
Biomarkers and Predictive Factors for Treatment Response to Tumor Necrosis Factor-α Inhibitors in Patients with Psoriasis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Statistical Analysis
3. Results
3.1. Background Factors of the Patients
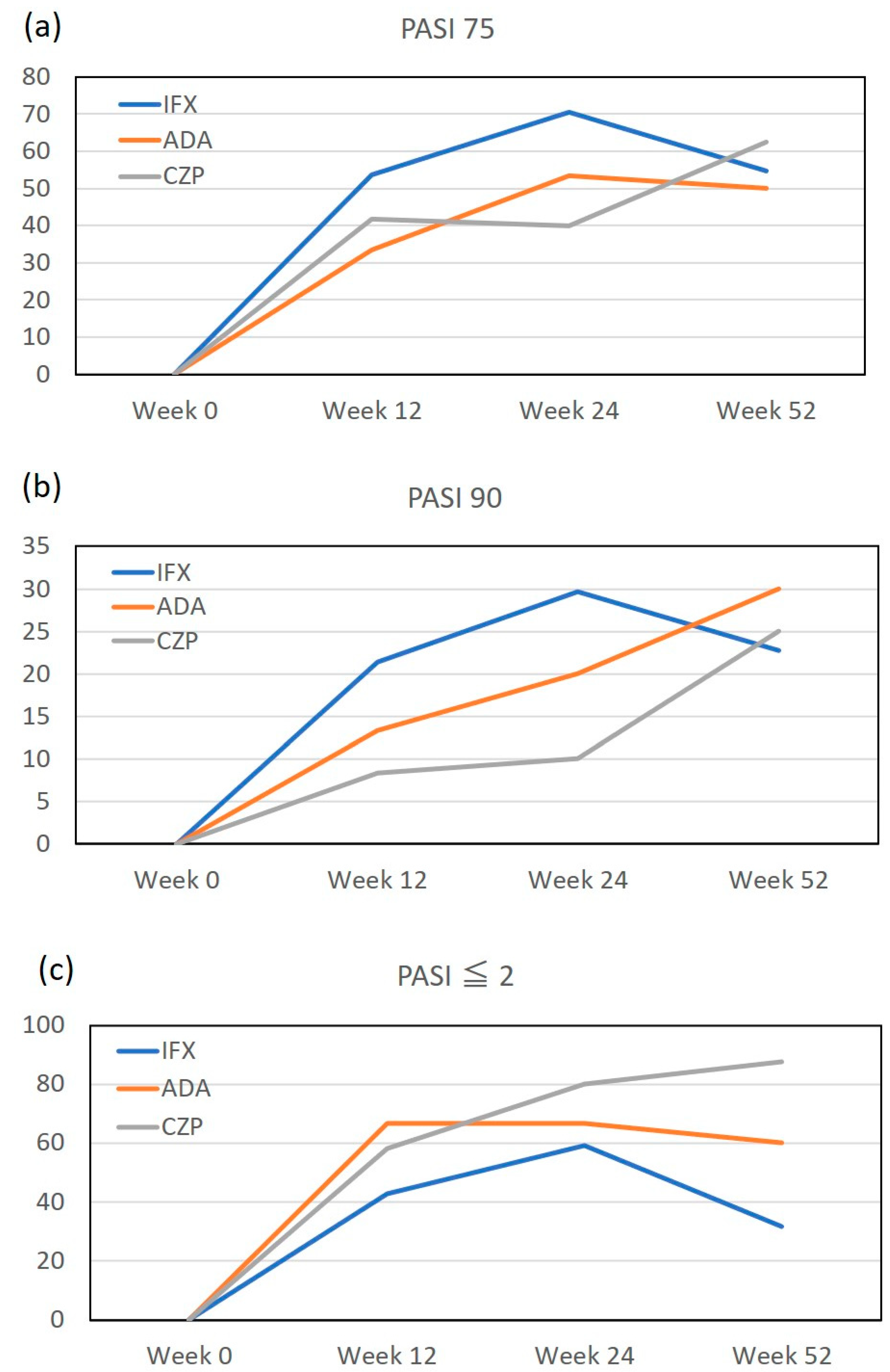
3.2. The Achievement Rate of PASI 75, PASI 90 and Absolute PASI ≤ 2 during the Treatment with TNF-α Inhibitors
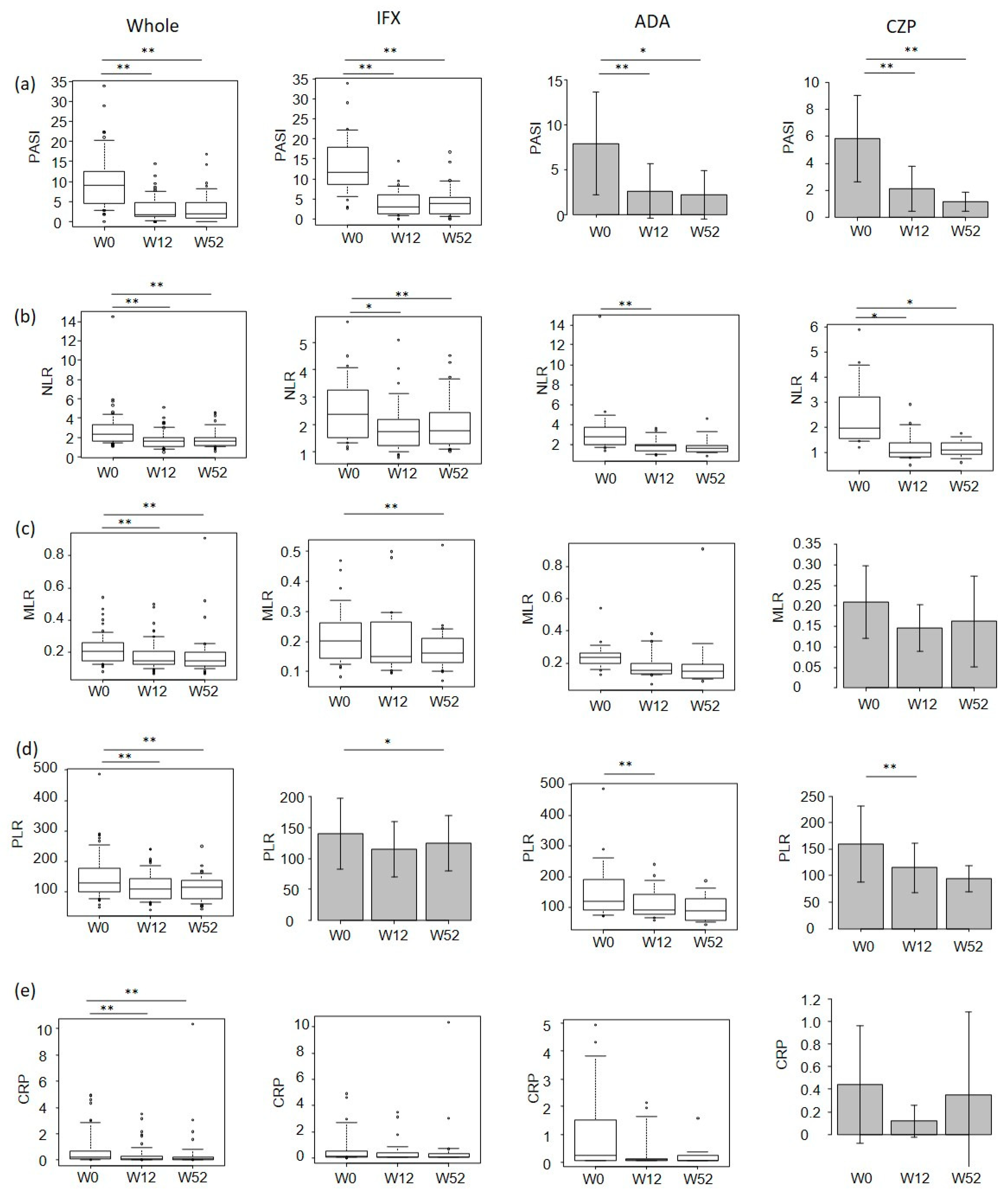
3.3. The Transition of PASI, NLR, MLR, PLR and CRP Values during the Treatment with TNF-α Inhibitors
3.4. Correlations between Individual Parameters
3.5. Correlations between Percent Reduction of PASI versus Those of NLR, MLR, PLR or CRP
3.6. The Background Factors Predicting Treatment Response to TNF-α Inhibitors in Patients with Psoriasis
4. Discussion
5. Clinical Relevance of This Study
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ten Bergen, L.L.; Petrovic, A.; Krogh Aarebrot, A.; Appel, S. The TNF/IL-23/IL-17 axis-Head-to-head trials comparing different biologics in psoriasis treatment. Scand. J. Immunol. 2020, 92, e12946. [Google Scholar] [CrossRef] [PubMed]
- Najar Nobari, N.; Shahidi Dadras, M.; Nasiri, S.; Abdollahimajd, F.; Gheisari, M. Neutrophil/platelet to lymphocyte ratio in monitoring of response to TNF-α inhibitors in psoriatic patients. Dermatol. Ther. 2020, 33, e13457. [Google Scholar] [CrossRef] [PubMed]
- Sen, B.B.; Rifaioglu, E.N.; Ekiz, O.; Inan, M.U.; Sen, T.; Sen, N. Neutrophil to lymphocyte ratio as a measure of systemic inflammation in psoriasis. Cutan. Ocul. Toxicol. 2014, 33, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Beygi, S.; Lajevardi, V.; Abedini, R. C-reactive protein in psoriasis: A review of the literature. J. Eur. Acad. Dermatol. Venereol. 2014, 28, 700–711. [Google Scholar] [CrossRef]
- Kim, D.S.; Shin, D.; Lee, M.S.; Kim, H.J.; Kim, D.Y.; Kim, S.M. Assessments of neutrophil to lymphocyte ratio and platelet to lymphocyte ratio in Korean patients with psoriasis vulgaris and psoriatic arthritis. J. Dermatol. 2016, 43, 305–310. [Google Scholar] [CrossRef]
- Lee, H.N.; Kim, Y.K.; Kim, G.T.; Ahn, E.; So, M.W.; Sohn, D.H. Neutrophil-to-lymphocyte and platelet-to-lymphocyte ratio as predictors of 12-week treatment response and drug persistence of anti-tumor necrosis factor-α agents in patients with rheumatoid arthritis: A retrospective chart review analysis. Rheumatol. Int. 2019, 39, 859–868. [Google Scholar] [CrossRef]
- Ataseven, A.; Bilgin, A.U.; Kurtipek, G.S. The importance of neutrophil lymphocyte ratio in patients with psoriasis. Mater. Sociomed. 2014, 26, 231–233. [Google Scholar] [CrossRef] [Green Version]
- Asahina, A.; Kubo, N.; Umezawa, Y.; Honda, H.; Yanaba, K.; Nakagawa, H. Neutrophil-lymphocyte ratio, platelet-lymphocyte ratio and mean platelet volume in Japanese patients with psoriasis and psoriatic arthritis: Response to therapy with biologics. J. Dermatol. 2017, 44, 1112–1121. [Google Scholar] [CrossRef]
- Asahina, A.; Umezawa, Y.; Yanaba, K.; Nakagawa, H. Serum C-reactive protein levels in Japanese patients with psoriasis and psoriatic arthritis: Long-term differential effects of biologics. J. Dermatol. 2016, 43, 779–784. [Google Scholar] [CrossRef] [Green Version]
- Annen, S.; Horiguchi, G.; Teramukai, S.; Ichiyama, S.; Ito, M.; Hoashi, T.; Kanda, N.; Saeki, H. Association study of transition of laboratory markers and transition of disease activity in psoriasis patients treated with biologics. J. Nippon Med. Sch. 2022, 89, 587–593. [Google Scholar]
- Biomarkers Definitions Working Group. Biomarkers and surrogate endpoints: Preferred definitions and conceptual framework. Clin. Pharmacol. Ther. 2001, 69, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Palframan, R.; Airey, M.; Moore, A.; Vugler, A.; Nesbitt, A. Use of biofluorescence imaging to compare the distribution of certolizumab pegol, adalimumab and infliximab in the inflamed paws of mice with collagen-induced arthritis. J. Immunol. Methods 2009, 348, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Lambert, B.; Carron, P.; D’Asseler, Y.; Bacher, K.; Van den Bosch, F.; Elewaut, D. (99m)Tc-labelled S-HYNIC certolizumab pegol in rheumatoid arthritis and spondyloarthritis patients: A biodistribution and dosimetry study. EJNMMI Res. 2016, 6, 88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aktaş Karabay, E.; Aksu Çerman, A.; Demir, D.; Kıvanç Altunay, I. The Effects of Systemic Psoriasis Therapies on the C-Reactive Protein and the Neutrophil-Lymphocyte Ratio. Ann. Dermatol. 2019, 31, 601–610. [Google Scholar] [CrossRef]
- Castro, A.R.; Silva, S.O.; Soares, S.C. The Use of High Sensitivity C-Reactive Protein in Cardiovascular Disease Detection. J. Pharm. Pharm. Sci. 2018, 21, 496–503. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Franco, R.S.; Wang, Y.; Pan, H.Q.; Eaton, D.; Cheng, T. Megakaryocytic differentiation of HIMeg-1 cells induced by interferon gamma and tumour necrosis factor alpha but not by thrombopoietin. Cytokine 1998, 10, 880–889. [Google Scholar] [CrossRef]
- Norlin, J.M.; Nilsson, K.; Persson, U.; Schmitt-Egenolf, M. Complete skin clearance and Psoriasis Area and Severity Index response rates in clinical practice: Predictors, health-related quality of life improvements and implications for treatment goals. Br. J. Dermatol. 2020, 182, 965–973. [Google Scholar] [CrossRef]
- Gooderham, M.J.; Lynde, C.; Turchin, I.; Avadisian, M.; Labelle, M.; Papp, K.A. Real-world, long-term treatment patterns of commonly used biologics in Canadian patients with moderate-to-severe chronic plaque psoriasis. J. Dermatol. 2022, 49, 95–105. [Google Scholar] [CrossRef]
- Lanna, C.; Zangrilli, A.; Bavetta, M.; Campione, E.; Bianchi, L. Efficacy and safety of adalimumab in difficult-to-treat psoriasis. Dermatol. Ther. 2020, 33, e13374. [Google Scholar] [CrossRef]
- Papadimitriou, I.; Bakirtzi, K.; Katoulis, A.; Ioannides, D. Scalp Psoriasis and Biologic Agents: A Review. Ski. Appendage Disord. 2021, 7, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Sola-Ortigosa, J.; Sánchez-Regaña, M.; Umbert-Millet, P. Efficacy of adalimumab in the treatment of psoriasis: A retrospective study of 15 patients in daily practice. J. Dermatolog. Treat. 2012, 23, 203–207. [Google Scholar] [CrossRef] [PubMed]
- Zangrilli, A.; Caldarola, G.; Bernardini, N.; Bavetta, M.; Graceffa, D.; Bonifati, C. Predictive factors of lack of response to adalimumab among bio-naive patients suffering from moderate-to severe psoriasis: Analysis of a multicenter data collection in Italy. Expert Opin. Biol. Ther. 2021, 21, 1291–1298. [Google Scholar] [CrossRef] [PubMed]
- Khosravi, H.; Siegel, M.P.; Van Voorhees, A.S.; Merola, J.F. Treatment of Inverse/Intertriginous Psoriasis: Updated Guidelines from the Medical Board of the National Psoriasis Foundation. J. Drugs Dermatol. 2017, 16, 760–766. [Google Scholar]
- Azab, B.; Camacho-Rivera, M.; Taioli, E. Average values and racial differences of neutrophil lymphocyte ratio among a nationally representative sample of United States subjects. PLoS ONE 2014, 9, e112361. [Google Scholar] [CrossRef] [Green Version]
- Kaya, T.; Açıkgöz, S.B.; Yıldırım, M.; Nalbant, A.; Altaş, A.E.; Cinemre, H. Association between neutrophil-to-lymphocyte ratio and nutritional status in geriatric patients. J. Clin. Lab. Anal. 2019, 33, e22636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barker, T.; Fulde, G.; Moulton, B.; Nadauld, L.D.; Rhodes, T. An elevated neutrophil-to-lymphocyte ratio associates with weight loss and cachexia in cancer. Sci. Rep. 2020, 10, 7535. [Google Scholar] [CrossRef]
- Lee, J.S.; Kim, N.Y.; Na, S.H.; Youn, Y.H.; Shin, C.S. Reference values of neutrophil-lymphocyte ratio, lymphocyte-monocyte ratio, platelet-lymphocyte ratio and mean platelet volume in healthy adults in South Korea. Medicine 2018, 97, e11138. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Biologic (n) | Whole TNF-α Inhibitors (55) | IFX (28) | ADA (15) | CZP (12) | IFX vs. ADA | IFX vs. CZP | ADA vs. CZP |
|---|---|---|---|---|---|---|---|
| Sex, n (%) † | |||||||
| Male | 43 (78.2) | 22 (78.6) | 12 (80.0) | 9 (75.0) | 1 | 1 | 1 |
| Female | 12 (21.8) | 6(21.4) | 3 (20.0) | 3 (25.0) | 1 | 1 | 1 |
| Age (years) ‡ | 55.33 ± 13.34 | 56.96 ± 13.91 | 53.8 ± 13.79 | 53.42 ± 11.95 | 1 | 1 | 1 |
| Body mass index (kg/m2) ‡ | 24.71 ± 4.21 | 25.48 ± 4.36 | 22.97 ± 3.67 | 24.96 ± 4.18 | 0.21 | 1 | 0.69 |
| Disease duration (years) § | 16 [8–27] | 16.5 [10–27.8] | 18.4 ± 9.3 | 6 [4–26.5] | 1 | 0.4 | 0.81 |
| Positive bio-switch, n (%) † | 16 (29.1) | 1 (3.6) | 10 (66.7) | 5 (41.7) | 0.000045 ** | 0.018 * | 0.773 |
| Presence of arthritis n (%) † | 38 (69.1) | 15 (53.6) | 11(45.8) | 12 (100) | 0.982 | 0.011 * | 0.318 |
| Presence of scalp lesions, n (%) † | 41 (74.6) | 20 (71.4) | 11(45.8) | 10 (83.3) | 1 | 1 | 1 |
| Presence of nail lesions, n (%) † | 30 (54.6) | 15 (53.6) | 10 (66.7) | 5 (41.7) | 1 | 1 | 0.77 |
| Presence of genital lesions, n (%) † | 17 (30.9) | 8 (28.6) | 3 (20.0) | 6 (50.0) | 1 | 1 | 0.68 |
| Diabetes mellitus, n (%) † | 8 (14.6) | 3 (3.6) | 4 (26.7) | 1 (8.3) | 0.65 | 1 | 1 |
| Cardiovascular disease, n (%) † | 1 (1.8) | 1 (3.6) | 0 (0) | 0 (0) | 1 | 1 | 1 |
| Current smoking status, ¶ n (%) † | 37 (67.3) | 17 (60.7) | 12 (80) | 8 (66.7) | 0.84 | 1 | 1 |
| Psoriasis area and severity index § | 9 [4.6–12.6] | 11.7 [8.6–16.9] | 7.94 ± 5.72 | 5.83 ± 3.21 | 0.0462 * | 0.0022 ** | 1 |
| Laboratory findings | |||||||
| Neutrophil-to-lymphocyte ratio § | 2.32 [1.61–3.35] | 2.54 ± 1.18 | 2.73 [1.99–3.68] | 1.98 [1.58–2.99] | 0.6 | 1 | 0.65 |
| Monocyte-to-lymphocyte ratio § | 0.21 [0.15–0.26] | 0.20 [0.14–0.26] | 0.23 [0.2–0.26] | 0.21 ± 0.088 | 0.88 | 1 | 0.97 |
| Platelet-to-lymphocyte ratio § | 129.1 [101.6–178.7] | 140.3 ± 50.6 | 119.4 [92.6–190.1] | 159.9 ± 71.5 | 1 | 1 | 1 |
| CRP (mg/dL) § | 0.18 [0.09–0.69] | 0.165 [0.095–0.57] | 0.25 [0.055–1.51] | 0.18 [0.15–0.53] | 1 | 1 | 1 |
| Sex † | Male | Female | p |
| n (%) | 43 (78.2) | 12 (21.8) | |
| NLR | 2.32 [1.58–3.20] | 2.44 [1.72–4.11] | 0.426 |
| MLR | 0.208 [0.155–0.259] | 0.194 [0.125–0.281] | 0.636 |
| PLR | 129.1 [93.0–177.8] | 141.2 [120.6–272.5] | 0.178 |
| CRP (mg/dL) | 0.18 [0.08–0.60] | 0.32 [0.11–0.83] | 0.547 |
| Bio-switch † | Absence | Presence | p |
| n (%) | 39 (70.9) | 16 (29.1) | |
| NLR | 2.32 [1.56–3.24] | 2.76 [1.77–3.78] | 0.29 |
| MLR | 0.196 [0.142–0.257] | 0.239 [0.171–0.283] | 0.0735 |
| PLR | 128.3 [98.4–165.8] | 161.0 [111.4–200.8] | 0.265 |
| CRP (mg/dL) | 0.180 [0.100–0.675] | 0.215 [0.058–0.655] | 0.985 |
| Arthritis † | Absence | Presence | p |
| n (%) | 17 (30.9) | 38 (69.1) | |
| NLR | 2.56 [1.68–3.23] | 2.25 [1.60–3.38] | 0.978 |
| MLR | 0.215 [0.146–0.253] | 0.204 [0.150–0.271] | 0.935 |
| PLR | 128.3 [104.2–155.2] | 132.8 [93.3–185.0] | 0.557 |
| CRP (mg/dL) | 0.22 [0.10–0.62] | 0.18 [0.085–0.713] | 0.708 |
| Scalp lesions † | Absence | Presence | p |
| n (%) ‡ | 13 (23.6) | 41 (74.5) | |
| NLR | 1.968 [1.726–3.299] | 2.537 [1.621–3.407] | 0.795 |
| MLR | 0.167 [0.141–0.196] | 0.222 [0.163–0.273] | 0.0513 |
| PLR | 128.3 [113.7–193.1] | 134.1 [99.0–178.5] | 0.81 |
| CRP (mg/dL) | 0.18 [0.05–0.62] | 0.18 [0.10–0.75] | 0.641 |
| Nail lesions † | Absence | Presence | p |
| n (%) ‡ | 23 (41.8) | 30 (54.5) | |
| NLR | 2.32 [1.67–3.53] | 2.43 [1.64–3.49] | 0.979 |
| MLR | 0.186 [0.144–0.212] | 0.255 [0.158–0.296] | 0.0165 * |
| PLR | 134.1 [106.5–190.1] | 128.7 [92.2–178.2] | 0.587 |
| CRP (mg/dL) | 0.16 [0.075–0.595] | 0.205 [0.11–1.015] | 0.31 |
| Genital lesions † | Absence | Presence | p |
| n (%) ‡ | 31 (56.3) | 17 (25.5) | |
| NLR | 2.32 [1.77–3.06] | 3.08 [1.59–4.34] | 0.494 |
| MLR | 0.215 [0.155–0.268] | 0.186 [0.146–0.256] | 0.782 |
| PLR | 136.5 [106.5–178.7] | 129.1 [113.7–193.1] | 0.881 |
| CRP (mg/dL) | 0.16 [0.055–0.855] | 0.46 [0.11–0.78] | 0.235 |
| Diabetes mellitus † | Absence | Presence | p |
| n (%) | 47 (85.5) | 8 (14.5) | |
| NLR | 2.32 [1.65–3.35] | 2.37 [1.54–3.19] | 0.716 |
| MLR | 0.210 [0.152–0.265] | 0.197 [0.127–0.226] | 0.378 |
| PLR | 137.1 [106.7–182.9] | 110.5 [75.7–134.7] | 0.103 |
| CRP (mg/dL) | 0.18 [0.08–0.685] | 0.135 [0.11–0.585] | 0.729 |
| Cardiovascular disease † | Absence | Presence | p |
| n (%) | 54 (98.2) | 1 (1.8) | |
| NLR | 2.38 [1.64–3.38] | 1.51 | 0.299 |
| MLR | 0.209 [0.150–0.263] | 0.081 | 0.095 |
| PLR | 131.6 [104.3–131.6] | 50.6 | 0.095 |
| CRP (mg/dL) | 0.18 [0.10–0.7175] | 0.08 | 0.344 |
| Current smoking status † | Absence | Presence | p |
| n (%) ‡ | 14 (25.5) | 37 (67.3) | |
| NLR | 2.25 [1.64–2.53] | 2.70 [1.62–3.95] | 0.33 |
| MLR | 0.179 [0.136–0.232] | 0.215 [0.156–0.277] | 0.144 |
| PLR | 127.6 [113.5–183.7] | 134.1 [97.8–178.6] | 0.654 |
| CRP (mg/dL) | 0.12 [0.0575–0.5425] | 0.18 [0.11–0.76] | 0.15 |
| Past tuberculosis † | Absence | Presence | p |
| n (%) | 51 (92.7) | 4 (7.3) | |
| NLR | 2.54 [1.61–3.49] | 2.15 [1.80–2.35] | 0.339 |
| MLR | 0.208 [0.145–0.262] | 0.225 [0.181–0.264] | 0.685 |
| PLR | 134.1 [104.4–182.9] | 104.7 [84.9–127.5] | 0.212 |
| CRP (mg/dL) | 0.18 [0.08–0.61] | 0.64 [0.4325–0.8375] | 0.284 |
| Correlations with age § | rho | p | |
| NLR | −0.207 | 0.13 | |
| MLR | −0.204 | 0.135 | |
| PLR | −0.43 | 0.00104 ** | |
| CRP (mg/dL) | −0.0544 | 0.693 | |
| Correlations with BMI § | rho | p | |
| NLR | −0.343 | 0.0111 * | |
| MLR | −0.248 | 0.0701 | |
| PLR | −0.379 | 0.00468 ** | |
| CRP (mg/dL) | −0.121 | 0.363 | |
| Correlations with disease duration § | rho | p | |
| NLR | −0.0666 | 0.629 | |
| MLR | 0.269 | 0.0473 * | |
| PLR | 0.105 | 0.446 | |
| CRP (mg/dL) | −0.144 | 0.294 | |
| Week 0 | Week 12 | Week 52 | |||||
|---|---|---|---|---|---|---|---|
| Biologic (n) | Parameters | rho | p | rho | p | rho | p |
| Whole TNF-α inhibitors (55) | NLR vs. MLR | 0.64 | 0.000000324 ** | 0.596 | 0.00000154 ** | 0.732 | 4.08 × 10−7 ** |
| NLR vs. PLR | 0.725 | < 2.2 × 10−16 ** | 0.624 | 0.0000007 ** | 0.485 | 0.0017 ** | |
| NLR vs. CRP | 0.504 | 0.000086 ** | 0.539 | 0.0000219 ** | 0.368 | 0.0194 ** | |
| MLR vs. PLR | 0.555 | 0.0000155 ** | 0.485 | 0.000172 ** | 0.479 | 0.00197 ** | |
| MLR vs. CRP | 0.293 | 0.0298 * | 0.305 | 0.0234 * | 0.457 | 0.00307 ** | |
| PLR vs. CRP | 0.236 | 0.0833 | 0.155 | 0.258 | 0.274 | 0.087 | |
| IFX (28) | NLR vs. MLR | 0.758 | 0.00000632 ** | 0.644 | 0.000302 ** | 0.698 | 0.000431 ** |
| NLR vs. PLR | 0.84 | 0.00000135 ** | 0.69 | 0.0000741 ** | 0.698 | 0.000431 ** | |
| NLR vs. CRP | 0.463 | 0.0132 * | 0.536 | 0.00325 ** | 0.478 | 0.0246 * | |
| MLR vs. PLR | 0.694 | 0.0000653 ** | 0.687 | 0.0000825 ** | 0.713 | 0.000288 ** | |
| MLR vs. CRP | 0.454 | 0.0151 * | 0.349 | 0.0691 | 0.638 | 0.0014 ** | |
| PLR vs. CRP | 0.406 | 0.0321* | 0.24 | 0.219 | 0.287 | 0.195 | |
| ADA (15) | NLR vs. MLR | 0.389 | 0.152 | 0.482 | 0.0711 | −0.212 | 0.56 |
| NLR vs. PLR | 0.711 | 0.00406 ** | 0.654 | 0.01 * | 0.77 | 0.0137 * | |
| NLR vs. CRP | 0.605 | 0.0168 * | 0.569 | 0.0268 * | 0.382 | 0.276 | |
| MLR vs. PLR | 0.511 | 0.0543 | 0.325 | 0.237 | 0.0545 | 0.892 | |
| MLR vs. CRP | 0.319 | 0.247 | 0.131 | 0.641 | 0.273 | 0.445 | |
| PLR vs. CRP | 0.317 | 0.249 | 0.161 | 0.567 | 0.287 | 0.422 | |
| CZP (12) | NLR vs. MLR | 0.35 | 0.266 | 0.515 | 0.0867 | 0.762 | 0.0368 * |
| NLR vs. PLR | 0.65 | 0.0259 * | 0.573 | 0.0555 | 0.738 | 0.0458 * | |
| NLR vs. CRP | 0.472 | 0.121 | 0.269 | 0.399 | −0.0479 | 0.91 | |
| MLR vs. PLR | 0.476 | 0.121 | 0.193 | 0.549 | 0.31 | 0.462 | |
| MLR vs. CRP | −0.0916 | 0.777 | 0.0549 | 0.866 | 0.0719 | 0.866 | |
| PLR vs. CRP | −0.0352 | 0.913 | −0.113 | 0.726 | 0.18 | 0.67 | |
| Week 12 | Week 52 | ||||
|---|---|---|---|---|---|
| Biologic (n) | Laboratory Parameters | rho | p | rho | p |
| Whole TNF-α inhibitors (55) | NLR | 0.0795 | 0.564 | 0.24 | 0.135 |
| MLR | 0.0406 | 0.768 | 0.251 | 0.119 | |
| PLR | 0.0287 | 0.835 | 0.356 | 0.0243 * | |
| CRP | 0.222 | 0.103 | 0.418 | 0.00725 ** | |
| IFX (28) | NLR | 0.0342 | 0.863 | 0.158 | 0.482 |
| MLR | 0.00904 | 0.964 | 0.219 | 0.327 | |
| PLR | 0.102 | 0.606 | 0.218 | 0.33 | |
| CRP | 0.268 | 0.168 | 0.466 | 0.0288 * | |
| ADA (15) | NLR | 0.192 | 0.512 | 0.317 | 0.41 |
| MLR | 0.258 | 0.374 | −0.05 | 0.912 | |
| PLR | 0.0705 | 0.811 | 0.4 | 0.291 | |
| CRP | 0.288 | 0.319 | 0.617 | 0.0857 | |
| CZP (12) | NLR | 0.273 | 0.39 | −0.599 | 0.117 |
| MLR | −0.035 | 0.914 | 0.311 | 0.453 | |
| PLR | −0.396 | 0.203 | −0.168 | 0.691 | |
| CRP | 0.378 | 0.226 | −0.247 | 0.555 | |
| Week 12 | Week 52 | ||||||
|---|---|---|---|---|---|---|---|
| Percent Reduction of PASI | Percent Reduction of PASI | ||||||
| Biologics | Laboratory Parameters | <75% | ≥75% | p | <75% | ≥75% | p |
| Whole TNF-α inhibitors | n | 28 | 27 | 18 | 22 | ||
| NLR | 34 [13–49] | 40 [16–60] | 0.457 | 27 [6–49] | 39 [19–52] | 0.325 | |
| MLR | 17 [–7–33] | 29 [–12–42] | 0.336 | 7 [–4–38] | 26 [13–37] | 0.251 | |
| PLR | 22 [–5–30] | 20 [10–42] | 0.553 | 22 [–11–31] | 27 [6–43] | 0.163 | |
| CRP | 27 [–10–62] | 55 [7–93] | 0.0676 | 15 [–19–68] | 63 [51–90] | 0.0106 * | |
| IFX | n | 11 | 17 | 10 | 12 | ||
| NLR | 30 [−1–35] | 24 [11–44] | 0.677 | 22 [6–27] | 19 [11–40] | 0.821 | |
| MLR | 7 [−17–28] | 25 [−16–41] | 0.611 | 15 [2–39] | 26 [8–32] | 0.872 | |
| PLR | 4 [−6–29] | 20 [−11–42] | 0.547 | 13 [−12–25] | 11 [1–44] | 0.346 | |
| CRP | −19 [−65–29] | 38 [13–92] | 0.0407 * | 8 [−34–43] | 59 [35–81] | 0.0697 | |
| ADA | n | 10 | 5 | 5 | 5 | ||
| NLR | 29 [8–43] | 61 [18–64] | 0.44 | 33 [−21–43] | 61 [52–68] | 0.0952 | |
| MLR | 21 [−8–34] | 32 [13–57] | 0.594 | 3 [−9–33] | 32 [30–41] | 0.421 | |
| PLR | 22 [−2–27] | 13 [13–44] | 0.44 | 28 [−21–32] | 42 [39–50] | 0.0556 | |
| CRP | 32 [4–56] | 87 [0–94] | 0.58 | 17 [0–71] | 78 [77–99] | 0.0159 * | |
| CZP | n | 7 | 5 | 3 | 5 | ||
| NLR | 49 [39–50] | 58 [49–70] | 0.268 | 50 [49–60] | 44 [37–49] | 0.571 | |
| MLR | 17 [1–37] | 32 [30–39] | 0.343 | −5 [−65–17] | 27 [18–27] | 0.25 | |
| PLR | 30 [22–38] | 22 [21–28] | 0.53 | 33 [28–43] | 26 [17–28] | 0.25 | |
| CRP | 71 [50–91] | 89 [28–90] | 0.568 | 72 [26–79] | 60 [56–60] | 1 | |
| Whole TNF-α Inhibitors (55) | IFX (28) | ADA (15) | CZP (12) | |||||
|---|---|---|---|---|---|---|---|---|
| Background Factors | rho | p | rho | p | rho | p | rho | p |
| Age | −0.0433 | 0.791 | 0.032 | 0.888 | −0.164 | 0.657 | −0.192 | 0.649 |
| BMI | −0.00324 | 0.984 | 0.188 | 0.402 | −0.31 | 0.417 | 0.0958 | 0.821 |
| Disease duration | −0.197 | 0.224 | −0.299 | 0.177 | −0.178 | 0.623 | −0.0783 | 0.854 |
| Baseline PASI | 0.248 | 0.122 | 0.225 | 0.315 | 0.648 | 0.049 * | 0.614 | 0.105 |
| Baseline CRP | 0.195 | 0.229 | 0.164 | 0.467 | 0.584 | 0.0765 | −0.735 | 0.0378 * |
| Baseline NLR | −0.104 | 0.522 | −0.312 | 0.158 | 0.164 | 0.657 | −0.0599 | 0.888 |
| Baseline MLR | −0.1 | 0.537 | −0.153 | 0.496 | 0.00606 | 1 | 0 | 1 |
| Baseline PLR | −0.0401 | 0.806 | −0.167 | 0.459 | 0.0182 | 0.973 | 0.204 | 0.629 |
| Sex | Arthritis | Scalp Lesions | Genital Lesions | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Biologics (n) | Male | Female | p | Absence | Presence | p | Absence | Presence | p | Absence | Presence | p | |
| Whole TNF-α inhibitors (55) † | n (%) | 43 (78.2) | 12 (21.8) | 17 (30.9) | 38 (69.1) | 13 (23.6) | 41 (74.5) | 31 (56.3) | 17 (30.9) | ||||
| Percent reduction of PASI | 74 [43–93] | 83 [76–87] | 0.327 | 69 [36–84] | 76 [58–90] | 0.345 | 75 [14–86] | 76 [57–89] | 0.44 | 83 [61–94] | 60 [44–81] | 0.0378 * | |
| IFX (28) † | n (%) | 6 (21.4) | 22 (78.6) | 13 (46.4) | 15 (53.6) | 7 (25.9) | 20 (71.4) | 15 (53.6) | 8 (28.6) | ||||
| Percent reduction of PASI | 75 [46–91] | 72 [62–81] | 1 | 68 [46–81] | 76 [62–87] | 0.307 | 78 [75–95] | 65 [49–82] | 0.319 | 82 [65–95] | 56 [40–75] | 0.0383 * | |
| ADA (15) ‡ | n (%) | 12 (80.0) | 3 (20.0) | 4 (26.7) | 11 (73.3) | 4 (26.7) | 11 (73.3) | 10 (66.7) | 3 (20) | ||||
| Percent reduction of PASI | 48.0 ± 49.6 | 87.3 ± 1.8 | 0.316 | 33.3 ± 94.3 | 61.5 ± 36.9 | 0.479 | −4.9 ± 26.3 | 82.0 ± 20.2 | 0.00043 ** | 61.8 ± 41.4 | 26.4 ± 84.4 | 0.404 | |
| CZP (12) ‡ | n (%) | 9 (75.0) | 3 (25.0) | 0 (0) | 12 (100) | 2 (16.7) | 10 (83.3) | 6 (50) | 6 (50) | ||||
| Percent reduction of PASI | 72.5 ± 17.2 | 88.0 ± 6.6 | 0.278 | Not done | 75.5 ± 24.2 | 76.6 ± 16.1 | 0.938 | 81.4 ± 19.1 | 71.3 ± 14.0 | 0.422 | |||
| Nail Lesions | Diabetes Mellitus | Current Smoking | Bio-Switch | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Biologics (n) | Absence | Presence | p | Absence | Presence | p | Absence | Presence | p | Absence | Presence | p | |
| Whole TNF-α inhibitors (55) † | n (%) | 23 (41.8) | 30 (54.6) | 47 (85.5) | 8 (14.6) | 14 (25.5) | 37 (67.3) | 39 (70.9) | 16 (29.1) | ||||
| Percent reduction of PASI | 81 [53–90] | 75 [56–89] | 0.746 | 76 [56–88] | 74 [55–91] | 0.805 | 76 [51–83] | 76 [57–92] | 0.797 | 76 [56–90] | 74 [45–88] | 0.755 | |
| IFX (28) † | n (%) | 11 (39.3) | 15 (53.6) | 25 (89.3) | 3 (10.7) | 8 (28.6) | 17 (60.7) | 27 (96.4) | 1 (3.6) | ||||
| Percent reduction of PASI | 80 [51–83] | 70 [53–84] | 0.722 | 76 [53–85] | 58 [55–62] | 0.458 | 80 [60–88] | 75 [56–83] | 0.663 | 76 [51–83] | 75 [75,75] | 1 | |
| ADA (15) ‡ | n (%) | 5 (33.3) | 10 (66. 7) | 11 (73.3) | 4 (26.7) | 2 (13.3) | 12 (80.0) | 5 (33.3) | 10 (66.7) | ||||
| Percent reduction of PASI | 28.4 ± 67.2 | 67.7 ± 35.2 | 0.245 | 52.2 ± 46.8 | 64.5 ± 55.9 | 0.727 | 18.5 ± 0.0 | 60.0 ± 47.6 | 0.432 | 64.5 ± 55.9 | 52.2 ± 46.8 | 0.727 | |
| CZP (12) ‡ | n (%) | 7 (58.3) | 5 (41.7) | 11 (91.7) | 1 (8.3) | 4 (33.3) | 8 (66.7) | 7 (58.3) | 5 (41.7) | ||||
| Percent reduction of PASI | 79.1 ± 17.7 | 68.0 ± 11.3 | 0.449 | 81.4 ± 19.1 | 71.3 ± 14.0 | 0.422 | 72.2 ± 13.5 | 78.9 ± 18.9 | 0.615 | 75.1 ± 14.5 | 80.0 ± 28.3 | 0.745 | |
| Biologic (n) | Whole TNF-α Inhibitors (55) | IFX (28) | ADA (15) | CZP (12) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β Coefficient | Standard Error | t | p | β Coefficient | Standard Error | t | p | β Coefficient | Standard Error | t | p | β Coefficient | Standard Error | t | p | |
| (Intercept) | 0.152 | 0.488 | 0.311 | 0.758 | 0.211 | 0.799 | 0.264 | 0.796 | 742.4 | 1132.1 | 0.657 | 0.559 | −937.3 | 411.1 | −2.2801 | 0.107 |
| Age | −0.001 | 0.004 | −0.321 | 0.750 | −0.004 | 0.006 | −0.791 | 0.442 | 0.0084 | 0.0047 | 1.796 | 0.170 | 0.00297 | 0.00397 | 0.7467 | 0.509 |
| Sex (Male = 1, female = 2) | 0.245 | 0.157 | 1.558 | 0.129 | 0.158 | 0.252 | 0.627 | 0.541 | 0.0977 | 0.4132 | 0.2364 | 0.828 | 0.32100 | 0.14414 | 2.2271 | 0.112 |
| BMI (kg/m2) | 0.014 | 0.014 | 1.0378 | 0.307 | 0.024 | 0.019 | 1.247 | 0.233 | 3.37 × 10−7 | 0.00000 | 0.6563 | 0.558 | −4.2 × 10−7 | 0.000 | −2.2815 | 0.107 |
| Baseline PASI | NA | 0.0343 | 0.0138 | 2.4885 | 0.089 | NA | ||||||||||
| Baseline CRP (mg/dL) | NA | NA | −0.1563 | 0.090448 | −1.7284 | 0.182 | ||||||||||
| Scalp lesions | NA | 0.8279 | 0.156 | 5.2933 | 0.013 * | NA | ||||||||||
| Genital lesions | −0.230 | 0.121 | −1.895 | 0.067 | −0.285 | 0.165 | −1.730 | 0.106 | NA | NA | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hagino, T.; Saeki, H.; Kanda, N. Biomarkers and Predictive Factors for Treatment Response to Tumor Necrosis Factor-α Inhibitors in Patients with Psoriasis. J. Clin. Med. 2023, 12, 974. https://doi.org/10.3390/jcm12030974
Hagino T, Saeki H, Kanda N. Biomarkers and Predictive Factors for Treatment Response to Tumor Necrosis Factor-α Inhibitors in Patients with Psoriasis. Journal of Clinical Medicine. 2023; 12(3):974. https://doi.org/10.3390/jcm12030974
Chicago/Turabian StyleHagino, Teppei, Hidehisa Saeki, and Naoko Kanda. 2023. "Biomarkers and Predictive Factors for Treatment Response to Tumor Necrosis Factor-α Inhibitors in Patients with Psoriasis" Journal of Clinical Medicine 12, no. 3: 974. https://doi.org/10.3390/jcm12030974
APA StyleHagino, T., Saeki, H., & Kanda, N. (2023). Biomarkers and Predictive Factors for Treatment Response to Tumor Necrosis Factor-α Inhibitors in Patients with Psoriasis. Journal of Clinical Medicine, 12(3), 974. https://doi.org/10.3390/jcm12030974