza, R.L.; Rabkin, S.D. Tumor growth inhibition by intratumoral inoculation of defective herpes simplex virus vectors expressing granulocyte-macrophage colony-stimulating factor. Mol. Ther. 2000, 2, 324–329. [Google Scholar] [CrossRef]
- Kohlhapp, F.J.; Kaufman, H.L. Molecular Pathways: Mechanism of Action for Talimogene Laherparepvec, a New Oncolytic Virus Immunotherapy. Clin. Cancer Res. 2016, 22, 1048–1054. [Google Scholar] [CrossRef] [Green Version]
- Hu, J.C.; Coffin, R.S.; Davis, C.J.; Graham, N.J.; Groves, N.; Guest, P.J.; Harrington, K.J.; James, N.D.; Love, C.A.; McNeish, I.; et al. A phase I study of OncoVEXGM-CSF, a second-generation oncolytic herpes simplex virus expressing granulocyte macrophage colony-stimulating factor. Clin. Cancer Res. 2006, 12, 6737–6747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Senzer, N.N.; Kaufman, H.L.; Amatruda, T.; Nemunaitis, M.; Reid, T.; Daniels, G.; Gonzalez, R.; Glaspy, J.; Whitman, E.; Harrington, K.; et al. Phase II clinical trial of a granulocyte-macrophage colony-stimulating factor-encoding, second-generation oncolytic herpesvirus in patients with unresectable metastatic melanoma. J. Clin. Oncol. 2009, 27, 5763–5771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andtbacka, R.H.; Kaufman, H.L.; Collichio, F.; Amatruda, T.; Senzer, N.; Chesney, J.; Delman, K.A.; Spitler, L.E.; Puzanov, I.; Agarwala, S.S.; et al. Talimogene Laherparepvec Improves Durable Response Rate in Patients With Advanced Melanoma. J. Clin. Oncol. 2015, 33, 2780–2788. [Google Scholar] [CrossRef]
- Andtbacka, R.H.I.; Collichio, F.; Harrington, K.J.; Middleton, M.R.; Downey, G.; Öhrling, K.; Kaufman, H.L. Final analyses of OPTiM: A randomized phase III trial of talimogene laherparepvec versus granulocyte-macrophage colony-stimulating factor in unresectable stage III-IV melanoma. J. Immunother. Cancer 2019, 7, 145. [Google Scholar] [CrossRef] [Green Version]
- Chesney, J.; Puzanov, I.; Collichio, F.; Singh, P.; Milhem, M.M.; Glaspy, J.; Hamid, O.; Ross, M.; Friedlander, P.; Garbe, C.; et al. Randomized, Open-Label Phase II Study Evaluating the Efficacy and Safety of Talimogene Laherparepvec in Combination With Ipilimumab Versus Ipilimumab Alone in Patients With Advanced, Unresectable Melanoma. J. Clin. Oncol. 2018, 36, 1658–1667. [Google Scholar] [CrossRef]
- Ribas, A.; Dummer, R.; Puzanov, I.; VanderWalde, A.; Andtbacka, R.H.I.; Michielin, O.; Olszanski, A.J.; Malvehy, J.; Cebon, J.; Fernandez, E.; et al. Oncolytic Virotherapy Promotes Intratumoral T Cell Infiltration and Improves Anti-PD-1 Immunotherapy. Cell 2017, 170, 1109–1119.e10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ribas, A.; Chesney, J.; Long, G.V.; Kirkwood, J.M.; Dummer, R.; Puzanov, I.; Hoeller, C.; Gajewski, T.F.; Gutzmer, R.; Rutkowski, P.; et al. 1037O MASTERKEY-265: A phase III, randomized, placebo (Pbo)-controlled study of talimogene laherparepvec (T) plus pembrolizumab (P) for unresectable stage IIIB–IVM1c melanoma (MEL). Ann. Oncol. 2021, 32, S868–S869. [Google Scholar] [CrossRef]
- Thompson, J.F.; Agarwala, S.S.; Smithers, B.M.; Ross, M.I.; Scoggins, C.R.; Coventry, B.J.; Neuhaus, S.J.; Minor, D.R.; Singer, J.M.; Wachter, E.A. Phase 2 Study of Intralesional PV-10 in Refractory Metastatic Melanoma. Ann. Surg. Oncol. 2015, 22, 2135–2142. [Google Scholar] [CrossRef] [Green Version]
- Westbrook, B.C.; Norwood, T.G.; Terry, N.L.J.; McKee, S.B.; Conry, R.M. Talimogene laherparepvec induces durable response of regionally advanced Merkel cell carcinoma in 4 consecutive patients. JAAD Case Rep. 2019, 5, 782–786. [Google Scholar] [CrossRef]
- Knackstedt, R.; Sussman, T.A.; McCahon, L.; Song, J.M.; Funchain, P.; Gastman, B. Pre-treated anti-PD-1 refractory Merkel cell carcinoma successfully treated with the combination of PD-1/PD-L1 axis inhibitors and TVEC: A report of two cases. Ann. Oncol. 2019, 30, 1399–1400. [Google Scholar] [CrossRef] [PubMed]
- Shalhout, S.Z.; Kaufman, H.L.; Emerick, K.S.; Miller, D.M. Immunotherapy for Nonmelanoma Skin Cancer: Facts and Hopes. Clin. Cancer Res. 2022, 28, 2211–2220. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Suryawanshi, Y.R.; Kordish, D.H.; Woyczesczyk, H.M.; Jeng, D.; Essani, K. Tanapoxvirus lacking a neuregulin-like gene regresses human melanoma tumors in nude mice. Virus Genes 2017, 53, 52–62. [Google Scholar] [CrossRef] [Green Version]
- Viale, D.L.; Cafferata, E.G.; Gould, D.; Rotondaro, C.; Chernajovsky, Y.; Curiel, D.T.; Podhajcer, O.L.; Veronica Lopez, M. Therapeutic improvement of a stroma-targeted CRAd by incorporating motives responsive to the melanoma microenvironment. J. Investig. Dermatol. 2013, 133, 2576–2584. [Google Scholar] [CrossRef] [Green Version]
- Vaha-Koskela, M.J.; Heikkila, J.E.; Hinkkanen, A.E. Oncolytic viruses in cancer therapy. Cancer Lett. 2007, 254, 178–216. [Google Scholar] [CrossRef]
- Zhang, T.; Suryawanshi, Y.R.; Szymczyna, B.R.; Essani, K. Neutralization of matrix metalloproteinase-9 potentially enhances oncolytic efficacy of tanapox virus for melanoma therapy. Med. Oncol. 2017, 34, 129. [Google Scholar] [CrossRef]
- Zhang, T.; Kordish, D.H.; Suryawanshi, Y.R.; Eversole, R.R.; Kohler, S.; Mackenzie, C.D.; Essani, K. Oncolytic Tanapoxvirus Expressing Interleukin-2 is Capable of Inducing the Regression of Human Melanoma Tumors in the Absence of T Cells. Curr. Cancer Drug Targets 2018, 18, 577–591. [Google Scholar] [CrossRef]
- Liu, B.L.; Robinson, M.; Han, Z.Q.; Branston, R.H.; English, C.; Reay, P.; McGrath, Y.; Thomas, S.K.; Thornton, M.; Bullock, P.; et al. ICP34.5 deleted herpes simplex virus with enhanced oncolytic, immune stimulating, and anti-tumour properties. Gene Ther. 2003, 10, 292–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, T.; Suryawanshi, Y.R.; Woyczesczyk, H.M.; Essani, K. Targeting Melanoma with Cancer-Killing Viruses. Open Virol. J. 2017, 11, 28–47. [Google Scholar] [CrossRef] [Green Version]
- Hawkins, L.K.; Lemoine, N.R.; Kirn, D. Oncolytic biotherapy: A novel therapeutic plafform. Lancet Oncol. 2002, 3, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, N.; Koga, H.; Kojima, T.; Tsutsumida, A.; Namikawa, K.; Yi, M.; Mera, K.; Pickett-Gies, C. Early safety from a phase I, multicenter, open-label, dose de-escalation study of talimogene laherparepvec (T-VEC) in Japanese patients (pts) with unresectable stage IIIB-IV melanoma (MEL). Ann. Oncol. 2018, 29, ix107. [Google Scholar] [CrossRef]
- Cancer Genome Atlas, N. Genomic Classification of Cutaneous Melanoma. Cell 2015, 161, 1681–1696. [Google Scholar] [CrossRef] [Green Version]
- Ascierto, P.A.; McArthur, G.A.; Dreno, B.; Atkinson, V.; Liszkay, G.; Di Giacomo, A.M.; Mandala, M.; Demidov, L.; Stroyakovskiy, D.; Thomas, L.; et al. Cobimetinib combined with vemurafenib in advanced BRAF(V600)-mutant melanoma (coBRIM): Updated efficacy results from a randomised, double-blind, phase 3 trial. Lancet Oncol. 2016, 17, 1248–1260. [Google Scholar] [CrossRef]
- Curti, B.D.; Faries, M.B. Recent Advances in the Treatment of Melanoma. N. Engl. J. Med. 2021, 384, 2229–2240. [Google Scholar] [CrossRef]
- Tarhini, A.A.; Lee, S.J.; Hodi, F.S.; Rao, U.N.M.; Cohen, G.I.; Hamid, O.; Hutchins, L.F.; Sosman, J.A.; Kluger, H.M.; Eroglu, Z.; et al. Phase III Study of Adjuvant Ipilimumab (3 or 10 mg/kg) Versus High-Dose Interferon Alfa-2b for Resected High-Risk Melanoma: North American Intergroup E1609. J. Clin. Oncol. 2020, 38, 567–575. [Google Scholar] [CrossRef]
- Eggermont, A.M.; Chiarion-Sileni, V.; Grob, J.J.; Dummer, R.; Wolchok, J.D.; Schmidt, H.; Hamid, O.; Robert, C.; Ascierto, P.A.; Richards, J.M.; et al. Prolonged Survival in Stage III Melanoma with Ipilimumab Adjuvant Therapy. N. Engl. J. Med. 2016, 375, 1845–1855. [Google Scholar] [CrossRef]
- Sun, L.; Funchain, P.; Song, J.M.; Rayman, P.; Tannenbaum, C.; Ko, J.; McNamara, M.; Marcela Diaz-Montero, C.; Gastman, B. Talimogene Laherparepvec combined with anti-PD-1 based immunotherapy for unresectable stage III-IV melanoma: A case series. J. Immunother. Cancer 2018, 6, 36. [Google Scholar] [CrossRef] [PubMed]
- Dummer, R.; Hoeller, C.; Gruter, I.P.; Michielin, O. Combining talimogene laherparepvec with immunotherapies in melanoma and other solid tumors. Cancer Immunol. Immunother. 2017, 66, 683–695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Long, G.; Dummer, R.; Johnson, D.; Michielin, O.; Martin-Algarra, S.; Treichel, S.; Chan, E.; Diede, S.; Ribas, A. 429 Long-term analysis of MASTERKEY-265 phase 1b trial of talimogene laherparepvec (T-VEC) plus pembrolizumab in patients with unresectable stage IIIB-IVM1c melanoma. J. ImmunoTher. Cancer 2020, 8 (Suppl. S3), A261. [Google Scholar] [CrossRef]
- Malvehy, J.; Samoylenko, I.; Schadendorf, D.; Gutzmer, R.; Grob, J.J.; Sacco, J.J.; Gorski, K.S.; Anderson, A.; Pickett, C.A.; Liu, K.; et al. Talimogene laherparepvec upregulates immune-cell populations in non-injected lesions: Findings from a phase II, multicenter, open-label study in patients with stage IIIB-IVM1c melanoma. J. Immunother. Cancer 2021, 9, e001621. [Google Scholar] [CrossRef] [PubMed]
- Chan, I.S.; Bhatia, S.; Kaufman, H.L.; Lipson, E.J. Immunotherapy for Merkel cell carcinoma: A turning point in patient care. J. Immunother. Cancer 2018, 6, 23. [Google Scholar] [CrossRef] [Green Version]
- Burns, C.; Kubicki, S.; Nguyen, Q.B.; Aboul-Fettouh, N.; Wilmas, K.M.; Chen, O.M.; Doan, H.Q.; Silapunt, S.; Migden, M.R. Advances in Cutaneous Squamous Cell Carcinoma Management. Cancers 2022, 14, 3653. [Google Scholar] [CrossRef]
- Curiel, C.N.; Stratton, D.; Cui, H.; Roe, D.; Tiwari, H.A.; Sundararajan, S. A single arm phase 2 study of talimogene laherparepvec in patients with low-risk invasive cutaneous squamous cell cancer. Interim analysis. J. Clin. Oncol. 2022, 40 (Suppl. 16), e21583. [Google Scholar] [CrossRef]
- Kai, M.; Marx, A.N.; Liu, D.D.; Shen, Y.; Gao, H.; Reuben, J.M.; Whitman, G.; Krishnamurthy, S.; Ross, M.I.; Litton, J.K.; et al. A phase II study of talimogene laherparepvec for patients with inoperable locoregional recurrence of breast cancer. Sci. Rep. 2021, 11, 22242. [Google Scholar] [CrossRef]
- Soliman, H.; Hogue, D.; Han, H.; Mooney, B.; Costa, R.; Lee, M.C.; Niell, B.; Williams, A.; Chau, A.; Falcon, S.; et al. A Phase I Trial of Talimogene Laherparepvec in Combination with Neoadjuvant Chemotherapy for the Treatment of Nonmetastatic Triple-Negative Breast Cancer. Clin. Cancer Res. 2021, 27, 1012–1018. [Google Scholar] [CrossRef]
- Hecht, J.R.; Pless, M.; Cubillo, A.; Calvo, A.; Chon, H.J.; Liu, C.; Snyder, W.; Chan, E.; Chaney, M.F.; Chesney, J.A.; et al. Early safety from a phase I, multicenter, open-label clinical trial of talimogene laherparepvec (T-VEC) injected (inj) into liver tumors in combination with pembrolizumab (pem). J. Clin. Oncol. 2020, 38 (Suppl. 15), 3015. [Google Scholar] [CrossRef]
- Silk, A.W.; LeBoeuf, N.R.; Rabinowits, G.; Puzanov, I.; Burgess, M.A.; Devata, S.; Moore, D.; Goydos, J.S.; Chen, H.X.; Kaufman, H.; et al. A phase II study of talimogene laherparepvec followed by talimogene laherparepvec + nivolumab in refractory T cell and NK cell lymphomas, cutaneous squamous cell carcinoma, Merkel cell carcinoma, and other rare skin tumors (NCI #10057). J. Clin. Oncol. 2018, 36 (Suppl. 5), TPS219. [Google Scholar] [CrossRef]
- Cilento, M.A.; Klein, O.; Egan, E.; Roberts-Thomson, R. Talimogene laherparepvec resulting in near-complete response in a patient with treatment-refractory Merkel cell carcinoma. Australas. J. Dermatol. 2022, 63, e222–e225. [Google Scholar] [CrossRef] [PubMed]
- Dummer, R.; Gyorki, D.E.; Hyngstrom, J.; Berger, A.C.; Conry, R.; Demidov, L.; Sharma, A.; Treichel, S.A.; Radcliffe, H.; Gorski, K.S.; et al. Neoadjuvant talimogene laherparepvec plus surgery versus surgery alone for resectable stage IIIB-IVM1a melanoma: A randomized, open-label, phase 2 trial. Nat. Med. 2021, 27, 1789–1796. [Google Scholar] [CrossRef] [PubMed]
- Havunen, R.; Kalliokoski, R.; Siurala, M.; Sorsa, S.; Santos, J.M.; Cervera-Carrascon, V.; Anttila, M.; Hemminki, A. Cytokine-Coding Oncolytic Adenovirus TILT-123 Is Safe, Selective, and Effective as a Single Agent and in Combination with Immune Checkpoint Inhibitor Anti-PD-1. Cells 2021, 10, 246. [Google Scholar] [CrossRef]
- Breitbach, C.J.; Bell, J.C.; Hwang, T.H.; Kirn, D.H.; Burke, J. The emerging therapeutic potential of the oncolytic immunotherapeutic Pexa-Vec (JX-594). Oncolytic Virotherapy 2015, 4, 25–31. [Google Scholar] [CrossRef] [Green Version]
- Shibakita, M.; Tachibana, M.; Dhar, D.K.; Kotoh, T.; Kinugasa, S.; Kubota, H.; Masunaga, R.; Nagasue, N. Prognostic significance of Fas and Fas ligand expressions in human esophageal cancer. Clin. Cancer Res. 1999, 5, 2464–2469. [Google Scholar]
- Liu, Z.; Ravindranathan, R.; Kalinski, P.; Guo, Z.S.; Bartlett, D.L. Rational combination of oncolytic vaccinia virus and PD-L1 blockade works synergistically to enhance therapeutic efficacy. Nat. Commun. 2017, 8, 14754. [Google Scholar] [CrossRef]


{kind=link}
| Reference | Study Drugs/Mechanisms of Action | Phase (n) | Disease | Treatment | Overall Response Rate | Progression-Free Survival (Month) | Overall Survival (Month) | |
|---|---|---|---|---|---|---|---|---|
| I | T-VEC monotherapy for melanoma | |||||||
| 1 | A Phase I Study of OncoVEXGM-CSF, a Second-Generation Oncolytic Herpes Simplex Virus Expressing Granulocyte Macrophage Colony-Stimulating Factor [6] | talimogene laherparepvec (TVEC)/oncolytic virus therapy (OVT) | Phase I (n = 30) | Refractory cutaneous and subcutaneous metastases from breast cancer, gastrointestinal adenocarcinoma, Malignant Melanoma, and Epithelial cancer of head and neck | TVEC | N/A | N/A | N/A |
| 2 | Phase II clinical trial of a granulocyte-macrophage colony-stimulating factor-encoding, second-generation oncolytic herpesvirus in patients with unresectable metastatic melanoma [7] | TVEC/OVT | Phase II (n = 50) | Stage IIIc unresectable metastatic melanoma | TVEC | 26% | N/A | 16 |
| 3 | Final analyses of OPTiM: a randomized phase III trial of talimogene laherparepvec versus granulocyte-macrophage colony-stimulating factor in unresectable stage III–IV melanoma (NCT00769704) [8,9] | TVEC/OVT GM-CSF/bone marrow stimulation | Phase III (n = 436) | Stage IIIB to IV melanoma | A: TVEC B: GM-CSF | 31.50% 6.40% | N/A | 23.3 18.9 A: 73.7% at 1 year, 49.8% at 2 year, and 38.9% at 3 year B: 69.1% at 1 year, 40.3% at 2 year, and 30.4% at 3 year |
| II | T-VEC combinational therapy for melanoma | |||||||
| 1 | Randomized, open-label phase II study evaluating the efficacy and safety of talimogene laherparepvec in combination with ipilimumab versus ipilimumab alone in patients with advanced, unresectable melanoma (NCT01740297) [10] | TVEC/OVT Ipilimumab/CTLA-4 inhibitor | Phase II (n = 198) | Melanoma | A: TVEC + ipilimumab B: ipilimumab | 39% 18% | 8.2 6.4 | 86.9% at 1 year, 76.6% at 2 year 81.4% at 1 year, 67.7% at 2 year |
| 2 | A phase 1/3 multicenter trial of talimogene laherparepvec in combination with pembrolizumab for unresected, stage IIIB-IV melanoma. MASTERKEY-265 (NCT02263508) [11] | TVEC/OVT Pembrolizumab/PD-1 inhibitor | Phase 1b (n = 21) | unresectable, stage IIIB-IVM1c melanoma | A: TVEC + Pembrolizumab B: Placebo + Pembrolizumab | N/A | 25.6 25.5 | N/A |
| 3 | 1037O MASTERKEY-265: A phase III, randomized, placebo (Pbo)-controlled study of talimogene laherparepvec (T) plus pembrolizumab (P) for unresectable stage IIIB–IVM1c melanoma (MEL). KENNOTE-034 (NCT02263508) [12] | TVEC/OVT Pembrolizumab/PD-1 inhibitor | Phase III (n = 692) | unresectable stage III-IVM1c melanoma | A: TVEC + Pembrolizumab B: Placebo + Pembrolizumab | 48.60% 41.30% | 14.3 8.5 | 66% at 2 year 49.2 |
| 4 | PV-10 vs Chemotherapy or Oncolytic Viral Therapy for Treatment of Locally Advanced Cutaneous Melanoma (NCT02288897) [13] | PV-10 (10% rose Bengal disodium)/oncolytic immunotherapy | Phase III (n = 20) | Cutaneous Melanoma | A: PV-10 (10% rose Bengal disodium) B: Dacarbazine, temozolomide or TVEC | N/A Only has complete response rate (CRR) | 6.1 (1.5 to 28.9) 8.6 (1.8 to 14.4) | N/A N/A |
| III | T-VEC treatment in other cutaneous cancer types | |||||||
| 1 | Talimogene laherparepvec induces durable response of regionally advanced Merkel cell carcinoma in 4 consecutive patients [14] | TVEC/OVT | (n = 4) | Regionally advanced Merkel cell carcinoma | TVEC | 100% | 16 + | 18.5 + |
| 2 | Pretreated anti-PD-1 refractory Merkel cell carcinoma successfully treated with the combination of PD-1/PD-L1 axis inhibitors and TVEC: a report of two cases [15] | TVEC/OVT | (n = 2) | Anti-PD-1 refractory Merkel cell Carcinoma | T-VEC and a PD-1/PD-L1 inhibitor | 100% | N/A | N/A |
| 3 | Immunotherapy for Nonmelanoma skin cancer: Facts and Hopes (NCT02819843) [16] | TVEC/OVT | Phase II (n = 19) | Cutaneous Melanoma Merkel Cell Carcinoma Other Solid Tumors | TVEC + Radiotherapy | Study completion June 2023 | Study completion June 2023 | Study completion June 2023 |
| Reference | Study Drugs/Mechanisms of Action | Stage (n) | Disease | Treatment | Key Outcomes | |
|---|---|---|---|---|---|---|
| 1 | Talimogene Laherparepvec and Pembrolizumab in Treating Patients With Stage III-IV Melanoma (NCT02965716) | TVEC/OVT Pembrolizumab/PD-1 inhibitor | Phase II (n = 47) | Advanced Melanoma Refractory Melanoma | Pembrolizumab and TVEC combination | Objective response rate, median progression-free survival, median overall survival |
| 2 | T-VEC in Non-melanoma Skin Cancer (NCT03458117) | TVEC/OVT | Phase I (n = 26) | Non-melanoma Skin Cancer Basal Cell Carcinoma Squamous Cell Carcinoma Cutaneous Lymphoma Merkel Cell Carcinoma | TVEC | Local immune response, systemic immune response |
| 3 | Talimogene Laherparepvec and Nivolumab in Treating Patients with Refractory Lymphomas or Advanced or Refractory Non-melanoma Skin Cancers (NCT02978625) | TVEC/OVT Nivolumab/PD-1 inhibitor | Phase II (n = 68) | Refractory T cell Lymphoma Refractory NK cell lymphoma Cutaneous Squamous Cell Carcinoma Merkel Cell Carcinoma Other Rare Skin Tumors | TVEC followed by nivolumab and TVEC combination | Response rate, best overall response rate, progression-free survival, overall survival |
| 4 | Study of TVEC in Patients With Cutaneous Squamous Cell Cancer (NCT03714828) | TVEC/OVT | Phase II (n = 11) | Cutaneous Squamous Cell Cancer | TVEC | Overall response rate (ultrasound, targeted lesions, non-injected lesions) |
| 5 | Talimogene Laherparepvec and Panitumumab for the Treatment of Locally Advanced or Metastatic Squamous Cell Carcinoma of the Skin (NCT04163952) | TVEC/OVT Panitumumab/Anti-EGFT monoclonal antibodies | Phase I (n = 5) | Advanced Squamous Cell Cancer | Panitumumab and TVEC combination | Response rate, best overall response rate, progression-free survival, overall survival |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, T.; Jou, T.H.-T.; Hsin, J.; Wang, Z.; Huang, K.; Ye, J.; Yin, H.; Xing, Y. Talimogene Laherparepvec (T-VEC): A Review of the Recent Advances in Cancer Therapy. J. Clin. Med. 2023, 12, 1098. https://doi.org/10.3390/jcm12031098
Zhang T, Jou TH-T, Hsin J, Wang Z, Huang K, Ye J, Yin H, Xing Y. Talimogene Laherparepvec (T-VEC): A Review of the Recent Advances in Cancer Therapy. Journal of Clinical Medicine. 2023; 12(3):1098. https://doi.org/10.3390/jcm12031098
Chicago/Turabian StyleZhang, Tiantian, Tony Hong-Ting Jou, Jerline Hsin, Zhe Wang, Kelly Huang, Jian Ye, Holly Yin, and Yan Xing. 2023. "Talimogene Laherparepvec (T-VEC): A Review of the Recent Advances in Cancer Therapy" Journal of Clinical Medicine 12, no. 3: 1098. https://doi.org/10.3390/jcm12031098
APA StyleZhang, T., Jou, T. H. -T., Hsin, J., Wang, Z., Huang, K., Ye, J., Yin, H., & Xing, Y. (2023). Talimogene Laherparepvec (T-VEC): A Review of the Recent Advances in Cancer Therapy. Journal of Clinical Medicine, 12(3), 1098. https://doi.org/10.3390/jcm12031098