
A 14-Day Therapeutic Exercise Telerehabilitation Protocol of Physiotherapy Is Effective in Non-Hospitalized Post-COVID-19 Conditions: A Randomized Controlled Trial

 ,
,  , ,
, ,
Abstract
:1. Introduction
- Does a therapeutic exercise telerehabilitation protocol based on strength and respiratory exercises produce benefits for people with post-COVID-19 conditions?
2. Materials and Methods
2.1. Design
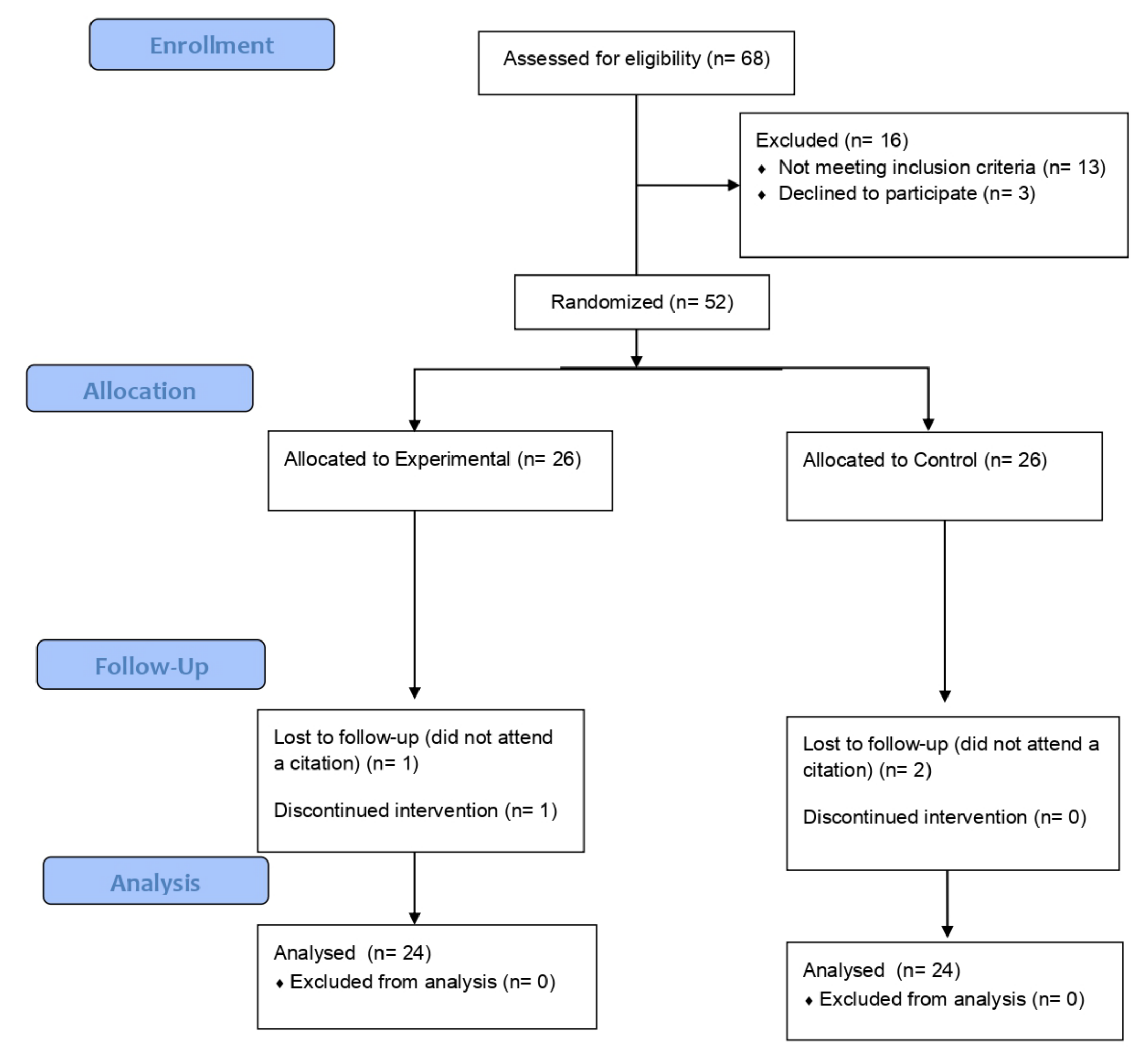
2.2. Participants and setting
2.3. Outcome Measures
- A.
- Visual Analog Fatigue Scale (VAFS). This is a self-report scale measured from 0 to 10, and it is a valid and reliable instrument for the quantitative assessment of fatigue [16], where a higher score indicates a worse score, although there are no minimal clinically significant differences for patients with respiratory pathologies for VASF. Participants could download the form at the following address: https://www.fisiosurid.com/wp-content/uploads/2020/11/ESCALA-VISUAL-ANALOGICA-FATIGA.pdf: accessed on 1 April 2021. The evaluators, via video call, asked the patients what the VASF value they considered adequate was, on day 1 and day 14.
- B.
- Six-Minute Walk Test (6MWT). It consists of recording the number of steps through the “StepsApp”, using the patient’s smartphone, and performing the following procedure: The evaluators asked the participants to walk as far as possible at home without generating 180° changes of direction, minimizing variability in the distribution of dwellings. The evaluators received the data recorded by the participants after performing the test, which can correctly determine the functional status [17]. The minimal clinically significant difference represents 54 m, or 75 steps [18]. A higher score indicates a better result on the test.
- C.
- Thirty-Second Sit-to-Stand Test (30STST). The following procedure was carried out to standardize the test: The evaluators asked the participants to place a chair without arms with a straight back and a hard seat, stabilizing it against a wall (height from the floor to the seat would be between 45 and 50 cm). Seated participants were asked to keep their feet flat on the floor and keep their arms across their chest without moving them during all trials. They would then stand up fully and sit down once without using their arms. Participants will start the test sitting in a chair and, when instructed through the online application, will get up and then sit back down as many times as possible in a 30 s period. This test is a valid tool and is reliable for evaluating the performance of the peripheral muscles of the lower limbs [19]. The participants performed the test, and the evaluator counted the number of repetitions and the minimum clinically significant difference [20]. A higher score indicates a better result on the test.
- D.
- Multidimensional Dyspnea-12 (MD12). We have applied this test, in its validated Spanish version, since it is a valid and reliable instrument to study the multidimensional character of dyspnea [21], with a minimum clinically significant difference of 2.83 points [22]. A higher score indicates a worse result on the test. Participants could download the form at the following address: https://www.fisiosurid.com/wp-content/uploads/2023/01/CUESTIONARIO-DISNEA-12.pdf: accessed on 1 April 2021. The evaluators, via video call, asked the participants to answer the questions on the scale, on day 1 and day 14.
- E.
- The modified Borg Scale of perceived effort (BS) [23]. This scale provides the criteria to adjust to the intensity of the exercise, that is, to the workload, and thus anticipate and dictate the different powers of activity in sports and medical rehabilitation. It measures the entire range of activities that the individual perceives when performing exercise, with a minimum clinically significant difference of 0.9 points [24]. A higher score indicates a worse result on the test. Participants could download the form at the following address: https://www.fisiosurid.com/wp-content/uploads/2020/11/ESCALA-BORG.pdf: accessed on 1 April 2021. The evaluators, via video call, asked the patients what the Borg Scale value they considered adequate was, on day 1 and day 14.
- The VAFS was assessed to determine the patient’s level of fatigue.
- The participants performed the 6MWT test and the 30STST test.
- The dyspnea and effort perceived were assessed by means of the MD12 and the BS, respectively.
2.4. Interventions
2.5. Sample Size Calculation
2.6. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Romano, C.; Chebabo, A.; Levi, J. Past, present, and future of COVID-19: A review. Braz. J. Med Biol. Res. 2020, 53, e10475. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO COVID-19 Dashboard. Available online: https://covid19.who.int/ (accessed on 3 December 2021).
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef] [PubMed]
- Borg, K.; Stam, H. COVID-19 and physical and rehabilitation medicine. J. Rehabil. Med. 2020, 52, jrm00045. [Google Scholar] [CrossRef] [PubMed]
- Scheiber, B.; Spiegl, C.; Wiederin, C.; Schifferegger, E.; Schiefermeier-Mach, N. Post-COVID-19 Rehabilitation: Perception and Experience of Austrian Physiotherapists and Physiotherapy Students. Int. J. Environ. Res. Public Health 2021, 18, 8730. [Google Scholar] [CrossRef] [PubMed]
- Jimeno-Almazán, A.; Pallarés, J.; Buendía-Romero, Á.; Martínez-Cava, A.; Franco-López, F.; Martínez, B.S.-A.; Bernal-Morel, E.; Courel-Ibáñez, J. Post-COVID-19 Syndrome and the Potential Benefits of Exercise. Int. J. Environ. Res. Public Health 2021, 18, 5329. [Google Scholar] [CrossRef]
- Thomas, P.; Baldwin, C.; Bissett, B.; Boden, I.; Gosselink, R.; Granger, C.L.; Hodgson, C.; Jones, A.Y.; E Kho, M.; Moses, R.; et al. Physiotherapy management for COVID-19 in the acute hospital setting: Clinical practice recommendations. J. Physiother. 2020, 66, 73–82. [Google Scholar] [CrossRef]
- Yong, S.J. Long COVID or post-COVID-19 syndrome: Putative pathophysiology, risk factors, and treatments. Infect. Dis. 2021, 53, 737–754. [Google Scholar] [CrossRef]
- Rigonato-Oliveira, N.C.; MacKenzie, B.; Bachi, A.; Oliveira-Junior, M.C.; Santos-Dias, A.; Brandao-Rangel, M.A.R.; Dellê, H.; Costa-Guimaraes, T.; Damaceno-Rodrigues, N.R.; Dulley, N.R.; et al. Aerobic exercise inhibits acute lung injury: From mouse to human evidence Exercise reduced lung injury markers in mouse and in cells. Exerc. Immunol. Rev. 2018, 24, 36–44. [Google Scholar]
- Mohamed, A.A.; Alawna, M. Role of increasing the aerobic capacity on improving the function of immune and respiratory systems in patients with coronavirus (COVID-19): A review. Diabetes Metab. Syndr. 2020, 14, 489–496. [Google Scholar] [CrossRef]
- Liu, K.; Zhang, W.; Yang, Y.; Zhang, J.; Li, Y.; Chen, Y. Respiratory rehabilitation in elderly patients with COVID-19: A randomized controlled study. Complement. Ther. Clin. Pract. 2020, 39, 101166. [Google Scholar] [CrossRef]
- Salawu, A.; Green, A.; Crooks, M.G.; Brixey, N.; Ross, D.H.; Sivan, M. A Proposal for Multidisciplinary Tele-Rehabilitation in the Assessment and Rehabilitation of COVID-19 Survivors. Int. J. Environ. Res. Public Health 2020, 17, 4890. [Google Scholar] [CrossRef]
- Rodríguez-Blanco, C.; Bernal-Utrera, C.; Anarte-Lazo, E.; Saavedra-Hernandez, M.; De-La-Barrera-Aranda, E.; Serrera-Figallo, M.A.; Gonzalez-Martin, M.; Gonzalez-Gerez, J.J. Breathing exercises versus strength exercises through telerehabilitation in coronavirus disease 2019 patients in the acute phase: A randomized controlled trial. Clin. Rehabilitation 2021, 36, 486–497. [Google Scholar] [CrossRef]
- Gonzalez-Gerez, J.; Saavedra-Hernandez, M.; Anarte-Lazo, E.; Bernal-Utrera, C.; Perez-Ale, M.; Rodriguez-Blanco, C. Short-Term Effects of a Respiratory Telerehabilitation Program in Confined COVID-19 Patients in the Acute Phase: A Pilot Study. Int. J. Environ. Res. Public Health 2021, 18, 7511. [Google Scholar] [CrossRef]
- Bernal-Utrera, C.; Anarte-Lazo, E.; De-La-Barrera-Aranda, E.; Fernandez-Bueno, L.; Saavedra-Hernandez, M.; Gonzalez-Gerez, J.; Serrera-Figallo, M.; Rodriguez-Blanco, C. Perspectives and Attitudes of Patients with COVID-19 toward a Telerehabilitation Programme: A Qualitative Study. Int. J. Environ. Res. Public Health 2021, 18, 7845. [Google Scholar] [CrossRef]
- Lee, K.A.; Hicks, G. Nino-Murcia G. Validity and reliability of a scale to assess fatigue. Psychiatry Res. 1991, 36, 291–298. [Google Scholar] [CrossRef]
- Ozalevli, S.; Ozden, A.; Itil, O.; Akkoclu, A. Comparison of the sit-to-stand test with 6 min walk test in patients with chronic obstructive pulmonary disease. Respir. Med. 2007, 101, 286–293. [Google Scholar] [CrossRef] [Green Version]
- Wise, R.A.; Brown, C.D. In the six-minute walk test and the test. COPD 2005, 2, 125–129. [Google Scholar] [CrossRef]
- Zanini, A.; Aiello, M.; Cherubino, F.; Zampogna, E.; Chetta, A.; Azzola, A.; Spanevello, A. The one repetition maximum test and the sit-to-stand test in the assessment of a specific pulmonary rehabilitation program on peripheral muscle strength in COPD patients. Int. J. Chronic Obstr. Pulm. Dis. 2015, 10, 2423–2430. [Google Scholar] [CrossRef] [Green Version]
- Zanini, A.; Crisafulli, E.; D’Andria, M.; Gregorini, C.; Cherubino, F.; Zampogna, E.; Azzola, A.; Spanevello, A.; Schiavone, N.; Chetta, A. Minimum Clinically Important Difference in 30-s Sit-to-Stand Test after Pulmonary Rehabilitation in Subjects With COPD. Respir. Care 2019, 64, 1261–1269. [Google Scholar] [CrossRef]
- Amado Diago, C.A.; Puente Maestu, L.; Abascal Bolado, B.; Agüero Calvo, J.; Hernando Hernando, M.; Puente Bats, I.; Agüero Balbín, R. Translation and Validation of the Multidimensional Dyspnea-12 Questionnaire. Arch. Bronconeumol. 2018, 54, 74–78, (In English and Spanish). [Google Scholar] [CrossRef]
- Ekström, M.P.; Bornefalk, H.; Sköld, C.M.; Janson, C.; Blomberg, A.; Bornefalk-Hermansson, A.; Igelström, H.; Sandberg, J.; Sundh, J. Minimal Clinically Important Differences and Feasibility of Dyspnea-12 and the Multidimensional Dyspnea Profile in Cardiorespiratory Disease. J. Pain Symptom Manag. 2020, 60, 968–975.e1. [Google Scholar] [CrossRef] [PubMed]
- Williams, N. The Borg Rating of Perceived Exertion (RPE) scale. Occup. Med. 2017, 67, 404–405. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, A.; Machado, A.; Marques, A. Minimal Important and Detectable Differences of Respiratory Measures in Outpatients with AECOPD†. COPD J. Chronic Obstr. Pulm. Dis. 2018, 15, 479–488. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Blanco, C.; Gonzalez-Gerez, J.; Bernal-Utrera, C.; Anarte-Lazo, E.; Perez-Ale, M.; Saavedra-Hernandez, M. Short-Term Effects of a Conditioning Telerehabilitation Program in Confined Patients Affected by COVID-19 in the Acute Phase. A Pilot Randomized Controlled Trial. Medicina 2021, 57, 684. [Google Scholar] [CrossRef]
- UK Office for National Statistics. Prevalence of Ongoing Symptoms Following Coronavirus (COVID-19) Infection in the UK: 1 April 2021; ONS: London, UK, 2021. [Google Scholar]
- Colas, C.; Bayle, M.; Labeix, P.; Botelho-Nevers, E.; Gagneux-Brunon, A.; Cazorla, C.; Schein, F.; Breugnon, E.; Garcin, A.; Feasson, L.; et al. Management of Long COVID—The CoviMouv’ Pilot Study: Importance of Adapted Physical Activity for Prolonged Symptoms Following SARS-CoV2 Infection. Front. Sports Act. Living 2022, 4, 877188. [Google Scholar] [CrossRef]
- Calvo-Paniagua, J.; Díaz-Arribas, M.J.; Valera-Calero, J.A.; Gallardo-Vidal, M.I.; Fernández-De-Las-Peñas, C.; López-De-Uralde-Villanueva, I.; del Corral, T.; Plaza-Manzano, G. A tele-health primary care rehabilitation program improves self-perceived exertion in COVID-19 survivors experiencing Post-COVID fatigue and dyspnea: A quasi-experimental study. PLoS ONE 2022, 17, e0271802. [Google Scholar] [CrossRef]
- Estebanez-Pérez, M.-J.; Pastora-Bernal, J.-M.; Martín-Valero, R. The Effectiveness of a Four-Week Digital Physiotherapy Intervention to Improve Functional Capacity and Adherence to Intervention in Patients with Long COVID-19. Int. J. Environ. Res. Public Health 2022, 19, 9566. [Google Scholar] [CrossRef]
- Cox, N.S.; Corso, S.D.; Hansen, H.; McDonald, C.F.; Hill, C.J.; Zanaboni, P.; A Alison, J.; O’Halloran, P.; Macdonald, H.; E Holland, A. Telerehabilitation for chronic respiratory disease. Cochrane Database Syst. Rev. 2021, 2021, CD013040. [Google Scholar] [CrossRef]
- Cavalheiro, A.H.; Cardoso, J.S.; Rocha, A.; Moreira, E.; Azevedo, L.F. Effectiveness of Tele-rehabilitation Programs in Heart Failure: A Systematic Review and Meta-analysis. Health Serv. Insights 2021, 14, 11786329211021668. [Google Scholar] [CrossRef]
- Fiuza-Luces, C.; Garatachea, N.; Berger, N.A.; Lucia, A. Exercise is the Real Polypill. Physiology 2013, 28, 330–358. [Google Scholar] [CrossRef] [Green Version]
- Lopez Bernal, J.; Andrews, N.; Gower, C.; Gallagher, E.; Simmons, R.; Thelwall, S.; Stowe, J.; Tessier, E.; Groves, N.; Dabrera, G.; et al. Effectiveness of COVID-19 Vaccines against the B.1.617.2 (Delta) Variant. N. Engl. J. Med. 2021, 385, 585–594. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| EG (n = 24) | CG (n = 24) | |||||
|---|---|---|---|---|---|---|
| PRE | POST | DIF | PRE | POST | DIF | |
| Age | 38.75 (15.40) [32.24 to 45.26] | 42.58 (11.40) [37.77 to 47.40] | ||||
| Gender | ♂ 11 (22.91) ♀ 13 (27.08) | ♂ 11 (22.91) ♀ 13 (27.08) | ||||
| Height | 166.46 (7.97) [163.09 to 169.82] | 165.83 (9.27) [161.91 to 169.74] | ||||
| Weight | 73.53 (18.33) [65.79 to 81.27] | 79.77 (20.99) [70.90 to 88.62] | ||||
| BMI | 25.66 (1.78) [24.91 to 26.41] | 25.74 (1.77) [24.99 to 26.49] | ||||
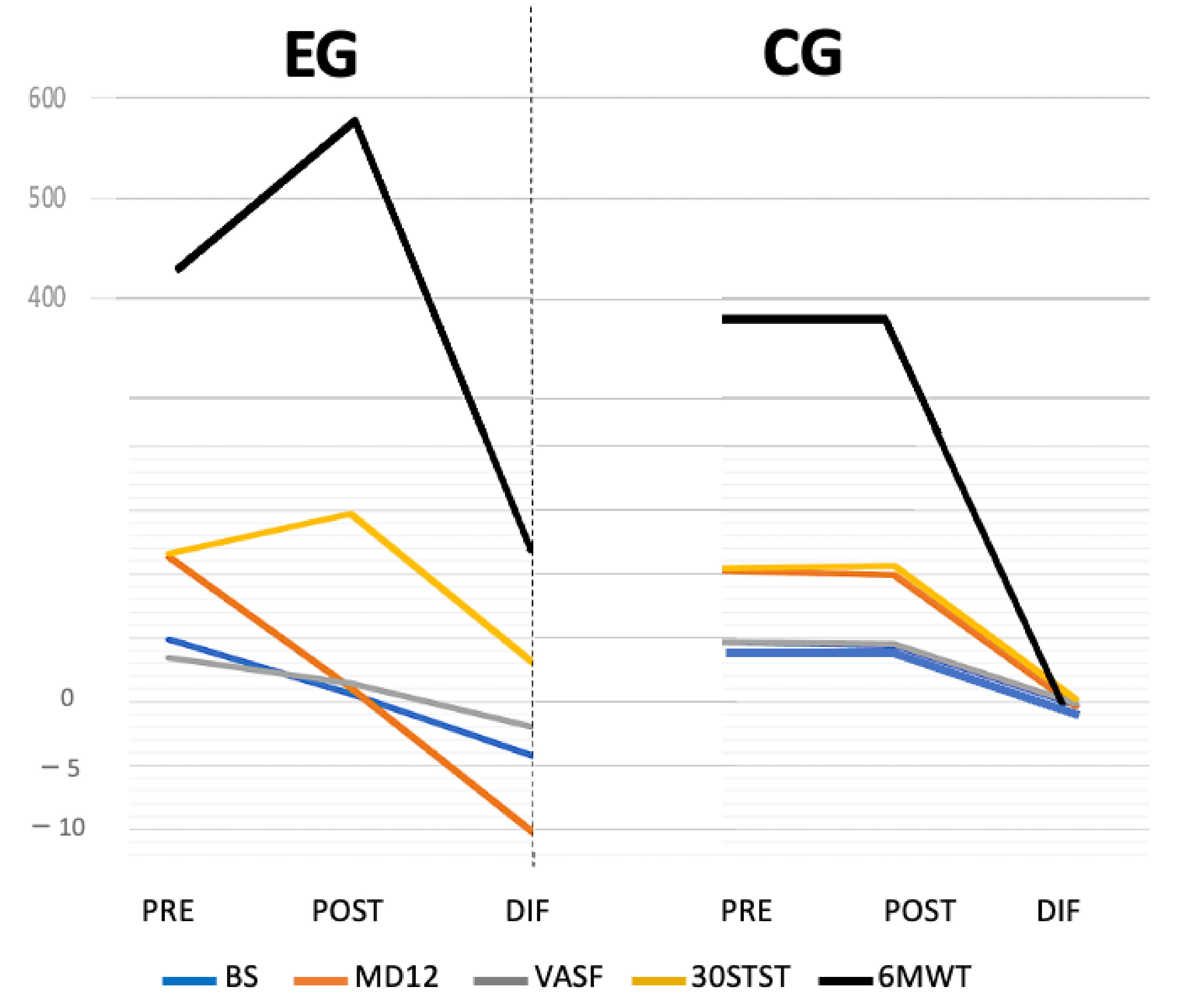
| BS | 4.87 (2.11) [3.98 to 5.77] | 0.62 (0.65) [0.35 to 0.90] | −4.25 (1.85) [−5.03 to −3.46] | 4.67 (1.95) [3.84 to 5.49] | 4.42 (1.84) [3.64 to 5.19] | –0.25 (0.53) [−0.47 to −0.02] |
| MD12 | 11.29 (7.54) [8.11 to 14.48] | 1.08 (1.53) [0.44 to 1.73] | −10.21 (6.66) [−13.01 to −7.40] | 10.29 (6.82) [7.41 to 13.17] | 9.92 (6.59) [7.13 to 12.70] | −0.37 (0.65) [−0.64 to −0.10] |
| VAFS | 3.42 (2.57) [2.33 to 4.50] | 1.42 (1.84) [0.64 to 2.19] | −2.00 (2.28) [−2.96 to −1.03] | 4.67 (2.26) [3.71 to 5.62] | 4.50 (2.15) [3.59 to 5.41] | −0.17 (0.70) [−0.46 to 0.12] |
| 6MWT | 429.63 (192.50) [348.34 to 510.91] | 577.54 (153.04) [512.92 to 642.16] | 147.92 (165.57) [78.00 to 217.83] | 379.46 (131.28) [324.02 to 434.89] | 379.08 (131.37) [323.61 to 434.56] | −0.37 (10.67) [−4.88 to 4.13] |
| 30STST | 11.63 (2.39) [10.61 to 12.64] | 14.71 (4.24) [12.92 to 16.50] | 3.08 (2.80) [1.90 to 4.26] | 10.42 (2.48) [9.37 to 11.47 ] | 10.63 (2.70) [9.49 to 11.76] | 0.21 (1.22) [−0.30 to 0.72] |
| DIF | DIF | |
|---|---|---|
| EG (n = 24) | CG (n = 24) | |
| BS | p < 0.001 | p > 0.05 |
| R2 0.693 | ||
| MD12 | p < 0.001 | p > 0.05 |
| R2 0.531 | ||
| VAFS | p < 0.001 | p > 0.05 |
| R2 0.235 | ||
| 6MWT | p < 0.001 | p > 0.05 |
| R2 0.294 | ||
| 30STST | p < 0.001 | p > 0.05 |
| R2 0.317 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodriguez-Blanco, C.; Bernal-Utrera, C.; Anarte-Lazo, E.; Gonzalez-Gerez, J.J.; Saavedra-Hernandez, M. A 14-Day Therapeutic Exercise Telerehabilitation Protocol of Physiotherapy Is Effective in Non-Hospitalized Post-COVID-19 Conditions: A Randomized Controlled Trial. J. Clin. Med. 2023, 12, 776. https://doi.org/10.3390/jcm12030776
Rodriguez-Blanco C, Bernal-Utrera C, Anarte-Lazo E, Gonzalez-Gerez JJ, Saavedra-Hernandez M. A 14-Day Therapeutic Exercise Telerehabilitation Protocol of Physiotherapy Is Effective in Non-Hospitalized Post-COVID-19 Conditions: A Randomized Controlled Trial. Journal of Clinical Medicine. 2023; 12(3):776. https://doi.org/10.3390/jcm12030776
Chicago/Turabian StyleRodriguez-Blanco, Cleofas, Carlos Bernal-Utrera, Ernesto Anarte-Lazo, Juan Jose Gonzalez-Gerez, and Manuel Saavedra-Hernandez. 2023. "A 14-Day Therapeutic Exercise Telerehabilitation Protocol of Physiotherapy Is Effective in Non-Hospitalized Post-COVID-19 Conditions: A Randomized Controlled Trial" Journal of Clinical Medicine 12, no. 3: 776. https://doi.org/10.3390/jcm12030776
APA StyleRodriguez-Blanco, C., Bernal-Utrera, C., Anarte-Lazo, E., Gonzalez-Gerez, J. J., & Saavedra-Hernandez, M. (2023). A 14-Day Therapeutic Exercise Telerehabilitation Protocol of Physiotherapy Is Effective in Non-Hospitalized Post-COVID-19 Conditions: A Randomized Controlled Trial. Journal of Clinical Medicine, 12(3), 776. https://doi.org/10.3390/jcm12030776